
Abstract
Objective
The purpose of this study was to assess the effects of adding electrical dry needling and thrust manipulation into a multimodal program of exercise, mobilization, and ultrasound in patients with lateral elbow tendinopathy.
Design
Randomized, single-blinded, multicenter, parallel-group trial.
Setting
Thirteen outpatient physical therapy clinics in nine different US states.
Participants
One hundred and forty-three participants (n = 143) with lateral elbow tendinopathy were randomized.
Intervention
Cervical spine manipulation, extremity manipulation, and percutaneous tendon electrical dry needling plus multimodal physical therapy (n = 73) or multimodal physical therapy (n = 70) alone.
Main measures
The primary outcome was elbow pain intensity and disability as measured by the Patient-Rated Tennis Elbow Evaluation at baseline, 1 week, 4 weeks, and 3 months. Secondary outcomes included the Numeric Pain Rating Scale, Tennis Elbow Functional Scale, Global Rating of Change, and medication intake.
Results
The 2 × 4 analysis of covariance demonstrated that individuals with lateral elbow tendinopathy receiving electrical dry needling and thrust manipulation plus multimodal physical therapy experienced significantly greater improvements in disability (Patient-Rated Tennis Elbow Evaluation: F = 19.675; P < 0.001), elbow pain intensity (Numeric Pain Rating Scale: F = 22.769; P < 0.001), and function (Tennis Elbow Function Scale: F = 13.269; P < 0.001) than those receiving multimodal physical therapy alone at 3 months. The between-group effect size was large for pain and disability (Patient-Rated Tennis Elbow Evaluation: standardized mean difference = 1.13; 95% confidence interval: 0.78, 1.48) in favor of the electrical dry needling and thrust manipulation group.
Conclusions
The inclusion of percutaneous tendon electrical dry needling and thrust manipulation into a multimodal program of exercise, mobilization and ultrasound was more effective than multimodal physical therapy alone in individuals with lateral elbow tendinopathy.
Introduction
Lateral elbow tendinopathy, also referred to as lateral epicondylalgia, lateral epicondylitis, and tennis elbow, is a common presentation of pain and resultant disability in the elbow.1,2 The overall incidence of lateral elbow tendinopathy is approximately 3%, and as high as 10% in those between 40 and 50 years of age in the United States. 3 Originally thought to be an inflammatory process of the common extensor tendon at the lateral epicondyle, lateral elbow tendinopathy has recently been identified as a pathology of the tendon at or close to its enthesis.2,4,5 Repeated mechanical loading in this area results in histological changes within the tendon.2,4–7 Importantly, other structures including the radial collateral ligament, annular ligament, radiocapitellar joint, radial nerve, and cervical spine should be included in the differential diagnosis.
Nonoperative management of lateral elbow tendinopathy includes physical therapy, injection (corticosteroid, platelet rich plasma, botulinum toxin),8–10 extracorporeal shockwave therapy11,12 and high-power laser therapy. 13 Multimodal physical therapy treatment programs including local manual therapy and exercise14,15 have shown beneficial effects in reducing pain and disability, and are supported in recent clinical practice guidelines. 2 Multimodal physical therapy seems to have similar benefits to corticosteroid injections in the short term (4–6 weeks),14,15 superior short-term success rates compared to wait and see, 14 and a much lower recurrence rate (5%) compared to corticosteroid injection (55%) at 1-year follow up. 15 Unfortunately, this type of multimodal approach seems to result in similar outcomes as wait and see intervention or corticosteroid injection/placebo injection at 1-year follow up.14,15
Other conservative treatments for lateral elbow tendinopathy including spinal thrust manipulation and needling therapies (dry needling and acupuncture) have recently gained popularity in the clinical setting, with some preliminary evidence to support its use in this patient population.16–24 Spinal thrust manipulation alone has been found to significantly increase pressure pain thresholds and pain-free grip strength in patients with lateral elbow tendinopathy in the short term.17,18 Dry needling in isolation has also been found to have equal to, or superior outcomes compared to corticosteroid injections,19,21 platelet-rich plasma injections, 23 and nonsteroidal anti-inflammatory drugs combined with counterforce bracing. 20 Similarly, acupuncture has been reported to exhibit a superior effect on pain reduction in patients with lateral elbow tendinopathy compared to nonsteroidal anti-inflammatory drugs and sham acupuncture. 24 The combined effects of thrust manipulation plus electrical dry needling have not been established in patients with lateral elbow tendinopathy. In a recent randomized trial on subacromial pain syndrome, the addition of thrust manipulation and electrical dry needling to a multimodal physical therapy treatment (i.e. local manual therapy, exercise, and electrothermal modalities) resulted in significantly greater reductions in pain and disability than multimodal physical therapy treatment alone. 16 Therefore, the purpose of this clinical trial was to investigate the effects of adding thrust manipulation and electrical dry needling to a multimodal physical therapy treatment program of manual therapy, exercise, and ultrasound in patients with lateral elbow tendinopathy. We hypothesized that individuals receiving thrust manipulation and electrical dry needling combined with a program of multimodal physical therapy would experience greater reductions in pain and disability than those receiving multimodal physical therapy alone.
