
Abstract
Objective
To systematically evaluate the effects of cardiopulmonary exercise test-derived, tailored pulmonary rehabilitation on cardiopulmonary outcomes in individuals with interstitial lung diseases.
Data sources
MEDLINE, Embase, CINAHL Ultimate, SPORTDiscus, CENTRAL, and the Cochrane Library were searched from inception up to 4th September 2025. Reference lists of the included studies were hand-searched for additional sources.
Review methods
Reporting followed PRISMA 2020 guidelines. Studies of any design published in English and involving participants with interstitial lung disease were eligible. Due to intervention heterogeneity, meta-analysis was not conducted.
Results
Eleven studies comprising 321 participants were included, with sample sizes ranging from 1 to 52. Designs encompassed single-cohort interventions (n = 4), comparative interventional studies (n = 3), randomised controlled trials (n = 3), and one case report. Pulmonary rehabilitation interventions included aerobic, interval, and resistance training, delivered over study durations ranging from 4 weeks to 4.5 years. Cardiopulmonary exercise testing outcomes included peak oxygen uptake; peak work rate; peak minute ventilation; maximum heart rate, and rate of perceived exertion. All studies assessing peak oxygen uptake and peak work rate reported improvements. Peak minute ventilation improvements were reported in six of seven studies. No serious adverse events were reported.
Conclusion
Tailored pulmonary rehabilitation via cardiopulmonary exercise test metrics appears to enhance peak oxygen uptake and peak work rate in individuals with interstitial lung disease. Findings support its potential efficacy; however, future research should prioritise standardised methods, consistent reporting, and longer follow-up durations to inform clinical practice.
Introduction
Interstitial lung diseases are a heterogeneous group of ∼200 chronic lung conditions, which are associated with lung parenchymal fibrosis and/or interstitial inflammation. 1 Unfortunately, these chronic conditions cannot be cured, and people with idiopathic pulmonary fibrosis, one of the most common subtypes of interstitial lung disease, have a median survival of 2–3 years from diagnosis. 2 Therefore, maintaining lung function, physical activity and quality of life for people with interstitial lung disease is a key focus. 3
A joint statement produced by the American Thoracic Society and European Respiratory Society recommends pulmonary rehabilitation to enhance cardiorespiratory health and quality of life outcomes for people with interstitial lung diseases. 4 Thus, the National Health Service, alongside the National Respiratory Audit Programme aim to improve pulmonary rehabilitation services in the United Kingdom. 5 The 2023 British Thoracic Society ‘Clinical Statement on Pulmonary Rehabilitation’ states validated exercise tests should be conducted to inform tailored exercise prescription. 6 A systematic review from Barratt et al. 7 highlighted the value of cardiopulmonary exercise testing (CPET) within interstitial lung disease care. Moreover, CPET is valid and reproducible in interstitial lung disease,8,9 supporting clinical implementation.
CPET is the gold standard for assessing exercise intolerance in chronic pulmonary conditions. 10 It provides integrated evaluation of cardiac, respiratory, and muscular function, and identifies limiting factors such as breathlessness and low motivation.11,12 In clinical settings, CPET can quantify aerobic capacity13–15 and guide tailored exercise prescription.16,17 Despite established pulmonary rehabilitation guidance in respiratory diseases, 18 no frameworks exist for interstitial lung diseases. Therefore, the James Lind Alliance ranked exercise optimisation for pulmonary fibrosis a top 10 research priority. 19
The challenge is exercise tolerance has been shown to be markedly reduced in interstitial lung diseases, 20 compounded by multisystem pathophysiological impairments, 11 which impacts the applicability of generic pulmonary rehabilitation. 21 Furthermore, field tests such as the 6-min walk distance and incremental shuttle walk test may not provide the physiological detail needed to tailor exercise in this population. 15 In contrast, CPET quantifies real-time physiological responses, enabling threshold-based exercise prescription using metrics like maximal heart rate, peak oxygen uptake, and peak work rate.11,22
To date, no systematic reviews have evaluated how CPET-derived measures can guide personalised rehabilitation for interstitial lung diseases. This review addresses that gap, identifying relevant parameters and intensities, and assessing their impact on cardiorespiratory health.
Methods
This systematic review was conducted and reported using the updated PRISMA 2020 guideline. 23 The protocol was registered on PROSPERO (CRD: 42024543174) on 7th May 2024, and a full protocol had published previously. 24 All full-text articles were obtained and screened for eligibility against the inclusion and exclusion criteria represented in Table 1.
Inclusion and exclusion criteria.
