
Abstract
Objective
The aim of this systematic review is to identify currently available tele-assessments for motor impairments of the upper extremity in adults after a stroke and to assess their psychometric properties and clinical utility.
Data sources
We searched for studies describing the psychometric properties of tele-assessments for the motor function of the upper extremity. A systematic search was conducted in the Cumulative Index to Nursing and Allied Health Literature, Medline via OVID, Embase, The Cochrane Library, Scopus, Web of Science and Institute of Electrical and Electronics Engineers Xplore from inception until 30 April 2024.
Review methods
The quality assessment for the included studies and the rating of the psychometric properties were performed using the COSMIN Risk of Bias Checklist for systematic reviews of patient-reported outcome measures.
Results
A total of 12 studies (N = 3912) describing 11 tele-assessments met the predefined inclusion criteria. The included assessments were heterogeneous in terms of quality and psychometric properties and risk of bias. None of the tele-assessments currently meets the criteria of clinical utility to be recommended for clinical practice without restriction.
Conclusion
The quality and clinical utility of tele-assessments varied widely, suggesting a cautious consideration for immediate clinical practice application. There is potential for tele-assessments in clinical practice, but the clinical benefits need to be improved by simplifying the complexity of tele-assessments.
Registration Number
CRD42022335035.
Introduction
In mitigating the escalating costs of stroke rehabilitation, the trend has shifted from extended inpatient care to early discharge, emphasizing outpatient and home-based therapy. 1 Within this context, and accelerated by the COVID-19 pandemic, tele-rehabilitation (i.e., providing rehabilitative treatments “at a distance” between the clinician and the patient's home) has gained significant interest.2,3
Tele-rehabilitation recommendations emphasise the relevance of therapist monitoring and adjusting interventions based on progress towards established goals. 4 Reliable and valid measurements for assessing the motor function following stroke are, therefore, essential. 5 Tele-assessments like in-person evaluations must exhibit reliability, validity and sensitivity to change. 6
Previous work in post-stroke motor rehabilitation has focused on assessments provided in person (whether technology-supported or not)7–10 and interventions delivered remotely.11–13 Whilst adapting questionnaires for remote use appears straightforward 14 ; “hands-on” assessments present greater challenges in remote settings. As of now, there is no comprehensive overview of such “hands-on” assessments for gauging the motor function and activity after stroke in remote contexts.
This review aims to identify clinically ready-to-use tele-assessments for the evaluation of the motor function and activity of the upper extremity post-stroke and to systematically investigate their measurement properties. Additionally, the clinical utility of these tele-assessments will be evaluated, and recommendations for their use will be provided.
Methods
This systematic review adheres to the “reporting guideline for systematic reviews of outcome measurement instruments” (PRISMA-COSMIN for OMIs, currently in development) 15 and is registered in PROSPERO (CRD42022335035). The qualities of the studies and the tele-assessments of the included papers are assessed separately. When necessary, additional data or clarifications were requested from the authors.
Studies were included if they met the following criteria: they tested a tele-assessment in adults (≥18) post-stroke; they reported about a tele-assessment, which measures the motor function or activity of the upper extremity and was either developed for remote use or adapted from a traditional in-person assessment for remote use; the tele-assessment measures the movement quality (i.e., how the movement was executed) rather than just quantity; the tele-assessment is clinically ready to use (i.e., completed remote testing, either between research facility and participants’ homes or between two separate rooms in a research facility); and the study was published in a peer-reviewed, scientific journal. Moreover, studies that solely provide information on patients’ or therapists’ perspectives or opinions towards tele-assessments and reviews were excluded.
Searches and Data Sources
A systematic literature search was initially conducted in July 2022 and last updated on 30 April 2024. Given the interdisciplinary nature of this topic, we incorporated the following seven databases: Cumulative Index to Nursing and Allied Health Literature (CINAHL), Medline via OVID, Embase, The Cochrane Library, Scopus, Web of Science and IEEE Xplore. The search strings were built using the Boolean operator OR between synonyms and the Boolean operator AND between concepts (“stroke”, “sensorimotor”, “teleassessment” and “upper extremity”). Controlled vocabulary and indexing systems as well as free text words were used for the search. The search strings were adapted to the respective databases. All search strings were developed in consultation with a librarian at the University of Zurich in April 2022. We included studies in all languages and of all publication dates. We translated two studies that were only available in Chinese using DeepL to be able to appraise the full texts. A full-search strategy for the CINAHL can be found in Supplement Table 1. The search strategies of the other databases are available on request from the authors.
All initially identified hits were imported into “Covidence”. 16 Duplicates were removed automatically and manually. Four reviewers screened titles and abstracts for eligibility, with each abstract being reviewed by at least two of these reviewers. Conflicts were resolved by an independent third reviewer. The remaining articles were subjected to full-text screening, whereby each article was evaluated independently by two of the same reviewers. Conflicts were resolved in team discussion.
