
Abstract
Objective
Technology-based interventions may enhance self-directed or caregiver-assisted activity during inpatient stroke rehabilitation, yet effective implementation strategies for technology-based tools remain unclear. This scoping review synthesises existing evidence on acceptability, feasibility and effectiveness of technology-based interventions in inpatient stroke rehabilitation, and maps barriers and enablers to implementation through the Capability, Opportunity, Motivation and Behaviour model.
Data sources
Comprehensive searches of MEDLINE, Embase, CINAHL and Google Scholar were conducted through to December 2025.
Review methods
Studies involving adult stroke survivors using self-directed technology-based interventions during inpatient rehabilitation were included. Arksey and O’Malley's scoping review framework guided data extraction. Analysis focused on acceptability, feasibility, effectiveness and behaviour change strategies.
Results
Eighteen high-moderate quality studies (20 papers) from 13 countries, involving 1081 participants, were included (10 pilot randomised controlled trials, 6 feasibility studies, 1 non-randomised and 1 observational study). Interventions were upper limb exergaming or robotics devices (n = 4) and tablet/smartphone applications with exercise videos (n = 14). Acceptability, feasibility and effectiveness outcomes were reported in 12 studies (63%), with rates of recruitment, safety and retention being reported in eight (67%), eight (67%) and six (50%) studies, respectively. All studies reported on at least one construct relating to barriers or enablers. Key enablers were caregiver involvement and additional support for more impaired individuals. Common barriers were stroke-related impairments and reduced staffing.
Conclusion
This review offers an integrated overview of the acceptability, feasibility and effectiveness of technology-based interventions in inpatient stroke rehabilitation, with identified strategies to support clinicians with implementation. Further research is needed on long-term outcomes.
Introduction
Stroke is a leading cause of disability worldwide, with an estimated 15 million cases annually. 1 Guidelines for stroke rehabilitation emphasise the importance of early, intensive, task-specific therapy to optimise recovery. The Australian and New Zealand Living Clinical Guidelines for Stroke Management recommend continuous engagement in rehabilitation activities through independent and semi-supervised exercises. 2 Despite this, stroke survivors face prolonged periods of inactivity3,4 with limited opportunities for engagement in meaningful tasks beyond scheduled therapies. 5 Prolonged periods of immobility can lead to a decline in physical function, increased risk of complications and delayed recovery. 6 Importantly, early and sustained engagement in rehabilitation can lead to better outcomes in functional abilities and a reduced need for long-term care. 7 Given the ongoing pressures on healthcare services, innovative strategies are needed to bridge the gap between recommended and current practice.
Self-directed or caregiver-assisted therapy is a promising approach to reducing inactivity outside structured therapy sessions 8 significantly increasing overall exercise dosage in inpatient stroke rehabilitation.9,10 Promoting self-directed therapy may support independent practice, allowing therapists to allocate resources more efficiently. 11 The success of self-directed or caregiver-assisted programmes depends on numerous factors, including the availability of appropriate supports for engagement. 12 Current resources to support self-directed therapy are ineffective and other approaches are needed. 13
The growing use of technology-based tools offers clinicians working in inpatient rehabilitation an innovative way 14 to support stroke survivors, and their caregivers, to better engage in self-directed activities. Technology-based interventions may be tailored to individual abilities and preferences, are able to be personalised 15 and can be made to be appropriately challenging and relevant to individual users.16,17 Whilst there is emerging evidence for the use of technology-based interventions in stroke, 18 there is no synthesised evidence on feasibility, acceptability and effectiveness of using such tools in an inpatient setting after stroke.
The aim of this scoping review is to examine what is known about the use of self-directed, and caregiver-assisted, technology-based interventions to engage in self-directed, or caregiver-assisted activity in an inpatient setting after stroke. Specifically, we aim to explore:
Current approaches on research design and types of technology-based interventions which are being used in inpatient rehabilitation settings after stroke. What is known about acceptability, feasibility and effectiveness of self-directed or caregiver-assisted technology-based interventions for stroke survivors in an inpatient setting. What are the known barriers and enablers to the use of technology-based interventions, from a patient, caregiver and/or clinician perspective, mapped to the Capability, Opportunity and Motivation Behaviour (COM-B) change framework.
Methods and materials
We applied the five stages of Arksey and O’Malley's methodological framework in this scoping review, which include identifying the research question, identifying relevant studies, study selection, charting the data and collating and reporting the results.19,20 We followed the Preferred Reporting Items for Systematic Reviews extension for Scoping Reviews (PRISMA-ScR) reporting guideline. 21 Our scoping review was registered with Open Science Framework (https://osf.io/prq3e/files/osfstorage/679983be4ef5cd4daf62d164).
A preliminary search of MEDLINE, the Cochrane Database of Systematic Reviews, PROSPERO and Open Science Framework was conducted to check that no systematic or scoping reviews on our topic were published, or in progress, prior to commencing this review. We then searched MEDLINE (Ovid), Embase (Ovid) and CINAHL from inception to October 2024. This was updated in December 2025 to capture newly published studies before finalising the review. Search terms were established by members of the research team with assistance from a health research librarian. Key terms were stroke, inpatient rehabilitation, self-directed (or caregiver-assisted), digital interventions and technology. Additionally, to reduce the risk of missing any relevant literature, a basic search using the above keywords was conducted in Google Scholar, with the first 100 articles screened for relevance. An example of a full search strategy for MEDLINE (Ovid) can be found in Supplemental File S1.
