
Abstract
Objective
To explore how individuals with chronic-stroke experience and engage in home-based self-training, aiming to highlight factors related to their adherence and overall experience of self-training.
Design
A qualitative study.
Setting
Community.
Subjects
Individuals with chronic-stroke.
Interventions
Participants underwent a structured 5-week home-based upper-extremity self-training via videogames or the Graded Repetitive Arm Supplementary Intervention which includes activities using everyday objects.
Main measures
Participants were interviewed following their participation in the self-training intervention, using a semi-structured interview. Interviews were transcribed verbatim and then analyzed using thematic analysis. Findings were validated through author discussions.
Results
Twenty-two participants (63% men) were included, aged 33 to 80, 6–36 months post-stroke. Participants had preserved cognitive ability, were mostly independent in daily living, and had a moderate upper-extremity motor ability (median (interquartile range (IQR)) Fugl-Meyer Motor Assessment score: 41 (29–47)/66 points). Three main themes were identified: 1) personal factors (e.g. devotion to perform self-training, commitment to the study, and personal roles), 2) self-training factors (e.g. experience and its influence on general condition), 3) environment-related factors (e.g. training equipment, home environment, and family support). The structured intervention and family support led to motivation and commitment. Challenges included time constraints, pain, and fatigue.
Conclusions
This qualitative study deepens understanding of home-based self-training experiences among individuals with chronic-stroke, highlighting how motivational, environmental, and self-training factors interact to shape long-term adherence. These insights can guide clinicians tailor interventions to promote long-term adherence and engagement by addressing individual, environmental, and task-related factors, and by identifying participants who may require additional support.
Introduction
Individuals with stroke often experience persistent neurological impairments 1 that affect function and independence and therefore require long-term rehabilitation. On-going rehabilitation following discharge can help maintain the gains achieved during the in-patient rehabilitation, further improve motor and cognitive functioning and enhance the reintegration into daily life. 2 Without continued therapy, these gains may be lost 3 particularly for individuals who do not spontaneously use their affected upper-extremity in daily activities. 4 However, ongoing rehabilitation may not be possible due to time constraints, lack of access or high costs.
Self-training interventions can improve individuals’ motor abilities and upper-extremity use after stroke. 5 These individuals are expected to perform the training independently, which differs completely from the one-on-one therapist treatment sessions they received during rehabilitation. Various self-training methods, such as videogames, 6 task-oriented training, 7 and virtual reality, 8 have been examined to improve upper-extremity function. Studies of specific home-based self-training interventions have focused on the feasibility, satisfaction, and adherence, 5 but the experience of engagement and adhering to self-training in a home setting has not yet been researched.9,10 This inquiry can provide insights regarding factors which might interfere with or facilitate ongoing engagement and adherence of self-training. This understanding might also help clinicians identify which of their clients are prone to perform the self-training while less suitable for others.
Self-training was implemented as part of a randomized controlled trial11,12 by using commercial videogames in one group and the Graded Repetitive Arm Supplementary Intervention (GRASP), proven to improve upper-extremity function, in the other group. Following the intervention, both groups showed functional improvement, 2 with high adherence and satisfaction levels. 13 This study aims to 1) explore the perceived experiences of home-based self-training of community-dwelling adults with chronic-stroke and 2) identify factors influencing engagement and adherence to the home-based self-training.
Materials and methods
This qualitative study was conducted at the end of the self-training intervention, as part of a randomized controlled trial [clinical trial number (NCT02393170)],2,13 and was approved by the Chaim Sheba Medical Center Helsinki Committee (SMC-1764-14) and Tel Aviv University's ethics committee. Using a phenomenological method, 14 we explored the subjective experiences of adults with chronic-stroke who participated in the self-training intervention.2,13
Participants
Participants were community-dwelling adults with chronic-stroke (beyond 6 months post-stroke 15 ). The inclusion criteria for this study were similar to the criteria for the randomized controlled trial: 1) Six to 36 months post-stroke, 2) living with a family member or caregiver, 3) moderate to mild weakness of the affected upper-extremity (score 15 to 55 out of a maximum of 66 points on the Fugl-Meyer Motor Assessment) which assesses motor function of the upper-extremity post-stroke, 16 4) without a significant cognitive deficit (Mini-Mental State Examination score >20), 17 and 5) can ambulate independently (with or without an aid). Participants with epilepsy or other neurological conditions, as well as those who were medically unstable (as determined by their family physician), were excluded.