The first author conducted data extraction for the included studies. For quality assurance, a second reviewer independently extracted a random data sample for comparison. A structured form (see online Supplementary Table 2) was used to extract the study characteristics (e.g. evidence level), characteristics of the tele-assessments (e.g. description of the assessment, psychometric properties) and results (e.g. usability the described tele-assessment).
Study Quality Assessment
We assessed the risk of bias (methodological quality) of the included studies using an adapted version of the COSMIN Risk of Bias Checklist for systematic reviews of patient-reported outcome measures. 17 The psychometric properties of reliability (COSMIN Box 6), measurement error (COSMIN Box 7), criterion validity (COSMIN Box 8), hypotheses testing for construct validity–convergent validity (COSMIN Box 9a) and construct approach (COSMIN Box 10b) of the included studies were analysed by two reviewers independently. Each criterion's (box's) score was determined by the lowest value among the respective items. 18 In addition, we applied the criteria for good measurement properties on a three-point rating scale (sufficient, insufficient and indeterminate). 19 Discrepancies were resolved with discussion. The criteria for good measurement properties used in this systematic review are listed in Supplement Table 4.
Clinical Utility
We used two tools to critically appraise the clinical utility of the tele-assessments. First, the overall clinical usefulness according to Fawcett 20 was chosen for its systematic approach to provide an in-depth qualitative overview. Here, clinical utility is described by the factors of cost, time, energy and effort, portability and acceptability. Second, the quantitative 10-point clinical utility framework by Tyson and Connell 21 was applied. Assessments scoring 9 or 10 are recommended for clinical use. 21
Results
The search resulted in 3912 publications, of which 80 were evaluated in full text, and 12 were included for data extraction (Figure 1).22–33 These 12 studies described 11 different (versions of) tele-assessments measuring the motor function or activity. Thirty-two studies were excluded during full text screening either because they had not been tested at a distance34–57 or were generally still in a very early stage of development.58–64 Another study did not fully meet the inclusion criteria. 53 We mention this special case because the authors have evaluated usability, but not specifically the psychometric properties of the assessment at a distance.
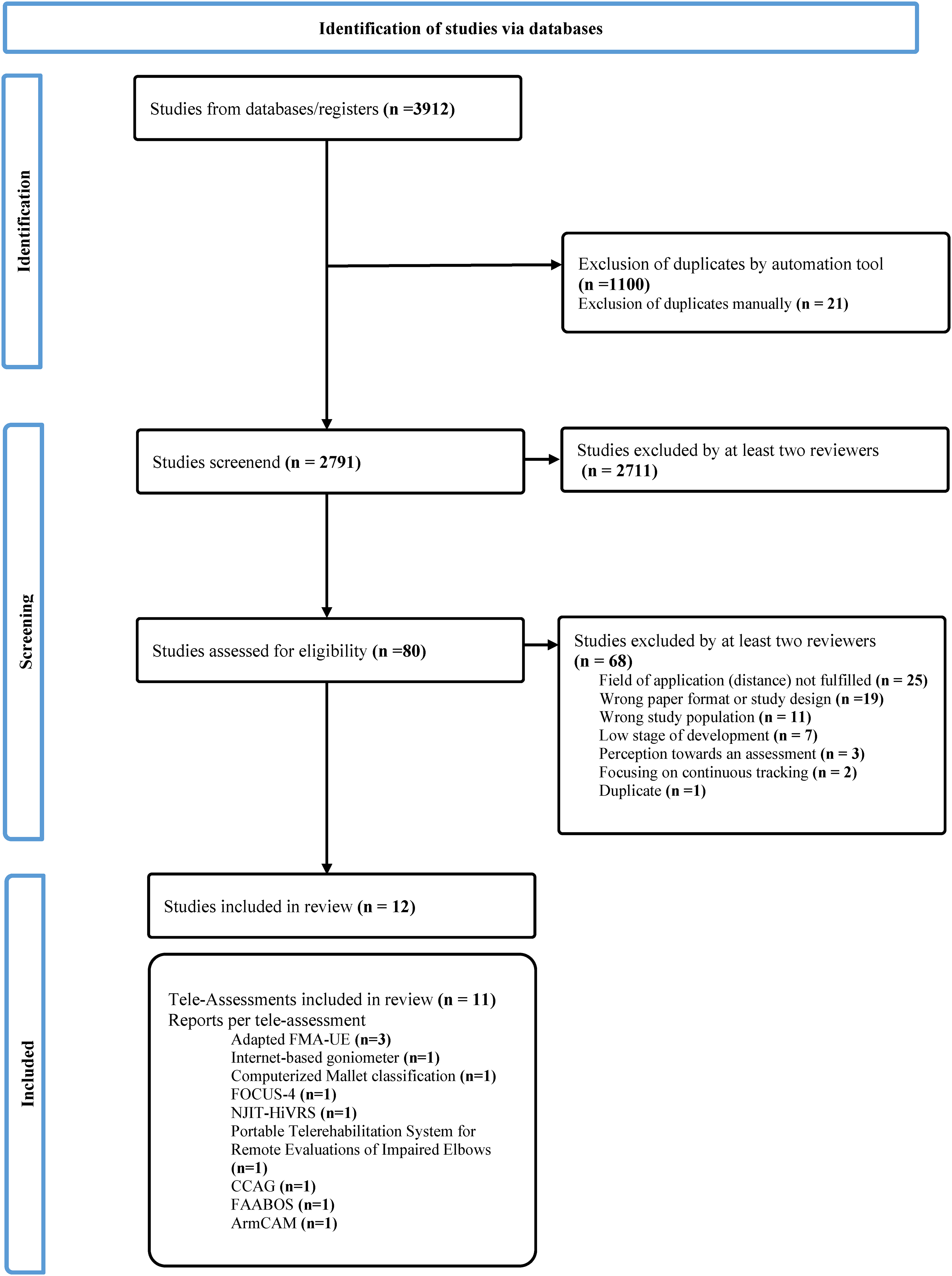
Preferred reporting items for systematic and meta-analysis (PRISMA) flow chart.