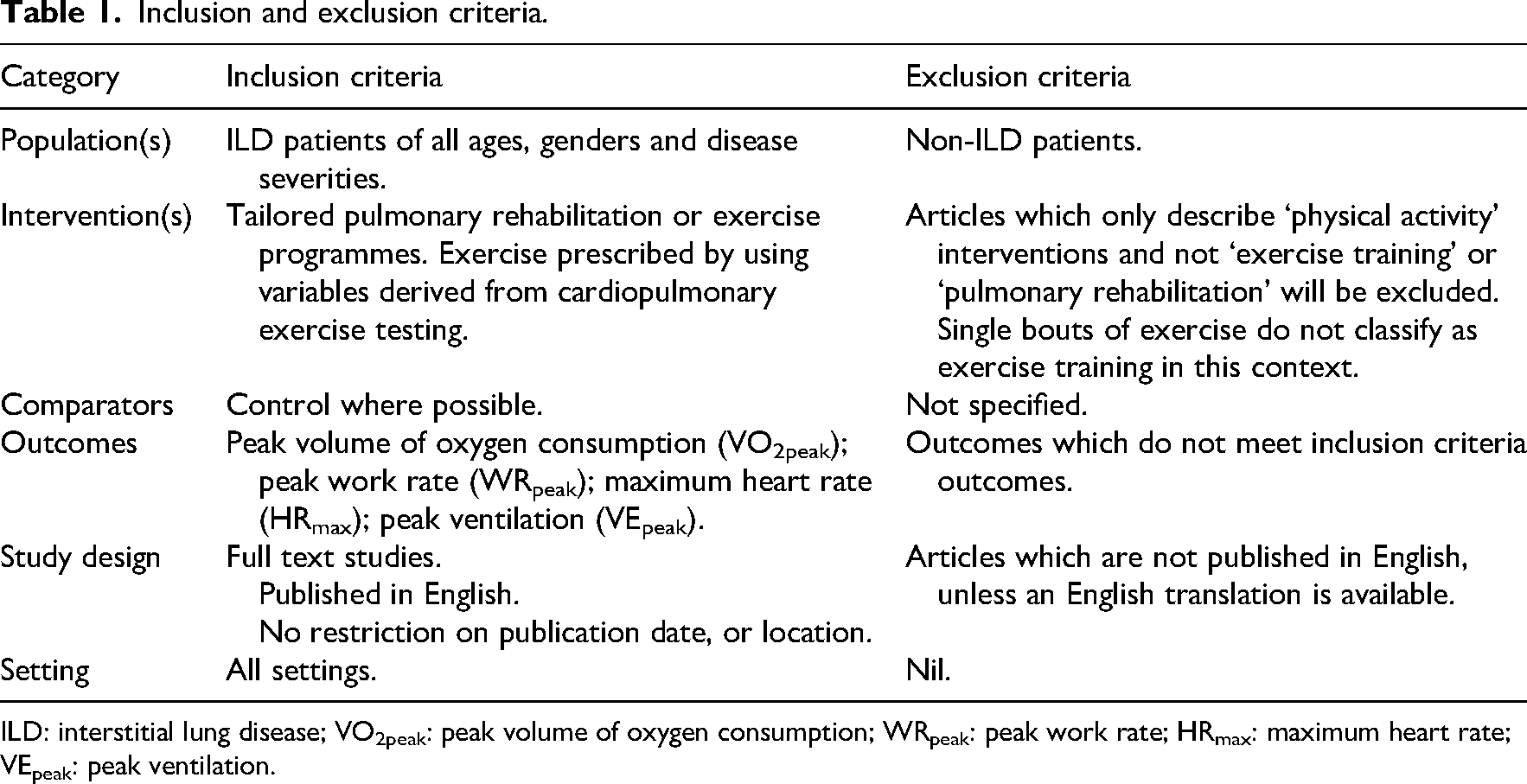
ILD: interstitial lung disease; VO2peak: peak volume of oxygen consumption; WRpeak: peak work rate; HRmax: maximum heart rate; VEpeak: peak ventilation.
Electronic searches were conducted using Ovid®, incorporating Ovid MEDLINE® and Ovid Embase™, EBSCO databases CINAHL Ultimate and SPORTDiscus, CENTRAL and the Cochrane Library. Searches were conducted in two phases, firstly from inception up to January 2025, and secondly from January 2025 to September 2025 as an update following initial peer review. The reference lists of the included studies and review articles were also reviewed to identify any potentially relevant studies not identified through the search process. No grey literature, theses, or dissertations were included. The full strategy is available online. 25
Initial search results obtained using the search strategy described above were screened for eligibility and inclusion according to title and abstract. Independent data extraction was performed using customised Microsoft Excel™ data extraction forms developed specifically for the study. The search results in the first search were double-screened by BB and TL-K, with OWT as a third reviewer if needed. In the second post-review search update, these were double-screened by BB and OWT.