Quantitative tools
In addition to the Fugl-Meyer Assessment and the Mini-Mental State Examination, The Functional Independence Measure 18 was also used to assess independence in 18 activities of basic living, such as eating and dressing. Using an interview format 19 each activity was rated from 1 (total dependent) to 7 (independence). Total score ranges from 18 to 126 points; higher scores indicate more independence. Demographic information (age, sex, years of education) was collected from all participants, as well as information about the stroke (date, side, and type).
Qualitative tools
A qualitative interview guide with open-ended questions (Supplementary 1) was developed by author DR, who is an experienced occupational therapist with expertise in neurological rehabilitation and qualitative research. The guide was constructed to better understand the participants’ experience following the 5-week self-training intervention. Questions inquired about the integration of self-training into their daily routines, motivation to consistently perform (or not perform) the self-training, emotional responses during and after the self-training, and perceived impact on upper-extremity performance and use.
Procedure
As part of the randomized controlled trial, 13 participants in both groups received a home-visit by an occupational therapist who taught them to perform the self-training. Participants were requested to perform the self-training for 1 hour a day for 5 weeks. Participants were asked to log their daily self-training and to send it to the occupational therapist once a week. The videogame group received a videogame console, which was connected to their television and was taught to play games as described in the illustrated manual. Three to five games were selected for each participant by the occupational therapist based on therapeutic relevance. Participants could decide which games to play. The GRASP group received a printed manual and a bag of equipment and was taught to perform different activities (such as buttoning, pouring, and lifting using everyday items such as a towel, a ball, and pegs). After 2 weeks, the occupational therapist conducted another home-visit for all participants, to confirm that the exercises were performed as instructed, address challenges and provide additional guidance as needed. The self-training intervention lasted for 5-weeks but the RCT included another follow-up session, 4-weeks later. For this period, participants were asked to keep the equipment and were told that the continuation of the self-training was optional.
Participants were interviewed immediately following the 5-week intervention so their experiences would be vivid. The interviews were carried out at the rehabilitation center at the end of the post assessment session by one of two occupational therapists, with experience in stroke rehabilitation, who were trained by DR, and were not involved in the delivery of the intervention or in the RCT. All participants provided written consent for the interview to be audiotaped. In cases where participants had mild speech difficulties, a family member joined the interview and assisted in communication.
Quantitative data analysis
Descriptive statistics were performed using SPSS 27. Owing to the small sample, each participant is presented separately, and data are presented as median and interquartile range (IQR).
Qualitative data analysis
The qualitative data were analyzed by the authors [KL, YBK, RM, CL, DR] based on the phenomenological method, 14 which is suitable for exploring a phenomenon (self-training at home) through the subjective experiences of adults with chronic-stroke. The analysis team included PhD-level occupational therapists (KL, DR), PhD students in occupational therapy (YBK, RM), and a PhD-level nurse (CL); all had training and experience in qualitative research.
Each transcript was reviewed for accuracy by at least two authors. The analysis (which was performed manually) included coding and categorizing the content to identify main themes and subthemes that encompassed factors related to self-training. The authors used open coding to identify key elements, followed by axial coding to identify relations between elements, and concluded with selective coding to create proposition themes explaining these relations. 20 During the coding, transcripts were used to form codes or subthemes and to format a codebook with detailed descriptions and interpretations of the data. 21 All codes, themes, code names, and coded passages reached intercoder agreement. 21 Data saturation was discussed toward the end of the data analysis.21,22 Throughout this process, findings were discussed among all the authors to confirm the logical reasoning and to determine the accuracy and credibility of the results and the main themes until a consensus on final themes was achieved.
Results
Participant characteristics
The current data is based on 22 of the 25 participants who consented to be interviewed (63% men), aged 33 to 80 with 6–30 years of education. Participants were 6–36 months post-stroke onset, 59% had a right-sided stroke, and 91% had an ischemic stroke. The participants had preserved cognitive ability (median (IQR) Mini-Mental State Examination score: 29 (27–30)/30 points), moderate upper-extremity motor ability (median (IQR) Fugl-Meyer Motor Assessment score: 41 (29–47)/66 points) and were mostly independent in daily living (median (IQR) Functional Independence Measure: 111 (100–114)/126 points). See Table 1 for the characteristics of each of the participants.