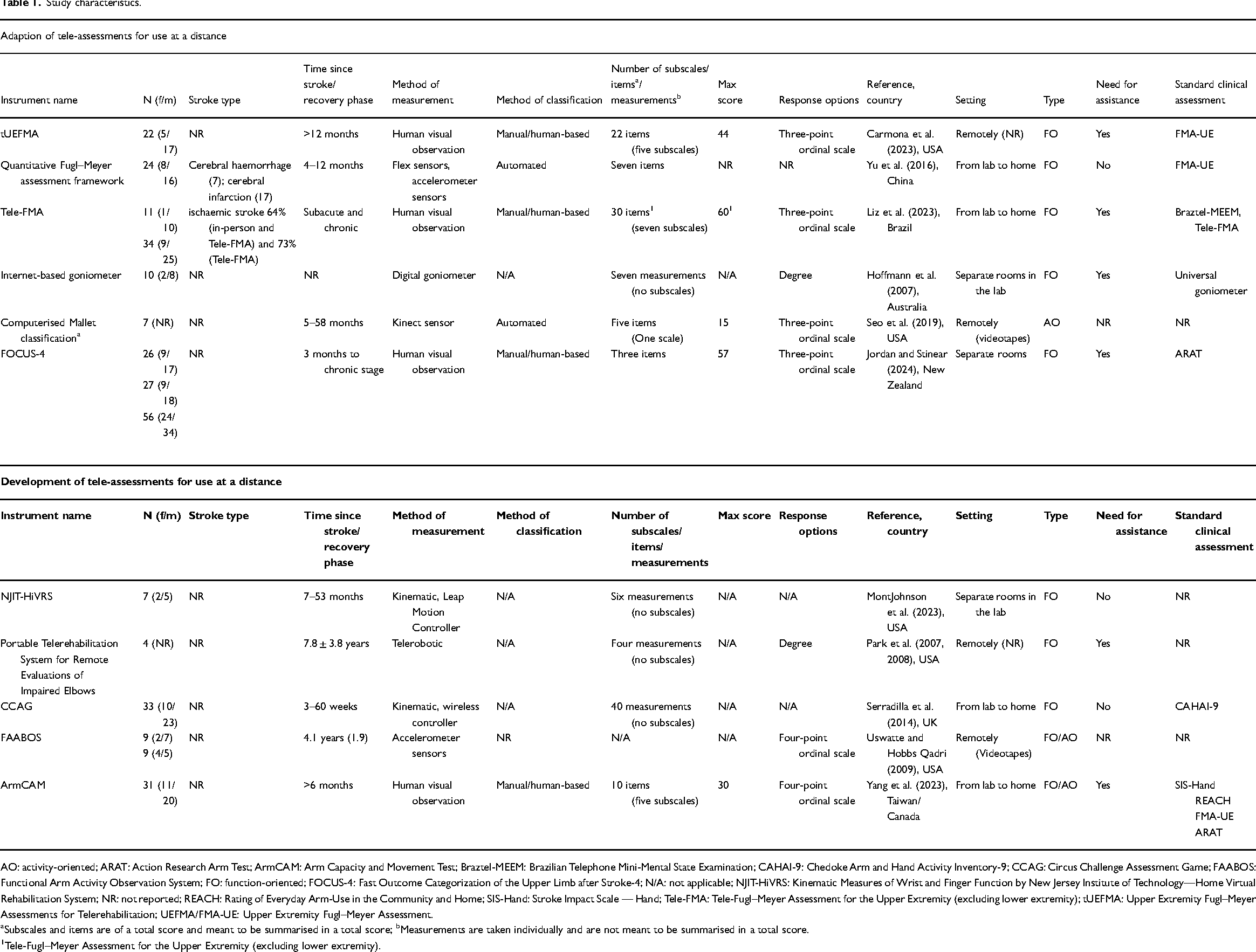
The characteristics of the 12 included studies are presented in Table 1. Six out of the 11 tele-assessments investigated modifications of existing clinical assessments, and five described assessments specifically developed for remote use (Table 1). Sample sizes in the 12 studies ranged from four to 56 individuals. All studies enrolled participants who were more than three months post-stroke.
