
Abstract
Objective
To identify healthcare professionals’ perceptions of pulmonary rehabilitation as a management strategy for people with chronic obstructive pulmonary disease (COPD).
Design
A qualitative interview study which adopted an interpretive phenomenological approach.
Methods
Twenty-seven healthcare professionals were recruited from general practices in the North West of England and two hospital trusts, consisting of: general practitioners, practice nurses, and doctors and nurses working on general medical wards. Audio recorded semi-structured interviews investigated healthcare professionals’ perceptions and knowledge of pulmonary rehabilitation; interpretive phenomenological analysis was conducted on the transcribed interviews.
Results
Three themes were identified: COPD Illness Perceptions, Pulmonary Rehabilitation Beliefs, and Organisational and Referral Pathway Perceptions. Commonalities and disparities were identified between primary and secondary care and amongst the different professional groups. Healthcare professionals held negative COPD illness perceptions including stigmatising beliefs in relation to the disease. These beliefs impacted their referral practice. Beliefs about pulmonary rehabilitation included views about patient suitability for the pulmonary rehabilitation programme. A lack of knowledge of pulmonary rehabilitation and the referral process was evident. Surprisingly, many working on general medical wards had not heard of pulmonary rehabilitation and none in their current role had referred to the programme. Organisational and referral pathway perceptions revealed barriers and facilitators to referral.
Conclusion
Referral to pulmonary rehabilitation programmes is influenced by healthcare professionals’ perceptions and knowledge of pulmonary rehabilitation, referral pathways and how COPD affects patients. Together health professional perceptions could act as a predictor of referral practice and inform strategies for increasing referral rates.
Introduction
Pulmonary rehabilitation is an established cost-effective evidenced-based intervention which reduces chronic obstructive pulmonary disease (COPD) related hospital admissions. 1 A non-pharmacological therapeutic management strategy, pulmonary rehabilitation is delivered by a multidisciplinary team, providing individualised care for patients regardless of where they are on the disease trajectory. 2 The aim is to assist with COPD self-management by offering support in three domains: physical, social and psychological. 3 Pulmonary rehabilitation should therefore be multifaceted and encompass an exercise regime to increase activity, education, breathing techniques, medication advice and psychological support.4,5
Regardless of the programme's proven effectiveness, attendance and adherence for patients with COPD is low. 6 Access, participation and attrition is a global issue, speculatively due to a lack of availability of the programme in low- or middle-income countries and being underutilised or inadequately resourced in high-income countries. 5 Literature highlights the perceived barriers to accessing pulmonary rehabilitation for individuals with COPD. 7 Some refuse referral believing their condition is self-inflicted due to smoking 8 ; others feel anxious, believing exercise induces breathlessness, a feeling they wish to avoid. 9 Transportation issues are also highlighted, 6 in addition to pulmonary rehabilitation often taking place during working hours. 8 Many are unfortunately unaware of pulmonary rehabilitation and cannot recall being offered referral. 10 Factors relating to income and location, which contribute to overall socio-economic status can also influence adherence. 11
It is recommended pulmonary rehabilitation should be provided to all who meet the criteria defined in COPD guidelines 12 along with those admitted to hospital with an exacerbation of their COPD. 4 However, the findings from The National Asthma and COPD Pulmonary Rehabilitation Audit 13 highlight only 5.2% (632) of UK patients were referred to pulmonary rehabilitation after admission to hospital with an acute exacerbation of COPD. Thus, improvement in access is required in secondary care, in addition to primary care referrals.
Currently, literature exists surrounding patients’ perceptions of pulmonary rehabilitation, 14 however little is known regarding healthcare professionals’ views. A systematic review drew attention to healthcare professionals’ perceptions with a significant focus upon the barriers to pulmonary rehabilitation, such as a lack of healthcare professional knowledge, diminished time to make a referral, and practical barriers such as transportation and long waiting lists. 15 Most referrals made to pulmonary rehabilitation in the UK are from primary rather than secondary care, 13 although those referred by a general practitioner (GP) are less likely to complete the programme. 16 Predictors of referral in primary care in Wales highlight it is less likely for those who are a current smoker, over the age of 70, female, deprived, or have a comorbidity such as asthma or a condition which leads to pain. 17 It is evident healthcare professionals are not referring patients as frequently as they could, however the reasons for this are unclear. 18 Much of the current literature regarding healthcare professionals’ perceptions focusses upon those with the ability to refer in primary care, with limited understanding of whether the perceptions of those in secondary care are similar. 15 The current study therefore aims to identify the perceptions of healthcare professionals both in primary and secondary care regarding pulmonary rehabilitation for patients with COPD.
