
Abstract
Nursing homes are a common site of death, but older residents receive variable quality of end-of-life care. We used a mixed methods design to identify external influences on the quality of end-of-life care in nursing homes. Two qualitative case studies were conducted and a postal survey of 180 nursing homes surrounding the case study sites. In the case studies, qualitative interviews were held with seven members of nursing home staff and 10 external staff. Problems in accessing support for end-of-life care reported in the survey included variable support by general practitioners (GPs), reluctance among GPs to prescribe appropriate medication, lack of support from other agencies, lack of out of hours support, cost of syringe drivers and lack of access to training. Most care homes were implementing a care pathway. Those that were not rated their end-of-life care as in need of improvement or as average. The case studies suggest that critical factors in improving end-of-life care in nursing homes include developing clinical leadership, developing relationships with GPs, the support of ‘key’ external advocates and leverage of additional resources by adoption of care pathway tools.
Introduction
Nursing homes are an increasingly common site of death. In England, 16% of all deaths take place in the long-term care sector, 1 with most occurring in nursing homes among over 85 year olds. 2 Predicted socio demographic trends show rapid increases in the numbers of people aged over 85 and of single households, with concomitant decreases in the availability of informal carers. These trends mean that nursing homes are likely to remain as important sites of end-of-life care for the foreseeable future. 3
Older people admitted to nursing homes have been estimated to have a life expectancy of 9–12 months, 4 with those who have dementia having the shortest life expectancy. 5 However, the complexity of chronic and co morbid conditions 6 among residents makes it difficult to recognize and manage the terminal phase. 7 Many residents die after a period of diffuse deterioration marked by increasing disability and frailty, 8 rather than a clearly identifiable ‘terminal illness’. 9 There is evidence that older people residing in care homes receive variable quality in terms of both continuing ‘chronic’ disease care and end-of-life care because of clinical and organizational factors. 10 One study in England 11 has shown that 47% of homes have no provision for chronic disease management for care home residents, such as rehabilitation or physiotherapy, and others have only minimal levels, even though many residents could benefit from the latter. General practitioner (GP) services to care homes are not always organized optimally because of poorly defined funding for the provision of medical care. 12 Similarly, input from clinical nurse specialists or palliative medicine clinicians is rare and, where it occurs, is reactive to crisis situations. 13 Pain and symptom control is often poor as a result, 14 and there is some evidence of inappropriate medication. 10,15 Surveys of bereaved carers show high levels of dissatisfaction with end-of-life care in care homes. 16,17
There has been a proliferation of different care home organizations across England, which creates challenges for the commissioning and funding of end-of-life care services in care homes. 18 In addition, residents’ care is likely to be funded by a mixture of National Health Service (NHS), local authority and private monies, which is likely to make rapid access to resources difficult. 19 Relationships between the range of health and social care agencies that intersect with care homes make care planning complex, and can lead to conflict in terms of the management of a resident’s final illness. This may increase the likelihood that some residents are admitted to hospital at the very end of life who might otherwise be supported in the care home setting. 20
In England, a range of developments have occurred over the last 15 years to support
the provision of end-of-life care in care homes. Specialist palliative care
provision has been supported through the work of: (i) Clinical Nurse Specialists;
(ii) the establishment of ‘hospice beds’ in nursing homes;
(iii) the provision of palliative care education and training for care home staff;
and (iv) the development of link nurse schemes.
20
The promotion of general palliative care for any resident is now the main
focus of developments,
21
as reflected in the emphases of the National End of Life Care Programme,
which has a specific stream of work concerning care homes.
22,23
Within this, a number of
initiatives are being promoted to support the provision of end-of-life care in care
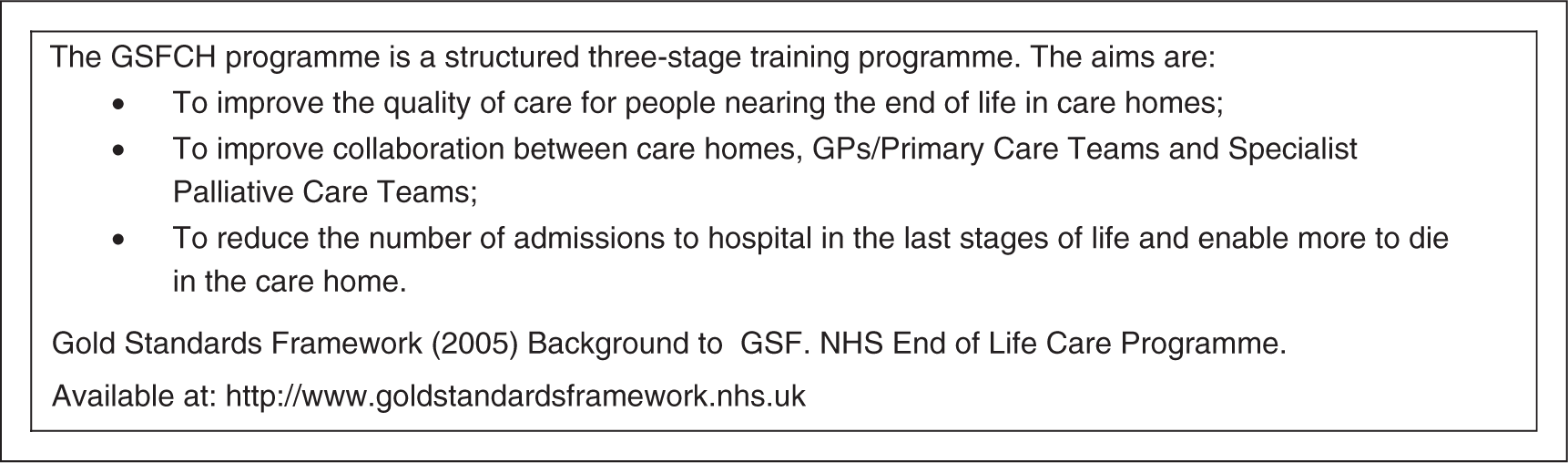
homes, including the care and service planning tools: the Liverpool Care Pathway
(LCP) for the Dying (Figure
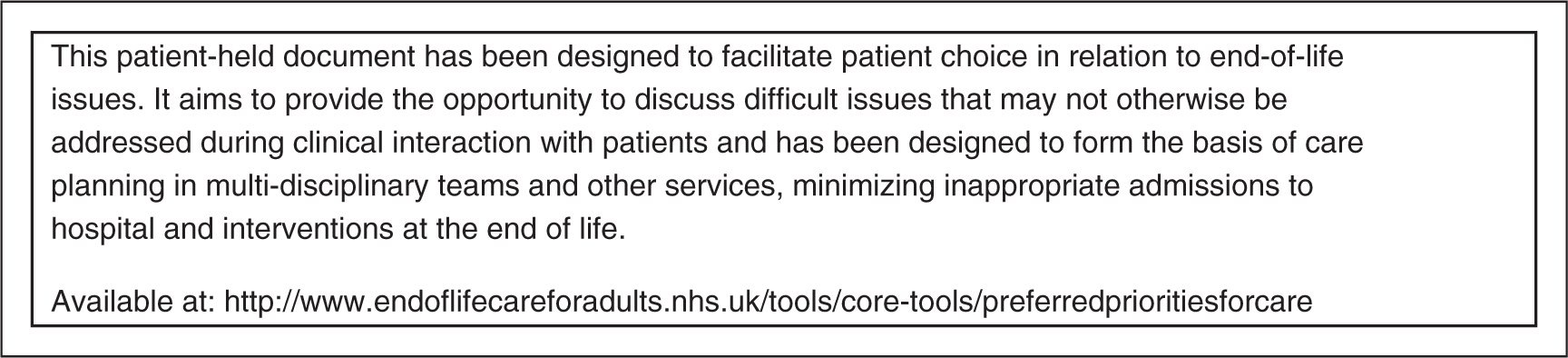
1); the Gold Standards Framework (GSF; Figure 2); and the Preferred Priorities for
Care (Figure 3). There are
also a large number of local initiatives and developments.