Study characteristics.
AO: activity-oriented; ARAT: Action Research Arm Test; ArmCAM: Arm Capacity and Movement Test; Braztel-MEEM: Brazilian Telephone Mini-Mental State Examination; CAHAI-9: Chedoke Arm and Hand Activity Inventory-9; CCAG: Circus Challenge Assessment Game; FAABOS: Functional Arm Activity Observation System; FO: function-oriented; FOCUS-4: Fast Outcome Categorization of the Upper Limb after Stroke-4; N/A: not applicable; NJIT-HiVRS: Kinematic Measures of Wrist and Finger Function by New Jersey Institute of Technology—Home Virtual Rehabilitation System; NR: not reported; REACH: Rating of Everyday Arm-Use in the Community and Home; SIS-Hand: Stroke Impact Scale — Hand; Tele-FMA: Tele-Fugl–Meyer Assessment for the Upper Extremity (excluding lower extremity); tUEFMA: Upper Extremity Fugl–Meyer Assessments for Telerehabilitation; UEFMA/FMA-UE: Upper Extremity Fugl–Meyer Assessment.
Subscales and items are of a total score and meant to be summarised in a total score; bMeasurements are taken individually and are not meant to be summarised in a total score.
Tele-Fugl–Meyer Assessment for the Upper Extremity (excluding lower extremity).
Four tele-assessments were tested between the research facility and the participants’ homes and two in a research facility between separate rooms. Two studies validated movement scoring from video recordings by comparing them to in-person scoring. Authors of three studies did not provide further detail about the setup of remote testing (upon request; Table 1). The Fugl–Meyer assessment (FMA; n = 3), range of motion measurement using a goniometer (n = 1), Mallet classification (n = 1) and Action Research Arm Test (ARAT; n = 1) are established clinical assessments that were adapted for use at a distance.22–26,33
According to the respective authors, the quantitative Fugl–Meyer assessment framework, 23 Kinematic Measures of Wrist and Finger Function by the New Jersey Institute of Technology — Home Virtual Rehabilitation System (NJIT-HiVRS) 27 and Circus Challenge Assessment Game (CCAG) 30 were designed, such that people after a stroke can set them up without assistance. For other included tele-assessments, it was explicitly stated that they were conducted with assistance involving clinicians at a distance or caregivers during the process (Table 1).22,24,25,29,32,33
Quality Assessment
The results of the quality assessment and detailed information on the psychometric properties of the included tele-assessments are reported in Supplement Tables 3 and 5. Seven tele-assessments had at least one measurement property classified as “sufficient” in a study with the methodological quality determined as at least “adequate”.22–25,30–32
Reliability was assessed for nine of the 11 included tele-assessments.22–27,31–33 Sufficient reliability, a high-evidence level, was found for the Tele-FMA, 24 tUEFMA (low-evidence level), Fast Outcome Categorization of the Upper Limb after Stroke-4 (FOCUS-4; low-evidence level), internet-based goniometer (high-evidence level), Functional Arm Activity Observation System (FAABOS; high-evidence level) and Arm Capacity and Movement Test (ArmCAM; high-evidence level).22,25,31–33
The measurement error was evaluated for six of the 11 included tele-assessments.22,24–26,31,32 It was deemed sufficient for Tele-FMA (high-evidence level). 24 For the ArmCAM (high-evidence level), 32 the measurement error was rated indeterminate for four tele-assessments.22,25,26,31
The criterion validity was assessed for five of the 11 tele-assessments.22,24,27,30,32 This item was rated sufficient for the tUEFMA (high-evidence level), Tele-FMA (high-evidence level), Circus Challenge Assessment Game (high-evidence level) and ArmCAM (high-evidence level).22,24,30,32
The established gold standard of the comparison measurement for the tUEFMA, the Tele-FMA and the ArmCAM was the FMA-UE, whilst for the Circus Challenge Assessment Game, the Chedoke Arm and Hand Assessment Inventory (CAHAI). For the Tele-FMA, the Stroke Impact Scale for Hand was additionally used as the gold standard for comparison. ArmCAM was additionally compared with the Stroke Impact Scale for Hand, the Rating of Everyday Arm-Use in the Community and Home (REACH scale) and the Action Research Arm Test (ARAT) for a subgroup. The criterion validity for the NJIT-HiVRS was rated insufficient because some measurements were below 0.70. 27 An overview of the psychometric properties of the included tele-assessments is provided in Table 2.