Quality assessment of the included studies was performed by two reviewers (BB and SG) using the critical appraisal skills programme checklists for single-cohort studies 26 and randomised controlled studies. 27 A third reviewer (OWT) was available if needed. The critical appraisal skills programme checklist items were assigned a numerical value of ‘1’ for ‘Yes’, if well described, and a value of ‘0’ for ‘Can’t Tell’ and ‘No’, if inadequate.28,29 The consensus on exercise reporting template 30 was utilised to assess the reporting and delivery of exercise interventions within the included studies. Assessment was performed by two reviewers (BB and SG), with a third reviewer (OWT) available if required.
The results of the included studies were synthesised based on the reported interventions and outcomes. Meta-analysis was not performed due to the wide heterogeneity of study design and interventions within the included studies, but also the lack of standardisation in outcomes. Therefore, the results are narratively synthesised based on the key findings of the outcome measures reported in the included studies.
There were some deviations from the published protocol to note. Firstly, the screening of all the included papers was due to be independent, with 10% double-screened by another member of the research team. However, it was decided to perform full double screening to enhance accuracy and reduce bias. Secondly, meta-analysis and assessment of evidence certainty were not performed due to widespread heterogeneity within the included studies. Thirdly, as formal data analyses were not performed, use of Review Manager 30 was not necessary. Outcome measures detailed in the protocol (e.g. volume of oxygen consumption at anaerobic threshold and rate of perceived exertion) were not detailed in main text, but are available in the Supplementary materials hosted on Open Science Framework. 25
Results
Study selection and characteristics
Electronic and hand searches identified 532 studies were suitable for inclusion screening. After assessing the articles against the inclusion criteria, 11 studies were included in the review (Figure 1), following good agreement (82%) in the initial double-screening process by BB and TL-K, before consensus (100%) was achieved via discussion. No additional articles were identified for inclusion in the second search phase, with 100% agreement between BB and OWT. Reasons for article exclusion are detailed in the Supplementary materials on Open Science Framework 25 and the selection process has been reported using a PRISMA flow diagram.
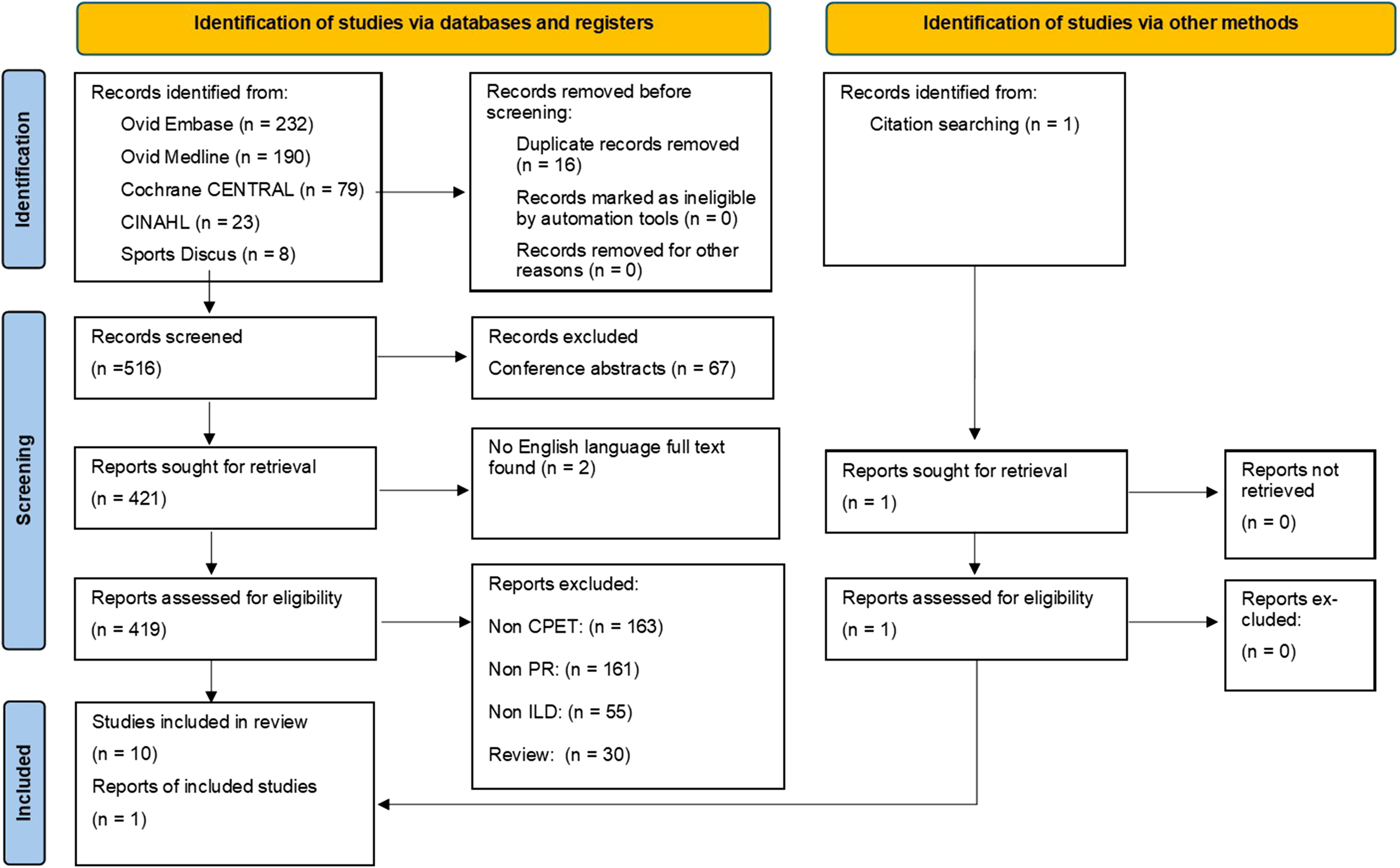
PRISMA flow chart. CINAHL: Cumulative Index to Nursing and Allied Health Literature; CPET: cardiopulmonary exercise test; PR: pulmonary rehabilitation; ILD: interstitial lung disease.