23
The Liverpool Care Pathway for the Dying. The Gold Standards Framework in Care Homes Programme (GSFCH). Preferred Priorities for Care (PPC) plan.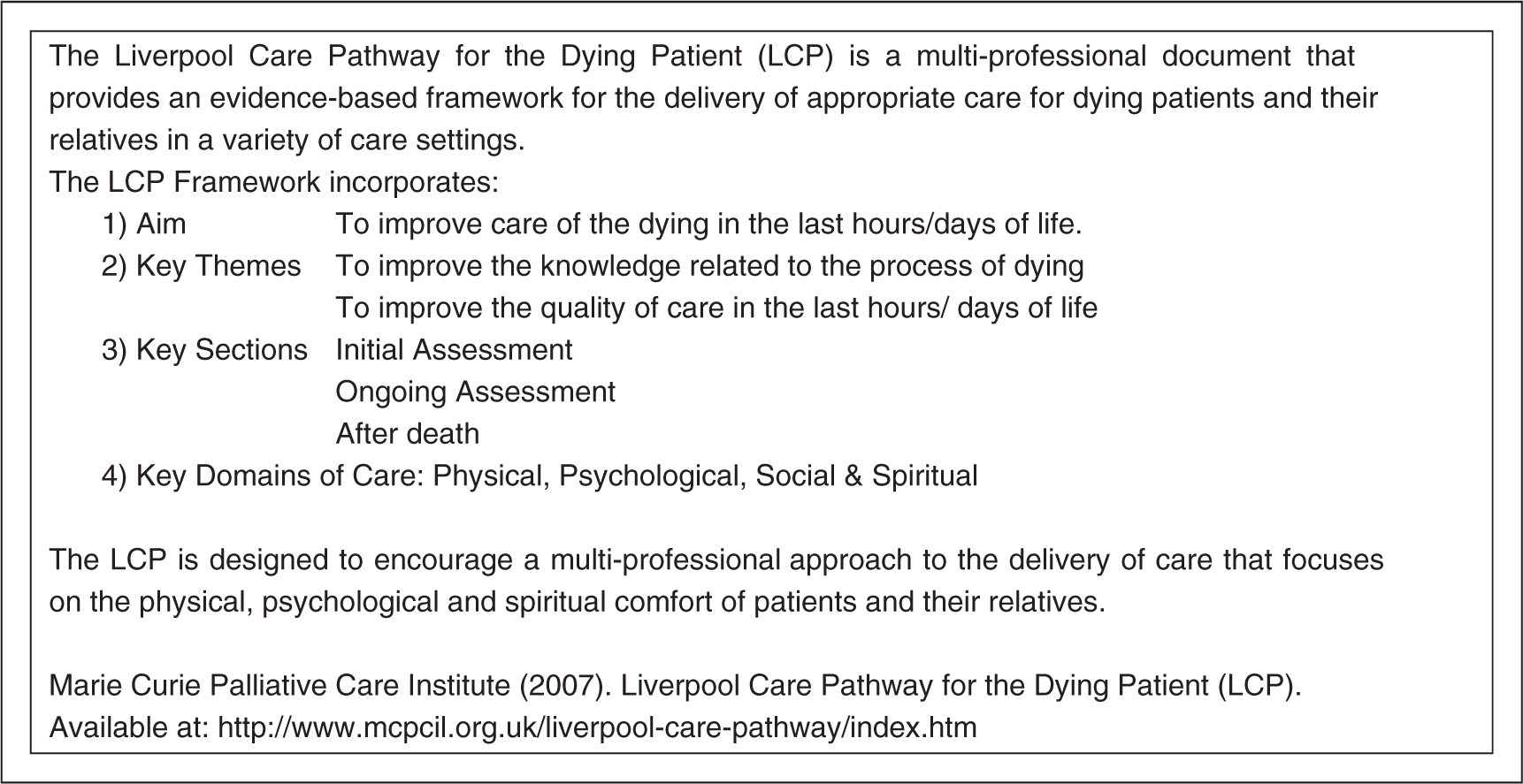
This paper draws from a study commissioned by the National End of Life Care Programme in England 24 in the context of the programme’s attempt to assess the effectiveness of the various initiatives outlined above and to inform recommendations for the further development of policy and practice. The aim of the study was to identify key factors in the wider health and social care system influencing the quality of end-of-life care provided in nursing homes. The study aim and method of enquiry was informed by an expert steering group made up of representatives from the funders, umbrella organizations for nursing home and care providers, regulatory bodies and NHS Trusts.
Methods
Setting and design
A mixed methods design was employed, consisting of two in-depth qualitative case studies 25 of nursing homes and a postal survey of the managers of 180 nursing homes surrounding the case study sites. Names and addresses of care homes with nursing care and registered to care for ‘old age’ (not falling into any other category) were identified from the Commission for Social Care Inspection (CSCI; now the Care Quality Commission) database, 26 which is the regulatory body for care homes in England. The survey was developed from a review of previous surveys used in related research 27,28 and piloted in two focus groups with care home staff. The survey included questions about the profile of deaths in the homes, access to external support and barriers to and perceived priorities for improving end-of-life care.