Psychometric properties of the included tele-assessments.
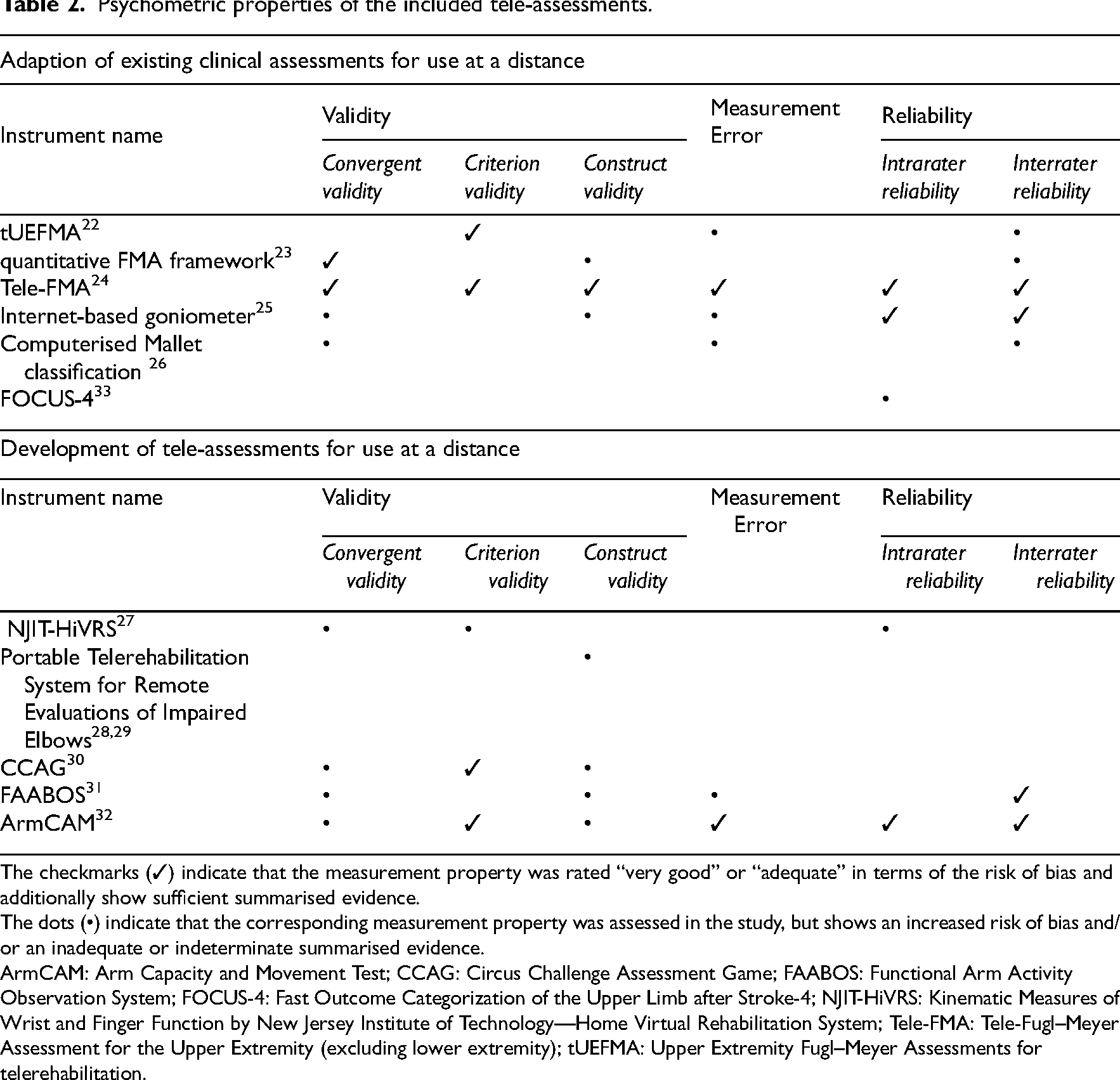
The checkmarks (✓) indicate that the measurement property was rated “very good” or “adequate” in terms of the risk of bias and additionally show sufficient summarised evidence.
The dots (•) indicate that the corresponding measurement property was assessed in the study, but shows an increased risk of bias and/or an inadequate or indeterminate summarised evidence.
