
Abstract
Objective
The objective of this systematic review and meta-analysis was to evaluate the effectiveness of social prescribing interventions in the management of long-term conditions in adults.
Data sources
Eleven electronic databases were searched for randomised and quasi-randomised controlled trials.
Review Methods
Outcomes of interest were quality of life, physical activity, psychological well-being and disease-specific measures. Bias was assessed with the Cochrane Risk of Bias 2 tool. A narrative synthesis and meta-analysis were performed.
Results
Twelve studies (n = 3566) were included in this review. Social prescribing interventions were heterogeneous and the most common risks of bias were poor blinding and high attrition. Social prescribing interventions designed to target specific long-term conditions i.e., cancer and diabetes demonstrated significant improvements in quality of life (n = 2 studies) and disease-specific psychological outcomes respectively (n = 3 studies). There was some evidence for improvement in physical activity (n = 2 studies) but most changes were within group only (n = 4 studies). Social prescribing interventions did not demonstrate any significant changes in general psychological well-being.
Conclusion
Social prescribing interventions demonstrated some improvements across a range of outcomes although the quality of evidence remains poor.
Keywords
Introduction
Long-term conditions are lifelong health problems, which tend to be managed through medication and other therapies.1,2. Though long-term conditions lack a universal definition 3 it is acknowledged that long-term conditions may present as individual or multiple diseases co-existing simultaneously 4 significantly impacting both physical5,6 and mental wellbeing7,8 and are associated with increasing age, female gender, lower income class and poor social network. 9 Patients with long-term conditions have poor quality of life,10,11 reduced ability to work, 12 greater dependence on hospital services 13 and experience premature death. 14 Healthcare providers are encouraged to adopt patient-centred models of care for individuals with complex multimorbidity 15 to prevent the treatment burden that accompanies fragmented delivery of poorly coordinated single-disease models of care. 16
Social prescribing is an innovative person-centred approach 17 to help individuals from socioeconomically deprived areas address the biopsychosocial factors associated with long-term conditions 18 and improve their quality of life19–21 by linking patients in primary care with existing tertiary support services in the community.22,23 Social prescribing may complement existing medical management by incorporating both horizontal and person-centred integration models of care. 24 A social prescription involves the referral of individuals by medical and allied health practitioners to non-clinical laypersons called ‘Community link-workers’ or ‘Community health workers’, who collaborate with these individuals to identify purposeful goals and co-design a social prescribing pathway involving relevant community-based support schemes.19,25–28 For the purpose of this review, non-clinical laypersons, recruited from the local community (that do not have existing health care qualifications) will be referred to as community link-workers. Social prescribing pathways vary from light touch signposting for housing and financial needs 29 and community groups referral for art therapy or exercise therapy30,31 to more intensive pathways offering increased community link-worker support to address the complex needs of individuals with long-term conditions. 19
Participants of social prescribing initiatives have reported improvements in numerous health domains, for example: Increased self-esteem; 32 increased sense of control and empowerment;30,32 improvements in psychological well-being; 33 reduction in anxiety and/or depression; 34 and improved physical health and lifestyle. 35 Previous systematic reviews exploring the effectiveness of social prescribing have highlighted the heterogeneity of the methodological approaches across the research. Uncontrolled before and after studies; lack of comparative controls; patients lost to follow up and inappropriate outcome measures for the population of interest are reported as limiting factors influencing the strength of the findings.19,25 Furthermore, previous systematic reviews were limited to specific countries19,25,36 or had a singular focus on particular outcomes of interest 37 and population. 38 This current systematic review will bridge this gap in the evidence by including only randomised/quasi-randomised controls, from different geographical regions, focusing on outcomes that reflect the multifactorial nature of long-term conditions. Given the limitations of the literature to date, the aim of this systematic review and meta-analysis was to determine the effectiveness of social prescribing in the management of long-term conditions in community-based adults.
Methods
A systematic review of the literature was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement. 39 The protocol for this review is registered with Open Science Framework https://osf.io/p5vf9/.
Study design
A systematic literature review of randomised and quasi-randomised controlled studies assessing the effectiveness of a social prescribing intervention on community-based adults with long-term conditions, utilising a ‘Community link-worker’ or ‘Community health worker’ was performed. A narrative synthesis was conducted on the identified studies and a meta-analysis performed on those studies that reported haemoglobin A1C (HbA1c) levels in diabetes.
Data sources and search strategy
A comprehensive literature search (Supplementary Material #1) of electronic databases was conducted from inception until November 2022 and updated in December 2023. Databases searched were: MEDLINE and MEDLINE in Process (via Ovid), EMBASE, Cochrane Central Register of Controlled Trials (CENTRAL), Cumulative Index to Nursing and Allied Health Literature (CINAHL), EU Clinical Trials Register, LILACS (Latin American and Caribbean Health Sciences Information Database), Scopus and AgeINFO. Trial registries including Clinicaltrials.gov, WHO trials search (ICTRP) and Trials Register of Promoting Health Interventions (TRoPHI) were also searched. The search was supplemented by hand-searching relevant journals and citation tracking. The Grey literature was searched using Irish Health Service Executive (HSE) Lenus, RIAN, Open Grey and World Health Organization Library Information System (WHOLIS).