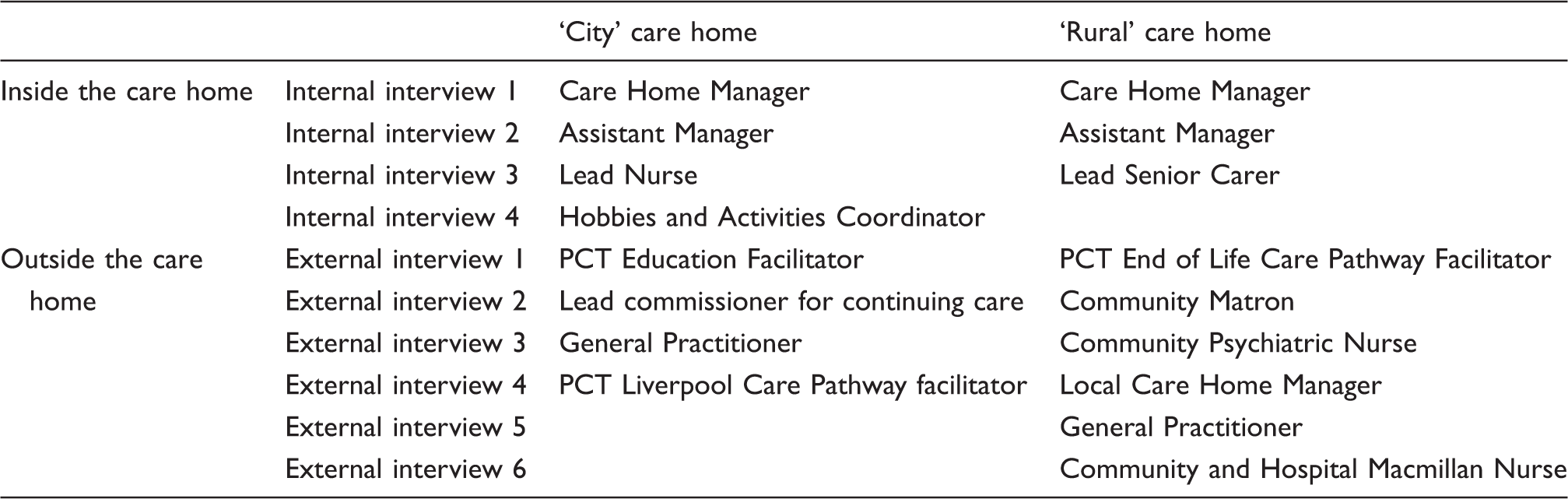
Interviews conducted in each case study
Analysis
Survey data were analysed to produce descriptive statistics with the aid of the Statistical Package for the Social Sciences (SPSS)©. Free text comments added to the survey document were subject to content analysis. The findings from the survey were used to design an aide memoire and initial coding frame for the qualitative interview data. The framework was then modified to include any new issues within interviewees’ accounts. In addition to a thematic analysis of the interviews, we sought to understand the narratives recounted about the recent history of the care homes and developed short historical profiles of each home, focusing on understanding how problems associated with external support for end-of-life care had been addressed. One researcher (AK) conducted the initial analysis, which was then checked by JS and KF. Summary reports of the project were sent to each care home that had participated in the study. Case study care homes provided comments on a draft of their case study report, clarifying points of detail and weight of interpretation. This acted as a means of respondent validation. 29
Ethical review
Ethical committee approval was gained through the UK National Research Ethics Service. We gained research governance approval to interview stakeholders in the case studies from relevant Primary Health Care Trusts.
Findings
Survey
Following one reminder, we received a response from 46% (82) of the nursing homes surveyed.
Profile of deaths, self-rating of end-of-life care and use of ‘pathways’