ArmCAM: Arm Capacity and Movement Test; CCAG: Circus Challenge Assessment Game; FAABOS: Functional Arm Activity Observation System; FOCUS-4: Fast Outcome Categorization of the Upper Limb after Stroke-4; NJIT-HiVRS: Kinematic Measures of Wrist and Finger Function by New Jersey Institute of Technology—Home Virtual Rehabilitation System; Tele-FMA: Tele-Fugl–Meyer Assessment for the Upper Extremity (excluding lower extremity); tUEFMA: Upper Extremity Fugl–Meyer Assessments for telerehabilitation.
Supplement Table 5 shows an overview of the evidence of hypothesis testing for construct validity and responsiveness.
Clinical Utility of Tele-Assessments
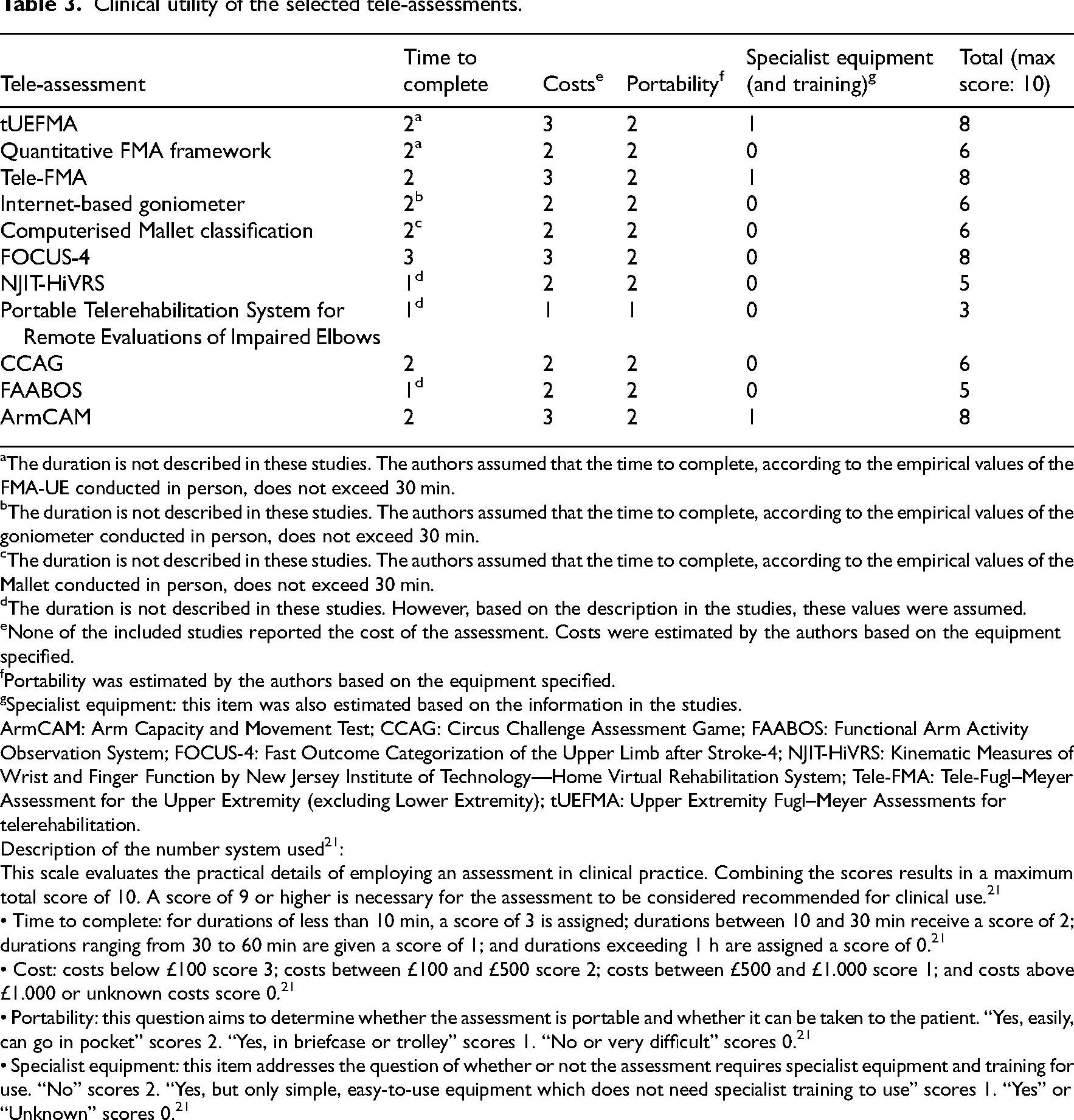
We describe the clinical utility according to Fawcett. 20 All studies reported what additional technical equipment was required. In addition to commercially available hardware (e.g. phone, computer, off-the-shelf cameras and Kinect camera) and software (e.g. video conferencing programs), several of the tele-assessments require further equipment such as accelerometer sensors, telerehabilitation systems, or a Leap Motion Controller (LMC, UltraLeap, California, USA).23,25–30 The authors of three studies reported that their tele-assessment is cost-effective because of the low-cost equipment.22,26,30 One research group deals with the high cost of their tele-assessment by offering leasing options. 29 Time to administer is outlined in four studies, varying between 5 min and approximately 20 min.24,30,32,33 Information on training effort and assistance (item Energy and Effort 20 ) is given for nine out of 11 tele-assessments.22–26,29,30,32,33 All selected studies previously examined use at a distance (either home setting, room to room or otherwise remotely); hence, we assumed that all included tele-assessments are portable. In one study, the System Usability Scale was used to draw conclusions about usability and acceptability. 27 In two other studies, it was reported that only some of the participants were satisfied with the home setting requirements.23,24 However, in one of these two studies, acceptance was reported by almost half of the participants (41%). 24 Further details on clinical utility are shown in Supplement Table 6. Based on Tyson and Connell, 21 none of the tele-assessments met the criteria for sufficient clinical utility (Table 3). We requested missing information from the authors, and in cases of a non-response, we made estimates using available evidence and clinical expertise. For the cost calculations, common household technologies (e.g. laptop and smartphone) were assumed and excluded from the calculation.