Objectives
To establish healthcare professionals’ understanding of pulmonary rehabilitation.
To explore the perceptions that healthcare professionals, both in primary and secondary care, have about referring those with COPD to pulmonary rehabilitation.
To explore barriers and facilitators to referral to pulmonary rehabilitation.
Methods
University ethical approval was obtained, in addition to National Health Service (NHS) Health Research Authority approval (IRAS ID: 208153). Purposeful recruitment of healthcare professionals with the ability to refer COPD patients to pulmonary rehabilitation was employed. Ability to refer to pulmonary rehabilitation was the homogenous factor. Participants were recruited from four professional groups: GPs and practice nurses in primary care, and doctors, and nurses working on general medical wards in secondary care. Recruitment took place in two clinical commissioning groups, and two hospital trusts in the North West of England. A general medical ward was defined as a ward with no specialism, which cared for patients with various conditions. This included, but was not exclusive to, medical assessment units, GP assessment areas, ambulatory units, general medicine departments, elderly care wards, acute medicine, and clinical decisions wards. A letter with a reply slip was sent to those working in primary care, and an email was sent by a gatekeeper to eligible healthcare professionals working on general medical wards in secondary care. A second strategy, due to a low response rate in secondary care, enabled the lead researcher (ES) to accompany the gatekeeper to general medical wards to discuss details of the study in person with the healthcare professionals working there.
Data collection
Individual semi-structured interviews were conducted; congruent with standard data collection methods for interpretive phenomenological analysis (IPA) studies. 19 All interviews were digitally audio recorded with the participants’ consent and took place at a mutually convenient time. Interviews conducted in primary care (n = 14) were all via telephone, at participants’ request. Conversely, most interviews in secondary care (n = 11) were conducted face to face at the hospital where the healthcare professional worked. These typically took place in offices off the general medical ward, or in an unoccupied family or day room. The remainder of secondary care interviews (n = 2) were conducted via telephone. Questions focussed on: experience with respiratory conditions, understanding and perceptions of pulmonary rehabilitation, the referral process, factors influencing a referral decision, and if they had received any feedback on the programme and its effectiveness. Details of participant demographics are provided in Tables 1 and 2.
Participant demographics primary care.
GP: General practitioner; PN: Practice nurse.
Participant demographics secondary care.
DR: Doctor working on a general medical ward; GN: Nurse working on a general medical ward; FY1: Foundation doctor (year one); FY2: Foundation doctor (year two).
A researcher reflexive diary was completed during the recruitment process by ES, with notes being taken after each interview, transcription, and during data analysis. This process allowed for any initial thoughts, feelings, or interpretations to be accounted for and later incorporated into the analysis. 20
Data analysis
IPA was employed. Verbatim transcription occurred after each interview. Commencing this process prior to the next interview allowed for instant immersion in the data and for any interesting new topics or emergent themes to be noted and incorporated into subsequent interviews. 19 Analysis was conducted using NVivo 11® and due to the ideographic nature of IPA 20 transcripts were analysed case by case and line by line, with notes made of any pertinent quotes in relation to healthcare professionals’ perceptions of pulmonary rehabilitation. As greater familiarity with the transcript was achieved, similarities, disparities and contradictions in participant perceptions throughout the transcript were noted. 20 The process of IPA has been summarised in Figure 1.
The main steps of IPA data analysis (adapted from Smith et al., 2009). 20
The data were analysed by ES and audited by CK to ensure super-ordinate and sub-ordinate themes were grounded in the data; agreement was achieved. A narrative was formed with the intention to take the reader on a journey through the participants’ experiences and views, providing verbatim quotes, discussing interpretation and acknowledging instances of disparity. 20
Results
Twenty-seven participants, consisting of GPs (n = 8) and Practice Nurses (n = 6) from primary care, and Doctors (n = 6) and General Nurses (n = 7) from secondary care, were interviewed. Table 3 details individual participant characteristics and general perceptions of pulmonary rehabilitation; this has been displayed to preserve the ideographic nature of IPA and allow the reader to become familiar with each participant before reading the narrative.
Individual participant characteristics and general perceptions of PR.