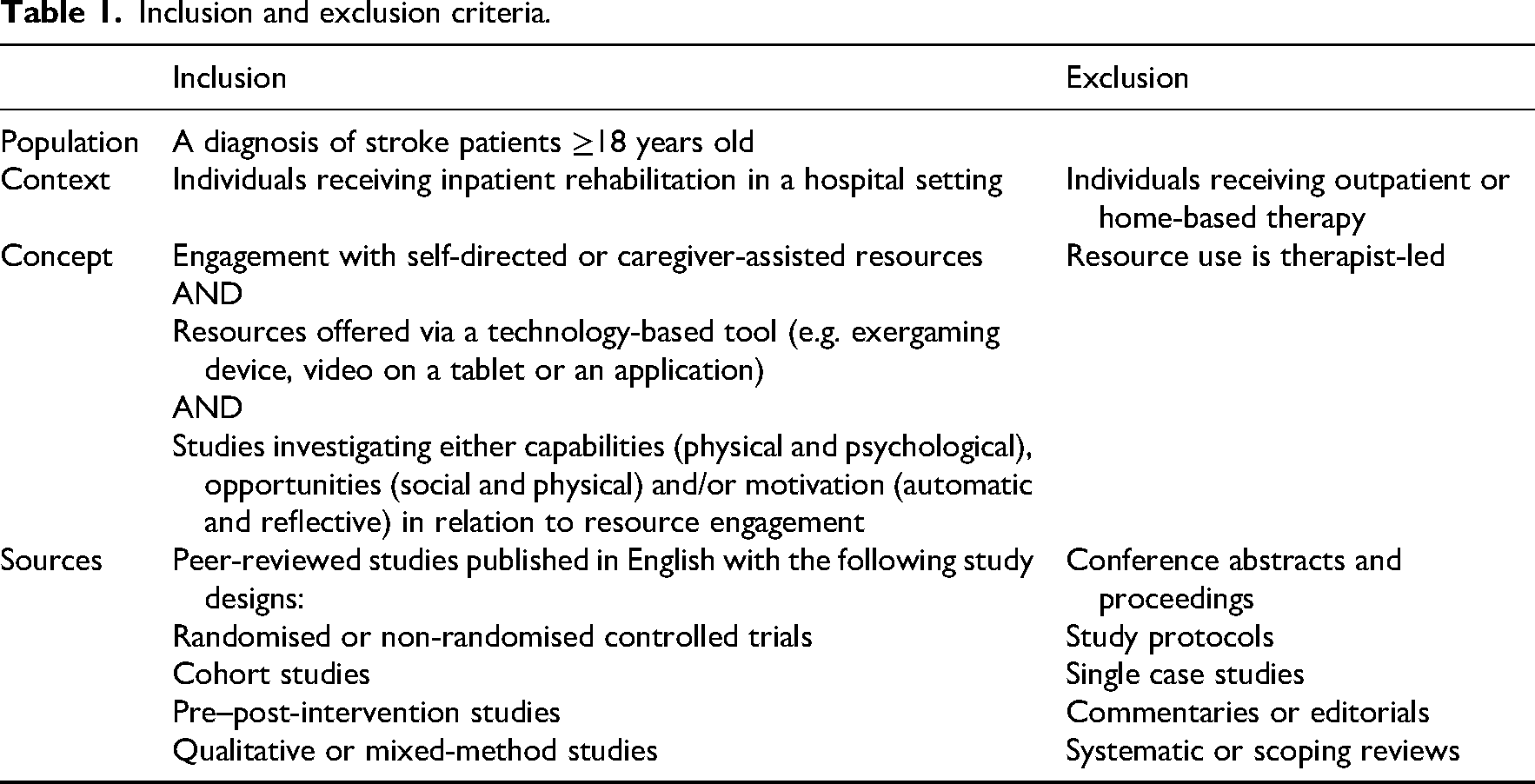
To be eligible for inclusion, participants in the included studies needed to be adults receiving inpatient rehabilitation after stroke and be exposed to self-directed or caregiver-assisted technology-based interventions examining either capabilities, opportunities or motivation for engagement (Table 1). Titles and abstracts were imported into Covidence 22 via EndNote 23 and duplicates were removed. The research team piloted the eligibility criteria on a sample of 100 papers and met to resolve any ambiguities. Titles and abstracts were screened independently by two authors (DP, JRAJ, SA, LJ, PYL and KJB). Similarly, all full texts were reviewed by two authors (DP and KJB). All conflicts were resolved through discussion. Reference lists of all the included studies were screened by another author (LJ).
Inclusion and exclusion criteria.
