
Abstract
Objective
The World Health Organization's Rehabilitation 2030 initiative represents a new strategic direction for the worldwide rehabilitation community and their Rehabilitation Competency Framework (RCF) was designed to describe the requirements of a rehabilitation workforce. This study aimed to identify and review global physiotherapy competencies and explore their congruence with the WHO-RCF.
Design
A document review and thematic analysis were conducted on competency documents sourced from World Physiotherapy member countries.
Methods
A three-pronged search strategy was used to identify physiotherapy competencies in all World Physiotherapy members that were listed on their website at the time of the study. All competency statements identified were sorted using the definitions of the five domains of the WHO-RCF. A desktop inductive thematic analysis of competencies was conducted to derive a conceptual framework for future competency framework development.
Results
Two thousand and one competency statements were extracted from 20 documents, all accommodated within the WHO-RCF. From the dataset, a conceptual framework was developed consisting of 17 themes and 59 sub-themes across five domains. Technological competence, entrepreneurship and broader competencies to advance the social justice agenda were identified as gaps.
Conclusion
To promote homogeneity, it is recommended that all rehabilitation professionals utilise a similar methodology using the WHO-RCF to develop future frameworks that are contextually relevant. Competencies needed for change in support of equitable access and better health for all should be included.
Keywords
Introduction
Health is not merely the absence of disease but involves an individual's overall wellbeing and optimal functioning on multiple levels. 1 However, healthcare often operates in silos, with various rehabilitation professions like physiotherapy, occupational therapy, and speech therapy working independently. 2 This approach has made access to specialised medicine and rehabilitation increasingly expensive and inaccessible to many.3,4 Despite advances in healthcare and a shift towards interdisciplinary collaboration, these efforts have done little to alleviate poor health and its burden on healthcare systems, nor have they addressed the growing disparities in access to quality care.4–8 Consequently, health needs often go unmet, especially in lower socioeconomic settings.9–13 It is evident that health professionals need to develop competencies that can drive change in their approach to poor health and existing health systems.
Competency frameworks have been established globally to guide service planning, set practice standards, and inform professional training. However, these frameworks have had a limited impact on improving quality of life. 14 They often exhibit disparate terminologies and conceptual understandings, making it challenging to apply them across different locations, specialisations, and professions.15,16 Some argue that these frameworks perpetuate fragmentation in healthcare rather than fostering a collaborative, transdisciplinary approach.
In response, the World Health Organization (WHO) launched the Rehabilitation 2030 initiative, promoting the development of new healthcare roles, task shifting, and skills mixing.17,18 As part of this initiative, the WHO published the Rehabilitation Competency Framework (WHO-RCF) to determine the needs and plans for the rehabilitation workforce in various settings. 19 The WHO-RCF defines five central domains for rehabilitation professionals: Practice, Professionalism, Learning and Development, Management and Leadership, and Research. 19
While collaboration and task-sharing among rehabilitation professionals can strengthen health systems, some caution that it should not be viewed as a panacea for all healthcare issues.20,21 The critical question is whether the physiotherapy profession is adequately guided and equips future healthcare professionals with the necessary competencies to advance the social justice agenda. Specifically, are we training graduates capable of making a meaningful impact on the health of the communities in which they practice?5,22,23
This study aimed to explore the alignment between documented physiotherapy competencies and those outlined in the WHO-RCF to guide the development of future rehabilitation professional competency frameworks. The objectives were to identify physiotherapy competencies reported in profession-specific documents and develop a conceptual framework based on the WHO-RCF structure.
Methods
A document review and thematic analysis were conducted on competency documents sourced from World Physiotherapy member countries. World Physiotherapy is the largest and probably the most recognised international voice for physiotherapy and represents more than 660,000 physiotherapists worldwide through its 125 member organisations. 24 To become a World Physiotherapy member, a national physiotherapy association must meet specific criteria defined in World Physiotherapy's Constitution. Membership provides access to shared resources, including competency frameworks and practice standard documents. Inductive thematic analysis of all competency statements extracted from these documents was conducted to identify core themes within each of the five domains of the WHO-RCF.