Methods
This randomized, single-blinded, multicenter, parallel-group clinical trial was conducted following the Consolidated Standards of Reporting Trials extension for pragmatic clinical trials. 25 The trial was approved by the ethics committee at Universidad Rey Juan Carlos, Madrid, Spain (URJC-DPTO 11–2017) and the trial was prospectively registered (ClinicalTrials.gov: NCT03167710).
Participants and Procedure
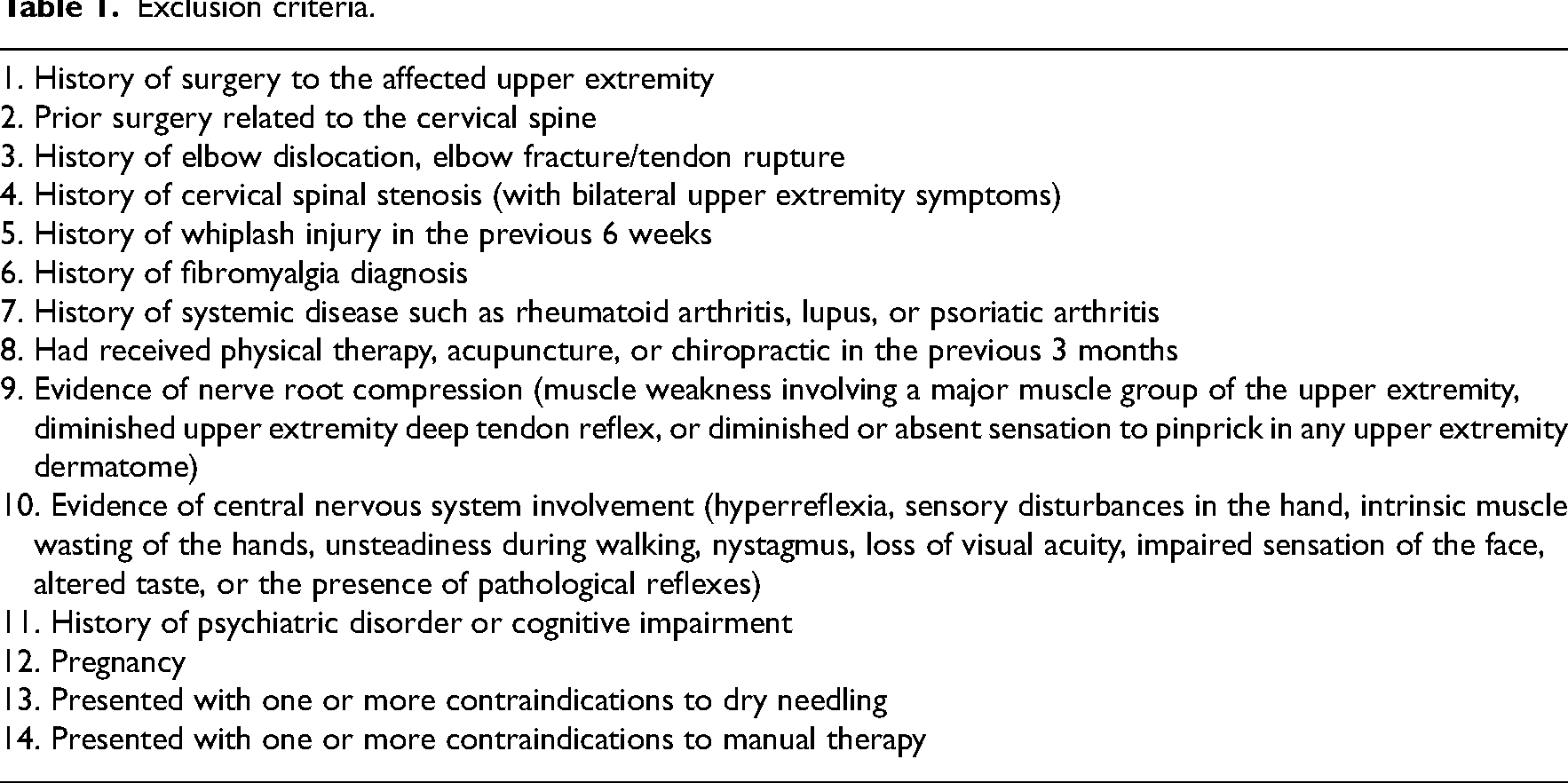
Consecutive individuals with lateral elbow tendinopathy from 13 outpatient physical therapy clinics in 9 different US states (Arizona, Maryland, Massachusetts, Minnesota, Montana, North Carolina, North Dakota, Oklahoma, and Wyoming) were screened for eligibility criteria and recruited over a 45-month period (from 15 June 2017 to 15 March 2021). To be eligible, patients had to (1) be between 18 and 60 years old, (2) meet the criteria for a clinical diagnosis of lateral elbow tendinopathy—[i.e. defined as two or more of the following: (a) pain on palpation over the lateral epicondyle and the associated common extensor unit, 26 (b) pain on gripping a hand dynamometer, 26 and (c) pain with stretching or contraction of the wrist extensor muscles 26 ], (3) have had lateral elbow and forearm symptoms for longer than 6 weeks, and (4) have an intensity of lateral elbow pain of at least 2 on the Numeric Pain Rating Scale (0–10). The exclusion criteria are described in Table 1.