Clinical utility of the selected tele-assessments.
The duration is not described in these studies. The authors assumed that the time to complete, according to the empirical values of the FMA-UE conducted in person, does not exceed 30 min.
The duration is not described in these studies. The authors assumed that the time to complete, according to the empirical values of the goniometer conducted in person, does not exceed 30 min.
The duration is not described in these studies. The authors assumed that the time to complete, according to the empirical values of the Mallet conducted in person, does not exceed 30 min.
The duration is not described in these studies. However, based on the description in the studies, these values were assumed.
None of the included studies reported the cost of the assessment. Costs were estimated by the authors based on the equipment specified.
Portability was estimated by the authors based on the equipment specified.
Specialist equipment: this item was also estimated based on the information in the studies.
ArmCAM: Arm Capacity and Movement Test; CCAG: Circus Challenge Assessment Game; FAABOS: Functional Arm Activity Observation System; FOCUS-4: Fast Outcome Categorization of the Upper Limb after Stroke-4; NJIT-HiVRS: Kinematic Measures of Wrist and Finger Function by New Jersey Institute of Technology—Home Virtual Rehabilitation System; Tele-FMA: Tele-Fugl–Meyer Assessment for the Upper Extremity (excluding Lower Extremity); tUEFMA: Upper Extremity Fugl–Meyer Assessments for telerehabilitation.
Description of the number system used 21 :
This scale evaluates the practical details of employing an assessment in clinical practice. Combining the scores results in a maximum total score of 10. A score of 9 or higher is necessary for the assessment to be considered recommended for clinical use. 21
• Time to complete: for durations of less than 10 min, a score of 3 is assigned; durations between 10 and 30 min receive a score of 2; durations ranging from 30 to 60 min are given a score of 1; and durations exceeding 1 h are assigned a score of 0. 21
• Cost: costs below £100 score 3; costs between £100 and £500 score 2; costs between £500 and £1.000 score 1; and costs above £1.000 or unknown costs score 0. 21
• Portability: this question aims to determine whether the assessment is portable and whether it can be taken to the patient. “Yes, easily, can go in pocket” scores 2. “Yes, in briefcase or trolley” scores 1. “No or very difficult” scores 0. 21
• Specialist equipment: this item addresses the question of whether or not the assessment requires specialist equipment and training for use. “No” scores 2. “Yes, but only simple, easy-to-use equipment which does not need specialist training to use” scores 1. “Yes” or “Unknown” scores 0. 21
Discussion
To our knowledge, this is the first review to describe and evaluate the measurement properties and clinical utility of the remote tele-assessments of the motor function and activity after stroke. We identified 11 tele-assessments in 12 studies that were examined for remote use (Table 1). The Mallet classification adapted for remote use was conducted in the study with post-stroke patients. It is important to emphasise that this classification for assessing brachial plexus palsy lacks prior validation for post-stroke use. 26 The quality of the tele-assessments in terms of the measurement properties varied from “sufficient” to “insufficient” and methodological quality from “inadequate” to “very good”. The included studies showed a high degree of heterogeneity both in terms of the assessments themselves and the methods conducted for data collection and interpretation. This underlines the wide range of quality of the tele-assessments included. This finding also precluded a meaningful comparison between the tele-assessments, making it difficult to draw overarching conclusions regarding the overall validity and reliability of tele-assessments. Such conclusions must be drawn on an individual basis.
