
Abstract
Objective
To investigate the effectiveness of a Pilates exercise program compared with home-based exercises in individuals with chronic non-specific low back pain.
Design
A randomised controlled trial with a six-month follow-up.
Setting
Rehabilitation clinic.
Participants
One hundred and forty-five individuals (18–50 years of age) with low back pain for ≥ 12 consecutive weeks were enrolled and randomly allocated to either Pilates (n = 72) or home-based exercise groups (n = 73).
Interventions
Method Pilates (Mat Pilates exercises using accessories) versus home-based exercise (postural exercises, muscle stretching and strengthening, and spine stabilisation/mobilisation), twice a week, for 6 weeks.
Main measures
Assessments were performed at baseline, post-intervention, and six months follow-up. Outcomes were pain intensity, disability, and health-related quality of life.
Results
At post-intervention, the Pilates group had significantly lower pain intensity (mean difference = −1.14; 95% CI −2.05; −0.23), less disability (mean difference = −6.7; 95% CI −11.3; −2.0), and higher health-related quality of life (mean difference = 0.102; 95% CI 0.054; 0151) compared to the home-based exercise group. At follow-up, the Pilates group had a significantly higher health-related quality of life (mean difference = 0.055; 95% CI 0.003; 0.106) compared with the home-based exercise group but there were no significant differences in pain and disability. A significant overall effect of Pilates compared to home-based exercise was found for disability (mean difference = −4.4; 95% CI −7.6; −1.1), and health-related quality of life (mean difference = 0.049; 95% CI 0.022; 0.076), but not for pain.
Conclusion
Although Pilates was significantly superior to home exercise for pain and disability, the differences were not considered clinically relevant. However, Pilates did provide significant and clinically relevant differences in utility.
Introduction
One of the most widespread musculoskeletal disorders worldwide is low back pain. Defined as persistent pain for more than 12 weeks with no clear cause, chronic non-specific low back pain is considered one of the most frequent reasons for disability and absenteeism worldwide.1,2 In addition, people with chronic non-specific low back pain are frequent users of health services. 3 The most commonly used strategy to manage this condition is exercise, which is recognised as beneficial for people with chronic non-specific low back pain and is the most prescribed intervention worldwide. 4
Exercise programs prioritising muscle strengthening and spinal stabilisation, such as Pilates,5,6 have gained considerable recognition in recent years and are being used as a first-line treatment option for chronic non-specific low back pain in primary care. 7 Studies have shown promising results on the effectiveness of Pilates in improving pain levels, disability, and quality of life in individuals with chronic non-specific low back pain.8–10 Furthermore, exercise performed at home has been considered as a treatment option for chronic non-specific low back pain as evidence has shown it to be beneficial for pain relief and functionality. 11
Despite the potential benefits of exercise therapies for chronic non-specific low back pain, systematic reviews have highlighted the need for further high-quality evidence regarding the effectiveness of Pilates and home-based exercises.5,12,13 Moreover, studies comparing the effectiveness of both exercise therapies are still scarce. 14 Therefore, the aim of this study was to compare the effectiveness of Pilates versus home-based exercises in individuals with chronic non-specific low back pain immediately after interventions and at six-month follow-up, in terms of pain intensity, disability, and health-related quality of life. It is hypothesised that Pilates would be more effective than home-based exercises.
Method
Study design
A randomised controlled trial was performed in which Pilates was compared to home-based exercises in individuals with chronic non-specific low back pain with a six-month follow-up. The study was conducted in a clinical setting in the city of Brasília, Brazil. This study was approved by the Ethics Committee (Campus UnB Ceilândia, protocol n. 2.163.607) and registered at ClinicalTrials.gov (NCT03113292). This randomised controlled trial was reported according to the CONSORT statement. 15
Setting and participants
The use of exercises for chronic non-specific low back pain has been a health policy of the Brazilian Ministry of Health since 2008. 7 However, Pilates is currently not officially included in the treatment options provided by public health services in Brazil.
Participants were eligible if they met the following criteria: (1) male or female gender (18–50 years of age); (2) chronic non-specific low back pain for more than 12 consecutive weeks before entering the study; (3) not having attended Pilates or physiotherapy interventions for low back pain for at least six months prior to enrolment. Participants were excluded if they presented: (1) history of trauma or fractures of the spine; (2) diagnosis of spine osteoarthritis, disc herniation, or spondylolisthesis; (3) self-reported referred pain (e.g. visceral, appendicitis, abdominal and pelvic surgeries); (4) previous spinal surgery; (5) root symptoms (e.g. sciatica and cauda equina syndrome), classified as levels three and four; and (6) pregnancy.