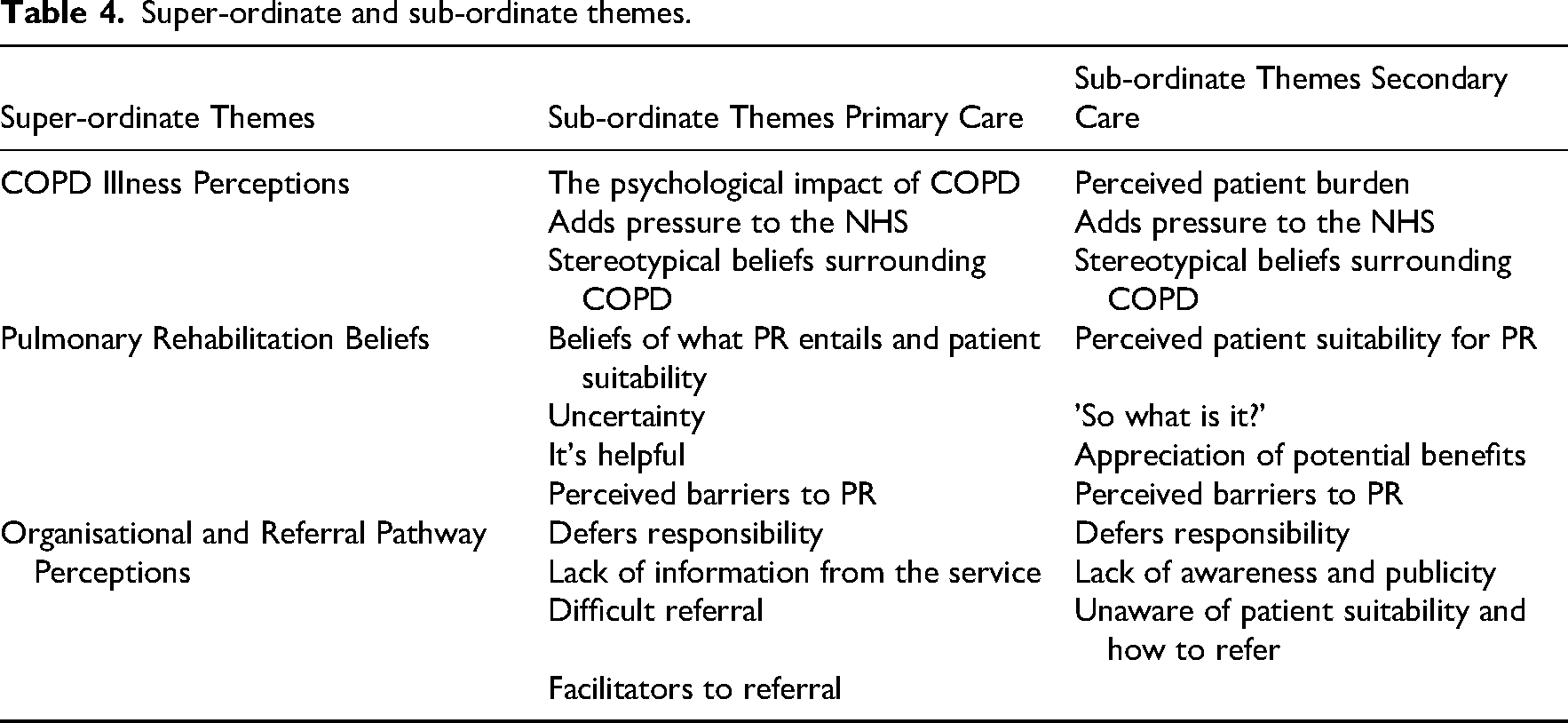
The data have been organised and displayed under three super-ordinate themes: COPD Illness Perceptions, Pulmonary Rehabilitation Beliefs, and Organisational and Referral Pathway Perceptions. Details of the different sub-ordinate themes within each super-ordinate theme for primary and secondary care can be seen within Table 4. Within the analysis each quote will be followed by a participant identifier in brackets to acknowledge which participant perception is being discussed. For example: (GN 2, 41–50, H2). GN represents general nurse, then follows the age range of the participant and H2 depicts the hospital the participant was recruited from.
Super-ordinate and sub-ordinate themes.