Seventy-four percent (n = 62) of the care homes that returned the survey reported that they were registered as both residential and nursing homes; the remaining provided nursing care only. Responding homes ranged in size from 19 to 180 beds and reported a mean of 18 deaths per home (range 2–90) in 2007. Of the 1182 residents’ deaths reported, 76.5% (904) took place in the home, 23.3% (275) in hospital and 0.25% (3) in a hospice. Seventy-seven percent of deaths were reported to be caused primarily by non-cancer conditions.
Seventy eight percent of the responding care homes (64) self-rated the quality of their end-of-life care. Of these, one home described it as ‘needs improving’, three as ‘average’, 33 as ‘good’ and 27 as ‘excellent’. Ninety-eight percent (80) of the responding care homes responded to a question about use of end-of-life tools. Most (50) reported use of the LCP, with smaller numbers reporting use of the GSF (21) and/or Preferred Priorities of Care (PPC) (4). Sixteen homes were using both the LCP and the GSF. Eight care homes reported they were using their own care pathway or one that had been locally developed. Of the 60 homes rating their end-of-life care as ‘good’ or ‘excellent’, the majority (46) reported use of a care pathway. The four homes rating their care as ‘needs improving’ or ‘average’ reported that they were not using a care pathway.
Levels of support received
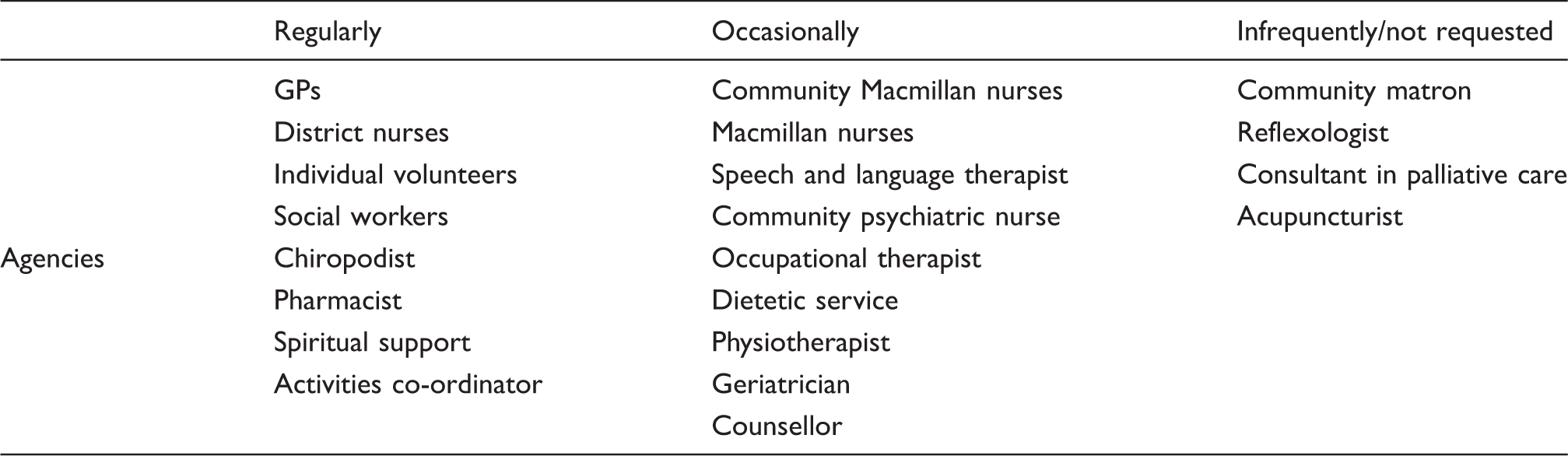
Reported levels of support received from external staff and agencies
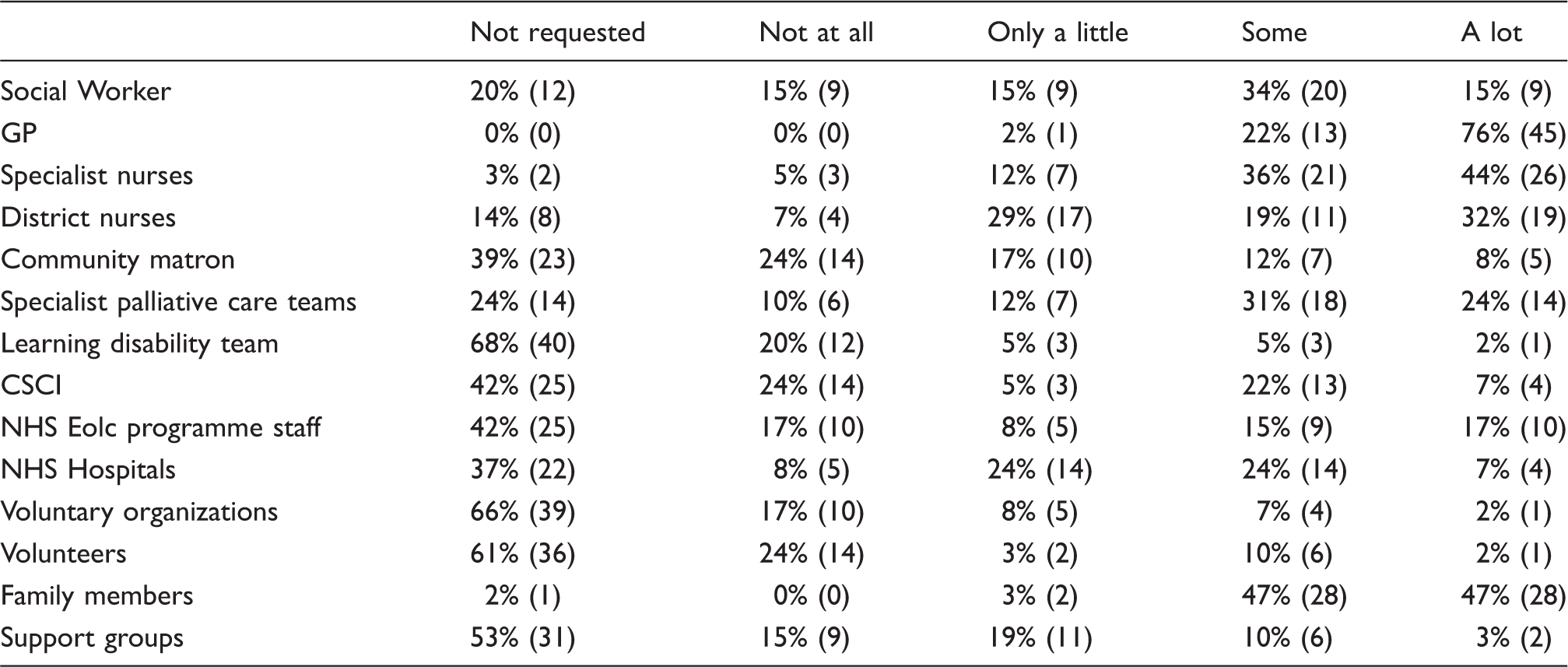
Reported frequency of visits by external staff and agencies
Sixty-six percent of responding care homes (53) reported that they accessed specialist palliative care support in the form of a direct advice line to the local hospice or Macmillan nurses. Ninety-three percent of responding care homes (76) reported a range of 1–11 GP practices with which they liaised (mean of five); and a range of 1–34 individual GPs with whom they liaised (mean of 12).