Description of the interventions
Pilates
The Pilates method was supervised face-to-face by a certified and experienced physiotherapist and Pilates instructor, with expertise in the prescription of exercises. The program consisted of Mat Pilates using accessories (Table 1). In the first two sessions (one week after randomisation), participants received instructions about the method and went through a familiarisation (i.e., a brief explanation of the exercise technique and concepts of Pilates). After the familiarisation, the six-week intervention started. There were two sessions per week, and 50 minutes long, with a maximum of four participants per session, including seven to ten exercises. For each exercise, two series of eight to 12 repetitions were adopted, according to the ability of each participant. When required, exercises were adapted and modified individually considering the three difficulty levels used in Pilates: basic, intermediate, and advanced. Exercises were based on Pilates principles, that is, (1) breathing (body coordination during the inspiratory and expiratory phase and deep muscle activation); (2) axial elongation and core control; (3) segmental mobilisation and spine stabilisation; (4) positioning of the head, neck, and shoulders; (5) weight-bearing and extremity alignment; (6) motor learning with refinement and coordination.
Description of the prescribed exercises and progression aims (stages).
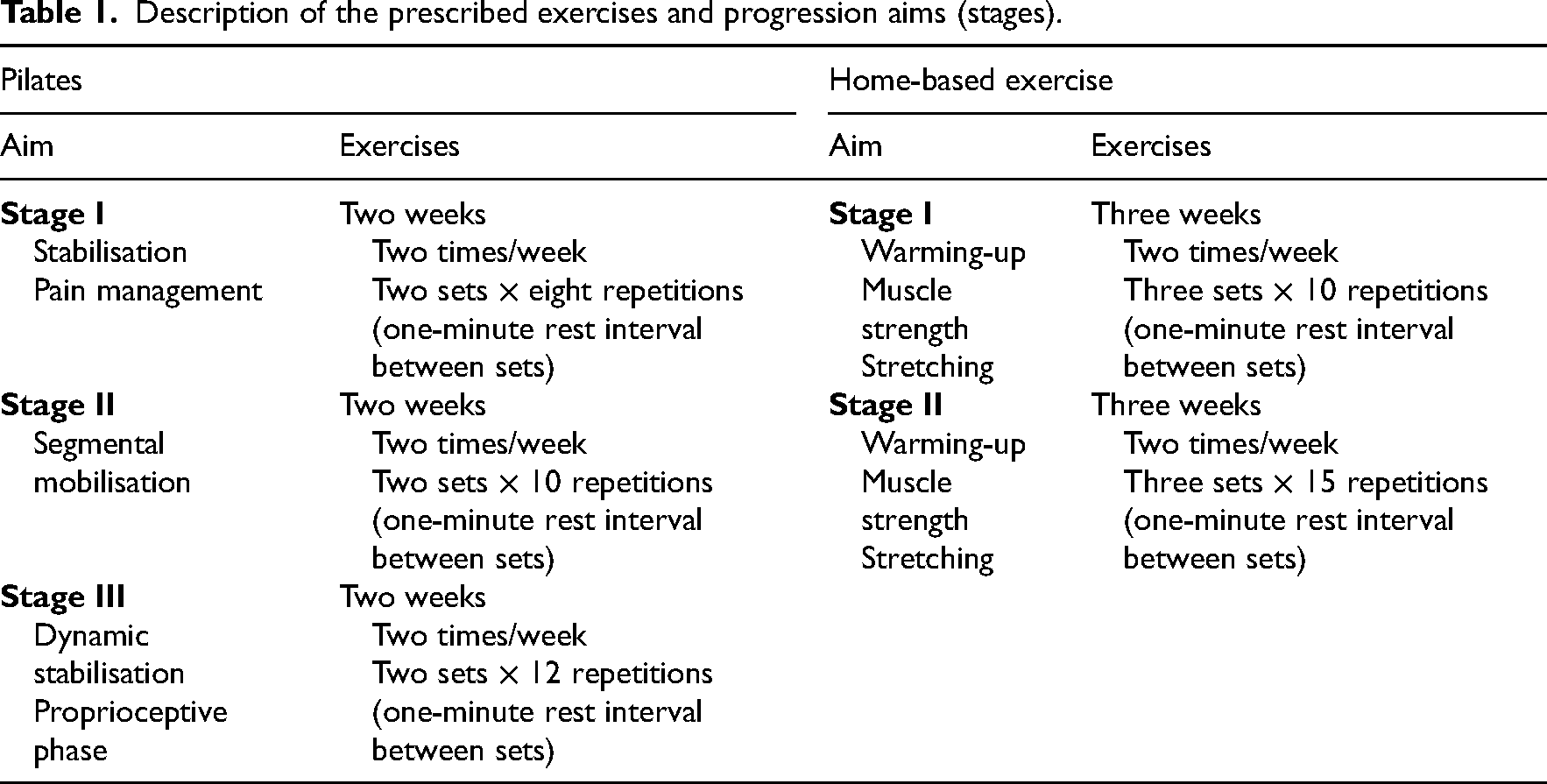
Further details of the Pilates exercises can be found in Supplementary Table S4.