Inclusion and exclusion criteria
To be included studies had to be randomised or quasi-randomised controlled trials incorporating a social prescribing model with a non-clinical community-based link-worker, recruited from the community, without a previous qualification in medical or health sciences or already working in a professional clinical role. The social prescribing interventions had to be community-based using a health promotion approach defined by the Social Prescribing Network Conference Report for Long-term Conditions in Community-Dwelling Adults. 34 Any long-term conditions appropriate for a social prescribing intervention could be included in this review (for example, diabetes mellitus, stroke, asthma, depression, chronic obstructive pulmonary disease, chronic kidney disease, hypertension, inflammatory arthropathies, irritable bowel syndrome, obesity, cardiovascular disease, low back pain, progressive neurological disorders, and cancer). Interventions could be face-to-face or remote. Outcome measures of interest were quality of life, physical activity, psychological well-being, and disease-specific measures. Only studies published in English were included and participants had to be at least 18 years.
All studies identified from the search strategy were exported to Covidence software. 40 After study duplicates were removed an initial screening of titles and abstracts was conducted independently by two authors (DJOS and JGMcV). Full text of suitable studies was obtained and independently screened against the inclusion criteria. Studies meeting the inclusion criteria were independently reviewed with any disagreements between the two reviewers arbitrated by a third reviewer (JH).
Data extraction
A data extraction template was developed a priori and trialled with one study. Study characteristics captured included author, year of publication, patient demographics (age, gender) and background, intervention, control, duration of the intervention, primary and secondary outcome measures, results. A further characteristic of the intervention table was also made. Both original tables may be found in the supplementary materials file.
Methodological quality evaluation and risk of bias
The methodological quality and reporting standards of this review were constructed using the Cochrane Collaboration's tool for assessing risk of bias in randomised and quasi-randomised trials (RoB2). 41 The Rob2 tool is structured into five domains 37 including; bias arising from the randomisation process; bias due to deviations from intended interventions; bias due to missing outcome data; bias in measurement outcome; bias in selection of the reported outcome. Risk of bias was assessed independently by two reviewers (DJOS, JGMcV) and differences resolved by discussion with a third researcher (JH). A judgement was made on each study as being low, high, or unclear risk of bias.
Data synthesis
Summary data on the study characteristics and the study interventions (Table 1) were extracted and presented in tabular form, (primary study characteristics table and primary intervention table are available in Supplemental materials). A narrative synthesis was conducted, and the data was explored to interpret the relationships in the data within and between studies. Data was analysed to determine the impact of variability in study designs, populations and outcome measures. A meta-analysis, was performed on four of the 12 included studies using the Hartung-Knapp-Sidik-Jonkman 42 random-effects method and illustrated graphically (Figure 2). The standardised mean difference and 95% confidence interval (95% CI) were used to analyse the effect of the community link-worker intervention on HbA1c in diabetes, when comparing community link-worker interventions to the control group. Where necessary, authors were contacted to solve possible uncertainty of effect size and RoB2 interpretations. To assess between-study variance we used tau-squared (the variance of true effects). The I² statistic was then used to determine any inconsistencies within the data. These statistical analyses were performed using IBM SPSS Statistics (Version 29). 43 Statistical significance was set at 5%. Sensitivity analyses were performed by removing the study with the highest ‘weight’ for each cluster.
Characteristics of the study and social prescribing intervention.