A three-pronged search strategy was used to identify physiotherapy competencies: (i) all World Physiotherapy members (n = 125) that were listed on their website at the time of the study (2022/2023) were emailed and requested a copy or access to any competency documents, if available; (ii) relevant member websites from these countries were also searched (non-English websites were screened with the translation functionality of the web browser (Google Chrome)) and (iii) for each World Physiotherapy member country, a Google search was conducted using the main keywords “country name” + “physiotherapy” OR “physical therapy” + “competency” + “competencies”. To be included in this study, all documents sourced were evaluated against specific criteria. Only official publications that contained organised statements on physiotherapy competencies and that presented authentic logos and publication details were included. All formats or layouts of these professional documents were considered, as well as all languages. Google Translate was used to translate non-English documents, and English versions were emailed back to host organisations to validate the translations. All publication dates were included. This review did not include draft versions and documents developed for sub-specialities or extended scopes of practice. Where an older document version existed, it was also excluded.
As this study involved a secondary analysis of existing data, no ethical approval was sought. Where documents were not available on public sites, the willingness to share information was deemed approval for inclusion of their documents in this study. All data sources were anonymised when competency statements were analysed.
All identified documents were imported to Altas.ti (V22) software. The primary investigator read through all the documents, including annexes. All competency statements in each document were then extracted and exported individually to Microsoft Excel for sorting and further analysis. As the primary investigator was familiar with the various texts at this point, all source identifiers were hidden to avoid bias in further steps.
The primary investigator reviewed each competency statement and using the definitions for the five domains of the WHO-RCF, 19 assigned it to the most appropriate domain. To prevent the same statement from appearing in several domains, each statement (or part of a statement) was only assigned to one of the five domains. Forty percent of all statements were then randomly selected by two other members of the research team (20% each) to check for appropriate domain allocation. The researchers discussed any allocation discrepancies by referring to the domain definitions. Systematic errors were identified through this process, and the primary investigator re-allocated competency statements accordingly. A few duplicate statements were also identified through this process and were deleted. The two team members again repeated their review and repeated this process until all members agreed to the final datasets.
Each of the five domains of the WHO-RCF with its dataset was exported to its sheet and transferred back into Atlas.ti (v22) for further thematic analysis. The primary investigator used an inductive approach as described by Braun and Clarke 25 and identified dominant themes within each WHO-RCF domain. The two co-researchers who also reviewed the statement allocation reviewed the themes identified, and where discrepancies arose, the team discussed them until a consensus was reached. The final themes and their descriptors were then used to design a conceptual framework that could be used for further competency framework development.
Trustworthiness
The research team made several attempts to ensure the trustworthiness of the data: strict inclusion criteria were applied to ensure the documents’ authenticity, representativeness and credibility. To validate the primary investigator's coding and analysis, investigator triangulation was applied, and the co-researchers reviewed the data on different points, as discussed above. The researchers aimed to provide a ‘thick description’ of the context of the study and the documents to enable transferability judgement from readers without assumptions having to be made. Iterative data collection and analysis, saturation, rigorous procedures and multiple reviewers all contributed to the dependability of the results. Finally, the research process and findings were recorded and described in detail to ensure the repeatability and confirmability of the study. 26
Results
The search strategy identified 59 potential documents. The documents sourced from associations in Belgium, Colombia, Costa Rica, Denmark, France, Germany, Latvia, the Netherlands, Portugal and Switzerland were translated using Google (Chrome) Translate. Not all associations commented or replied to the translated versions, but no association objected to us using the English-translated version in this document review. Based on the outcome of those who had no objection to their translated version, the review team concluded that it was essential to include all translations to avoid potential bias. After removing duplicates, 31 documents were screened according to the inclusion criteria. Eleven documents were further excluded: six documents (n = 6) did not describe physiotherapy competencies, two documents (n = 2) were created for a sub-specialty of physiotherapy, one document (n = 1) was an unpublished/draft version and two documents (n = 2) were older versions of documents already included (Figure 1).