Home-based exercise
The home-based exercise was supervised by another experienced physiotherapist. Initially, two face-to-face familiarisation sessions were held (one week after randomisation). The intervention was composed of general exercises (postural exercises, muscle stretching and strengthening, and spine stabilisation/mobilisation), prescribed twice a week with 50-minute sessions (Table 1). Participants received a booklet containing the exercise description, series and repetitions, and safety issues to be alert for during sessions. The progression was held face-to-face at halfway through the intervention period (3 weeks), in which participants were presented with more challenging exercise variations by changing body position (e.g. variation in arm levers and range of motion). Progression occurred in the absence of postural compensation and correct technique when performing the minimum number of repetitions. The difficulty level was determined individually. During the intervention, all participants were instructed to use a printed exercise sheet to monitor exercise performance, and adherence/compliance, and to report possible adverse effects. Participants were also contacted weekly via email and/or text message for supervision as well as monitoring adverse effects and adherence to the intervention. During the weekly message, the physiotherapist asked about adherence and whether participants performed the exercises as instructed, and sent messages with reminders about the importance of performing the exercises.
Participants of both groups were instructed to take their usual medication, and this information was monitored during post-intervention re-evaluations.
Outcomes measures
The primary outcome measures were pain intensity and disability. Secondary outcome measures were health-related quality of life and perceived recovery. Participants were assessed at baseline; post-intervention (i.e. immediately after the completion of the intervention); and 6 months post-intervention (follow-up).
Pain intensity was measured by the Numerical Rating Scale. This scale consists of numbers ranging from zero to 10, where zero is equivalent to no pain and ten to the worst possible pain. Participants were instructed to mark the number representing the intensity of their pain in the last week. Disability was assessed using the Brazilian version of the Quebec Back Pain Disability Scale Questionnaire, 16 which assesses the difficulty in performing routine activities through 20 questions. The final score is obtained by summing the responses and ranges from zero to 100. The higher the score, the greater the level of disability. Health-related quality of life was measured using the validated version of the EuroQol-5D-3L questionnaire for the Brazilian population. Participants described their health state based on five health dimensions (i.e. mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) and three response levels (i.e. no problems, some problems, and extreme problems). Subsequently, health states were converted into utility values ranging from −0.176 to 1 (perfect health) using the Brazilian tariffs. 17 For the assessment of perceived recovery, the Global Perceived Effect Scale, which contains a Likert-scale of 11 points, was applied. The scale is divided into categories ranging from −5 (‘much worse’), 0 (‘no change’), to 5 (‘completely recovered’). 18
Baseline measurements
The following variables were collected at baseline to characterise the participants: age, gender, body mass index, kinesiophobia, and dynamic balance (Y-balance test). Further details on the kinesiophobia measurements can be found in the validation study. 19 In brief, we used the Brazilian version of the Tampa scale, in which scores range from 17 to 68, and the higher the score, the worse the kinesiophobia. The Y-balance test was used to evaluate dynamic balance, that is, the displacement of the lower limbs in anterior, posteromedial, and posterolateral directions. The average scores of three attempts in each direction were used in the analysis, representing an index of dynamic postural control (presented as a percentage). Details can be found elsewhere. 20 The risk of worst prognosis of low back pain was assessed using the Brazilian version of the STartBack Screening Tool, in which scores range from 0 to 9 (worst score), and can be classified as low risk (good prognosis), medium (less-favourable prognosis), and high risk (unfavourable prognosis). 21
Randomisation and blinding
Participants were recruited at rehabilitation clinics, and at health units located in the city of Brasília, Brazil. Participants who agreed to participate signed the informed consent, and underwent baseline measurements, after which they were randomly assigned into one of two groups in a 1:1 ratio: (1) Pilates or (2) home-based exercises. For the randomisation procedure, we used a random numbers table (random.com). The allocation was concealed by using opaque and sealed envelopes containing cards with the names of each intervention. This procedure was performed by an independent researcher who was not aware of the aims and study's procedures.