COPD illness perceptions – primary care
In primary care illness perceptions were evident, with many healthcare professionals having a strong belief about the psychological impact which a diagnosis of COPD can have. There was a perceived negative influence of COPD on both emotional and mental health: ‘what we have to remember is living with a life-long illness requires a lot of sort of emotion, and mental resources’ (PN 3, 51–60)
It was deemed many with COPD are anxious, and this impinged patients’ lives; the worry and apprehension can alter belief in abilities and cause refrainment from activities. As a result, individuals enter a ‘breathlessness vicious cycle’ (PN 5, 25–30), whereby they become trapped in a continuum of inactivity, due to trepidation surrounding perceived shortness of breath. GPs discussed how those with COPD wanted a quick fix, a ‘miracle answer to everything’ (GP 3, 41–50). They viewed this group as resistant to change, particularly surrounding exercise, with the perception that medical intervention was only wanted via prescription: ‘it's you know exercise, it can’t possibly make them significantly better, and it has to be something on prescription, you know be it a tablet or an inhaler, and why could anything else work.’ (GP 6, 51–60)
Many held similar stereotypical beliefs and drew attention to the perceived stubbornness and unwillingness of those with COPD. It was a struggle to convince patients that exercise was appropriate, with them often creating excuses rather than being open-minded: ‘they’ve often got an answer for it. If you tell them to go swimming, “oh I don’t like swimming, I can’t swim, it's too cold the water”. They’ll come out with everything, rather than realising that you know walking, swimming, whatever, is going to improve their health in the long run.’ (GP 8, 51–60)
There was a consistent belief that ‘COPD has been caused by smoking’ (GP 7, 41–50), and this was defined as the root cause for the disease by those working in primary care. It was felt that COPD was more commonly being diagnosed at a younger age, with one GP associating the disease with those living in a socially deprived area and being in receipt of state benefits: ‘We’ve got people in their forties… it's quite a deprived big council estate, most of them on benefits and they’re all still smoking’ (GP 8, 51–60)
COPD illness perceptions – secondary care
Within secondary care healthcare professionals perceived COPD as a burden for individuals and a ‘deteriorating condition’ (GN 2, 41–50, H2). General health and symptoms were sensed to deteriorate as the disease progresses. It was deemed a particularly troublesome condition with an inability to restore health to its previous state: ‘it just tends to basically get worse … you can’t cure it as such’ (GN 1, 51–60, H2)
Shortness of breath was considered a demanding aspect. Many doctors associated breathlessness with their medical knowledge of the mechanics of ventilation. Although knowledgeable about symptoms, definitions significantly focussed on the multi-facetted, unpredictable nature, its impact upon breathing and limits on exercise: ‘it's a chronic condition, associated with sort of fixed airway obstruction and difficulty with ventilating, patients tend to have sort of exertional shortness of breath, chronic cough, often they produce a lot of sputum’. (DR 4, 25–30, H1)
Those in secondary care perceived COPD added pressure to the NHS and this was commonly associated with COPD patients being viewed as frequent attenders at hospital. COPD was noted as ‘probably one of the most [common] things we tend to see’ (GN 1, 51–60, H2). Although sometimes a primary presentation, many discussed how patients on general medical wards regularly had COPD in ‘the background’ (DR 4, 25–30, H1). The condition was believed to trigger a cyclical process, whereby an individual becomes better whilst in hospital, but shortly after discharge they become unwell, and require readmittance: ‘we see a lot of exacerbations of COPD and they’re multiple admittances’ (GN 5, 51–60, H2)
Those in secondary care also held stereotypical COPD illness beliefs, perceiving COPD was ‘most commonly caused by smoking’ (DR 6, 25–30, H2). One doctor expressed her view that smoking was a negative health decision, she thought a lack of commitment to smoking cessation was related to people with COPD not wanting to take ownership of their health and adhere to pulmonary rehabilitation: ‘if they’re not engaged in doing things for themselves, for example like stopping smoking, they will be more unlikely to be engaged with a programme where they have to take responsibility.’ (DR 1, 25–30, H1)
There was also the view that ‘compliance is a big issue with COPD patients’ (DR 5, 25–30, H2) and that they lacked conformity and would not engage with health-related programmes. These illness beliefs defined their perceived suitability for pulmonary rehabilitation.
Pulmonary rehabilitation beliefs – primary care
All healthcare professionals in primary care discussed opinions of what pulmonary rehabilitation entails and patient suitability. Several GPs provided a general definition of pulmonary rehabilitation, rather than focussing on details of their local programme. They often concentrated on the exercise component describing it as ‘an exercise programme used to improve the breathing’ (GP 4, 31–40). Although, others appeared unsure and speculated what their local programme entailed: ‘I think it's quite limited [knowledge] I’m afraid, I just know that you can refer into it and then the patients have like, probably about, I think a set number of sessions, like six or eight sessions in a programme.’ (GP 2, 31–40).