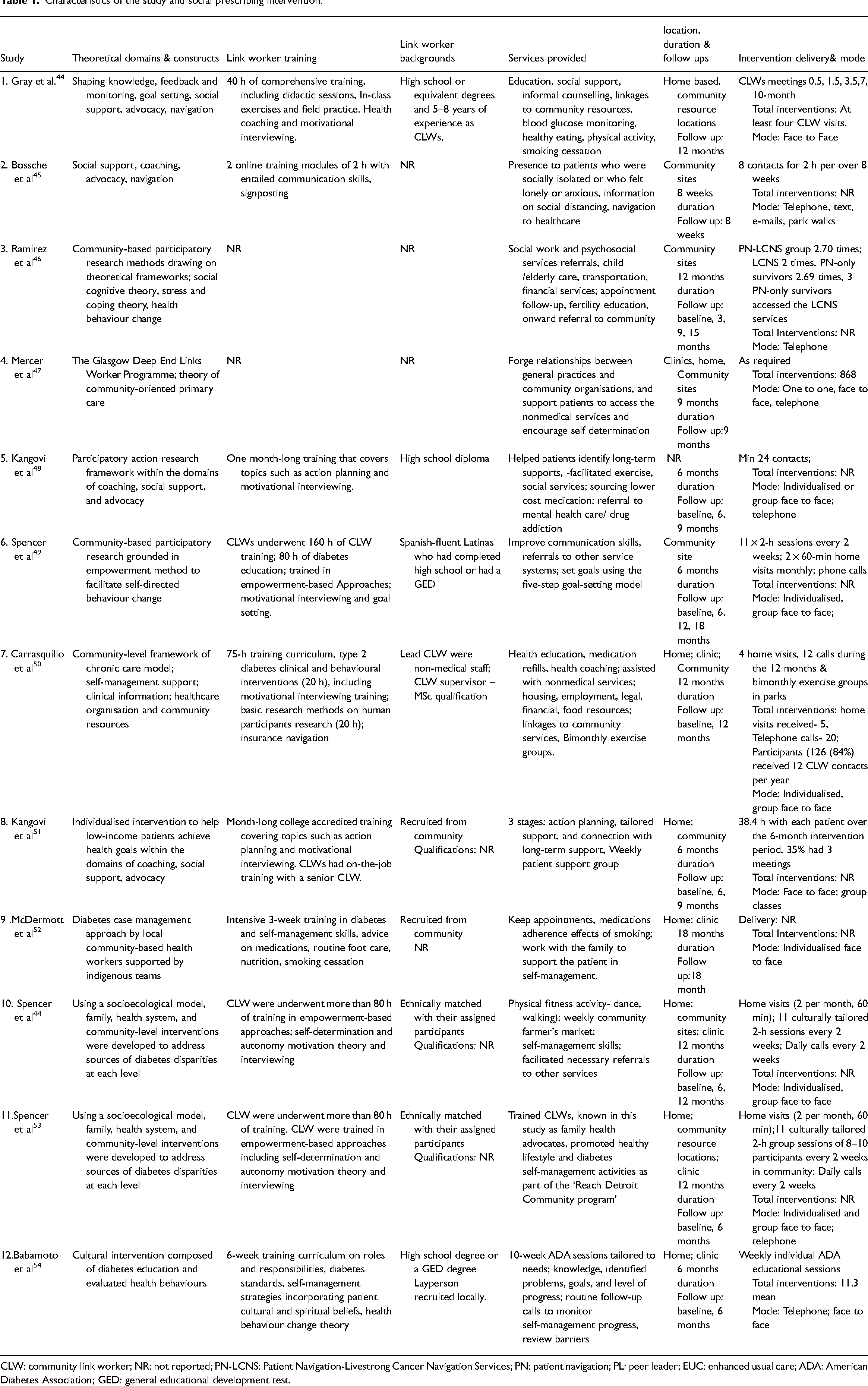
CLW: community link worker; NR: not reported; PN-LCNS: Patient Navigation-Livestrong Cancer Navigation Services; PN: patient navigation; PL: peer leader; EUC: enhanced usual care; ADA: American Diabetes Association; GED: general educational development test.
Results
Electronic searches identified 5807 potential studies. After duplicates were removed (n = 444), 5363 studies were screened for title and abstract content of which 191 studies were eligible for full text screening (n = 3566). Two reviewers (DJOS, JGMcV) independently assessed the eligibility of these studies and 12 studies were selected for this review. An updated search of the literature was conducted in December 2023 but did not identify any further studies. Figure 1 outlines the PRISMA flow chart.