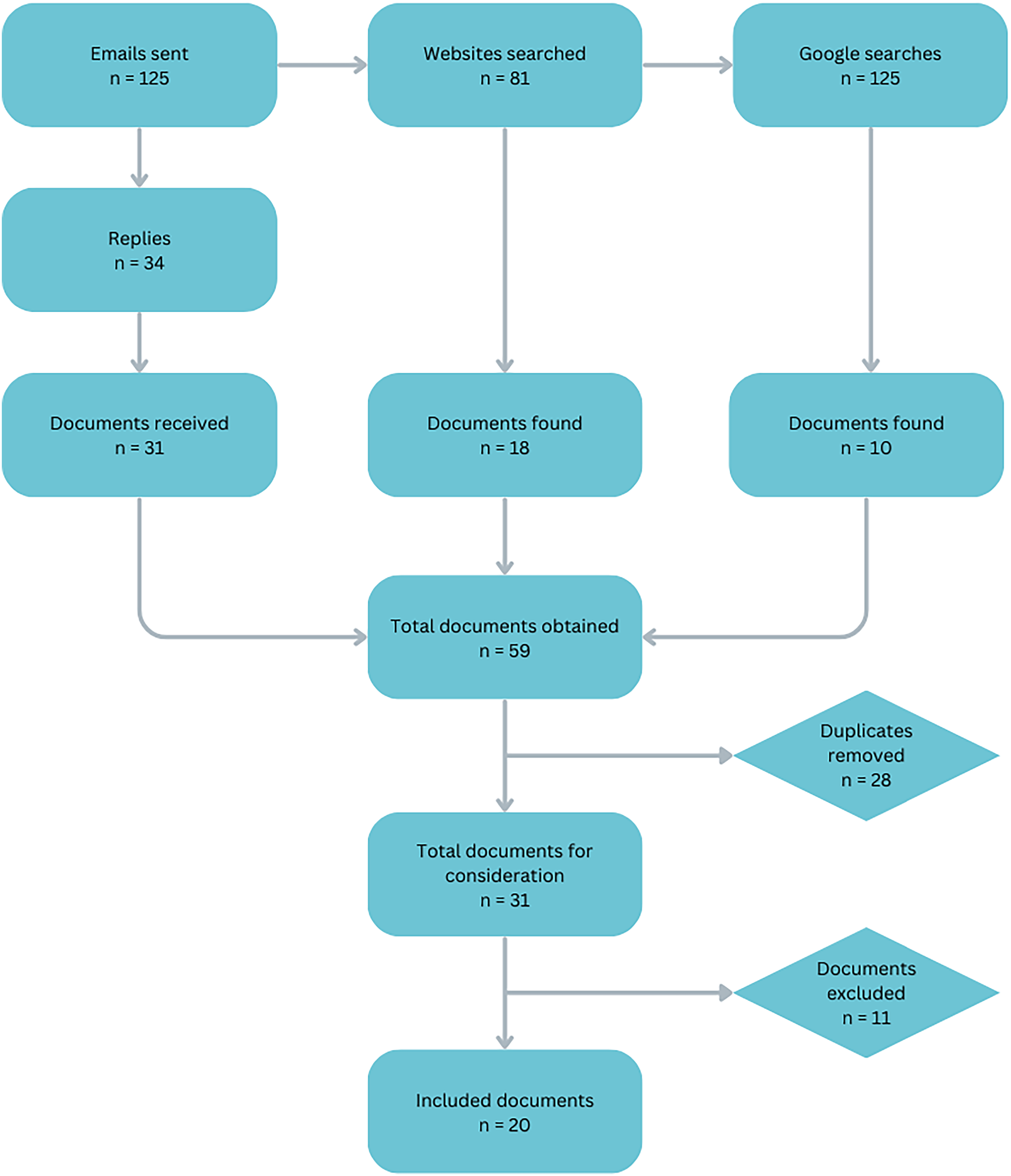
Summary of results from the search strategy.