Demographic and stroke characteristics, cognition, motor ability, independence in daily activities and training time for each of the participants (N = 22).
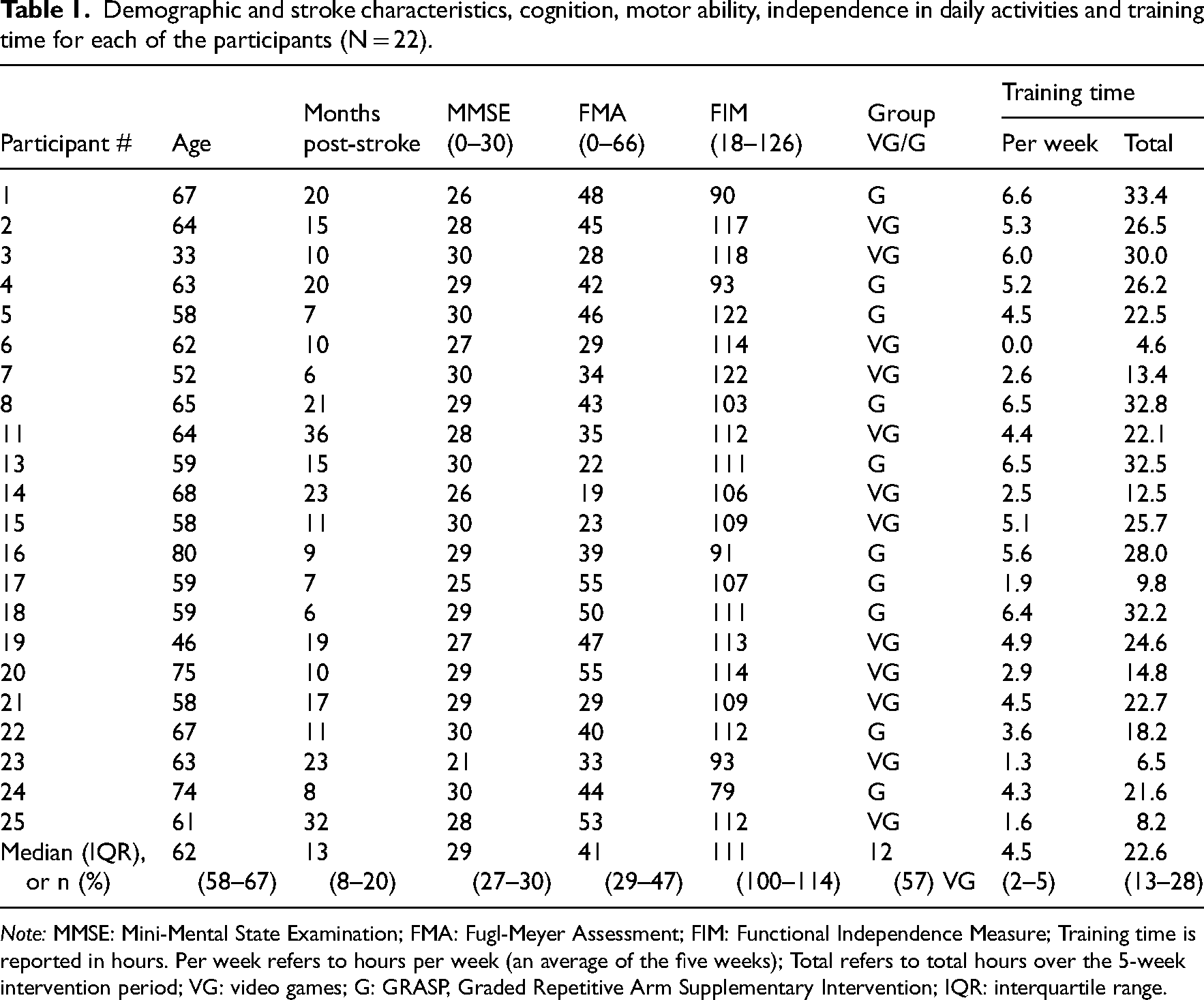
Note: MMSE: Mini-Mental State Examination; FMA: Fugl-Meyer Assessment; FIM: Functional Independence Measure; Training time is reported in hours. Per week refers to hours per week (an average of the five weeks); Total refers to total hours over the 5-week intervention period; VG: video games; G: GRASP, Graded Repetitive Arm Supplementary Intervention; IQR: interquartile range.