Practice nurses recognised a purpose of pulmonary rehabilitation was providing an escape ‘coffee and a chat’ (PN 3, 51–60) for those who may be socially isolated. They viewed pulmonary rehabilitation as increasing health-related knowledge, and improving well-being: ‘Pulmonary rehabilitation has been providing a source of education with supportive data demonstrating positive outcomes on quality of life for years’ (PN 3, 51–60)
Perceived patient suitability was commonly discussed, and healthcare professionals held different criteria as to who they would consider for pulmonary rehabilitation. Some appeared to follow general guidance set by the local programme suggesting ‘they have to have roughly an MRC [Medical Research Council Dyspnoea Scale] 3 scale’ (PN 3, 51–60). Others believed it may not be suitable for those who were continuing with daily activities and able to work. An internal conflict was apparent, as it was deemed referral should not be left too late: ‘there are patients that are still active and working, and coping with COPD, and it might not be suitable for them because they’re not actually experiencing any difficulties. But then we’ve got to be careful that we don’t wait till they are experiencing very, very vast difficulties.’ (PN 2, 41–50)
Frequent exacerbations were a prominent symptom which triggered GPs to consider pulmonary rehabilitation, as it was often deemed appropriate for those at the worse end of the spectrum. Strikingly, several GPs considered pulmonary rehabilitation as a last resort: ‘I see quite a lot of people who are on maximal therapy and have multiple exacerbations of their COPD, I could refer some of those I suppose’ (GP 4, 31–40)
Others referred patients for the psychological support provided, rather than any overt physical benefits. They felt strongly about the depth of psychological impact associated with COPD, which included refrainment from activities and a considerable impact on quality of life. For those impacted in this way pulmonary rehabilitation was viewed as a lifeline, and a prompt to start discussions about the programme: ‘I might be talking with someone about you know, when they were going out and seeing their friends … the things that make us smile and bother to stay on this earth sort of thing, and if their breathing was something that was stopping them doing that, or their confidence in their breathing was something that was stopping that, then I might start a conversation [about PR]’ (GP 3, 41–50)
There was a disparity between perceived patient suitability with some aware of and adhering to local programme criteria, and others making their own presumptions based upon individual patient characteristics.
Pulmonary rehabilitation beliefs – secondary care
Opinions ranged regarding patient suitability and the characteristics required to attend pulmonary rehabilitation. Doctors perceived pulmonary rehabilitation was for patients with ‘worsening breathlessness, their inhalers aren’t really working, you’ve kind of tried everything’ (DR 1, 25–30, H1), whereas general nurses believed it was better if ‘you catch them early, to start them off with these exercises’ (GN 4, 41–50, H2).
A notable finding in secondary care was many ‘didn’t really know it [PR] was a service’ (DR 2, 25–30, H1) or what it involved. Each healthcare professional in secondary care worked on a general medical ward with many COPD patients; a prominent feature of many interviews was: ‘it's the first time I’ve heard about it [PR]’ (DR 3, 31–40, H1). Although not intentional, participation in the research interview raised awareness for many.
The term rehabilitation caused confusion, with it sometimes being associated with a bridge between hospital and independent living. One general nurse highlighted uncertainty when they asked: ‘are you talking about when they’re going home?’ (GN 4, 41–50, H2). Rehabilitation was associated with the perception that patients can return to a state of health held prior to a diagnosis or accident. This was not deemed possible for those with COPD and therefore the name ‘pulmonary rehabilitation’ resulted in confusion: ‘we don’t really have anyone on that, the rehab ward, I have worked in the rehab ward, that was for hips.’ (GN 5, 51–60, H2)
Interestingly, many were aware of cardiac rehabilitation and chose to discuss this instead. One general nurse who had been working with COPD patients for many years was shocked: ‘I’ve worked in acute medicine for 20 years, and I’ve never heard of pulmonary rehab, I’ve heard cardiac rehab but I’ve not heard pulmonary rehab.’ (GN 2, 41–50, H1)
Despite lacking knowledge of pulmonary rehabilitation, healthcare professionals discussed how they could appreciate the potential benefits. The non-medicalised approach was considered to improve lung capacity and ultimately enhance patients’ ‘well-being and way of life’ (DR 1, 25–30, H1). Healthcare professionals valued the educational aspect, as this was deemed vital in assisting self-management of symptoms. Education was perceived to provide a pragmatic, representational view of disease progression: ‘it can educate them, so they can try and pre-empt and reduce exacerbations, and try and find ways in which they can manage their condition a lot better.’ (GN 7, 41–50, H2)
Organisational and referral pathway perceptions – primary care
Many in primary care deferred the responsibility of referral. This appeared closely associated with not considering pulmonary rehabilitation a priority. Some GPs discussed how they previously made referrals but now felt deskilled. They felt it was not their role to refer patients, and often deferred responsibility to practice nurses: 'She's [nurse practitioner] basically as good as a GP… but she's got a lot more knowledge and confidence to manage this [pulmonary rehabilitation], so she can admit to hospital and all sorts of things’ (GP 8, 51–60)