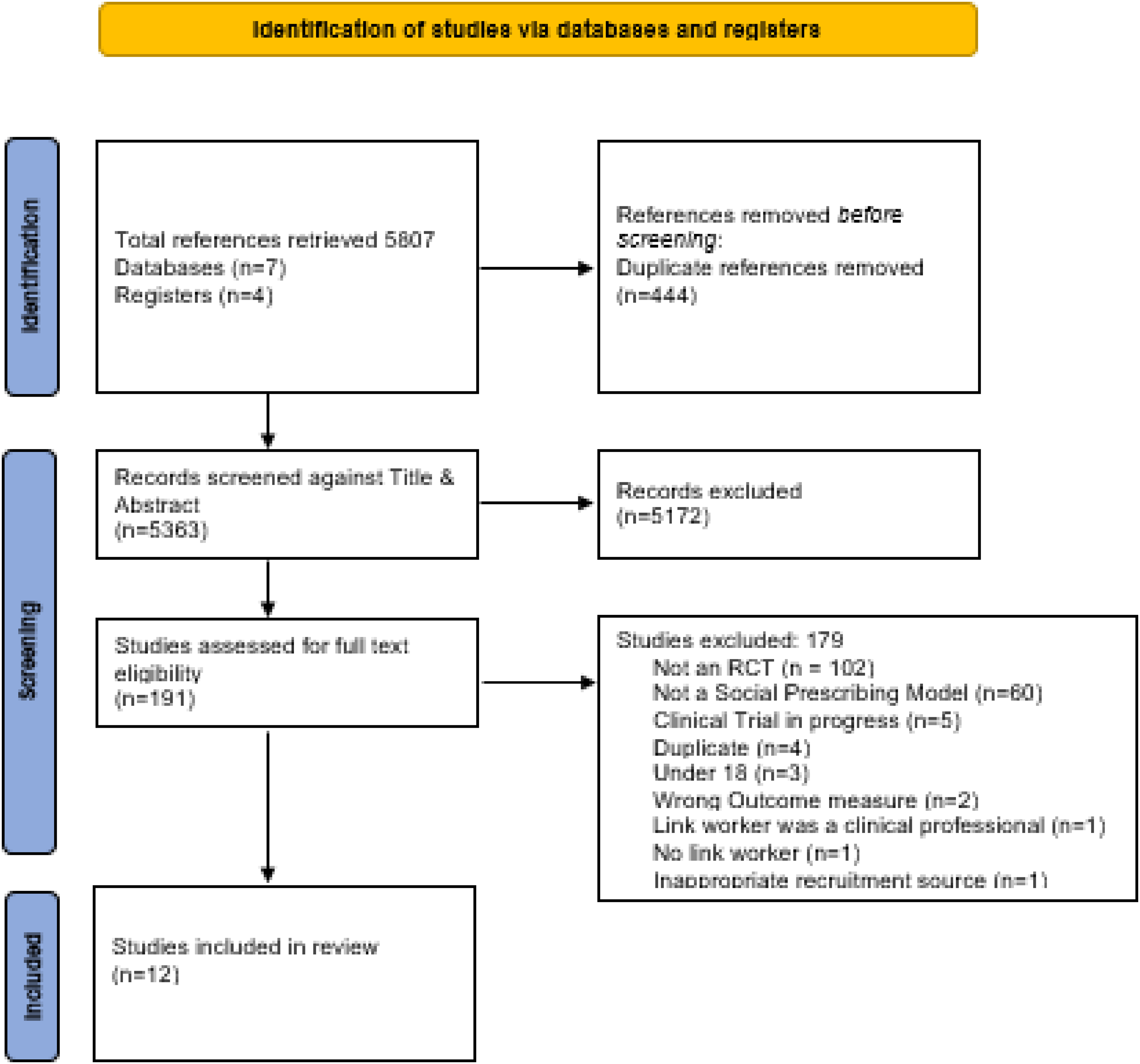
Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flow diagram.
Study characteristics
The selected studies were conducted in the United States of America (n = 9),44,46,53,54 United Kingdom (n = 1), 47 Belgium (n = 1) 55 and Australia (n = 1) 52 and were heterogeneous in design. Cancer (n = 1) 46 and diabetes (n = 7)48–54 were the main long-term conditions identified. Comparison groups included waiting list 52 usual care,45,47,48,51,54,55 enhanced care,46,49,50 or delayed access to the intervention.44,53 Study duration ranged from 8 weeks 55 to 18 months49,52. The total number of participants included in the 12 studies was n = 3566, (female n = 2179, male n = 1387) with a mean age of 48 years.
Risk of bias
Overall, nine studies were judged to have a high risk of bias44,45,46,47,49,52–55 and three studies were judged to have low risk of bias.48,50,51 The ‘measurement of the outcome’ presented as the greatest risk of bias in eight studies and the ‘missing outcome data’ domain had the lowest risk of bias in all 12 studies, supplementary material. There was moderate level of agreement between the two independent reviewers’ risk of bias judgements using the Kappa coefficient (K = 0.488).
Risk of bias summary judgements and judgements on outcome domains are available in supplementary materials.
Intervention characteristics
Community link-workers led the intervention in all included studies and were recruited from the community of interest. The duration of community link-worker training ranged from 4 55 to 160 h. 49 The social prescribing interventions utilised in the included studies were grounded in behavioural change theoretical frameworks and behavioural models such as social cognitive theory45,46 self-regulation theory 45 ; stress and coping theory and health behaviour change theory. 46 The attrition rate across all studies was generally high and ranged from 9% to 29%. The characteristics of each study and the social prescribing intervention are summarised in Table 1.
Outcome measures used in the social prescribing intervention
Forty-one different outcome measures (self-reported, n = 33) were used to determine the effects of a social prescribing intervention on primary and secondary outcomes. The duration of social prescribing interventions ranged from 8 weeks 55 to 18 months.49,52 Outcomes of interest were categorised as quality of life (n = 12), physical activity (n = 2), psychological wellbeing (n = 8), disease-specific outcomes (n = 17) and uncategorised (n = 2).