Qualitative results
Twenty-two participants (12 from the videogames group and ten from the GRASP group) were interviewed in-person. Three participants preferred to have their spouses present during the interview. The three remaining participants were interviewed via phone because they could not stay for the interview immediately after the assessments. All interviews lasted between 15 and 45 min. Three main themes emerged from the data analysis and reflected the participants’ experiences regarding various factors related to self-training: personal, environmental, and self-training-related factors. Figure 1 illustrates the subthemes and the interplay among these three main themes (factors) associated with the experience of participation in self-training. Below is a detailed description of the themes and subthemes enriched with exemplar quotes from participants—participant # (group – GRASP or videogame) to illustrate their experiences.

Main themes of self-training experience: personal, environmental, and training-related factors.
Personal-related factors
This category identified participants’ personal factors related to self-training and included three subthemes: 1) Devotion to perform self-training, 2) Commitment to the study's team and intervention, and 3) Personal roles.
Devotion to perform self-training—Participants described a strong personal devotion to perform the self-training, often driven by a clear desire to improve their physical function and sense of independence post-stroke. This intrinsic motivation was rooted in a personal commitment to recovery and a belief in the importance of consistency and effort. For many, the self-training became a daily obligation, similar to any other important responsibility. As participant 17 (GRASP) noted: “I wanted to succeed. Look, I wanted to improve the coordination in my hand, and if there were issues with my hand, I wanted to address them.” Participants also described a sense of commitment in maintaining the daily training, despite time pressure and fatigue. For example, participant 5 (GRASP) said: “I knew I committed myself to do an hour [of self-training], and I was fighting against the clock as time passed, but I didn't give up, I didn't cut it short.” Participant 18 (GRASP) emphasized their strong sense of commitment: “I know that I need to do it… I'm committed to do it… I know it will help me maintain my hand.” This overarching theme of devotion highlights how participants internalized the self-training as a meaningful and purposeful part of their rehabilitation, even when it required overcoming personal and logistical challenges.
Commitment to the study's team and intervention—Beyond personal goals, participants also described a strong sense of commitment to the study's team and the structured framework of the intervention. This external source of motivation often reinforced their daily adherence to the self-training routine. The presence and guidance of the occupational therapists, as well as being part of a formal research process, contributed to participants’ sense of obligation and motivation. As participant 5 (GRASP) shared: “It [participation in the research] motivated me to exercise for an hour every day…”. Similarly, participant 17 (GRASP) noted: “Nevertheless, I did it because I felt committed to both [of the OTs in the research team].” This sense of accountability to the team sometimes outweighed internal motivation, especially when the training became challenging or repetitive. However, this external commitment also revealed its limitations. Once the formal study period ended, some participants reported a decline in their training routine. For example, participant 22 (GRASP) reflected: “She [the OT] told me that I can relax, meaning, from now on, I am no longer obligated [as part of the study] to continue the training. I have to admit that since that day, I haven't exercised. But in my mind, there is an intention to return to it…”. These reflections suggest that while structured support can enhance motivation during interventions, additional strategies may be needed to sustain adherence beyond the formal study period.
Personal roles—Some participants found that their involvement in activities related to their roles, such as work or family responsibilities, posed challenges to performing the self-training. Participant 5 (GRASP) described a week where work commitments impacted his self-training, leading him to reduce his engagement due to a busy schedule and lower stress levels: “I was at work, had a busy schedule, I did it but less systematically…”. Participant 14 (videogames) shared how family responsibilities impacted his ability to participate: “In the last ten days, I haven't engaged in any activities because we were not at home; we were babysitting our grandchildren.”
Self-training factors
Two subthemes were identified as self-training factors: 1) The self-training experience and 2) The influence on participants’ general condition.