A summary of the included study characteristics is presented in Table 2. Study designs included four single-cohort intervention studies,31–34 three comparative interventional studies,35–37 three randomised controlled trials,38–40 and one case report. 41 Four studies did not use a control group.31,32,34,41 A control group of continued medical management was utilised in six studies.35–40 One study used an age- and sex-matched cohort of participants without a diagnosis of idiopathic pulmonary fibrosis as a control. 33 A control group consisting of study drop outs was formed in one study. 40
Study and participant characteristics.
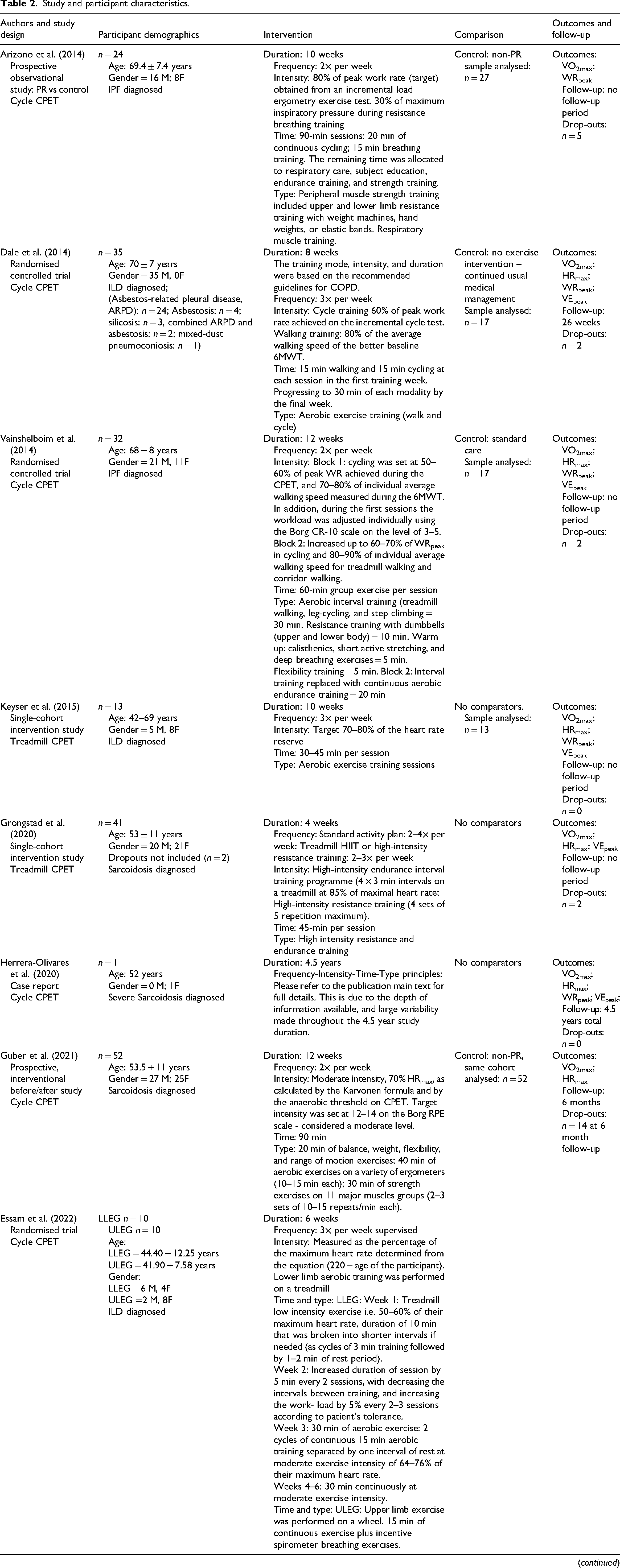
M: male; F: female; LLEG: lower limb exercise group; ULEG: upper limb exercise group; VO2max: maximal volume of oxygen consumption; WRpeak: peak work rate; HRmax: maximum heart rate (BPM); VEpeak: peak ventilation; AT: anaerobic threshold; HRR: heart rate reserve; CPET: cardiopulmonary exercise test; 6MWT: 6 min walk test; LAM: lymphangioleiomyomatosis; COPD: chronic obstructive pulmonary disease; Borg CR-10 scale: rate of perceived exertion 0–10 score; ILD: interstitial lung disease; HIIT: high intensity interval training.