Effect of the social prescribing intervention on quality of life outcomes
There are short to long-term improvements in quality of life for those receiving social prescribing interventions, 46 particularly for those attending more frequently (>3 visits). 47 Mercer et al 47 (high Risk of Bias) found significant improvements in quality of life with three or more face-to-face engagements with the community link-worker intervention as measured by the EQ-5D-5L questionnaire 0.071 (95%CI, 0.016, 0.126); P < 0.011). Male and female participants with similar cancer presentations responded differently after an enhanced community link-worker led intervention. 46 Female colo-rectal cancer survivors in remission derived up to 15 months health related quality of life improvements when measured by the Functional Assessment of Cancer Therapy – General Scale (FACT – G Scale): 0.171; (95% CI, 0.025–0.317; P = 0.021) compared to males who had only short term improvement in health-related quality of life (3 months): 10.074 (95%CI, 2.030–18.119; P = 0.014).
Effect of social prescribing intervention on physical activity
Seven studies used physical activity45,47,48,50,51,53,54 as a primary (n = 4)45,47,48,54 or secondary outcome (n = 3).50,51,53 Two high Risk of Bias studies45,54 reported significant increments in the frequency 54 of physical activity (3 times per week) from baseline n = 21(28%) to 6-month follow-up n = 47(63%) P < 0.05) and the duration of physical activity 45 (mins/week) by 141 min (95% CI 46.4, 236.4) (p < 0.004) in the community link-worker intervention group (baseline: 12 months: 271.3(mins) (421.6) to 344.2 (mins) (455.6) (+72.8) compared to controls (baseline: 12months; 240.1 (mins) (364.1) to 199.9 (mins) (350.0) (−40.2)) who regressed during the 12-month intervention. The remaining three low-Risk-of-Bias studies48,50,51 and two high-Risk-of-Bias studies47,53 reported significant within-group improvements only in physical activity levels. There is some evidence from a subgroup analyses conducted in one high Risk of Bias study 47 that participants attending the ‘Glasgow Deep End’ community link-worker intervention more frequently (>3 in person visits) showed small but significant within-group improvements only in self-reported exercise levels over time 0.339 (95%CI, 0.071−0.607); P < 0.013).
Effect of the social prescribing intervention on psychological wellbeing outcomes
Three studies47,48,55 two high Risk of Bias47,55 and one low Risk of Bias 48 used indicators of psychological wellbeing as either primary 55 (emotional support, social isolation, anxiety measured by the PROMIS score) or secondary outcomes47,48 (Short Form 12-Mental 56 and Hospital Anxiety Depression Scale (HADS-Anxiety / HADS-Depression) 57 )). Two studies48,55 did not demonstrate any significant between-group improvements in psychological wellbeing for participants of a community link-worker intervention. However, participants from Mercer et al 47 study that met face-to-face with the community link-worker more than three times did show significant between-group improvement in their HADS-Anxiety score (−1.380)(95%CI, −2.339, −0.421); P < 0.005) and HADS – Depression score (−1.280)(95%CI, −2.209, −0.352; P < 0.007) but overall, did not demonstrate any significant effects on this outcome at the end of the trial.
Effect of the social-prescribing intervention on disease-specific measures
HbA1c test measures the percentage of haemoglobin proteins in the blood that are saturated with glucose (normal: <42 mmol/mol (6%)). The HbA1c test is a direct indicator of long-term glycaemic control that correlates well with complications arising from diabetes. 58 Seven studies48–54 explored the effect of a community link-worker intervention on HbA1c blood levels in patients with diabetes as a primary outcome (n = 6)49–54 or as a secondary outcome (n = 1). 48 Four studies49,50,52,53 reported significant between-group improvements in HbA1c levels at 6 months;49,53 12 months49,50 and 18 months49,52.
Due to the heterogeneity of the intervention and outcome reporting, it was only possible to conduct a meta-analysis on the pooled data from four studies (n = 1329), 2 low Risk of Bias48,51 and 2 high Risk of Bias49,52 to compare the effects of community link worker interventions on individuals’ HbA1c levels from baseline to 18 months. The respective calculated effect sizes are displayed in Figure 2. The forest plot (red dashed line) indicates a small non-significant effect of −0.07 (95% CI −0.23, 0.10): P = 0.31. The Tau-square test represented the variance of the effect size across the studies, the value of 0 means that there is no significant between-study variance beyond what would be expected by chance alone.