Factors related to the self-training experience—Participants expressed a sense of enjoyment and satisfaction that they derived from the self-training. Some participants mentioned deriving enjoyment from the animations presented in the videogames, as participant 2 (videogames) said “The commentator/announcer in the game… constantly cheers you on … he talks to you: ‘It's your day'! ‘You're doing something amazing'! … It motivates me to keep going and the graphics are good.” Participant 25 (videogames) added that the “Ping pong game was extremely fun.” Others experienced enjoyment following the self-training even when they felt exhausted: “on one hand, it's exhausting; you get very exhausted, but on the other hand, I feel that it does good, it truly does good.” Participant 15 (videogames) experienced enjoyment and acknowledged that the self-training was beneficial for him: “I think it helped… Yes, I enjoyed it. I really enjoyed it. Every time, I would truly enjoy it.” Others experienced satisfaction from the sense of accomplishment, despite initial challenges in performing the game. For example, participant 3 (videogames) engaged in videogames described initial frustration due to early difficulties, but over time, noticeable improvement brought a strong sense of satisfaction. As expressed by: “On the one hand, I felt frustration when they [the study's team] introduced the game to me, at the beginning I wasn’t successful. On the other hand, I felt a sense of satisfaction because I saw that I was improving, and I persistently kept doing it every day… Overall, a feeling of satisfaction.” However, some participants conveyed negative experiences related to their participation in self-training, including feelings of boredom. As participant 17 (GRASP) said: “There was progress, but [the hand] did not change. There was an improvement, although the fact that the exercises were easy and not challenging somewhat hindered the improvement.” Also, participant 7 (videogames) shared that he did not have enough patience for the self-training, attributing it to boredom: “They [research team] asked me to exercise one hour a day, but this was beyond my patience … it was just boring.”
Some participants highlighted the impact of the presence of others (family members or members of the research team) on their self-training experience. Participant 5 (GRASP) shared that his sister pointed out the improvement in his affected upper-extremity functioning during training sessions by saying that the difference between his two hands is no longer apparent. Thanks to his sister's feedback, he could notice the difference “because maybe it's just a millimeter each day…someone from the outside might be able to see it, but I don't,” but he did feel some change while using his hand in daily activities: “when I pick up a bottle of water, I immediately notice that I'm drinking like this.” Some noted that receiving guidance and supervision from the occupational therapist was perceived as a positive factor impacting engagement in self-training, as participant 3 (videogames) mentioned: “I spoke [to the OT] and we decided that I will do [only] part of the first disc because it was too hard, I did not train for the whole hour.” Participant 17 (GRASP) added that it was “a lot of effort to complete it [the training], and [the OT] tried her best to make me engage in it.”
Factors that influenced participants’ general condition—Within this subcategory, participants shared the outcomes from the self-training, with a primary emphasis on physical aspects. They articulated a range of outcomes experiencing positive, negative, or no change. Some participants reported improvements in the range of motion of their affected upper-extremity following self-training. This enhancement, in turn, facilitated the spontaneous use of their hand in various daily activities. For instance, participant 3 (videogames), a young mother, shared: “Simply, I feel that I'm using my hand more…. There's also an improvement in the hand's quality of movement. In everyday life, I rely more on my hand in what I can do… I lift my baby with both hands…. I am opening doors, carrying grocery bags, and… I feel that I use it [the hand] much more.” Participant 22 (GRASP) provided an example of experiencing improvement and using her hand more spontaneously: “Without intending to, and even not consciously, suddenly I reach my left hand to do things… this means the hand is more active in a more instinctive way… and there are more natural movements.” Other participants shared that the observed improvement enhanced their self-confidence in using their hands, as participant 15 (videogames) stated: “Confidence…, let's say I'm using my hand. Before [the self-training], I was a bit afraid to lift it [the hand], and now I do.“Conversely, others reported negative outcomes which appeared immediately following the self-training session, including pain, fatigue, and an increase in spasticity. Participant 11 (videogames) expressed: “At least from my perspective, shorter periods [of training] with longer breaks seem to decrease the fatigue… these games are exhausting.” Participants 15 (videogames) noted similar outcomes, adding: “Sometimes [training] was exhausting, my hand was shaking …because of the fatigue and effort, the spasticity increased.” Others expressed no change in their condition following the self-training, as said participant 13 (GRASP): “When I don't see improvement, it doesn't give me the desire to continue this research, [despite] all my good will.”