Quality of the included randomised controlled trials was appraised using the 11-item (10-point) Physiotherapy Evidence Database (PEDro) scale, 24 which evaluates internal and external validity of randomised controlled trials. The scale has strong convergent and construct validity 25 and moderate inter-rater reliability. Because blinding of participants and therapists is often not feasible in exercise trials, a maximum PEDro score of 8/10 is considered high quality. 26 Studies scoring 6 to 8 on the PEDro scale were categorised as good quality, 4 to 5 as fair and 0 to 3 as poor. 27 Quality of observational, cohort or feasibility trials was appraised using the Critical Appraisal Skills Programme checklist. 28 This checklist is widely used for assessing qualitative research, with a grading system ranging from 0 to 10 based on 10 methodological questions. 29 Studies with a quality score of 9 to 10 were categorised as high quality, 7.5 to 8.9 as moderate, or less than 7.5 as low. 30
A customised data extraction form was developed and piloted. Extracted data included study design, and methodology, country of the study, participant characteristics, description of the intervention, outcome measures, key findings and future directions relevant to the review questions. Data were extracted by one reviewer (DP) and independently cross-checked by another (SA or PYL). Any discrepancies or disagreements were resolved through discussion, or by a third reviewer (KJB). Analysis involved descriptive statistics to summarise study characteristics and basic coding to categorise findings related to acceptability, adherence, feasibility and effectiveness of technology-based interventions.
We defined acceptability as participants’ affective attitude towards technology-based interventions, their usage intentions (e.g. willingness to engage with the tool), and their satisfaction after having engaged with the tool. 31 Adherence was defined as actual usage (e.g. frequent interaction with the tool). Feasibility was defined as rates of recruiting users to engage with the technology-based intervention, level of assistance needed and safety considerations. 32 Finally, effectiveness was defined as the extent to which engaging with a technology-based intervention produced a beneficial outcome under typical, real-world conditions. 33 Data on barriers and enablers were deductively mapped to the six sub-domains of the COM-B change framework. 34 The COM-B framework was chosen because it provides a clear, theory-based way to identify the capability, opportunity and motivation factors that influence uptake and ongoing use of technology-based interventions. Importantly, COM-B directly links behavioural barriers and enablers to intervention functions and behaviour change techniques, supporting both intervention design and implementation planning. This makes it a practical and actionable framework for translating research findings into real-world implementation strategies.
Results
The search strategy yielded 8797 studies and was reduced to 4750 after duplicates were removed (Figure 1). After screening titles, abstracts and reference lists, 100 full texts were retrieved. Of these, 80 were excluded based on eligibility criteria. Common reasons for exclusion were that interventions were not self-directed (n = 62), participants were not inpatients (n = 10), interventions were not technology-based (n = 5), papers were not published in English (n = 2) and participants were not stroke survivors (n = 1). Twenty papers from 18 unique studies, representing 19 datasets, were included in our review.
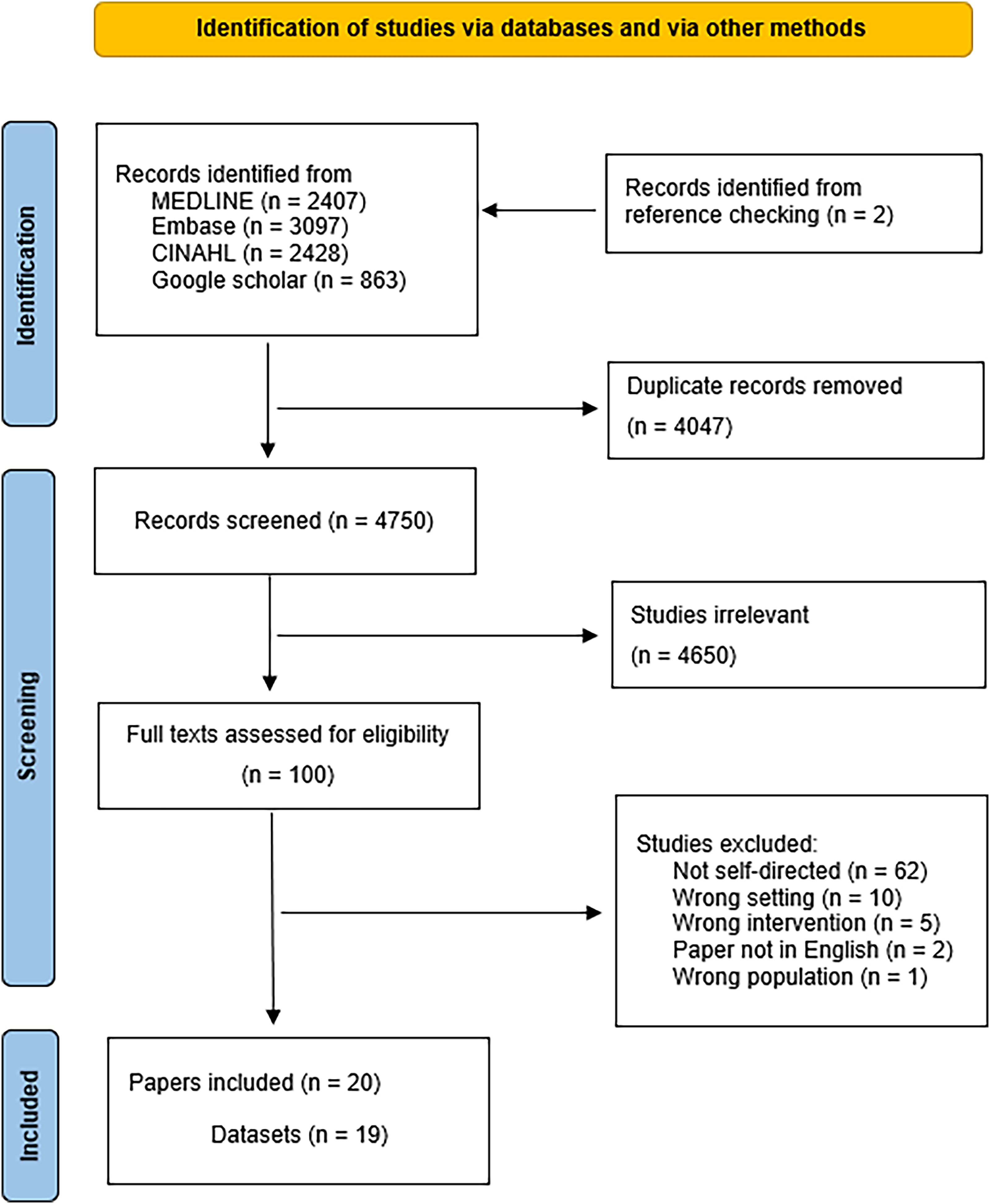
Study selection flow chart.