Others ‘kind of assumed that they’ve [patients] already been referred’ (GP 4, 31–40), and regarded it as the role of secondary care, or should be ‘automatic’ (GP 5, 41–50), after a hospital admission. Interestingly, after a period of reflection one GP came to the realisation that other healthcare professionals may also assume someone else is initiating referral: ‘I bet quite a few of the secondary care [healthcare professionals] think that we’re doing it all [referrals]’ (GP 8, 51–60)
Practice nurses took greater responsibility for referrals and when discussing pulmonary rehabilitation were predominantly positive. They however felt too much pressure to complete a referral during a COPD annual review. Although not deemed the most appropriate decision on some occasions due to time restrictions, pulmonary rehabilitation was sometimes overlooked: ‘due to time constraints and being busy I just thought, oh I’ll wait and we’ll review you next year and see how you’ve got on, but really I felt that the intervention would have been better early.’ (PN 2, 41–50)
There was agreement that better communication was required between the service and referrers. It was considered difficult to be knowledgeable about the benefits of pulmonary rehabilitation: 'So, there's no real details about the course itself … we never got this is week one, week two, week three, the content … we were referring people blind if you like.’ (PN 1, 61+)
Practice nurses believed referrals took tremendous effort but were disheartened that the pulmonary rehabilitation team did not inform them of patient progress. It was perceived their efforts would be worthwhile if they knew the patients had benefitted from the sessions. There was the notion that a lot was expected from them, however they received very little back from the service: ‘it seems like a one way road of information, that we send loads of information about medication, spirometry, history, all this sort of stuff, and we either get patient attended pulmonary rehab, or patient failed to attend’ (PN 1, 61+)
Uncertainty was coupled with the perception pulmonary rehabilitation was a complicated sell. Many found it difficult to initiate conversations surrounding pulmonary rehabilitation, as they perceived ‘a lot of them [patients] are not interested to start with’ (GP 5, 41–50). Practice nurses tried to encourage attendance, although this was not always straightforward; it was considered the phrase ‘light exercise’ (PN 1, 61+) evoked fear. Others believed the ease of the sell was dependent on individual demographics: ‘I’ve come to a much younger group, I mean the number of people in their forties and fifties that we’re diagnosing, got quite a high cannabis use area as well, and basically just to get them to understand that something that isn’t a medicine is going to help them, is a much more difficult concept to get across to this group’ (PN 3, 51–60)
Referrals were considered time-consuming, and in some cases acted as a deterrent. There was the notion that: ‘if referrals are made easy then you do a lot more of them’ (PN 2, 41–50). It was evident key facilitators, such as having a ‘simple pro-forma’ (GP 2, 31–40) greatly assists referral.
Organisational and referral pathway perceptions – secondary care
All healthcare professionals in secondary care believed there was a lack of awareness and publicity surrounding pulmonary rehabilitation. Low awareness was often attributed to pulmonary rehabilitation not being discussed in detail, or forming a core part of the COPD curriculum during either medical or nursing degree: ‘it's just mentioned as a part of the management plans generally in terms of medical education. There's no formal mention of it [pulmonary rehabilitation] really’ (DR 4, 25–30, H1)
Lack of publicity was closely aligned with a lack of awareness, however in this instance healthcare professionals often blamed the service for their dearth of knowledge. It was considered the responsibility of the service to raise awareness and the profile of pulmonary rehabilitation: ‘I’ve known nothing about it before, so if there are services available it probably does need to be advertised a bit more.’ (DR 5, 25–30, H2)
Many in secondary care also deferred responsibility to justify their lack of referral. They considered it was not their role as they ‘don’t deal with that [pulmonary rehabilitation]’ (GN 5, 51–60, H2). A prominent justification was the primary role of those working on general medical wards was to assist patients with their acute condition. Hospital was considered as a holding area, where medical intervention was administered. The responsibility of referral was deferred to primary care: ‘in hospital, especially in the acute wards, we’re so focused on getting people into hospital, treating them for their acute conditions and then sending them home when they are back to their baseline. So, I think therefore there's probably more of a place in primary care, in terms of it being a bit more of a holistic approach to, to their treatment.’ (DR 1, 25–30, H1)
Although not specifically articulating a deferral of responsibility, a doctor contemplated the situation in primary care: ‘I don’t know whether the GPs have better knowledge of it, or whether it's just hospital doctors that don’t’ (DR 5, 25–30, H2)
Healthcare professionals in secondary care also discussed patient suitability and how to refer as a prominent issue. Being unsure of patient eligibility and the referral process acted as a barrier. Some stated ‘I wasn’t aware I could [refer to pulmonary rehabilitation]’ (GN 6, 41–50, H2). Many also stated that they ‘don’t know what the requirements are’ (DR 1, 25–30, H1).