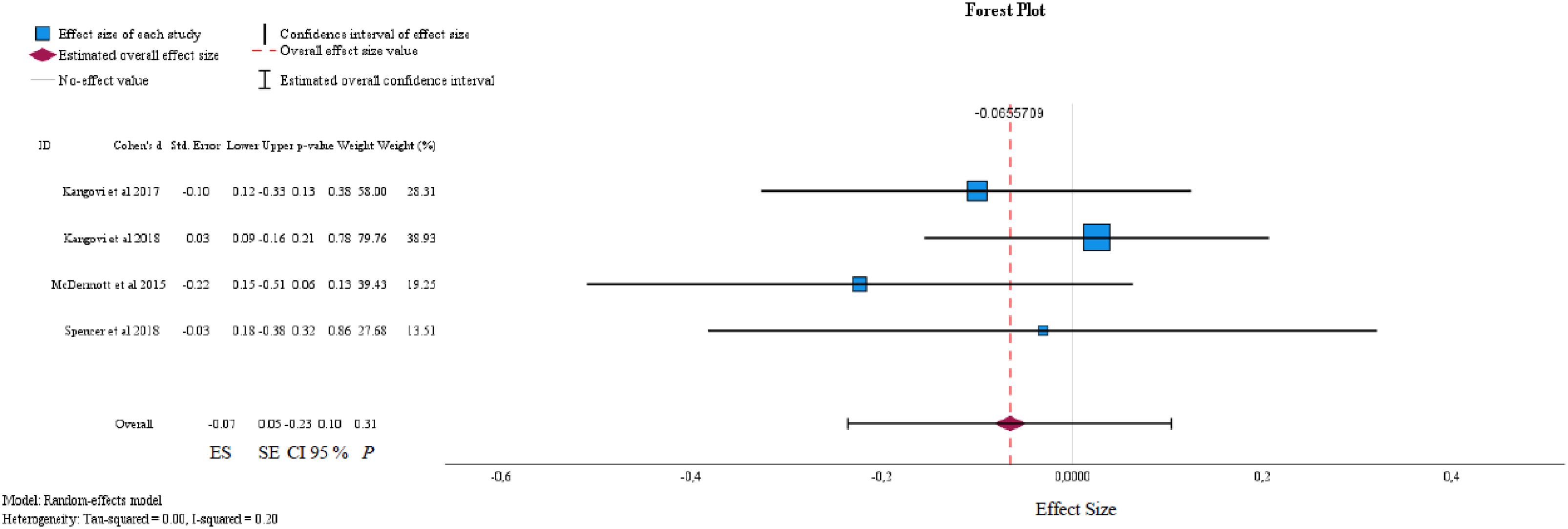
Meta-analysis of social prescribing intervention on haemoglobin A1C (HbA1c) levels in diabetic patients.
Four studies,44,49,53,54 three of which were from the same author44,49,53 and all having high Risk of Bias44,49,53,54 used eight separate diabetes-specific patient-reported outcome measures to determine the effectiveness of a community link-worker intervention on diabetes-related distress, depression, self-management and self-efficacy required to control diabetes. Spencer et al44,49,53 examined the levels of distress experienced by people with diabetes using the Problem Areas in Diabetes Scale in two early studies44,53 and later the Diabetes Distress Scale. 49 The first of these studies 53 did not find any significant change between the community link-worker group and the control. However, in the later 12-month study, 44 after adjusting for demographic variables the authors reported significant changes in the intervention group (n = 72) at baseline 23.8 (95% CI, 18.7, 29.0) and six months −6.5 (95% CI, −11.2, −0.04); P < 0.05) and 6–12 months −7.8 (95% CI, −12.5, −1.4); P < 0.05) compared to the delayed intervention group (n = 92) at baseline 25.9 (95%CI, 21.2, 30.6) and six months (−1.7 (95% CI, −7.0, 5.3); P > 0.05) and 6–12 months −6.2 (95%CI, −11.0, 0.2); P > 0.05). These findings are again supported in another later study 49 using the Diabetes Distress Scale which demonstrated significant reduction in diabetes-related distress of −0.4 (95%CI, −0.7, −0.1); P < 0.05) for up to 18-months in the community link-worker group only. Spencer et al44,49 also examined the effectiveness of a community link-worker intervention on diabetes-related depression using the Patient Health Questionairre-9. 59 In the latter of these two studies individuals randomised to the extended peer-led community link-worker intervention (6–18 months) demonstrated significant decrements in depressive episodes at 18 months −2.2 points (95% CI −4.1, −0.3) P < 0.05) compared to the enhanced usual care group. The effectiveness of Community link-worker interventions on diabetes self-management was measured in three studies49,53,54 by the Diabetic Care Profile, 60 Summary of Diabetes Self-Care Activities Measure 61 and the Diabetes Knowledge Scale. 62 The Diabetic Care Profile 60 used by Spencer et al 49 which assesses a patients’ understanding of the social and psychological factors related to the self-management of diabetes reported the extended peer-led community link-worker group demonstrated a significant between-group improvement of 0.3 points (95% CI, 0.1, 0.6); P < 0.05) after 12 months against the enhanced usual care group but not the community link- worker only group. The Diabetes Knowledge Scale was used in one study only 54 . Significant between-group results were reported at the 6-month follow-up for community link-worker intervention versus case management versus standard care (P < 0.05). Spencer et al49,53 were the only studies to examine the effectiveness of community link-worker interventions on diabetes-related self-efficacy utilising the Perceived Competence of Diabetes Scale 63 and Diabetes Social Support, 64 respectively. At 6 months’ time point diabetes self-efficacy was significantly improved 0.5 (95%CI, 0.2,0.8); P < 0.01) in the community link-worker group only 49 .