Study characteristics are detailed in Table 2. The review included 18 studies (20 papers): 10 pilot randomised controlled trials,35–44 6 feasibility studies,8,45–49 1 non-randomised trial 18 and 1 observational study. 50 All studies were published in the last 12 years with 14 out of 18 (78%) studies undertaken in the last 5 years. Studies spanned 13 high-income countries, with the United Kingdom (n = 4), Australia (n = 2), Korea (n = 2) and Netherlands (n = 2) most represented. Intervention aims included improving upper limb function, language impairment (in the presence of aphasia), functional recovery (physical and cognitive), exploring the impact of pre-commitment on levels of engagement and understanding patient preferences relating to technology-based interventions. Most studies evaluated interventions targeting stroke survivors alone (n = 16), with a smaller number looking at interventions with patient–caregiver dyads (n = 2). Intervention durations ranged from 2 to 14 weeks. Technology-based tools were varied and included upper limb exergaming or robotic devices (n = 4)8,38,45,48 and tablet/smartphone applications (n = 14).18,35–37,39–44,46,47,49,50 Data in this review represents the experience of 1081 participants. Age was reported using various summary measures, with the average of reported mean ages being 68 years (range 58–74). Sex of participants was reported in 17 (94%) studies, and most participants were male (56%). Other baseline characteristics included stroke type and severity, time since stroke, functional status and prior technology use (see Table 2).
Characteristics of the included studies.

AI: artificial intelligence; FIM: functional independence measure; FMA-UE: Fugl-Meyer Assessment-upper extremity; IQR: inter-quartile range; LL; lower limb; MoCA: Montreal Cognitive Assessment; mRS: modified Rankin Scale; NIHSS: National Institutes of Health Stroke Scale; OT: occupational therapy; PC: personal computer; PT; physiotherapy; STAPP: speech therapy app; TV: television; UL: upper limb.
Quality appraisal
Using the PEDro Scale, most randomised controlled trials were rated good (n = 6)38,40–44 or fair (n = 3)35,37,39 in quality, with one assessed as poor quality 36 (Supplemental File S2). The non-randomised, feasibility and observational studies were either rated as high (n = 3)8,36,49 or moderate (n = 6)8,18,42,43,45,48 in quality, using the Critical Appraisal Skills Programme checklist (Supplemental File S3).
Outcome measures
Acceptability outcomes were reported in 12 (63%) studies8,36,38,40,43,45–51 (Table 3). Measures for acceptability varied across the included studies, with the most common concepts pertaining to participants’ and caregivers’ perceived usefulness, ease of use and satisfaction. Most participants perceived technology-based tools to be convenient, usable and acceptable. In one study, 49 participants preferred a technology-based format over paper alone, as it was perceived to be more engaging and meaningful. Adherence to the intervention protocol was reported in eight (67%) studies43–48,50,51 and varied from 42% to 83%. Feasibility outcomes were reported in 12 (63%) studies.8,36,38,40,43–48,50,51 Recruitment rates, reported in eight studies (67%), ranged from 38% to 81%. Retention rates, reported in six studies (50%), were generally very high and commonly attributed to daily contact and encouragement from treating therapists. Levels of assistance required for participants to be able to interact with their technology-based tool were reported in five (42%) studies. In three of those studies,36,38,45 only minimal assistance was needed by enrolled participants, whereas in the other two studies,8,50 half of their participants required at least some level of assistance to engage with their technology-based tool. One study 50 reported that limited prior experience with the use of computers or tablets, as well as moderate aphasia, was negatively correlated with participants’ level of independence. However, in another study 45 participants felt well supported in using technology-based tools even without prior experience. Safety was reported in eight (67%) studies,3,8,40,43–46,48 with seven (88%) reporting no adverse events. In one study, 44 there were a significant number of participants who withdrew their consent, but this did not appear to be related to safety concerns pertaining to the intervention. Three episodes of device failure were reported in another study, 8 but these were rectified in a timely manner by a member of the research team.
Acceptability and feasibility.