Participant characteristics
The 11 included studies consisted of 321 participants in total, of which 168 subjects were male. Two studies recruited single-sex participants only.31,38 Participant age ranged from 36 to 80 years with sample sizes ranging from 1 41 to 52. 36 Participants were categorised into interstitial lung disease-subtypes, including: IPF33,35,37,39 (n = 4), sarcoidosis34,36,41 (n = 3), lymphangioleiomyomatosis 31 (n = 1), mixed- 32 (n = 1), fibrosing- 40 (n = 1), and dust-related interstitial lung disease 38 (n = 1).
Risk of bias
The overall critical appraisal skills programme quality of reporting score for the included single-cohort studies31–37 (n = 7) ranged from 8 to 12, with a mean score of 10 out of a possible maximum of 12 (Supplemental materials). The critical appraisal skills programme scores for the randomised controlled trials38–40 (n = 3) ranged from 7 to 10, with a mean score of 9 out of a possible maximum score of 11 (Supplemental materials). The most common reasons for a low critical appraisal skills programme score in the cohort studies were inadequate follow-up31–35 (n = 5) and inaccurate measure of exposure and outcome to minimise bias34,37 (n = 2). However, within the randomised controlled trials, low scores were most commonly found due to inadequate study methodology39,40 (n = 2).
Cardiopulmonary exercise testing
All studies performed cardiopulmonary exercise tests using either a cycle ergometer31,3336–39,41 (n = 7) or a treadmill32,34,35,40 (n = 4). The CPET protocols, as described by authors, included: incremental36,40,41 (n = 3), both incremental ramp and constant work-rate exercise test33,37 (n = 2), ramp 39 (n = 1), Balke 31 (n = 1), modified Bruce 35 (n = 1), modified Naughton 32 (n = 1), step 35 (n = 1), and symptom-limited and endurance cycle test 38 (n = 1).
No study confirmed a plateau of oxygen consumption or performed supramaximal exercise bout to confirm a maximal effort; the indexes for potential identification of maximal effort reported were minute-ventilation/oxygen uptake slope31,33,35,39,40 (n = 5), rate of perceived exertion31,35,36,38,41 (n = 5), and respiratory exchange ratio32,34,35,40 (n = 4). Therefore, use of the term ‘maximal oxygen uptake’ herein does not necessarily reflect a true maximal effort, but reflects individual authors interpretation and reporting. 42
Exercise prescription
The quality of exercise reporting within the included studies was assessed using the aforementioned, 16-item internationally endorsed consensus on exercise reporting template to strengthen the assessments of the included studies 30 (Supplemental materials). The overall consensus on exercise reporting template quality of exercise intervention reporting score for the included studies ranged from 6 36 to 18, 33 with a mean score of 14 out of a possible maximum of 19. The most common domains for a low consensus on exercise reporting template score within the included studies were inadequate description of participants baseline exercise experience31,3234–41 (e.g. beginner, intermediate, advanced, etc.) (n = 10), lack of detailed description for motivational strategies31,32,36,39,40 (n = 7), and poor description of non-exercise components31,33,36,40,41 (n = 5).
Exercise intervention duration ranged from 4 weeks 34 to 4.5 years, 41 with many of the included studies lasting 8–12 weeks.33,35,38,39 A total of n = 7 exercise programmes were supervised.32,33,35,3638–40 Four studies did not have a control group.31,32,34,41 The frequency of exercise ranged between 2× and 4× per week for all of the included studies. The initial time spent for each exercise session varied from 25 31 to 90 min.36,37 A progressive duration of total exercise was performed in three studies,31,38,40 therefore by the end of the studies patients were performing at least a total of 45 min exercise sessions in all studies. No warm up duration was reported in seven studies.31,33,34,36–38,40 A warm up was performed in two studies32,39 for a duration of 5 to 10 min, which was not classed as part of the main exercise intervention.