Environment-related factors
In this category, participants highlighted environmental factors that either facilitated or hindered their engagement in the self-training. This encompassed the: 1) Training equipment (for the videogames group), 2) Physical environment of their home, and 3) Family members.
Training equipment—Some participants found the self-explanatory nature of the videogames were easy to engage in self-training, as participant 3 (videogames) said: “The exercise came with an instruction booklet; it was self-explanatory. It's incredibly easy for our generation; there's no problem operating such things (videogames). Additionally, I was familiar with it from the rehabilitation center.” For some participants, family members played a motivating role to encourage the self-training. Participant 17 (videogames) shared that when lacking motivation, discussing this with his sister enhanced his ability to continue adhering to the self-training: “I shared with my sister that it [the training] was not interesting, and she motivated me to cooperate, to keep trying and complete the study.” Similarly, participant 20 (videogames) described the positive outcomes of her husbands’ encouragement to train, even when she felt too tired: “I'm amazed by how I even managed to do it (the exercise) at all. My husband suggested that I try the exercises today. I tried, completing the exercises for about three-quarters of an hour, and felt like a new person.”
The physical environment of their home—Participants also mentioned that their home environment played a role in enabling or hindering self-training. Some of the participants related to the physical space, for example having a large and private area allowed practice whenever and as much as they wanted, as stated by participant 4 (GRASP): “We have a big home, with separate rooms for each of us” and there were participants, who described how the technological equipment takes up a lot of space on the sideboard at home, and this is limiting Participant 7 (videogames).
Family members—The presence and routines of family members significantly influenced participants’ ability to engage in self-training. While some participants received support and encouragement, others found that shared living spaces and family schedules limited their training opportunities. Participants often had to adjust the timing and location of their training based on household dynamics. For example, participant 6 (videogames) shared: “When my son is at work, I could sit in his room, because he has a big TV screen, and it is more comfortable to train there.” Participant 7 (GRASP) described: “We have four televisions at home, but when my son brings his friends over, I can't use the device and can't practice like I usually would.” These insights highlight the importance of considering family routines and home dynamics when designing home-based interventions.
Discussion
This study explored the perceived experiences of home-based self-training among 22 community-dwelling adults with chronic-stroke. 13 The in-depth interviews were conducted after participants had gained rich experience in performing the upper-extremity self-training intervention and by trying to integrate it into their lives. Long-term adherence remains suboptimal 23 and a significant challenge 24 for individuals with chronic-stroke and therefore understanding participants’ experiences is imperative, emphasizing the relevance of this inquiry.
The qualitative analysis revealed three main themes which shaped participants’ experiences of home-based self-training.
Within the personal factors theme, participants with chronic-stroke demonstrated a strong personal commitment to improve their physical abilities through self-training, specifically upper-extremity function. Despite the inherent difficulties and challenges that they encountered during the self-training process, their commitment strongly motivated them to persist with the self-training protocol. This was particularly evident among participants in the GRASP group, who reported less enjoyment, and their engagement was often driven by their strong sense of commitment. Stroke recovery studies emphasize motivation as a key factor for increased training and participation. 25 Indeed, highly motivated patients are prone to reach better recovery compared to patients who have low motivation. 26 While intrinsic motivation is related to joy, commitment, or interest by doing a certain activity, extrinsic motivation occurs when the goal of performing an activity is for receiving an external reward, separate from the activity itself. 26 The self-training was part of a structured research and therefore included constant monitoring and support by the research team, which strengthened the participants’ commitment and enhanced their extrinsic motivation. The use of videogames may have further contributed to extrinsic motivation by providing an enjoyable challenge, immediate feedback, and rewards, acting as an additional external incentive for engagement. Self-management principles, 27 holistic approaches, or a structured framework seems essential for ensuring long-term adherence to rehabilitation interventions in chronic disease management.28,29 Occupational therapists can play a crucial role in ensuring long-term integration of self-training practices with frequent follow-ups and help in integrating the self-training in the individuals’ daily routines.