Five studies48,50,51,53,54 investigating the effect of a community link-worker intervention on body mass index,50,51,54 cholesterol48,50,53 and blood pressure48,50 did not report any significant within group or between group changes across the trial periods.
Discussion
The aim of this systematic review was to determine the effectiveness of social prescribing in the management of long-term conditions in community-based adults. To the best of our knowledge, this is the first systematic review to conduct a meta-analysis of the data on the effectiveness of social prescribing focusing on outcomes that reflect the multifactorial nature of long-term conditions. Twelve randomised controlled trials across different geographical locations, in areas of socioeconomic deprivation, were included in this review. Most studies included in this review utilised a tailored social prescribing model directed at improving diabetes self-management. This review found some evidence to support the effectiveness of social prescribing in improving quality of life and disease-specific outcome measures. There is some evidence that adherence to a social prescribing intervention may result in positive outcomes for the participant. Most significant improvements were in reducing diabetes-related distress; diabetes-related depressive episodes and improving diabetes self-management efficacy. Given the heterogeneity of the included studies and outcome measures and like previous review conclusions19,36,37 it is not possible to determine the effectiveness of social prescribing in the management of long-term conditions in community-based adults.
The results of this review suggest that an enhanced social prescribing intervention with increased uptake of support services provided over a longer duration will lead to improvements in both short and long-term quality of life outcomes.47,65 As females reported longer-term improvements (15 months) there may be other factors influencing the gender response to the social prescribing intervention. This contrasts with previous evidence that found men with poor health, anxiety, and social networks had greater benefit from social prescribing interventions than women 66 and may be explained by the possible gender differences in coping strategies of cancer patients. 67 It is unclear if there is a gender response to social prescribing which is a possible area for future research.
There is some evidence from this review that participating in a social prescribing intervention can significantly influence a participant's uptake of physical activity in the short term 54 and also the weekly duration of physical activity in the long-term 45 helping participants with controlled diabetes meet recommended physical activity guidelines 68 with minimal support. 45 Other studies within this review48,50,51,53 also demonstrated significant improvements in physical activity but within group only. The control groups also receiving physical activity advice and access to free services e.g., dance classes, exercise classes and walking groups may explain these improvements. No study in the present review utilised external activity monitors e.g., pedometers that would provide objective measures of activity and eliminate response bias. Social prescribing interventions did not demonstrate any significant between-group changes in psychological well-being in participants experiencing anxiety and depression44,47 or in patients with limited social network. 55 High dropout rates and lack of reporting on intervention adherence makes it difficult to interpret these results with confidence.
The results from individual studies44,45,49–54 within this review suggest that targeted disease-specific community link-worker interventions can significantly improve HbA1c levels in patients with diabetes in the short (six months) and long-term (18 months) to those recommended by the American diabetes guidelines. 69 However, when the data from suitable studies48,49,51,52 were pooled in a meta-analysis the results showed social prescribing interventions had only a small non-significant impact on HbA1c levels at six months (P = 0.31). This finding is contrasted in a recent large-scale study 70 which found a small statistically significant reduction in HbA1c (−1.11 mmol/mol) (95% CI: −1.878, −0.342); P < 0.05), however, the authors concluded this was not sufficient to be clinically significant, thus echoing our results. Psychological co-morbidities are common in people with physical long-term conditions71,72 and may influence the lifelong trajectory of their illness.73,74 This review has highlighted some evidence to support the role of social prescribing in significantly improving disease-related distress, 49 depression, 44 self-management knowledge 54 and self-efficacy 53 which play an integral role in patient empowerment.75,76 The heterogeneity and unblinding of outcome measures (n = 41) used to measure the effect of the intervention on quality of life, physical activity, psychological wellbeing and disease-specific parameters lessens the credibility of their findings and made evidence synthesis challenging. Outcome reporting bias and inconsistency in the measurement of outcomes could be minimised through the development77,78 and reporting 79 of standardised core outcome sets with established Minimal Clinical Important Difference values similar to other areas. 80 This review has identified key factors that may influence future clinical practice; targeted and enhanced social prescribing interventions improve self-management and self-efficacy of long-term conditions; the use of technology in the measurement of physical activity should support self-reported measures of physical activity in social prescribing interventions.