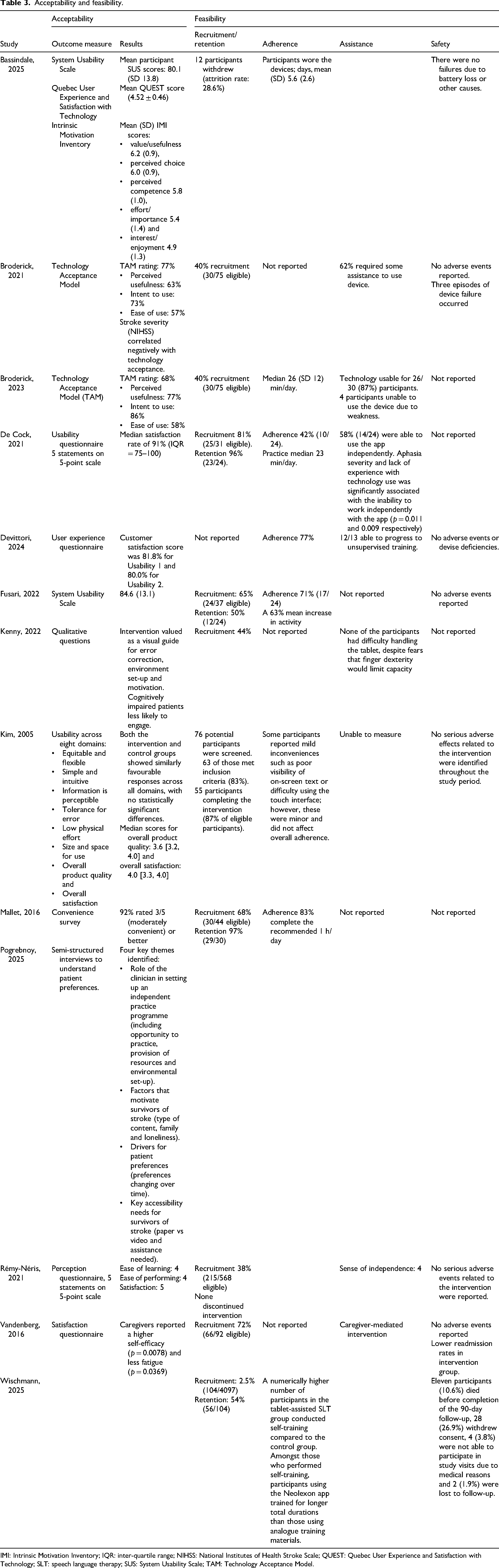
IMI: Intrinsic Motivation Inventory; IQR: inter-quartile range; NIHSS: National Institutes of Health Stroke Scale; QUEST: Quebec User Experience and Satisfaction with Technology; SLT: speech language therapy; SUS: System Usability Scale; TAM: Technology Acceptance Model.
Eleven studies (58%) evaluated the effectiveness of a technology-based intervention (Table 4). The most common outcome measuring effectiveness was the completion of self-directed activity outside of therapy (measured in minutes). Other outcomes included stroke-related disability (modified Rankin Scale, Functional Independence Measure, National Institutes of Health Stroke Scale and Stroke Impact Scale), mobility (Timed Up and Go Test), activities of daily living (modified Barthel index), upper limb function (Fugl-Meyer Assessment–Upper Extremity, Action Research Arm Test), self-efficacy (Self-Efficacy Scale), aphasia severity (Bielefelder Aphasia Screening-Rehabilitation Version) and balance (Berg Balance Scale, Functional Reach Test). Effectiveness for caregivers was measured using the Caregiver Strain Index and Caregiver Quality of Life Scale. 41 Seven (64%) studies8,18,35,37,40,42,45 reported significant differences in favour of the intervention groups whilst four (36%) studies38,41,43,44 found no significant between-group differences.
Effectiveness.
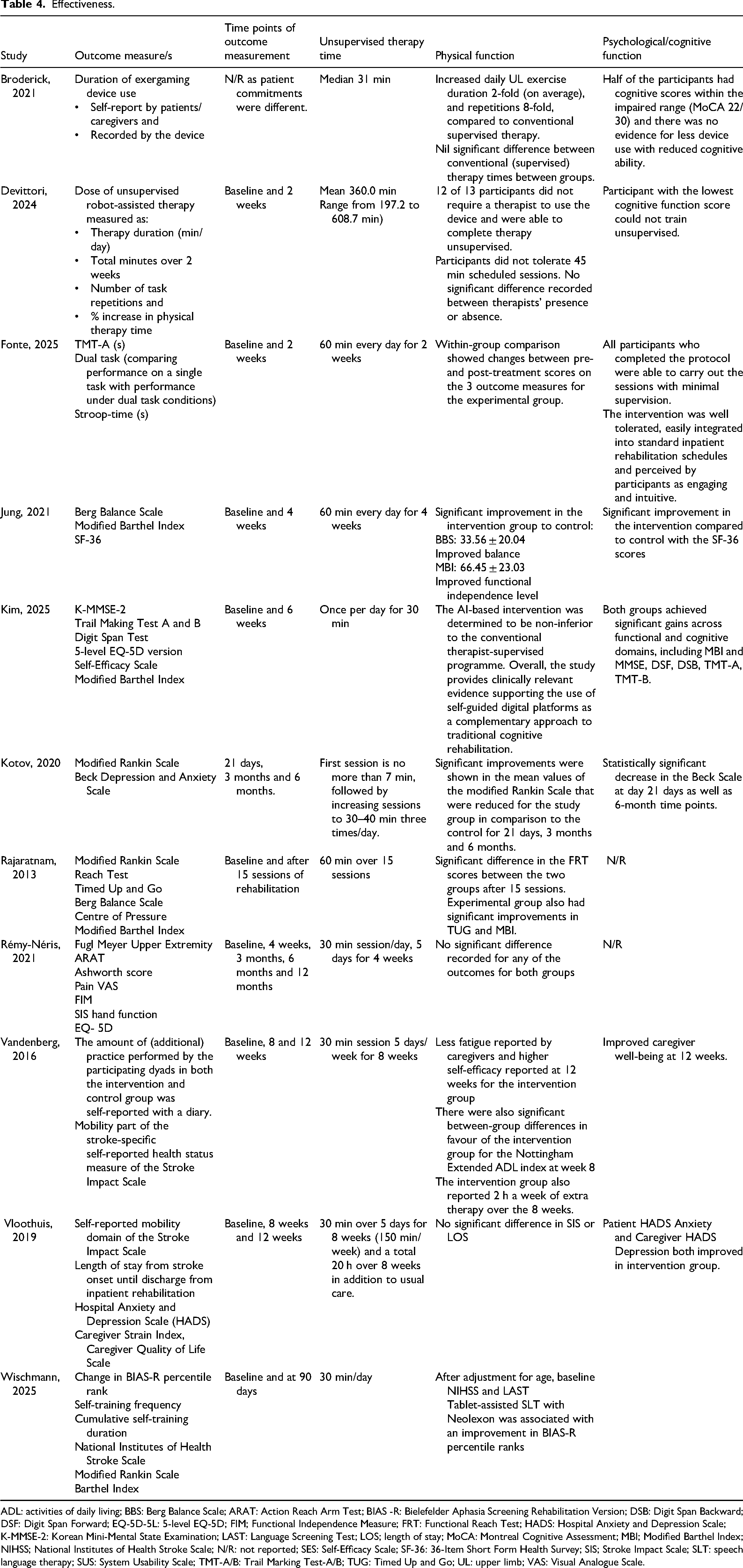
ADL: activities of daily living; BBS: Berg Balance Scale; ARAT: Action Reach Arm Test; BIAS -R: Bielefelder Aphasia Screening Rehabilitation Version; DSB: Digit Span Backward; DSF: Digit Span Forward; EQ-5D-5L: 5-level EQ-5D; FIM; Functional Independence Measure; FRT: Functional Reach Test; HADS: Hospital Anxiety and Depression Scale; K-MMSE-2: Korean Mini-Mental State Examination; LAST: Language Screening Test; LOS; length of stay; MoCA: Montreal Cognitive Assessment; MBI; Modified Barthel Index; NIHSS; National Institutes of Health Stroke Scale; N/R: not reported; SES: Self-Efficacy Scale; SF-36: 36-Item Short Form Health Survey; SIS; Stroke Impact Scale; SLT: speech language therapy; SUS: System Usability Scale; TMT-A/B: Trail Marking Test-A/B; TUG: Timed Up and Go; UL: upper limb; VAS: Visual Analogue Scale.