The type of exercise differed within the included studies. Aerobic exercise was performed by walking,32,38,40 using a treadmill32,34,35,40 or cycling on an ergometer33,36–38 via methods of continuous32,36–40 or interval training.33–35 Some studies implemented upper limb and lower limb resistance exercises34,36–40 in combination with aerobic exercise,31,35,37–40 rather than focussing on one method alone. Breathing retraining and chest expansion exercises,35,37 flexibility, 36 balance, and range of motion exercises 36 and group training which included aerobics, water gymnastics, outdoor walking, medical yoga, and psychomotor physiotherapy 34 were also implemented. Tailored pulmonary rehabilitation, within the included studies, was derived from guidelines related to chronic obstructive pulmonary diseases,38,40 respiratory disease, 39 and cancer 33 ; however seven studies31,32,34–37,41 did not use guidelines.
The cardiopulmonary exercise test-derived exercise prescription methods included: heart rate reserve31,32,35 (n = 3), maximum heart rate34,36,40 (n = 3), work rate37–39 (n = 3), anaerobic threshold and maximal oxygen uptake 33 (n = 1), rate of perceived exertion 36 (n = 1), and multiple methods 41 (n = 1). Cardiac indexes were most commonly used to prescribe exercise within the six included studies.31,32,34–36,40 With relation to heart rate reserve derived exercise, a total of three studies used this index,31,32,35 however the intensities were different in each of these studies. For two steady-state studies, intensity was set at 65–75% 31 and 70–80% 32 heart rate reserve. For an interval training study, 35 a 10-min warm-up at 50–70% heart rate reserve was conducted which was followed by five 3-min intervals of walking on a treadmill at 70–85% of the heart rate reserve, four 3-min walks at 50–70% of the heart rate reserve, and then a 10-min cool down at 50–70% of the heart rate reserve. 35
A percentage of actual maximum heart rate was used in one study to prescribe treadmill intervals of 3-min at 85% maximum heart rate. 34 The maximum heart rate equation (220 − age of the participant) was also utilised in one study for exercise prescription means 40 ; this study used an initial low intensity of 50–60% maximum heart rate that progressed to a target of 30 min continuous, moderate intensity exercise at 64–76% maximum heart rate via a unique range of progressions in pulmonary rehabilitation design. 40
Three studies utilised work rate indexes to define the intensity of their respective exercise programmes.37–39 The combination of anaerobic threshold and maximal oxygen uptake were used by one study to personalise exercise. 33 Interval training was performed on an electromagnetically braked cycle-ergometer for 3 min at moderate intensity using 80% of work rate at the anaerobic threshold, followed by a 2-min block at severe intensity which was calculated by using work rate equal to midpoint between anaerobic threshold and peak oxygen consumption. 33 Training intensity was progressed from 4× to 6× intervals after the first two sessions, or after the interim cardiopulmonary exercise test at week 4. 33
Synthesis of results
The main findings of the outcome measures are presented in Table 3. The most commonly reported cardiopulmonary exercise test outcomes within the included studies were maximal oxygen uptake32–41 (n = 11), maximum heart rate31,32,34–36,38–41 (n = 9), peak work rate32,33,37–41 (n = 7), and peak minute ventillation32–34,38–41 (n = 7). All the included studies that reported pre-to-post values for maximal oxygen uptake and peak work rate found improvements in these parameters (maximal oxygen uptake: 0.6 33 –44% 41 ; peak work rate: 7 38 –32% 32 ). Seven studies indicated statistically significant increases in peak work rate.32,33,37–41 Improvements in peak minute ventilation (5 34 –60% 41 ) were found in six studies,33,34,38–41 with only one study indicating a decline in peak minute ventilation (−4% 32 ). Maximum heart rate found variable results, whereby five studies31,35,39–41 increased (0.4 40 –6% 41 ), while four studies32,34,36,38 decreased (0.7 34 –2.7% 32 ). No adverse events were reported in any of the 11 included studies.
Key CPET outcome measure findings.