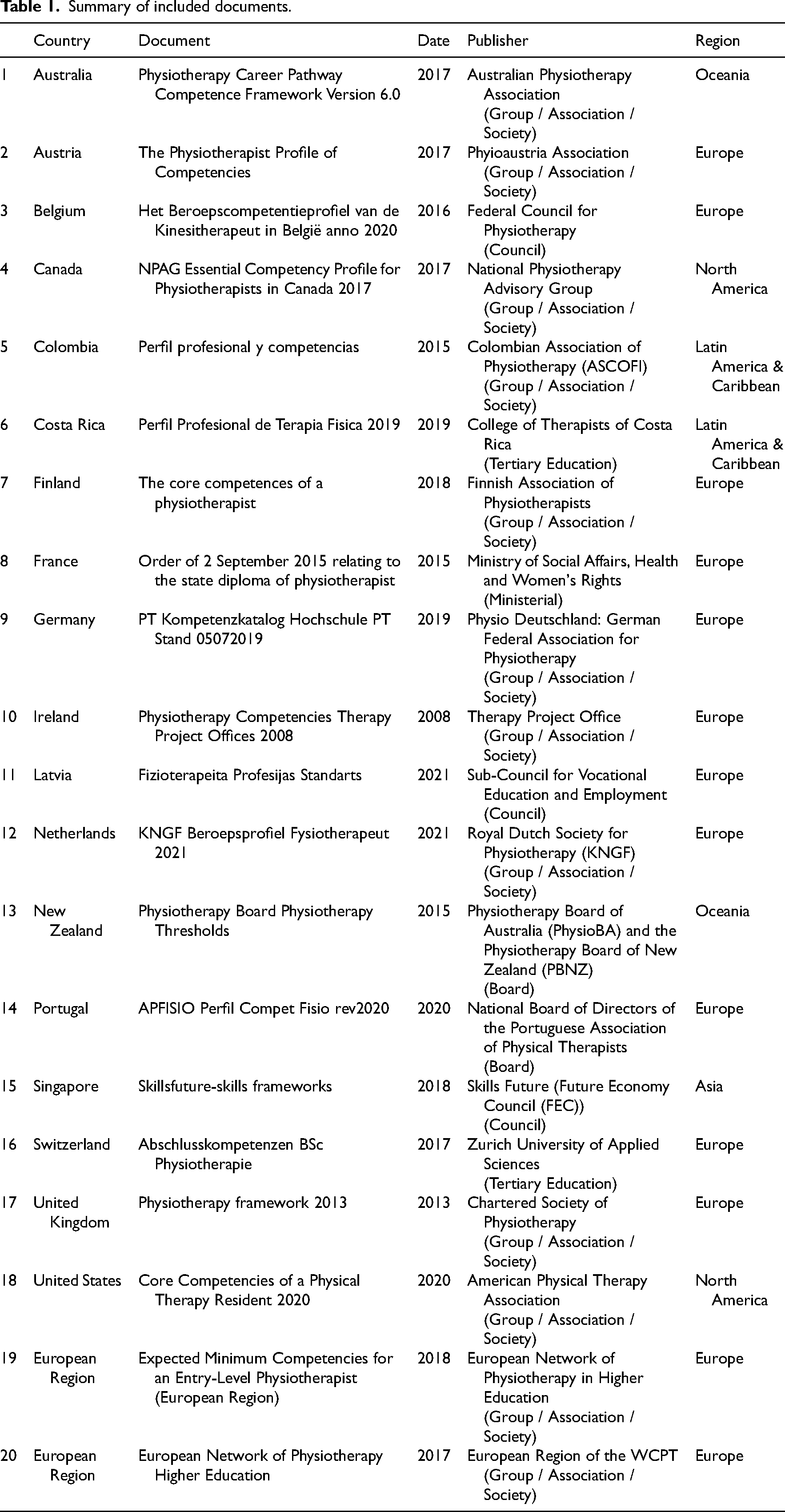
A total of 20 documents were included in this study, of which 18 were country-specific and two were regional (European region) (Table 1). Thirteen documents came from Europe, two from Oceania, two from North America, two from Latin America and the Caribbean, and one from Asia. No documents were found from the African continent.