It should be noted that there are some limitations with this review. Firstly, only studies published in the English language were considered for inclusion, it is possible some studies published in another language were missed. Secondly, while the search strategy was comprehensive, including nine databases, three trial registries and the grey literature, it could be argued that the range of keywords used could have been more extensive. It is possible that using specific conditions and outcome measures may have resulted in a more focused search and perhaps additional papers. Notwithstanding this, we are confident we have identified all relevant papers.
This comprehensive systematic review only includes quasi-randomised and randomised controlled trials whose study design matches the current definition of social prescribing
23
and is the first review of social prescribing to use a meta-analysis to analyse the data. The studies included within our review were heterogeneous in terms of patient populations, interventions delivered, and outcome measures used, which substantially influences the ability to make meaningful comparisons. This review suggests that social prescribing interventions designed to target specific long-term conditions, i.e., cancer and diabetes, demonstrated significant improvements in quality of life and disease-specific psychological outcomes respectively. There was some evidence for improvement in physical activity levels, but most findings were within-group changes only. Social prescribing interventions did not demonstrate any significant changes in psychological well-being. The findings from this review suggest it is not possible to determine the effectiveness of social prescribing in the management of long-term conditions.
Tailored social prescribing interventions improved quality of life in cancer remission patients. Social prescribing interventions improved diabetes-specific psychological outcomes. Social prescribing interventions may improve the frequency and duration of physical activity in people with diabetes.Clinical messages
Supplemental Material
sj-docx-1-cre-10.1177_02692155241258903 - Supplemental material for The effectiveness of social prescribing in the management of long-term conditions in community-based adults: A systematic review and meta-analysis
Supplemental material, sj-docx-1-cre-10.1177_02692155241258903 for The effectiveness of social prescribing in the management of long-term conditions in community-based adults: A systematic review and meta-analysis by Declan J O’Sullivan, Lindsay M Bearne, Janas M Harrington, Jefferson R Cardoso and Joseph G McVeigh in Clinical Rehabilitation
Supplemental Material
sj-docx-2-cre-10.1177_02692155241258903 - Supplemental material for The effectiveness of social prescribing in the management of long-term conditions in community-based adults: A systematic review and meta-analysis
Supplemental material, sj-docx-2-cre-10.1177_02692155241258903 for The effectiveness of social prescribing in the management of long-term conditions in community-based adults: A systematic review and meta-analysis by Declan J O’Sullivan, Lindsay M Bearne, Janas M Harrington, Jefferson R Cardoso and Joseph G McVeigh in Clinical Rehabilitation
Supplemental Material
sj-docx-3-cre-10.1177_02692155241258903 - Supplemental material for The effectiveness of social prescribing in the management of long-term conditions in community-based adults: A systematic review and meta-analysis
Supplemental material, sj-docx-3-cre-10.1177_02692155241258903 for The effectiveness of social prescribing in the management of long-term conditions in community-based adults: A systematic review and meta-analysis by Declan J O’Sullivan, Lindsay M Bearne, Janas M Harrington, Jefferson R Cardoso and Joseph G McVeigh in Clinical Rehabilitation
Supplemental Material
sj-docx-4-cre-10.1177_02692155241258903 - Supplemental material for The effectiveness of social prescribing in the management of long-term conditions in community-based adults: A systematic review and meta-analysis
Supplemental material, sj-docx-4-cre-10.1177_02692155241258903 for The effectiveness of social prescribing in the management of long-term conditions in community-based adults: A systematic review and meta-analysis by Declan J O’Sullivan, Lindsay M Bearne, Janas M Harrington, Jefferson R Cardoso and Joseph G McVeigh in Clinical Rehabilitation
Supplemental Material
sj-pdf-5-cre-10.1177_02692155241258903 - Supplemental material for The effectiveness of social prescribing in the management of long-term conditions in community-based adults: A systematic review and meta-analysis
Supplemental material, sj-pdf-5-cre-10.1177_02692155241258903 for The effectiveness of social prescribing in the management of long-term conditions in community-based adults: A systematic review and meta-analysis by Declan J O’Sullivan, Lindsay M Bearne, Janas M Harrington, Jefferson R Cardoso and Joseph G McVeigh in Clinical Rehabilitation
Footnotes
Author contributions
Concept/idea/research design were done by D.J OS., J.M H., L.M B., and J.G McV. Writing Review and Editing were done by D.J OS., J.M H., L.M B., J.G McV., and J.R C. Data collection was done by D.J OS. and J.G McV. Data analysis was done by D.J OS., J.G McV. and J.R C. Project management was done by D.J OS. and J.G McV. Providing institutional liaisons was done by J.G McV. Consultation (including review of manuscript before submitting) was done by J.M H, L.M B., J.G McV. and J.R C.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental materials
Please find the following supplemental material visualised and available to download via Figshare in the hyperlink below. Where there are more than one item, you can scroll through each tab to see each separate item 10.6084/m9.figshare.24099798
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.