Prior reviews focused on a distinct category of measuring the motor function, for example, wearable devices like sensors.65,66 In addition, clinical utility was not addressed in these reviews. Appropriate clinical utility is an important key element for implementation in clinical practice, which must be considered in the development and contribution of tele-assessments. 67 Whilst some of the tele-assessments we included demonstrated strong utility scores, none met the critical threshold of nine points, limiting our ability to make unreserved recommendations for clinical practice. Key limiting factors are technical considerations and/or training. 67 All included tele-assessments require special equipment and/or training. In our context, this implies the following example: specialised tele-rehabilitation interfaces are needed,29,30 or training of caregivers is necessary to assist patients post-stroke in conducting the assessment.24,33 One added value of tele-rehabilitation is that it should save costs in the healthcare system. To minimise entry barriers for the implementation of tele-assessments and ensure the ongoing use of tele-rehabilitation, we recommend ensuring that the necessary equipment and training and general costs are kept at a minimum.
In the process, we found 32 tele-assessments that are at an early stage of development.34–64 These technologies have not yet undergone comprehensive testing for the use at a distance and did, therefore, not fulfil the inclusion criteria for this review. However, they show great potential in attaining clinical relevance with further refinement soon. They underline the dynamic and rapidly evolving nature of the domain of tele-assessments.
Two of these studies focused on establishing a ground truth for artificial intelligence (AI) applications in the assessment domain.62,63 Whilst we did not specifically search for AI-based assessments, we came across studies establishing a ground truth for AI applications during the whole literature search and selection process. We, therefore, anticipate that remote assessments will increasingly incorporate the AI technology in the future.
We acknowledge several limitations in this review. The findings of this review were constrained by incomplete reporting in the studies we included. Despite our efforts to request missing information from the authors, the responses were often missing. Therefore, we estimated certain values when assessing the clinical utility. The utility scale refers to the costs in British Pounds. We see limitations in the generalisability of the results to other regions with differing socio-economic standards. Another essential consideration about clinical utility is whether or not the devices hold the necessary certification. This aspect is not mentioned in the clinical utility scale and is outside the scope of this review, but should be considered in future work on this topic. In addition, studies were excluded from this review if there were uncertainties regarding testing at a distance, and the relevant information could not be obtained from the corresponding authors. This may have led us to exclude relevant studies at an early stage, which may have had an impact on the analysis.
In conclusion, this systematic review provides an overview of the emerging field of tele-assessments. We identified 11 different tele-assessments in 12 studies. The assessment and study quality varied widely, ranging from poor to very good. Reducing complexity, including materials and training, and lowering costs are desirable ways to improve.
Clinical messages
None of the tele-assessments met the criteria for clinical utility, underscoring the need for cautious consideration in recommending their immediate adoption in clinical practice due to existing limitations.
There is potential for responsible use, although we recognise that their clinical utility needs to be further improved.
Supplemental Material
sj-docx-1-cre-10.1177_02692155241258867 - Supplemental material for Remotely Assessing Motor Function and Activity of the Upper Extremity After Stroke: A Systematic Review of Validity and Clinical Utility of Tele-Assessments
Supplemental material, sj-docx-1-cre-10.1177_02692155241258867 for Remotely Assessing Motor Function and Activity of the Upper Extremity After Stroke: A Systematic Review of Validity and Clinical Utility of Tele-Assessments by Lena Sauerzopf, Andreas R. Luft, Anna Baldissera, Sara Frey, Verena Klamroth-Marganska and Martina R. Spiess in Clinical Rehabilitation
Supplemental Material
sj-pdf-2-cre-10.1177_02692155241258867 - Supplemental material for Remotely Assessing Motor Function and Activity of the Upper Extremity After Stroke: A Systematic Review of Validity and Clinical Utility of Tele-Assessments
Supplemental material, sj-pdf-2-cre-10.1177_02692155241258867 for Remotely Assessing Motor Function and Activity of the Upper Extremity After Stroke: A Systematic Review of Validity and Clinical Utility of Tele-Assessments by Lena Sauerzopf, Andreas R. Luft, Anna Baldissera, Sara Frey, Verena Klamroth-Marganska and Martina R. Spiess in Clinical Rehabilitation
Footnotes
Acknowledgements
We thank Martina Gosteli, a librarian at the University of Zurich, for her support in developing the search strategy. We also thank the corresponding authors of the included studies for their time and efforts in responding to our emails. Furthermore, we thank our research interns Madita Hotz and Valeria Maeusli for their support.
Contributorship
In the Methods section, the contributorship in data collection and analysis is described in detail. L.S. created the first draft of the manuscript. M.S. and A.R. contributed their expertise in revising the manuscript and proofreading. All authors reviewed and edited the manuscript and approved the final document.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for this research and/or authorship for this article: This study was supported by the ZHAW Zurich University of Applied Sciences, School of Health Sciences, Institute of Occupational Therapy.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.