Summary of included documents.
From the 20 documents included in this review, 2001 individual competency statements were identified and allocated to one of the WHO-RCF's five domains. As depicted in Figure 2, main themes and sub-themes were identified for each domain.
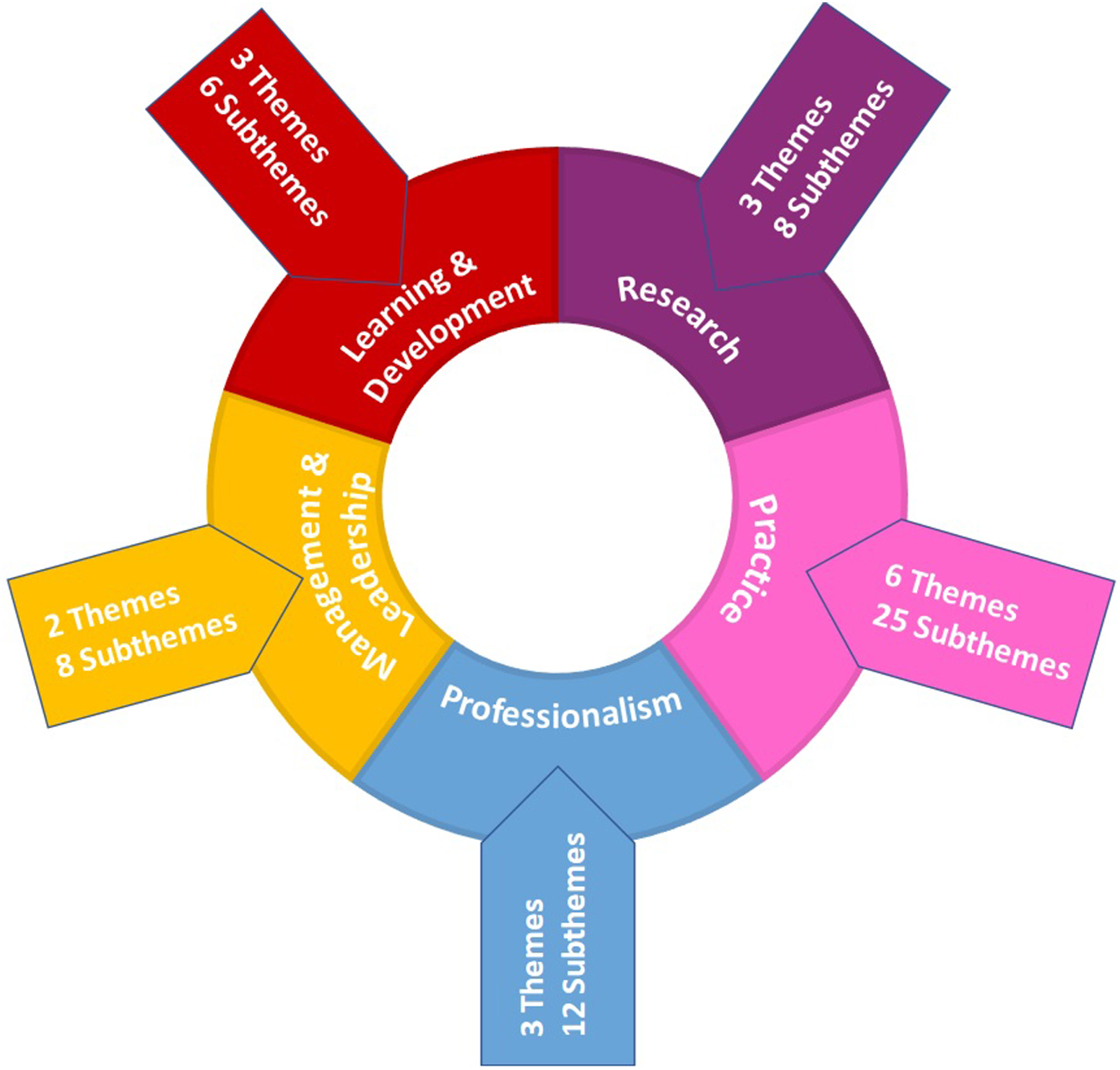
Summary: number of themes and sub-themes per World Health Organization Rehabilitation Competency Framework domain.