Overall, it was apparent that many clinicians on general medical wards would ‘definitely consider’ (DR 1, 25–30, H1) referral to pulmonary rehabilitation if aware of patient suitability and if the referral process was simple and undemanding.
Discussion
This study is the first to investigate the perceptions of healthcare professionals working in primary care and on general medical wards within secondary care, regarding pulmonary rehabilitation as a management strategy for individuals with COPD. The findings raise several important considerations surrounding healthcare professionals’ perceptions of pulmonary rehabilitation and the ability for these beliefs to impact referral practice. It was surprising that, healthcare professionals (aware of programmes such as cardiac rehabilitation) largely lacked knowledge of pulmonary rehabilitation. Poignantly, none of those working on General medical wards had referred a COPD patient to pulmonary rehabilitation, despite caring for those with COPD daily. This study identifies a need for enhanced awareness of non-pharmacological management strategies to support those with COPD, with many healthcare professionals favouring a medicalised approach.
The associated beliefs surrounding a diagnosis are referred to as illness perceptions; these are internal beliefs which individuals develop to try to make sense of their condition. 21 Healthcare professionals illness perceptions regarding COPD were surprisingly varied, with some holding negative views surrounding the cause of COPD, for example considering it as a smoker's disease. Others generalised COPD patients’ motivation surrounding exercise programmes and held opinions surrounding their socio-economic status and education. This supports Mathiopudakis et al.'s work which highlights a stigmatisation that some individuals with COPD feel from healthcare professionals and the impact this has on the care they receive. 22 Previously, the literature has focussed upon COPD illness perceptions from a patient's view with regards to how they perceive, and then manage their condition, 23 the current study extends this to investigate beliefs from a healthcare professionals’ perspective.
Within primary care healthcare professionals focussed on the psychological impact of COPD, such significance, however, was not placed on physical symptoms. In contrast, in secondary care the complexities of the physical symptoms were centred upon, and no cure. The burden of multiple symptoms and the impact on quality of life has been previously discussed. 4 It could be proposed the strict use of the medical model may influence healthcare professionals’ perceptions of the disease, whereby focus is placed upon treating the condition rather than assisting patients to live with it. In the current study, in secondary care it was perceived that exercise induces breathlessness. This illness perception has the potential to impact referral to pulmonary rehabilitation and is consistent with a Spanish study of 338 medical students (47.1%), who did not recommend exercise for those with COPD. 24
Negative beliefs surrounding COPD were common in primary and secondary care. Despite evidence to display the correlation between the incidence of COPD and smoking, 25 the frequency with which healthcare professionals in the current study mentioned smoking, suggests they consider COPD as a smoker's disease. The findings of the current study highlight smoking being associated with receipt of benefits and geographical location. Notably, it appeared some healthcare professionals stigmatised whole communities, or groups, based upon the cognitive representation they had built regarding their practice location; something not previously discussed in the literature with regards to COPD. Reference to compliance, concordance, and adherence to self-management has however previously been referred to. 26 The literature also emphasises that socio-economic status and where an individual lives can also impact adherence to pulmonary rehabilitation. 11 The findings of the current study highlight those in secondary care perceive COPD patients as being unable to take control of their health, are resistant to change, and this was related to the notion patients often lacked compliance and engagement with healthcare.