A trained assessor who was unaware of the group allocation performed the interviews to collect the outcome measures (blind assessor). All outcome measures were self-reported (scales and questionnaires). Statistical analysis was also performed by an evaluator who was blind to the group allocation, by receiving the numerically coded data set (groups/individuals). It was not possible to blind the therapist and participants due to the nature of the intervention. More detailed information can be found in the study protocol. 22
Sample size
The sample size calculation is detailed elsewhere. 22 Briefly, we used the OpenEPI software, 23 considering a statistical power of 80% and an alpha of 5% to detect the difference in pain intensity and disability between Pilates and home-based exercise groups equivalent to mean differences from previous studies. The mean decrease in pain intensity and standard deviation of the Pilates (3.30 ± 2.30) and the home-based exercise (2.15 ± 1.99) were based, respectively, on data from a previous study, 24 and a pilot study. The mean disability and SD were based on a pilot study (8.4 ± 5.6 for the Pilates group and 13.6 ± 13.6 for the home-based exercise group). The calculation demonstrated a required sample size of 126 participants. Assuming a dropout of 15%, we determined that 144 participants were needed (72 participants per group).
Statistical analysis
Analyses were conducted following the intention-to-treat principle. SPSS version 29 software was used. Missing data were imputed using multiple imputations, assuming a completely at random pattern of missing values (missing completely at random). Variables associated with missing data and outcomes were included in the model (i.e. baseline data). The number of imputed datasets was five to reach a fraction of missing information of less than 5%.
The effectiveness analysis was performed using a linear mixed model, to estimate the differences between the interventions (Pilates vs. home-based exercises) over time (baseline, post-intervention, and six-month follow-up), in the outcomes of interest. Baseline covariates were included in the model to adjust effect estimates for age, gender, and prognosis. Discussions of minimally clinically important differences between groups took into account the following thresholds, that is, > 2 points difference for pain (numerical rating scale), 25 > 20 points for disability, 26 and > 0.03 for utility. 27
We performed a sensitivity analysis of the effectiveness data between groups, by comparing the results by intention-to-treat and complete case analysis. We also performed a second sensitivity analysis considering the adherence to the intervention. Participants were divided into three subgroups within each intervention (NC: non-compliant – adherence ≤ 25%; PC: partially compliant – adherence >25% < 75%; FC: fully compliant – adherence ≥ 75%), and the analysis compared the effects of compliance on the outcomes studied.