Eight hundred eighty-two statements related to the Practice domain, the most densely described domain, with 6 themes and 25 sub-themes emerging (Figure 3). The statements mainly described client interactions and the physiotherapeutic procedure across the continuum of care, including the documentation thereof. Respect for clients and their rights and safety is emphasised.
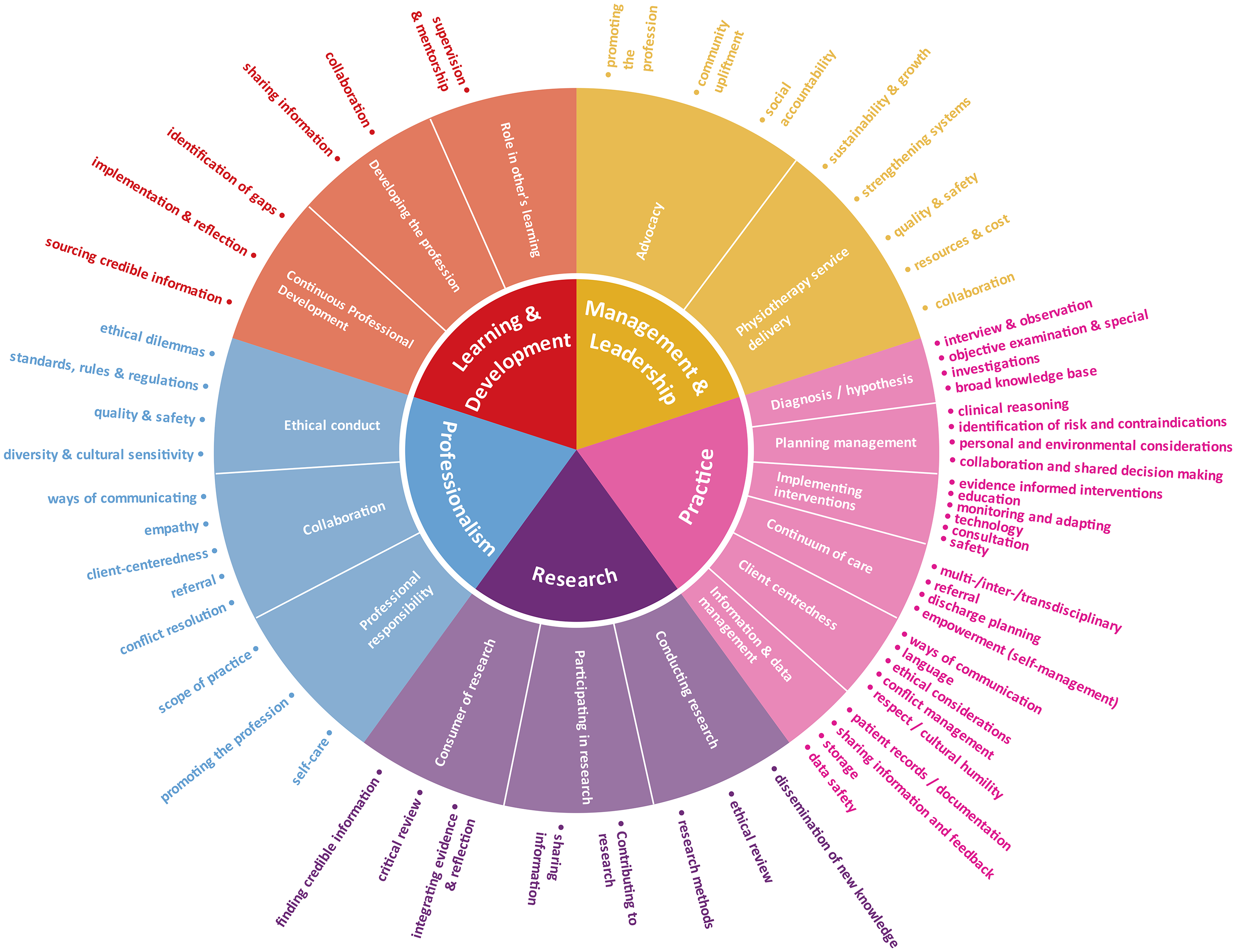
Conceptual framework of competencies derived from a synthesis of globally reported physiotherapy competencies.