Unfamiliarity with pulmonary rehabilitation eligibility criteria has previously been discussed within the literature. 15 Fundamentally, healthcare professionals in primary care in the current study had a good understanding of what pulmonary rehabilitation entails, yet some questioned the ideal time to refer and whether this should be pre or post significant impact upon lifestyle. Those in secondary care in the current study perceived pulmonary rehabilitation as an add on. Others perceived eligibility would depend upon the age of the patient, believing younger patients would achieve more. This however is a misconception and a lack of belief in older patients’ abilities, as pulmonary rehabilitation can improve lung function, general health, and quality of life in the elderly. 27
The effectiveness of pulmonary rehabilitation in reducing COPD related hospital admissions is proven 4 and given the concern from healthcare professionals in secondary care surrounding pressures on hospital capacity, the lack of awareness surrounding pulmonary rehabilitation was an unexpected finding. Healthcare professionals never having heard of pulmonary rehabilitation has been highlighted previously in Saudi Arabia, 28 however this is not a known finding in the United Kingdom. There were commonalities in perceptions of barriers to the programme between professional groups and primary and secondary care, such as location, transportation and session times. These issues are prominent within the literature, for healthcare professionals, 28 and patients alike. 6
In the current study, healthcare professionals on general medical wards attributed their lack of awareness of pulmonary rehabilitation to limited publicity. Consistently, pulmonary rehabilitation was viewed as being missing from the medical and nursing curricula. This is a unique finding, as it is believed a lack of teaching has not previously been attributed as a barrier to referral.
Deferral of responsibility was discussed in primary and secondary care, and the pertinence of this issue is reinforced in the literature. 15 The lack of responsibility for referral contradicts the patient centred care approach, which endeavours to meet patient needs whilst providing a positive healthcare experience. 29 In the current study, it was unusual for practice nurses to defer referral responsibility. Referral often took place during a 30-minute COPD annual review; practice nurses believed there was not enough time to complete other tasks in addition to referral. Restricted primary care appointment times have also been cited as a barrier in Australia, 30 highlighting the issue is not exclusive to the UK. In the current study, other than practice nurses, everyone deferred referral, each believing it was another's role. This could also further emphasise the lack of referrals highlighted in the National Pulmonary Rehabilitation Audit. 18
This is the first study to include the perceptions of both those working in primary care and secondary care in relation to pulmonary rehabilitation for those with COPD. Attention was given to the suitability of IPA as it could be argued 27 is a large sample size. It is however suggested there is no definitive answer to the correct number of participants in IPA, as data collection should be driven by the richness of the data obtained and dependent upon how the researcher compares different accounts. 20
A potential weakness was that interviews were conducted by a non-healthcare professional (ES), however this instead appeared to facilitate conversation, with healthcare professionals providing examples with no assumption of shared knowledge, resulting in rich data being collected. Challenges associated with assumed knowledge and power dynamics have previously been highlighted, and it is suggested that reflective notes can mitigate these issues, 31 something which the current study employed.
In conclusion, referral to pulmonary rehabilitation appears dependent upon individual healthcare professionals, their perceptions of pulmonary rehabilitation, how COPD affects patients, and their knowledge of referral. These aspects pieced together, could act as a predictor of referral practice and inform strategies for increasing referral rates. It is hoped this research will contribute to the limited knowledge of healthcare professionals’ perceptions of pulmonary rehabilitation and add a unique perspective and potential explanation as to why the National Pulmonary Rehabilitation Audit 18 concluded referrals to pulmonary rehabilitation were lacking. Further research would be beneficial to survey those working in primary care and secondary care across the UK, to assess if the findings could be generalised, and highlight beliefs with regards to pulmonary rehabilitation amongst a larger group. Those working on respiratory wards would add further insight, to determine if their knowledge or understanding of the programme is also lower than expected and how often they refer. Lastly, given healthcare professionals discussed a lack of teaching or exposure to pulmonary rehabilitation during their medical or nursing degrees, additional research is required to determine how pulmonary rehabilitation is incorporated into the curricula.
Clinical messages
The illness perceptions healthcare professionals hold about chronic obstructive pulmonary disease can influence pulmonary rehabilitation referrals.
Greater communication is required between healthcare professionals surrounding referral to pulmonary rehabilitation. It should not be assumed other colleagues are making a referral.
Better education and awareness raising is required for healthcare professionals. This should come from local pulmonary rehabilitation services and be better integrated into medical and nursing degrees.
Footnotes
Acknowledgements
The authors acknowledge the support gained from clinical commissioning groups and two hospital trusts within the Northwest of England, who the participants were recruited from. Also, they extend their thanks to the healthcare professionals working within the NHS who gave up their valuable time to participate in the study.
Author contributions
ES, MOB, SP and CK were all involved in the design of the project. ES applied for ethical approval, conducted the literature review and recruited participants. ES conducted the data collection and lead the data analysis, MOB and SP were involved in refining the analysis and super-ordinate and sub-ordinate themes. The data analysis was audited by CK to check for agreement between ES and CK. The first draft of the manuscript was written by ES and all authors reviewed and edited the manuscript and approved the final version.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.