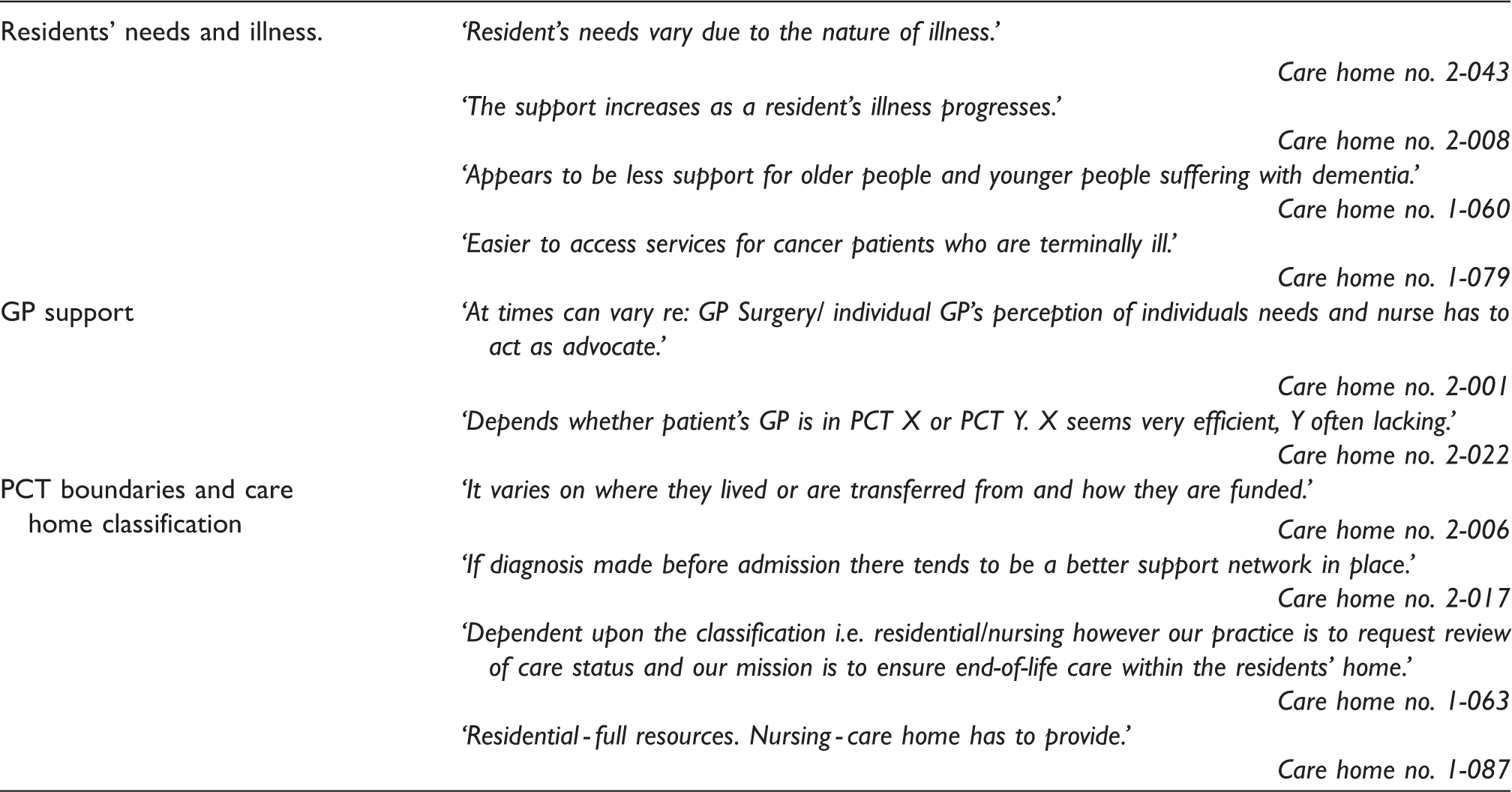
Examples of qualitative comments about support received for end-of-life care
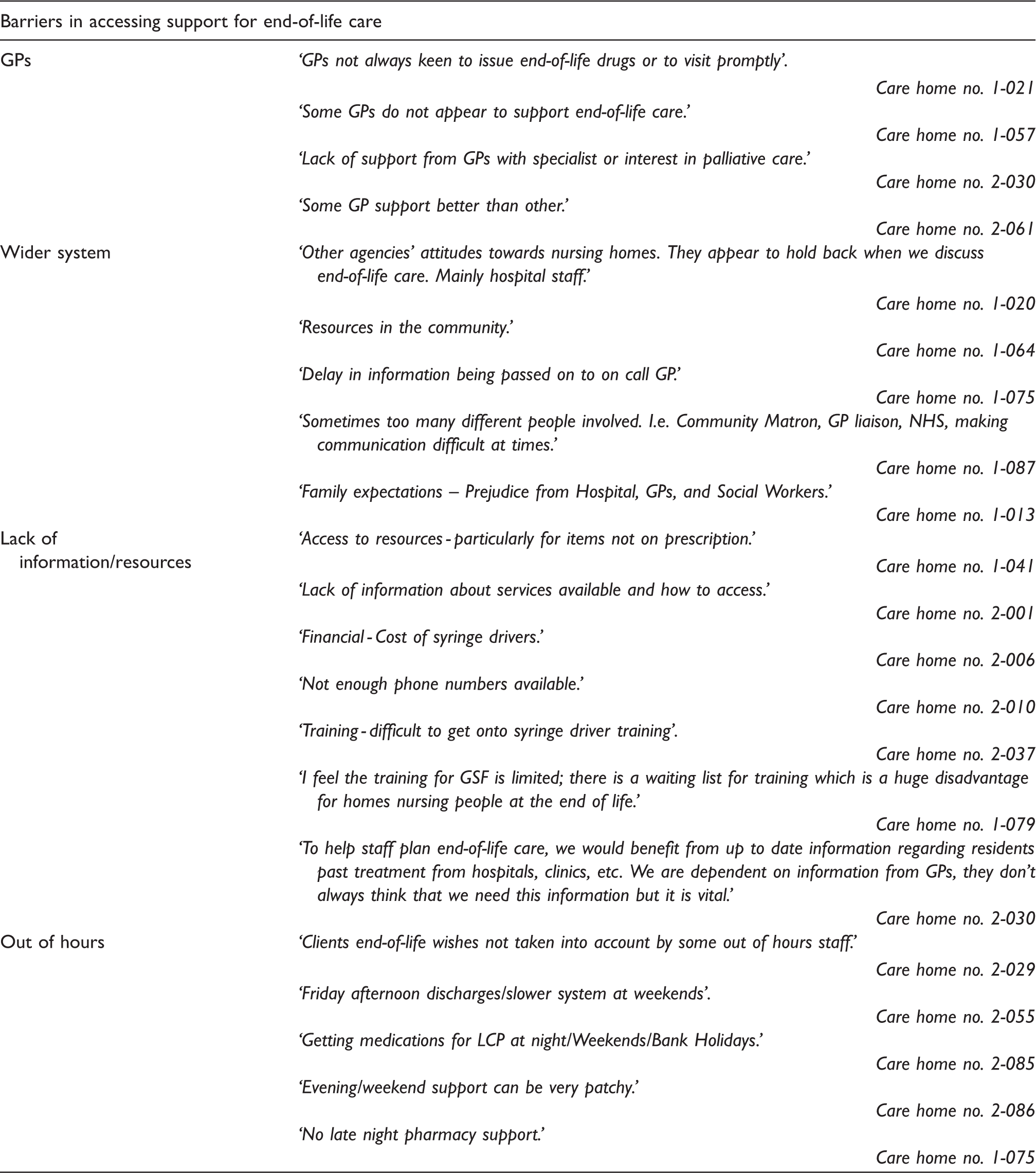
Barriers to end-of-life care
Examples of qualitative comments about barriers to end-of-life care
The case studies were conducted to shed light on how issues revealed by the survey were encountered in contrasting rural and urban contexts, by two homes judged by expert stakeholders to provide a good quality of end-of-life care.
Case studies
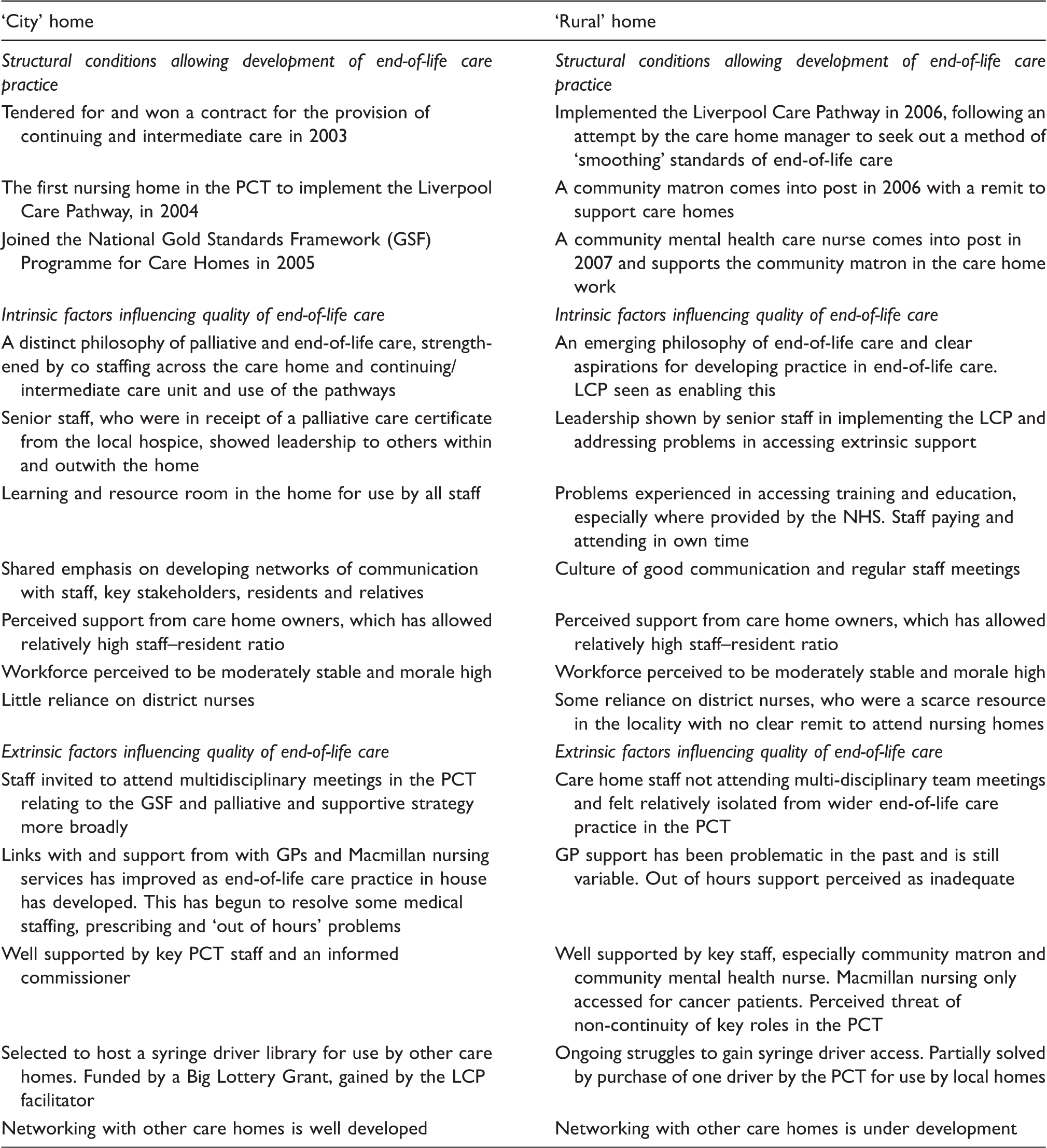
Key findings from the case studies
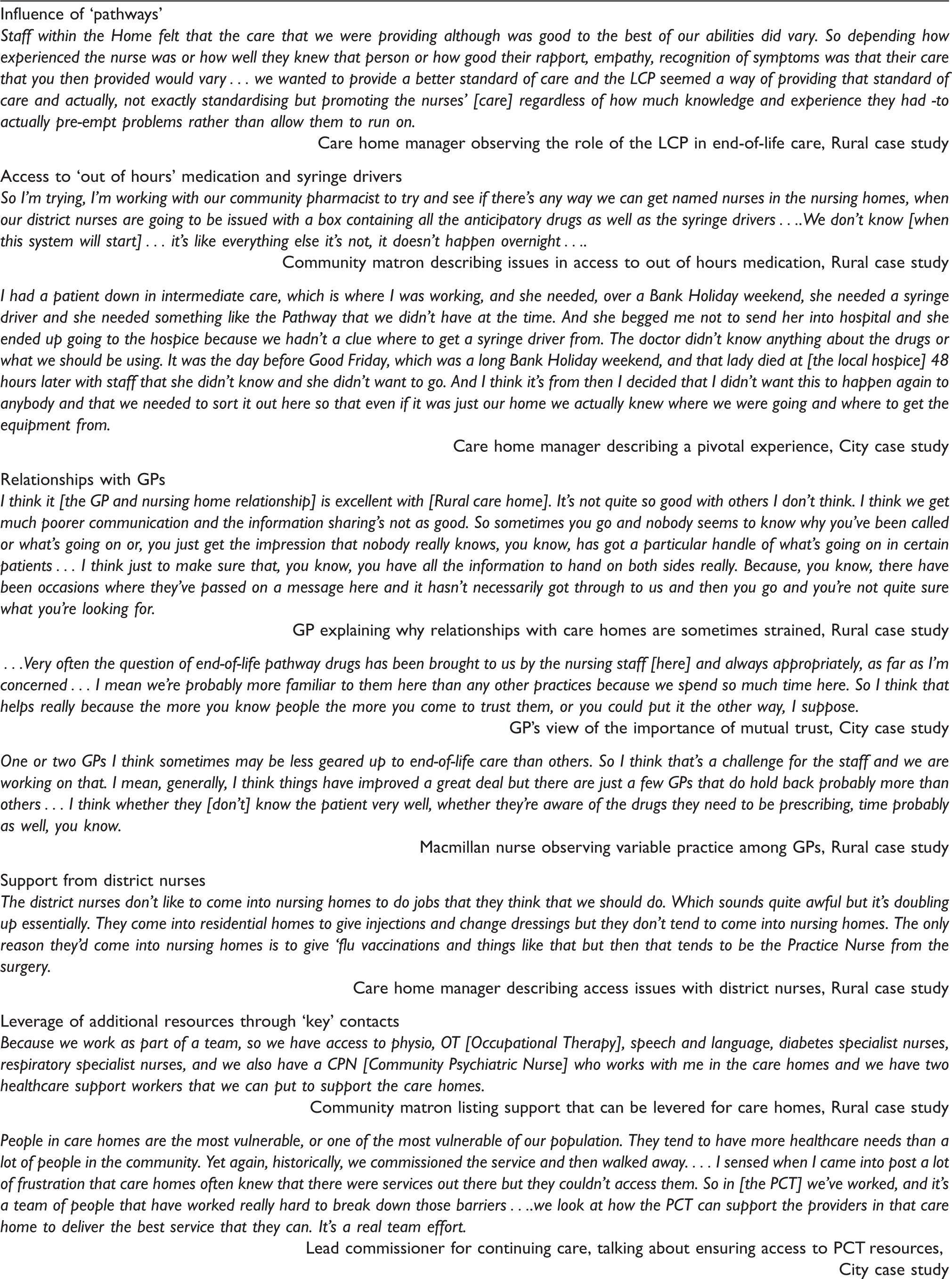
Examples of interview quotes about external support accessed by the case study homes

The ‘City’ care home
(Code for Interviews: A: care home manager; B: assistant manager; C: lead nurse; D: education facilitator; E: lead commissioner for continuing care; F: GP; G: LCP facilitator.)
The City care home was providing care to 58 residents at the time of the study. It had an integral unit for the delivery of intermediate and continuing care. Between 1 January and 31 December 2007, there were 30 residents who died in the home and five residents who died at the local hospitalc. The CSCI completed an unannounced inspection of the home in December 2006 and found the atmosphere within the home as ‘welcoming and warm’. The ‘staff and residents spoken to had a sense of humour and appeared relaxed and comfortable’. The report described the ‘communication skills of the staff with individuals [was observed] to be very positive’. The report further found ‘residents and visiting relatives said the staff