Barriers and enablers
Barriers and enablers were mapped to the three domains of the COM-B framework (Figure 2).
Barriers to physical capability were identified as severity of stroke, poor literacy in technology use as well as significant cognitive, motor and visual deficits. Reported enablers were optimising the technology-based intervention to the intended user, family involvement, education and patients having an opportunity to familiarise themselves with the technology-based tool before being expected to manage the tool independently. Barriers to psychological capability were participant low mood and not understanding the purpose of self-directed practice. Enablers were regular contact with prescribing clinicians, education for caregivers and patients and availability of caregivers. Barriers to physical opportunity included the inability of patients to manage navigation of the technology-based tool due to stroke-related impairments. Enablers were a well set-up room, availability of required equipment and reliable technical support. Barriers to social opportunity were set-up costs, a lack of multi-lingual resources and a lack of external encouragement whilst enablers were structured clinician and family support and shorter sessions. Barriers to reflective motivation were fatigue and not having clear targets for expected activity outside of therapy time, whilst enablers were having access to motivating content, providing patients with choice, customisation of the technology-based tool and offering training opportunities to caregivers and patients. Barriers to automatic motivation were being prescribed repetitive tasks and not understanding the purpose of self-directed therapy, and enablers were scheduling self-management on the timetable, clarity in instructions and group activity.