The Mann-Whitney U-test was applied to compare the perceived recovery between intervention groups in the post-intervention and follow-up moment, with significance set at 5% (P < 0.05).
Results
Participants
One hundred and sixty-two subjects were screened for eligibility, and seventeen were excluded (14 did not meet inclusion criteria and three declined to participate). One hundred and forty-five subjects were included and randomised. All participants remained in the initially assigned intervention groups and no adverse events were reported (Figure 1).
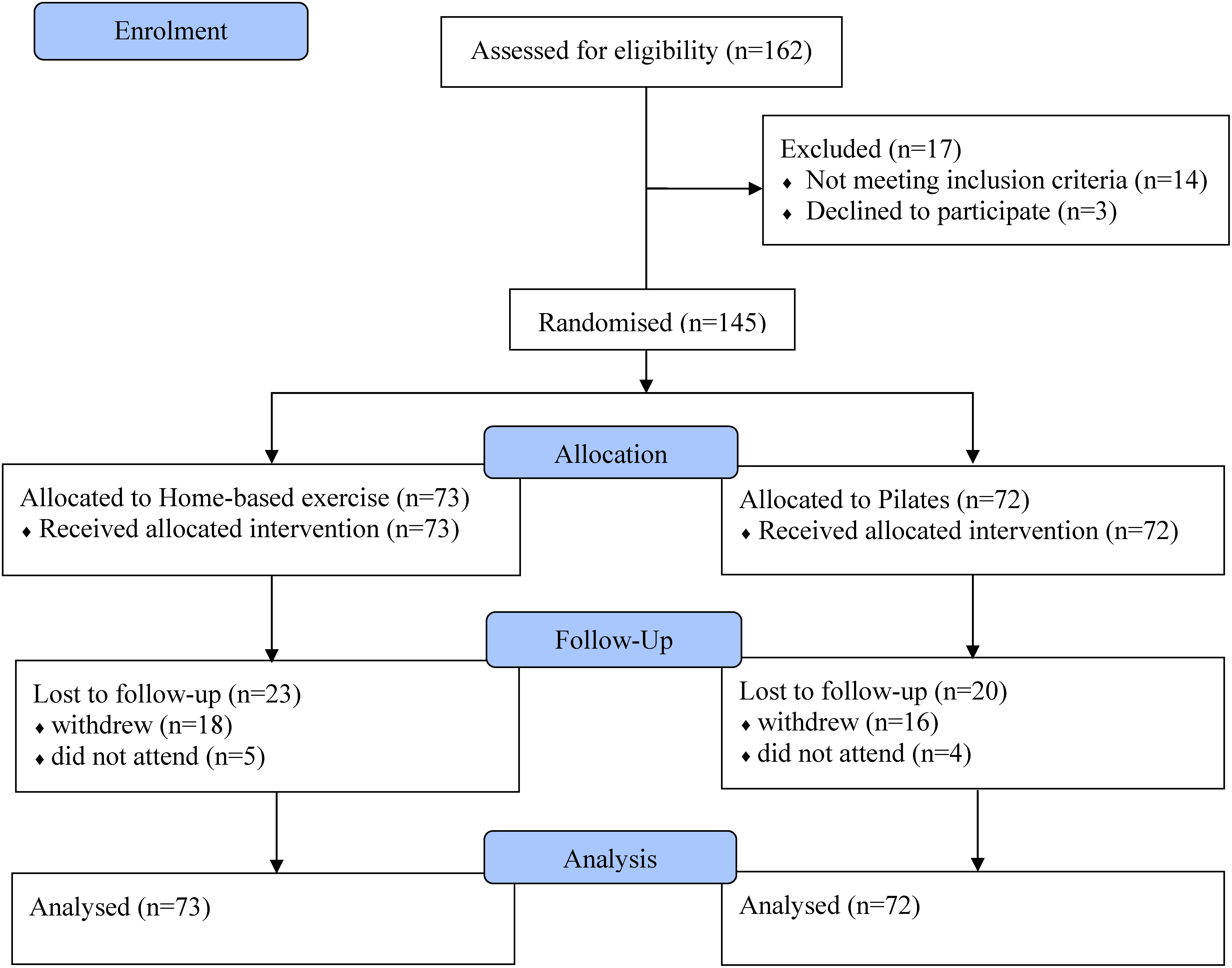
Study flowchart.
Twenty-three and twenty participants were lost to follow-up in the Pilates and home exercises groups, respectively (Figure 1). Notwithstanding, the sensitivity analysis showed that there were no relevant differences between the intention-to-treat and complete case analyses. Further information is presented in Supplemental Table S1.
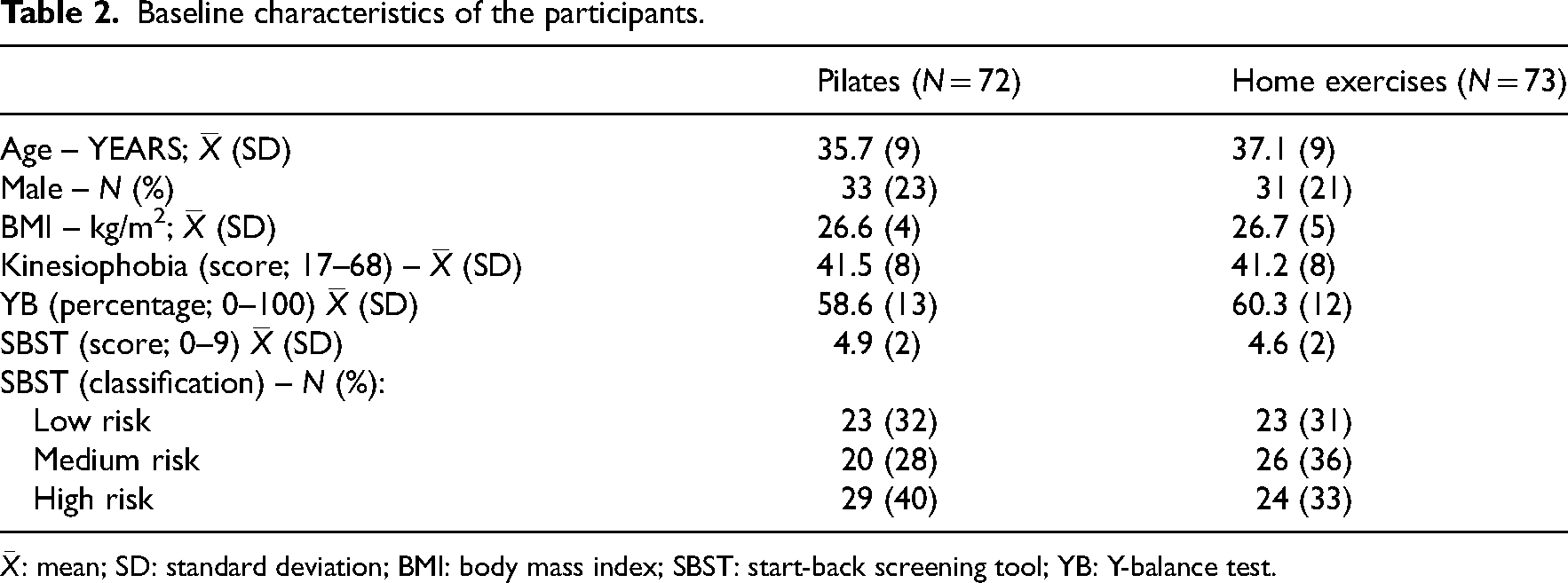
The characteristics of the participants at baseline showed no relevant differences (Table 2). During the intervention, over 50% (n = 40) of the individuals in the Pilates group successfully attended around 70% of the sessions, while over 50% (n = 37) of the participants in the home-based exercise group completed at least 50% of the sessions. Sensitivity analysis showed no relevant between-group differences in the outcomes studied due to adherence, except that individuals in the Pilates group who were fully compliant had better post-intervention outcomes for pain intensity than those who were fully compliant with the home exercises (Supplemental Table S2).
Baseline characteristics of the participants.
Data for the outcomes measured at baseline, post-intervention, and six-month follow-up are presented in Table 3. At post-intervention, significant differences were found between Pilates and home-based exercise for pain (mean difference: −1.14, 95% CI −2.05; −0.23), disability (mean difference: −6.66, 95% CI −11.29; −2.03), and quality of life (mean difference: 0.102, 95% CI 0.054; 0.151). At follow-up, quality of life was significantly higher in the Pilates compared to the home-based exercise (mean difference: 0.055, 95% CI 0.003; 0.106). The overall effect of Pilates compared to home-based exercise was significantly better for disability (mean difference: −4.4, 95% CI −7.6; −1.1) and quality of life (mean difference: 0.049, 95% CI 0.022; 0.076).
Results on the outcomes measured at baseline, post-intervention, and follow-up.
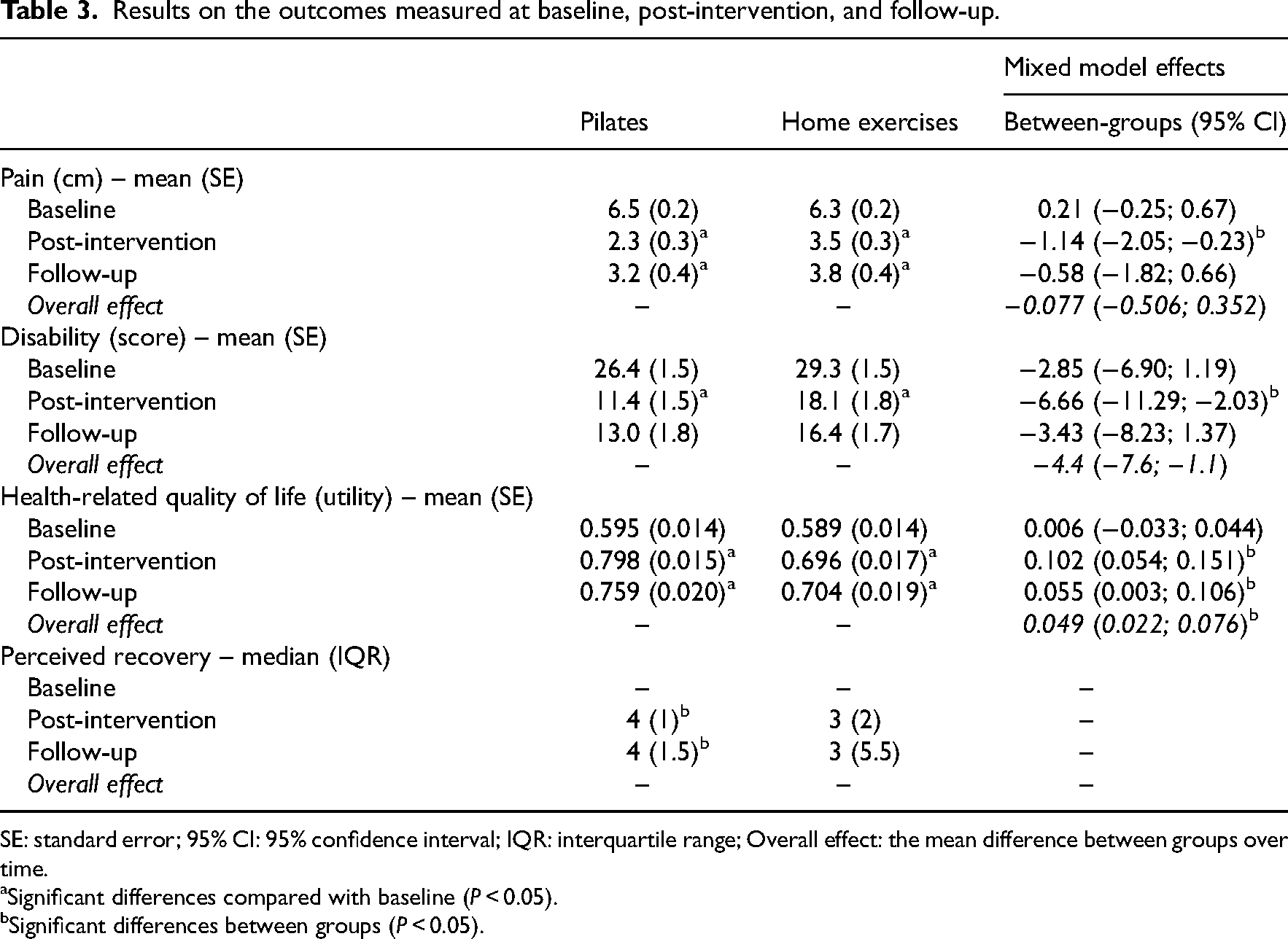
SE: standard error; 95% CI: 95% confidence interval; IQR: interquartile range; Overall effect: the mean difference between groups over time.
Significant differences compared with baseline (P < 0.05).
Significant differences between groups (P < 0.05).