were generally very kind, helpful and friendly’ and ‘the relationship between residents/relatives and staff appeared positive and the residents were treated with respect’ (Commission for Social Care Inspection (2006); Inspection report). The current manager came into post in 2001, having previously worked as a district nurse for 25 yearsa. She has a very clear vision for the development of palliative care in the home, strengthened by co staffing across the care home and continuing/intermediate care unit. She had encouraged senior staff and others to undertake training and education in this area and was able to access training events in the locality. She had developed a resource room for use by care home staff. Staff morale was high and turnover relatively low.
The City home was the first within its Primary Care Trust (PCT) to implement the LCP for the Dying and the GSF, securing, in the opinion of a key stakeholder, its role as a leader in end-of-life care practice among its ‘peer’ care homesg. This followed the development of a palliative care strategy across the local PCTs in 1998, which had been followed by some changes in commissioning practice. The subsequent implementation of the GSF in the City home followed intensive mentorship provided to the care home staff by the LCP facilitatorg and the attendance of care home senior staff at GSF meetings. The care home manager reported that as a result of these regular meetings it had been possible for the City home to build good networks and rapport both with other local care homes and with colleagues in general practice and in specialist palliative care. These in turn enabled them to make timely referrals when they needed help with residents’ end-of-life care needsa,b,c.