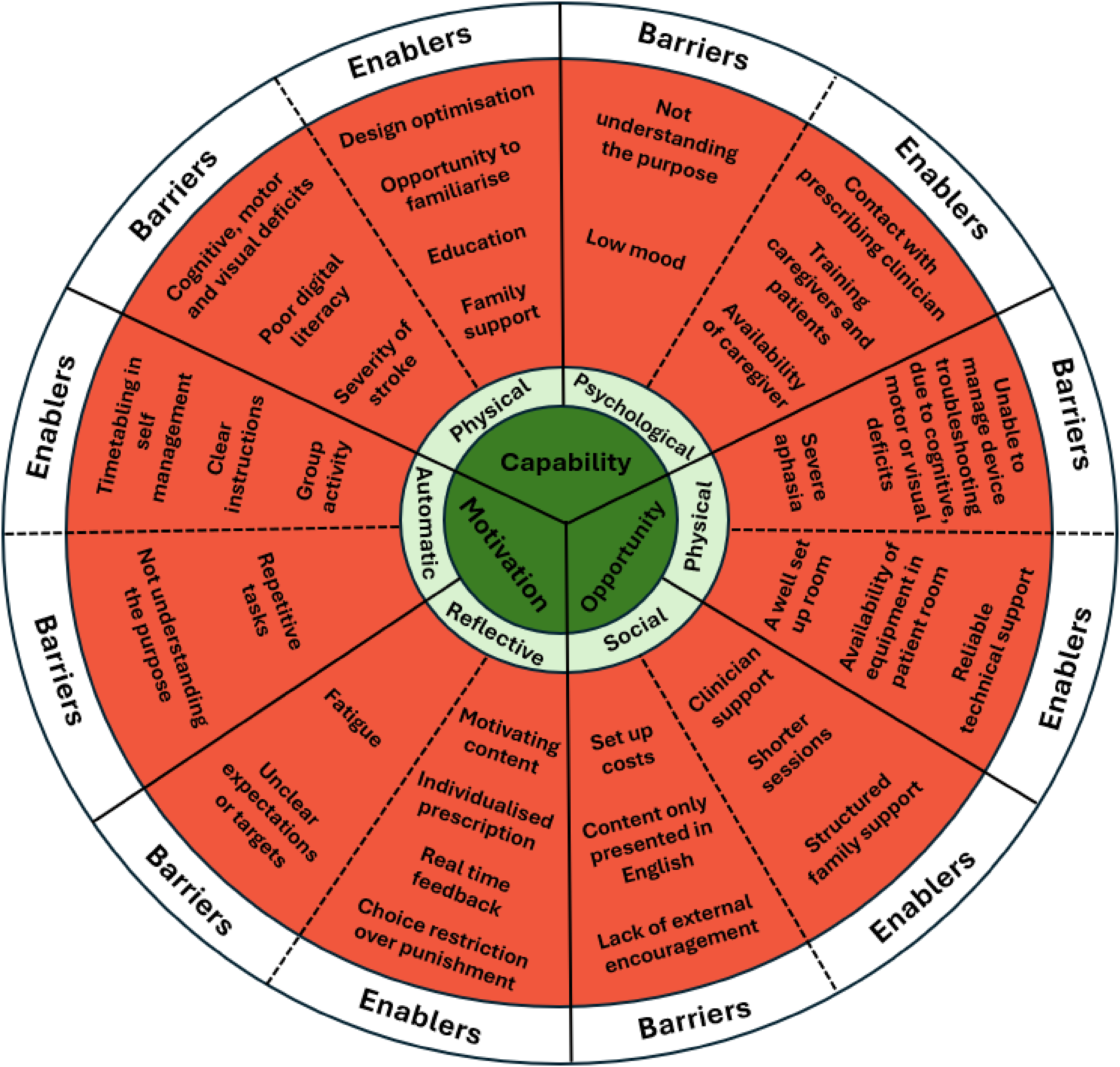
Data mapped to the COM-B framework. 34 Capability refers to whether an individual has the knowledge, skills and abilities to engage in a behaviour. Domain of capability is separated into physical and psychological. Psychological capability includes mental state, knowledge and skill, whereas physical capability is when an individual feels physically capable of performing a behaviour or achieving an outcome. Opportunity refers to external factors that make the execution of a behaviour possible. Domain of opportunity is broken up into social and physical. Physical opportunity describes opportunities provided by the physical environment, whereas social opportunity is opportunities provided through a social setting. Motivation refers to internal processes that influence decision making and behaviour. Domain of motivation is broken up into automatic and reflective. Reflective motivation describes the reflective process involved in making plans, whereas automatic motivation more describes impulses and inhibitions. COM-B: Capability, Opportunity, Motivation and Behaviour.
Discussion
Our findings, derived from 18 studies (19 datasets), suggest that it is feasible, acceptable and safe to use technology-based interventions for most individuals undergoing inpatient stroke rehabilitation. It appears that technology-based interventions have the capacity to successfully promote increased patient activity outside of structured therapy time. Key enablers were clinician support during set-up, opportunities for practice and structured scheduling. Barriers included participant cognitive or physical limitations, fatigue and low mood.
Engaging in self-directed programmes outside of structured therapy time can address the known gap that exists between recommended levels of activity and the known inactivity amongst survivors of stroke undergoing inpatient rehabilitation. 8 Literature on existing resources, aimed at supporting patients to increase their activity levels during inpatient rehabilitation, often provided in the form of paper-based prompts or verbal instructions, suggests that current practice is ineffective. 52 Our review suggests that technology-based interventions have the potential to more effectively support increased activity outside of therapy time when compared to usual care, with 7 out of 11 included studies reporting superior outcomes for participants who engaged with technology-based interventions. These findings align with emerging literature supporting the role of technology in increasing rehabilitation engagement.53–55
Clinicians who wish to prescribe the use of technology-based tools during inpatient rehabilitation need to consider patient, prescribing clinicians and environmental barriers as part of their prescription. Findings from our review highlight that technology-based interventions, which are intended for use by survivors of stroke, need to be designed to consider stroke-specific impairments which are known to influence engagement. Accessible design needs to not only consider physical impairments but also take into account the impact of visual and memory deficits as well as the impact of altered cognition and fatigue. Content needs to be motivating, and user feedback needs to be provided regularly to promote sustained engagement. Finally, environmental factors, technical support requirements and safety considerations need to be carefully planned for during programme set-up. Clinicians play a critical role in helping patients overcome barriers to engagement when they initially prescribe technology-based interventions to their patients. Clinicians are encouraged to reflect on their own practice and consider if they are appropriately supporting their patients in setting up effective self-directed programmes when they are initially prescribed and subsequently reviewed during the rehabilitation episode. Findings from this review should give clinicians the confidence that prescribing technology-based interventions to survivors of stroke undergoing inpatient rehabilitation can effectively promote increased self-directed (or caregiver-assisted) activity.