Within the Pilates group, 88% of the participants provided perception of recovery ratings of three, four, and five during the post-intervention, while 71% maintained this rating during the follow-up. In the home-based exercise, the corresponding percentages were 67% in the post-intervention and 49% in the follow-up. Additionally, significant differences were found showing that participants in the Pilates group presented a higher perception of recovery compared with the home-based exercises (Table 3). Further information can be found in Supplemental Table S3.
Discussion
The aim was to investigate the effectiveness of Pilates compared with home exercise on pain, disability, and utility in people with chronic non-specific low back pain. At post-intervention, we demonstrated that Pilates resulted in significantly lower pain intensity and disability, and a higher quality of life compared with home exercise. At the six-month follow-up, we found a significant overall positive effect of Pilates compared with home exercise on disability and quality of life, but not on pain. However, these differences were not clinically relevant for pain and disability because the minimum score required is at least two points on the numerical rating scale,25,26 and 20 points on the disability scale. 26 Differences in quality of life between groups were considered clinically relevant (i.e., > 0.03). 27
Our results are consistent with a previous study 14 which compared a Mat Pilates intervention with home exercise in people with chronic non-specific low back pain. The intervention lasted 8 weeks and only the Pilates was supervised. Their results showed that although pain and disability improved in both groups, greater improvement was reported in the Pilates group. Previous studies8,28 also compared Pilates with general exercise in people with chronic non-specific low back pain for 6 to 8 weeks, with sessions twice a week and supervision in both Pilates and general exercise. The authors reported that Pilates had similar effects to general exercise in improving pain and disability, which were mainly explained by the introduction of supervision. In addition, the disability of our sample at baseline was not considered to be high, which may have prevented the detection of clinically relevant effects. This is interesting because in our study both pain and disability improved over time in both groups, although Pilates provided significantly greater improvements. A possible explanation may be the supervision. Bronfort et al. 29 compared supervised exercises, manipulation, and unsupervised home exercises in patients with chronic non-specific low back pain, and showed that supervision explained improvements in pain and disability. Overall, supervision seems to provide adequate guidance, 14 and is recommended for the management of chronic non-specific low back pain. 30 However, the evidence for supervised versus unsupervised exercise is limited, and conclusions from current studies are inconsistent. 31