Over time City home staff have been able to build good rapport with local GP practicesa. They have developed a relationship of trust with one GP in particular from whom they now regularly receive visits. The support given from this and other GPs in providing end-of-life care is now highly esteemed by the senior staff and is complemented by the care home’s long-standing relationship with a local pharmacist, which aids access to prescribed medication when requested ‘out of hours’c. The role of the City home in end-of-life care was supported by an enlightened commissioner for continuing care, who recognized the importance of supporting practice in care homes and aiding access to PCT resources to ensure good end-of-life care for residentse. In the view of the commissioner, collaborative work across the Primary Health Care Trust boundary was beginning to break down the isolation of care homes. As a result, discriminatory attitudes and practices, which meant that once individuals were admitted to care homes with nursing they tended to be regarded as no longer entitled to the services commissioned by the PCT, were changinge.
Following a grant from the Big Lottery Fund (http://www.biglotteryfund.org.uk/ (accessed 15 June 2010)) in 2007, the LCP facilitator explained how he was able to set up a ‘syringe driver library’ in the City home, which is for the use of care homes with nursing in the local areag. This had immediately resolved some, although not all, of the problems of access to syringe drivers among care homes in the locality. The City home was selected to hold the library because of its recognized expertise in end-of-life care.
The ‘Rural’ care home
(Code for interviews: H: care home manager; I: deputy sister; J: senior carer; K: LCP facilitator; L: community matron; M: community psychiatric nurse; N: local care home manager; O: GP; P: Macmillan nurse.)
The Rural home was providing care to 44 residents at the time of the study. Between 1 January and 31 December 2007, there were 25 deaths among residents, of whom 23 died in the home and two died in the local hospitalh. The CSCI was involved in an unannounced inspection the home in April 2007 (Commission for Social Care Inspection (2007); Inspection report) and described the home as ‘domestic in character and well maintained’. The report further notes that there was: ‘ …a warm and welcoming atmosphere was evident on entering the home’ and ‘there was evidence that staff, service users and relatives have a good relationship and they chatted freely’, with service users and visitors having expressed that ‘care was at a good standard and staff were very kind and attentive’. The current care home manager has been in post for approximately four years, since 2004, and is a qualified Registered General Nurse (RGN). She had a clear view of the priorities for end-of-life care practice development in the home.
The Rural home implemented the LCP for the first time in 2006, following a deliberate attempt to seek knowledge about the pathway by the Care Home Manager. Its implementation was perceived to have ‘smoothed’ standards of end-of-life care, making them less dependent upon the particular skills and knowledge of staff or the attributes of their relationships with residents. However, unlike the City home, the Rural home encountered some significant problems in extending progress further, largely because of factors that lie outside of its control in the locality.
A key factor was perceived as the cessation of the contract for the end-of-life care facilitator within the PCT in 2008h,l,m,p. As a result, there is no longer a dedicated role within the PCT to introduce and provide ongoing training for the LCP. The manager of the Rural home also reported that accessing GP support, prescribed medication and transferring a resident to the hospital during out of hours was very difficulth. Some GPs endeavoured to overcome problems by ensuring medication was pre-emptively prescribed for individuals prior to the weekends, but this did not always provide the solution to unexpected problems among residentsh,j,o. Lack of involvement in PCT meetings meant that staff in the Rural home felt isolated from wider end-of-life care developments in the localityh,m,n. This was improving since the appointment of a community matron with a remit for care homes and a community psychiatric nurse who supported the matron’s work with care homes.
The care home manager was keen that staff undertook training to develop their knowledge in end-of-life care issues, but found it difficult to access courses locally, since most of these were only available for NHS staffh,j,k,m. Those staff who did attend development events often did so in their own time and using their own funds. In spite of this, staff morale was high and turnover relatively low h,i,j,k.
Accessing syringe drivers when these were needed was also a problem. The care home manager reported that the GP practice would be the first point of call for obtaining a syringe driverh. If the GP practice could not provide one then she would telephone the community matron or the local hospice and usually, by this lengthy process, would manage to obtain oneh. However, gaining assistance with setting up the driver was sometimes problematic. The care home manager related a recent occasion when a driver was needed but she had not used one for over six months and no longer felt confident to set one up. After some difficulty, she managed to get advice and help from a district nurseh. Support from district nurses was generally perceived to be much needed but hard to accessh,i,j,o. At the time of fieldwork, the community matron was trying to arrange for the care home manager to attend syringe driver training on a regular basis (potentially every three months) at the local hospice. It was reported that this was a means of pre-empting difficulties in using and calibrating syringe drivers, of reducing dependence on district nurses, and of strengthening the care home manager’s ability to cascade syringe driver training within the homel,o. By the end of the fieldwork, the PCT had loaned one syringe driver to the Rural home for them to use and to lend out to other care homes as requiredl.
Study limitations
Since the study was small scale and exploratory, a decision was made to focus on homes registered to provide nursing care, as opposed to looking more generally at homes providing solely personal care (previously known in England as ‘residential care homes’). It is likely, however, that some of the issues reported here are also relevant to the latter. Furthermore, the homes we studied as ‘cases’ were not part of a wider ‘chain’ provider: this needs to be noted in making sense of the findings. There are a number of other limitations in the study. In keeping with other surveys of care homes, we had a relatively low response rate, 13,30 which limits the representativeness of the findings. However, our response rate was considerably higher than that achieved by a National Audit Office survey of care homes on a similar theme and shows some similar findings. 30 In the case studies, we were not able, for resource reasons, to access the views of older residents or their family carers about their experiences of care; nor, with one exception, were we able to gather the views of front line care assistant staff within care homes. Moreover, our purposive sampling of the two care homes with nursing that are the key case studies in the project meant that it was clearly in their interests to present the care that they provided in a largely positive light. However, by conducting a survey of other care homes in the localities of the cares home involved in the case studies, we have been able to contextualize the case study findings and thus enhance the validity of the study’s conclusions about the support that care homes need in order to provide appropriate end-of-life care. Furthermore, in their interviews with us staff were open and candid about the issues they faced in their daily work: they reported problems and ongoing challenges, as well as those things that were going well, communicating a sense of shared purpose in seeking to improve the capacity of care homes and build on the potential of care homes to provide excellent end-of-life care.
Discussion
This paper has sought to examine the external influences on end-of-life care provision, reporting on how some issues from a simple survey to which 82 homes responded were manifest in two care homes selected as ‘instrumental’ case studies. It was conducted some 10 years after a seminal study in England, which showed how external influences are pivotal to the quality of palliative and end-of-life care provided in care homes for older people 31 and took place at a time when the End of Life Care Strategy in England 32 directed attention towards the need to improve end-of-life care in all settings and among all groups of patients in need.
The majority of nursing homes that took part in the survey reported some access to specialist palliative care services, such as the Macmillan nursing service and/or local hospice in the form of a 24-hour advice telephone line. This was supported by the experiences of the case study care homes both of which had some access to specialist palliative care support. However, in neither the case studies nor the survey did specialist palliative care support appear to be a regularly occurring feature of care provision. Rather, it was apparently dependent upon requests from the homes for such help. In the case of the City home, attendance at local palliative care and GSF meetings meant that they had developed networks of support that they could draw upon for end-of-life care issues. In addition, there is some evidence, from the survey data, of a lack of knowledge in nursing homes about available resources or about key staff who may be able to assist with end-of-life care, particularly for residents with needs arising from conditions other than cancer, such as dementia. It seems that external end-of-life care support provided to nursing homes, in most cases, is still predicated on a model of palliative care provision required for the classic ‘cancer’ trajectory, which is increasingly at odds with the reality of residents’ needs. Similar findings were found in a survey of clinical nurse specialists in palliative care, who reported that they tended to work only with cancer patients and in response to crisis situations in care homes. 12 In the Rural home case study, it was clear that a major contribution to the ability of the home to cope with the residents’ needs was the recently instigated help they received from a community matron and a colleague with whom she worked closely, a community psychiatric nurse, both of whom had special responsibility for care homes in that area. The input the home received from these individuals was regular, proactive and planned, as opposed to irregular and crisis oriented.