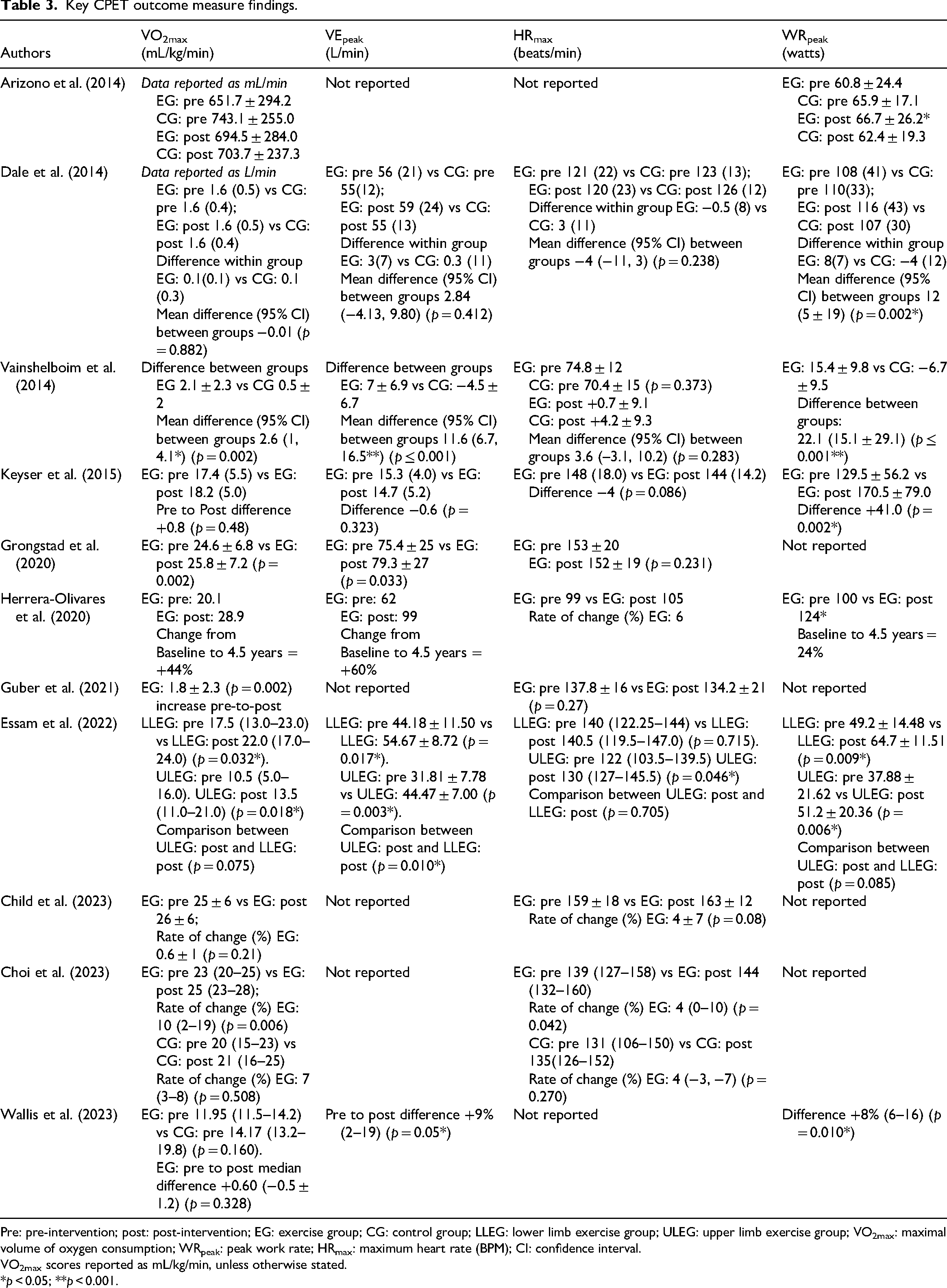
Pre: pre-intervention; post: post-intervention; EG: exercise group; CG: control group; LLEG: lower limb exercise group; ULEG: upper limb exercise group; VO2max: maximal volume of oxygen consumption; WRpeak: peak work rate; HRmax: maximum heart rate (BPM); CI: confidence interval.
VO2max scores reported as mL/kg/min, unless otherwise stated.
*p < 0.05; **p < 0.001.
Discussion
This review highlights consistent improvements in maximum oxygen uptake, peak work rate, and peak minute ventilation following tailored, cardiopulmonary exercise test-derived pulmonary rehabilitation for people with interstitial lung disease. Peak work rate was the most consistently enhanced metric, with statistically significant gains across seven studies (+7 38 to +32% 32 ), supporting the physiological efficacy of tailored pulmonary rehabilitation. Peak ventilation improvements suggest enhanced ventilatory efficiency, while heterogeneous maximum heart rate responses (−3 32 to +6% 41 ) reflect variability potentially linked to cardiovascular conditioning,22,43 abnormal autonomic regulation,22,43 or inconsistencies in prescription methodology.
The exercise intensity that is applied for tailored pulmonary rehabilitation prescription is of paramount importance for optimising training outcomes. 22 Many studies highlight that exercise intensities for tailored pulmonary rehabilitation should be based on the individuals cardiopulmonary exercise test measures,33,36,44 exercise performance,31,36,45,46 and preferences. 36 Within the included studies, intensity was commonly set at fixed or ranged percentages of maximum heart rate, work rate, and cardiorespiratory performance values.