Another aspect that might explain our findings was dosage (i.e., weekly frequency, intervention duration). The six-week intervention, with two 50-minute sessions per week, was sufficient to produce effects. A previous study examined the effectiveness of a 12-week Pilates intervention in people with chronic low back pain, with two 50-minute sessions per week, and showed similar results, with the greatest change in disability at six weeks and no change within groups between six and twelve weeks. 32 Despite the wide variation and inconsistency of Pilates protocols in clinical trials, a recent review suggests that the greatest improvements in pain and disability are achieved with at least one to two sessions per week, sessions of < 60 minutes, and 3 to 9 weeks of intervention. 33
Regarding utility, we found significant differences between-groups, also considered clinically relevant. 27 Moreover, these effects were maintained after the intervention period. Hence, Pilates resulted in a better quality of life over time, corroborating previous studies with chronic non-specific low back pain participants.9,14,34 As the Pilates sessions were held face-to-face in small groups, it is possible to assume that social interaction between participants might explain the better utility. 14 Furthermore, utility improvements may also be explained by decreases in pain and disability, since both can affect the quality of life of individuals with chronic low back pain.14,27 Most individuals who participated in Pilates expressed a sense of complete and near-complete recovery during the post-intervention and follow-up period. The reported percentages were somewhat higher in Pilates in comparison to the home exercises. These results are consistent with previous research suggesting that Pilates produces greater improvements in overall perceptions of recovery, particularly following a six-week intervention.9,34
This trial has several strengths. We used proper randomisation and concealed allocation to reduce the risk of selection bias. In addition, the statistical analyst was blinded. We implemented intention-to-treat analysis and used multiple imputations to reduce selection bias due to attrition. We also ensured that we used the expertise of a certified and experienced Pilates instructor and an experienced physiotherapist to supervise the home exercises, to ensure the highest quality of treatment. Finally, our sample size was adequate and we were able to recruit the intended number of participants.8,14,28