The Professionalism domain contained 488 statements, from which 3 themes and 12 sub-themes emerged (Figure 3). This domain refers to ideas such as professional integrity, safety and quality of care, as well as factors enabling the performance of a professional role. Patient-centredness and empathy are described in this domain, as is the notion of self-care.
Two hundred and sixteen statements were analysed in Learning and Development. Six themes and three sub-themes could be easily distinguished, as statements were similar and focused (Figure 3). Self-development and growth and keeping up to date with current advances were dominant, but this domain also emphasises practitioners’ responsibility towards the profession.
Three themes and 8 sub-themes emerged from analysing 100 statements allocated to the Research domain (Figure 3). These statements revealed that physiotherapy must demonstrate its legitimacy through research that supports its efficacy, helps to improve healthcare, and develops the field. The scholarship of physiotherapy is emphasised here and suggests support of, as well as participation in, research and the dissemination of novel/new understandings and practice.
Two themes and 8 sub-themes were derived from the 315 statements in the Management and Leadership domain. Although the terms ‘management’ and ‘leadership’ were used interchangeably, the two overarching themes identified in this domain related to advocacy (leadership) and service delivery (management) (Figure 3), more specifically towards health promotion and community upliftment. Recognition of physiotherapy's accountability towards society is evident in this domain.
Discussion
The purpose of this study was to collate documented physiotherapy competencies and align them with those of the WHO's RCF to assist in guiding future rehabilitation professional competency framework development. All 2001 competency statements could be ‘accommodated’ within the five domains of the WHO-RCF. This study further evidences that physiotherapy competencies described across the globe align with those defined by the WHO required for an effective rehabilitation workforce. 19 The conceptual framework emanating from this study demonstrates an appreciation of physiotherapy's autonomy while simultaneously recognising that collaborating with other healthcare professionals with the patient at the centre is key. Furthermore, the framework highlights the various roles physiotherapists play, and their work extends beyond just treating patients’ pain and movement disorders. Although not an explicit aim of this study, it has inadvertently identified gaps in existing physiotherapy frameworks.
In the ever-changing healthcare landscape, rehabilitation professionals, including physiotherapists, will continuously need to develop competencies beyond clinical competence that overlap with other health professions and/or practitioners to meet these challenges.5,6,27 The purpose of using the WHO-RCF to develop this (harmonised) conceptual physiotherapy competency framework was to ensure uniform professional standards aligned with other rehabilitation professions and thereby promote workforce mobility towards providing rehabilitation services to previously underserved areas of society.10,15,21,28–31
The results of this study demonstrated that although physiotherapy does report competencies in all domains of the WHO-RCF, the focus on the ‘Practice’ domain is dominant, demonstrating an appreciation for the discipline's conceptual and procedural knowledge, skills and attributes. However, given that these frameworks are used to inform undergraduate training programmes, this may negatively impact the profession's transformational role in influencing health systems outside their clinical (discipline) practice roles. Most undergraduate physiotherapy training programmes, however, span of 3 to 4 years, leaving little time to develop critical skills, including providing enough opportunities for students to examine existing (own) biases, often needed to transform into reflective and responsive practitioners.