Exercise intensity was prescribed using heart rate recovery within four studies,31,32,35 however the intensities were markedly different. For the steady-state studies, intensity was set at 65–75% 31 and 70–80%, 32 and 50–70% 35 to 70–85% for interval studies, showing a marked variation in exercise prescription methods with each interventional approach. All three studies found some benefit (+10%, 35 +5%, 32 +2.5% 31 ) in maximal oxygen uptake; but also suggests room for improving exercise prescription methods. Moreover, intensity was also derived from the maximum heart rate equation (220 − age of the participant) in one study, 40 with an initial low intensity exercise of 50–60% maximum heart rate that progressed to a target of 30 min continuous, moderate intensity exercise at 64–76% maximum heart rate via a unique range of progressions in pulmonary rehabilitation design. 40 The results were far more promising than studies which utilised heart rate reserve to prescribe pulmonary rehabilitation; however, this must be taken with the consideration that the 220 − age equation is not a valid predictor of maximum heart rate 47 and a younger patient sample with less advanced interstitial lung disease was used in this study. 40
A ‘one size fits all’ approach, relying on predictive methods (220 − age) for maximum heart rate and estimated heart rate reserve to prescribe exercise appears to have some benefit as mean fitness increases have been shown in people with interstitial lung disease, 21 aligning with similar evidence found in cardiology. 16 However, it may be that fixed heart rate reserve ranges (e.g. UK guidelines: 40–70%) may not reflect true metabolic thresholds. 16 A recent study found 54% of participants had ventilatory anaerobic thresholds outside this range 16 and thus misaligned intensity can impair adherence and minimise benefit. Tailored approaches based on metabolic thresholds (e.g. gas exchange thresholds), may induce a more appropriate exercise stimulus which matches the persons capabilities, thus promoting adherence to pulmonary rehabilitation and the associated benefits.
When considering robustness of prescription, risk of bias appraisal indicated variable methodological quality, with cohort studies limited by follow-up (n = 5) and outcome measurement (n = 2), and bias in two randomised controlled trials linked to design limitations, emphasising the importance of transparent reporting to support clinical interpretation. Moreover, exercise reporting via the ‘Consensus on Exercise Reporting Template’ revealed frequent reporting gaps in baseline activity levels (n = 10) which could result in bias due to differences in the participants previous exercise levels, and possible motivation for participation in activity, 48 as motivational strategies (n = 7) and non-exercise components (n = 5) were often omitted, hindering clinical translation.
Limitations in this review include significant heterogeneity in design, sex representation, pulmonary rehabilitation protocols, and interstitial lung disease subtypes, which precluded analysis and restricted generalisability. However, notable strengths include this being the first systematic review to evaluate the role of cardiopulmonary exercise test-derived, tailored pulmonary rehabilitation in people with interstitial lung disease, synthesising data from 11 studies involving 321 participants; an encouraging yield for an emerging field. Robust appraisal tools strengthen the methodological rigour 30 and highlights pathways for clinical implementation.
In summary, tailored pulmonary rehabilitation, informed by CPET, shows promise in enhancing exercise capacity and ventilatory efficiency for interstitial lung diseases. Consistent improvements in maximum oxygen uptake, peak work rate, and peak ventilation support its clinical utility, while variability in cardiac-based responses underscores need for more precise prescription methods. Future research should compare tailored pulmonary rehabilitation with standard care, evaluate alternative cardiopulmonary exercise test prescription indexes (such as the gas exchange threshold), and adopt transparent, standardised reporting for clinical translation.
Clinical messages
Tailored pulmonary rehabilitation may improve exercise outcomes such as peak oxygen uptake and peak work rate in people with interstitial lung disease.
All seven studies assessing peak work rate reported statistically significant improvements, supporting its use as a primary outcome measure for rehabilitation effectiveness.
No serious adverse events were reported across the included studies, confirming the safety of structured rehabilitation programmes for this population.
Exercise prescription methods varied between studies; future research should prioritise standardised protocols and consistent reporting to enhance clinical applicability.
Footnotes
Author contributions
BB, CAW, MAG, CJS, and OWT developed the protocol. The searches and analysis of the review were performed by BB, TL-K, and OWT. Data extraction was performed by BB, SG, and TL-K. BB, CAW, MAG, CJS, and OWT reviewed the final synthesis. All authors have contributed to the manuscript and agreed on the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study/research is funded by the National Institute for Health and Care Research and Exeter Biomedical Research Centre. The views expressed are those of the authors and not necessarily those of the National Institute for Health and Care Research or the Department of Health and Social Care. The funder has had no role in the design of this research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Prior publication
A provisional abstract associated with this work was presented at the 2024 British Thoracic Society Meeting, and published as a supplement under the following citation: Bowhay et al. (2024), P249 Exploring the potential of cardiopulmonary exercise testing for individualised pulmonary rehabilitation in people with interstitial lung disease: a systematic review, Thorax, 79(S2): A258–A259.