Early initiation of self-directed rehabilitation is known to be beneficial for patients who require inpatient rehabilitation after stroke. 56 Findings from our review suggest that technology-based interventions are acceptable and feasible for most survivors of stroke undergoing inpatient rehabilitation. This is in keeping with prior work in relation to self-directed interventions in an inpatient rehabilitation setting but existing literature is not specific to stroke or to technology-based tools which can be used in a self-directed manner. 12 Most participants in studies included in our review found technology-based tools easy to use, they perceived the interventions to be useful, and reported feeling satisfied with their experience of interacting with their technology-based tool. Findings from this review suggest that patients with aphasia or with limited technology exposure prior to their stroke are still able to benefit from being prescribed a technology-based intervention but may require additional education and support from their clinician, or caregiver, to help build their capability. It should be noted that in two studies,8,44 stroke severity correlated negatively with technology acceptance and in another, 50 aphasia severity and lack of experience with technology use was significantly, and negatively, associated with self-directed engagement. From this, a reasonable hypothesis is that whilst technology-based tools appear to be acceptable to most survivors of stroke undergoing inpatient rehabilitation, they may only be a feasible option, for self-directed use, by patients with mild-to-moderate physical impairment, mild-to-moderate aphasia and for patients who have a caregiver available for support.
We believe future research should focus on evaluating the long-term impact of technology-based interventions on the physical, cognitive and social recovery of survivors of stroke including health-related quality of life and participation in activities of daily living. It is important to further explore which types of technology-based tools and approaches are most acceptable and effective in the inpatient rehabilitation setting for survivors of stroke and their caregivers. Finally, literature on applicability and acceptability of technology-based interventions in diverse healthcare settings and with culturally and linguistically diverse patient cohorts remains sparse and should be a focus of future research.
A key strength of this review is our comprehensive search strategy, increasing the likelihood that all relevant published work, in this emerging field, was captured. The inclusion of studies using a variety of technology-based interventions and involving participants with a range of functional abilities increases the generalisability of our findings. However, the total number of studies included was relatively small (n = 18), and variation in study design as well as the types of technology-based tools used limited the ability to draw strong conclusions. Only studies published in English were included, which may limit the international relevance of this review. Furthermore, all studies took place in high-income countries; therefore, findings from this review may not be translatable to other settings where access to technology and literacy in technology use may differ.
Clinical messages
Technology-based interventions are acceptable, feasible and safe during inpatient rehabilitation after stroke.
Some barriers to engagement include cognitive impairment, severe aphasia, low mood, not understanding the purpose and insufficient support.
Enablers include appropriate training, targeted scheduling and motivating content with real-time feedback.
Further research must investigate their effects.
Supplemental Material
sj-docx-1-cre-10.1177_02692155261428703 - Supplemental material for Self-directed and caregiver-assisted technology-based interventions in inpatient stroke rehabilitation: A scoping review
Supplemental material, sj-docx-1-cre-10.1177_02692155261428703 for Self-directed and caregiver-assisted technology-based interventions in inpatient stroke rehabilitation: A scoping review by Dina Pogrebnoy, Jennifer RA Jones, Shahad Alsawaf, Lourdes Joseph, Pak Yin Lau and Kelly J Bower in Clinical Rehabilitation
Supplemental Material
sj-docx-2-cre-10.1177_02692155261428703 - Supplemental material for Self-directed and caregiver-assisted technology-based interventions in inpatient stroke rehabilitation: A scoping review
Supplemental material, sj-docx-2-cre-10.1177_02692155261428703 for Self-directed and caregiver-assisted technology-based interventions in inpatient stroke rehabilitation: A scoping review by Dina Pogrebnoy, Jennifer RA Jones, Shahad Alsawaf, Lourdes Joseph, Pak Yin Lau and Kelly J Bower in Clinical Rehabilitation
Supplemental Material
sj-docx-3-cre-10.1177_02692155261428703 - Supplemental material for Self-directed and caregiver-assisted technology-based interventions in inpatient stroke rehabilitation: A scoping review
Supplemental material, sj-docx-3-cre-10.1177_02692155261428703 for Self-directed and caregiver-assisted technology-based interventions in inpatient stroke rehabilitation: A scoping review by Dina Pogrebnoy, Jennifer RA Jones, Shahad Alsawaf, Lourdes Joseph, Pak Yin Lau and Kelly J Bower in Clinical Rehabilitation
Footnotes
Acknowledgements
We would like to acknowledge the University of Melbourne Doctor of Physiotherapy students, Zac McCosh, Amen Kassa and Chelsea Lee, who contributed to the early stages of this review as part of their Research Capstone subject.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: We acknowledge that a qualitative study included in this scoping review is co-authored by an author of this review. Data extraction from this qualitative study was completed by two independent authors to reduce the risk of bias.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.