The survey data indicated that most support with end-of-life care is provided to nursing homes by GPs and family members, while support from nurses external to the home was somewhat less marked. Neither of the case study care homes reported accessing district nursing support with any regularity; in the case of the City home, the existence of a continuing care unit meant that they could ‘cross cover’ for nursing needs and so perhaps no longer needed such support. In contrast, in the Rural home, district nursing support was a scare but much needed resource, particularly in relation to the management of syringe drivers. Where district nurse help had been received, it was in the knowledge that it was not an ‘allowable’ form of help, since no primary health care trust funds were available for the provision of additional nursing support to nursing homes. This issue of additional nursing support required by residents in nursing homes was highlighted by the Royal Commission on Long Term Care, 32 and has never subsequently been resolved in the UK.
Support from GPs was clearly essential but was associated with a number of characteristic difficulties. Survey respondents briefly alluded in their qualitative comments to problems of communication, ‘out of hours’ coverage and variability in interest, skills and willing attendance to residents’ needs among the GPs they came into contact with: issues also reported in other studies. 30,34 The case studies provided an opportunity to examine this issue from the point of view of two homes that had largely resolved problems with GP care. In the case of the City home, we heard how serious problems in the fairly recent past had been addressed by the development of collegial relationships nurtured by attendance of care home staff at local end-of-life care meetings. In the case of the Rural home, problems were still in evidence, but ameliorated by the development of mutual trust and understanding between one GP and the care home staff. The development of the latter was seen as essential by the two GPs whom we interviewed within the case studies; a condition of its development seemed to be in turn care home staff reaching a certain level of competence and expertise so that they could assess patients’ needs and appropriately refer patients to GPs.
The survey showed that nursing homes which implement an end-of-life care tool, such as the GSF or LCP, were more likely to describe their end-of-life care as ‘excellent’ and ‘good’. Providing some insight into how crucial the implementation of pathways was perceived to be among care home staff and their stakeholders, the case study data reveal how in each home implementation of the LCP, and, in the City home also the GSF, were seen as pivotal to end-of-life care improvement. Similar findings were found in a survey of care homes in England by the National Audit Office, although the validity of the findings from the latter are undermined by a very low response rate of below 10%. 30 The relationship between the use of ‘tools’ and quality of end-of-life care has been identified as needing further examination 35 in all care settings, including nursing homes. One worrying finding was the inconsistent access to education reported by the homes that responded to the survey and the case study homes: staff were often attending study days in their own time and using their own resources and found they were sometimes excluded from mainstream NHS provision. It is likely that the in-house education levered by participation in the LCP and GSF is critical, although whether the cost of participating in the GSF programme inhibits some homes from participation needs to be ascertained. Gibbs, 36 in study of knowledge about pain management, noted how nurses in private nursing homes feel less skilled, are isolated and lack educational opportunities about ‘mainstream’ practice in palliative care. Under-treated pain remains a significant problem in care homes internationally. 37
In the case study homes, clinical leadership and a reasonably stable workforce (supported by a good CSCI reports) meant that the homes had the capacity to successfully implement the tools and to provide some degree of ongoing education to staff. The role of clinical leadership in care homes has been identified as critical to care quality. 38 The care managers in the case study homes were in turn supported by key individuals external to the care homes, such as GSF and LCP facilitators, who often were in a position to ‘lever’ additional resources. The importance of resource leverage and the role of nurses in the latter were similarly observed in a study of the outcomes of Macmillan Nursing conducted in the UK in the 1990s, but remains an under-researched issue in palliative and end-of-life care. 39 In the case of the City home, the influence of a supportive lead commissioner for continuing care was also evident. This commissioner had been able to implement changes in commissioning practice through a process of participating in strategic developments directed at improving the co-ordination of palliative and end-of-life care in the wider vicinity. The City home particularly demonstrates the powerful synergy that can occur between factors such as small-scale practice innovation, personal aspirations, the provision of effective external links for networking and support and wider changes in commissioning practice and attitudes. These all coalesced in the City home, such that they had begun to overcome some intractable problems reported elsewhere. They are now in a position to provide support to other care homes in the locality and to be a ‘beacon’ of good practice. Questions need to be asked about those nursing homes that do not have such a fortunate set of circumstances: it was clear from the survey data that a minority of homes were excluded from the outside support that flows from participation in the LCP and GSF implementation process, where the latter become ‘enablers’ of practice development within the care home and levers of support outside it. Care must be taken to ensure that such isolation does not become a catalyst for the widening of inequalities rather than a factor that motivates key stakeholders in end-of-life care to concentrate their efforts in such environments.
Conclusion
This study has demonstrated how the delivery of good quality end-of-life care in care homes requires an effective balance of external support, such as systems to access medication and syringe drivers, with internal resources, such as staff who are well trained and who work in a supportive culture in which they are able to make residents’ and their relatives’ needs and concerns their first priority. The mixed methods design has shed light on some critical factors that assist homes to manage some characteristic problems of access to external support: clinical leadership, clear understanding and vision about the need to improve end-of-life care, networking with GPs and other local staff and leverage of resources by one or two key external ‘supporters’ have been shown to be particularly important. In addition, the introduction of frameworks or pathways of care appears to assist staff to progress in terms of practice development and education in palliative and end-of-life care, but this needs further study.
The challenge of improving end-of-life care in care homes is usually described in terms of inadequacies in knowledge and training among care home staff. However, suggesting that training of care home staff will solve the issue of quality is a error of simplistic thinking. 40 Rather, attention should in addition focus on challenging those discriminative attitudes, beliefs and practices in the wider system that contribute to the isolation of nursing homes and enhancing the ability of homes to demonstrate leadership in practice development. Although this exploratory study has provided some insights into the complex social structural network surrounding nursing homes, much more work is needed to enable integration of nursing homes into the wider systems of end-of-life care and to enable collaboration across organizational, institutional and funding boundaries, so that patients receive a better quality of end-of-life care regardless of the care setting in which they are located. Moreover, end-of-life care management in care homes should be integrated with and seen as an extension of chronic disease management and rehabilitation; attention to one will improve the other and is likely to result in improved quality of life, pain and symptom management for residents, 11 regardless of any prognostic uncertainty about their status as ‘dying’.
Footnotes
Acknowledgements
Thanks are due to the members of the advisory group and to care home and community staff who participated in the study.
Funding
This work was funded by the National End of Life Care Programme in England.
Competing interests
The authors declare that they have no competing interests.