Notwithstanding, we had limitations. We were not able to collect data on one of the outcomes (i.e. dynamic balance), mostly due to the COVID-19 pandemic which restricted the follow-up assessments of some participants. Thus, we decided to use dynamic balance as a baseline measurement. We also decided to use dynamic balance measurements instead of static balance measures (as defined in the protocol), because clinical findings from dynamic conditions would be more informative. Secondly, part of our volunteers were affected by the pandemic, as the last intervention session and follow-up measurements were scheduled within the first wave of COVID-19 and lockdown. Therefore, this aspect also influenced their adherence to some extent, although our sensitivity analysis showed that the only relevant finding was that individuals in the Pilates group who were fully compliant had better post-intervention outcomes for pain intensity than those who were fully compliant with the home exercises.
Our results provide evidence that Pilates is significantly superior to home exercise for pain and disability in patients with chronic non-specific low back pain, but these differences were not considered clinically relevant. Nevertheless, we found clinically relevant improvements in health-related quality of life in favour of Pilates. This is interesting because a recent systematic review suggested that among different types of exercises, Pilates was considered the most effective. 33 Thus, the implementation of Pilates in clinical settings within the healthcare system could be considered by policy-makers and decision-makers.
Clinical messages
Individuals with chronic low back pain might benefit from Pilates for reducing pain and disability, although the clinical relevance is uncertain;
Pilates provide clinically relevant improvements in the health-related quality of life of individuals with chronic low back pain.
Supplemental Material
sj-doc-1-cre-10.1177_02692155241277041 - Supplemental material for Effectiveness of Pilates compared with home-based exercises in individuals with chronic non-specific low back pain: Randomised controlled trial
Supplemental material, sj-doc-1-cre-10.1177_02692155241277041 for Effectiveness of Pilates compared with home-based exercises in individuals with chronic non-specific low back pain: Randomised controlled trial by Caroline Ribeiro Tottoli, Ângela Jornada Ben, Everton Nunes da Silva, Judith E Bosmans, Maurits van Tulder and Rodrigo Luiz Carregaro in Clinical Rehabilitation
Footnotes
Authors contributions
CRT, ENS, and RLC: methodology, data curation, formal analysis, writing–original draft, and visualization. MvT, ENS, AJB, and JEB: review and editing, writing–original draft, and visualization.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by: the Federal District Research Support Foundation [process n. 00193-001711/2017]. This study was also financed in part by Coordination for the Improvement of Higher Education Personnel (finance code 001), Doctoral Program in Physical Education, University of Brasília, and University of Brasília/Dean of Research and Innovation. The funding agencies have no role in the design and implementation of the study or in the data analysis and presentation of the results.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.