Among the self-training-related factors, participants highlighted enjoyment and improved physical abilities as the most prominent experiences. Enjoyment is a key factor for ensuring ongoing participation in exercise interventions 29 and can potentially lead to higher engagement in and adherence to self-training.2,13 Notably, participants from the videogames group reported more enjoyment during training sessions compared to the GRASP group. It was therefore not surprising that more participants from the videogames group continued their self-training after the formal intervention period ended, suggesting that videogames, which include interactive visuals, engaging gameplay and immediate feedback, may be a sustainable solution for individuals with chronic-stroke. 13 In contrast, the GRASP's activities, while functionally relevant, lack stimulating or novel elements that reinforce participation. These differences highlight the importance of tailoring self-training strategies not only based on therapeutic goals, but also on the user experience and motivation they elicit. In addition, witnessing physical improvements boosted participants’ adherence and commitment to home-based self-training, even when the training involved discomfort or pain. These factors eased the participants’ physical strain, emphasizing the need to balance the training effort with positive reinforcement. 30
Environmental factors, such as training equipment, physical surroundings, and family involvement, were key facilitators of self-training for individuals with chronic-stroke. Training equipment should be easy to use, accessible and engaging to sustain self-training. Technology and videogames significantly influenced engagement, offering enjoyable experiences when easy to use, but could be overwhelming for those with limited experience or older age. 29 Only a few participants reported technical issues, likely due to the fact the consoles were connected to their television by the occupational therapists who also provided ongoing support, which was essential for promoting adherence 31 and addressing low compliance. 32 The home environment, including space and resources, significantly impacted training effectiveness. Support from others, especially family involvement, was essential for adherence and safety and the shared spaces and use of the television required mutual consideration from family members. A pre-intervention home-visit or video consultation is recommended to assess and adapt the environment as needed and to guide the family members. With less motivated participants, clinicians should set goals to enhance motivation, involve family support, and provide follow-up as needed.
The study used in-depth interviews to gather detailed information regarding the experiences from a relatively large sample, notable for a qualitative study. Some interviews were conducted with the presence of a family member who assisted when needed, allowing to interview all participants. The interviews, which were conducted post-intervention, provided comprehensive insights into participants’ full self-training experience. This approach enabled to include a broader and more representative range of experiences while maintaining the integrity of the data collection process. The inclusion of two distinct types of self-training (videogames and GRASP) allowed for some comparison of how different self-training modalities may influence engagement, adherence, and satisfaction. Participants were randomized into the groups, and they did not choose the modality of the self-training. Future studies can perhaps allow participants to choose their preferred modality, which might impact their adherence. The sample may not reflect the broader chronic-stroke population, because of the inclusion criteria of preserved cognitive function, moderate upper-extremity impairment, and family support. Individuals who live alone may not be able to participate in self-training programs and might need the therapist's support. In addition, we only included participants who participated in the RCT, which required an initial level of motivation.
In conclusion, this qualitative study provided a deeper understanding of the self-training process, revealing how internal and external motivation interact to influence long-term adherence. In addition, environment-related factors and self-training-related factors also played an important role in shaping engagement. Clinicians should consider addressing these factors when supporting sustained engagement in self-training interventions post-stroke.
Fostering a sense of commitment in individuals with stroke (to achieve personal goals and towards their therapist) is important to promote adherence to self-training programs. To promote adherence to home-based self-training, it is recommended to assess and adapt the home environment, provide user-friendly training equipment, and actively involve family members as supporters in the home-based intervention. On-going monitoring by health professionals can serve as a source of external motivation, ensuring long-term adherence and helping individuals integrate self-training into their daily routines.Clinical messages
Supplemental Material
sj-docx-1-cre-10.1177_02692155251344850 - Supplemental material for Home-based self-training: A qualitative exploration of the experiences of individuals with chronic-stroke
Supplemental material, sj-docx-1-cre-10.1177_02692155251344850 for Home-based self-training: A qualitative exploration of the experiences of individuals with chronic-stroke by Khawla Loubani, Yishai Bachar Kirshenboim, Ruth Maman, Chedva Levin and Debbie Rand in Clinical Rehabilitation
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.