Although not an explicit aim of this study, the document review also illustrated the absence or weakness related to competencies students need to shape the future we strive for. Irrespective of profession, the Organisation for Economic Cooperation and Development (OECD) describes three transformative competencies, namely creating new value (curiosity, collaboration, and thinking ‘out of the box’ to find innovative solutions), reconciling tensions and dilemmas (becoming comfortable with not knowing) and taking responsibility for their actions. 32 The challenge facing undergraduate health professions training programmes is to develop these competencies without neglecting discipline-specific or clinical skills competence. 8 However, all disciplines and specialisations should consider emerging interprofessional competency frameworks that support collaborative healthcare delivery when renewing their curricula.
Another gap in physiotherapy competencies, and likely in other health professions’ frameworks, is the limited reference to technical competence. Technology can enhance clinical competence but can also significantly improve how we communicate with others. 33 Being able to communicate in a way (language or otherwise) is central to better understanding the patient and the health condition he/she may present with. 34 Technological advances have the potential to strengthen the health system and provide a platform to extend our reach, especially in resource-constrained settings. 35 The same is true for artificial intelligence despite the current concern that this poses to compassion in healthcare. 36
This study found that the physiotherapy competencies, as described by various countries across the globe, can be accommodated within the five domains of the WHO-RCF. This study is the first step in developing a united front within the rehabilitation professions. Undertaking a similar methodology, other rehabilitation professionals should reconceptualise their discipline-specific competency frameworks using the WHO-RCF. Harmonised terminologies and an understanding of critical concepts in rehabilitation will foster collaboration in care and future research. Working together will assist in task-shifting and training others in various contexts.
Strengths and Limitations
This study offers a synthesis of physiotherapy competencies and provides a conceptual framework for any setting to develop contextually relevant physiotherapy competency frameworks. However, it needs to be interpreted within the context of its limitations. The search strategy was based on data available from World Physiotherapy at the time (2022/2023) and included 125 countries. Non-member countries were thus excluded from this study. Similarly, given that physiotherapy is regulated in many, if not most, countries, the regulatory authorities were not approached, nor were training institutions. The latter was purposefully not included as many higher educational institutions have academic autonomy, and curricula may differ across these institutions and not represent their country. Alternative search strategies such as snowballing and inclusion of regulatory authorities such as health professional councils or boards should be considered.
One of the challenges in reviewing similar documents developed by different authors for different environments, economics, and other factors was dealing with the overlap of competencies across domains. Many statements ‘fitted’ into two or even three domains, and the researchers finally agreed to split statements if necessary to better fit in a respective domain or domains.
A notable language barrier was experienced when identifying relevant documents. Because of the study's time and budget constraints, the researchers could not employ a professional translator, so Google Translate was used where documents were unavailable in English. Despite most countries providing us with English versions, it was evident that English was not their first language, which sometimes made interpretation of some of the statements difficult.
Clinical messages
The described physiotherapy competencies are congruent with the WHO-RCF.
Broader competencies must be included in rehabilitation professional competency frameworks to affect change and ensure equitable access for all.
The summarised competencies from this study can be used as a guiding framework for developing contextually relevant competency frameworks for physiotherapy.
Footnotes
Author Contributions
MM, MU, and SH contributed to the study design. MM completed the search strategy, analysed data and drafted the manuscript. MU and SH contributed to the quality appraisal and review processes. All authors contributed to revising the manuscript and approving the final manuscript.
Consent for Publication
All authors have approved this manuscript for publication. This manuscript has not previously been published and is not pending publication elsewhere.
Data Availability
The authors will make the raw data supporting this article's conclusions available without undue reservation.
Declaration of Conflicting Interest
The authors declare no potential conflicts of interest for this article's research, authorship, and publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.