Exclusion criteria.
Thirteen physical therapists (mean age, 39.7 years, standard deviation 8.9) delivered interventions in this trial. The clinicians had an average of 13.2 (standard deviation 9.2) years of clinical experience, had completed a 54-hour postgraduate certification program that included practical training in electrical dry needling for lateral elbow tendinopathy, and were current students in a 60-hour postgraduate certificate program that included practical training in nonthrust joint/soft-tissue mobilization and thrust-manipulation techniques to the cervical spine, radio-humeral joint, ulno-humeral joint, radiocarpal joint, and antebrachial region. All treating therapists were Fellows-in-Training within the American Physical Therapy Association-accredited, American Academy of Manipulative Therapy Fellowship in Orthopaedic Manual Physical Therapy program, had heterogeneous backgrounds in terms of prior manual therapy/orthopedic training, and worked in private outpatient physical therapy practice. All participating therapists were required to study a manual of standard operating procedures and participate in a 6-hour training session with a principal investigator to ensure the standardization of the protocol and treatment.
Following baseline examination, patients were randomly assigned to the (1) active comparison group: conventional physical therapy (exercise, elbow joint/soft-tissue mobilization, and ultrasound) or (2) experimental group: conventional physical therapy plus cervical spine/extremity thrust manipulation and electrical dry needling. Randomization was conducted using a computer-generated randomized table of numbers created by a statistician, not otherwise involved in the trial. Individual and sequentially numbered index cards with the random assignment were prepared, folded, and placed in sealed opaque envelopes for each of the 13 data collection sites. Each therapist was trained specifically in the study protocols and treated patients in both allocation groups; however, the clinicians administering the self-report outcome questionnaires were blinded to the patient's treatment group assignment. It was not possible to blind patients or treating therapists.
Interventions
All participants received up to eight treatment sessions at a frequency of twice per week over a 4-week period. The interventions were designed to treat lateral elbow tendinopathy. In either group, fewer treatment sessions could be completed, if symptom resolution occurred sooner. Both groups received a program of multimodal physical therapy which consisted of an impairment-based therapeutic eccentric exercise26–29 and stretching program, 30 impairment-based manual therapy 26 using Mulligan's mobilization with movement, 31 deep transverse friction massage,26,32–34 and therapeutic ultrasound34,35 (Sonicator, Mettler Electronics, Anaheim, California; 3 MHz, 1.5 W/cm2, 20% duty cycle) for 5 minutes over the elbow (Supplemental material—File 1). Although the 2022 clinical practice guidelines “do not recommend ultrasound as a stand-alone treatment” for lateral elbow tendinopathy, 2 there is limited evidence that continuous and/or pulsed ultrasound improves pain-free function (compared with chiropractic care and exercise) in the short term (6 weeks), 36 is more effective at reducing pain than placebo treatment (13 weeks), 37 and is superior to sham ultrasound for improvements in pain and function (6 weeks). 38 Exercises and stretching were initially taught, supervised, and gradually progressed by the treating therapist over the course of the treatment sessions. No further instructions on exercise were given after the last treatment visit. In addition to manual therapy, exercise, and ultrasound, patients allocated to the treatment group also received up to eight sessions of electrical dry needling at a frequency of 1–2 sessions per week for 20 minutes using an 8-point standardized protocol targeting intramuscular trigger points, musculotendinous junctions, teno-osseous attachments and/or periarticular tissue over the lateral elbow (Figure 1) and thrust manipulation to the elbow targeting the proximal radial head (Mill's technique)39,40 and/or humeroulnar joint, to the wrist targeting the scaphoid 41 and to the C5–C6 facet joints. 16 Descriptions of all interventions, including details regarding needle size, insertion site, angulation, depth, anatomical target, 42 manipulation,43–47 and electrical stimulation parameters47–53 are summarized in Supplemental material—File 1.
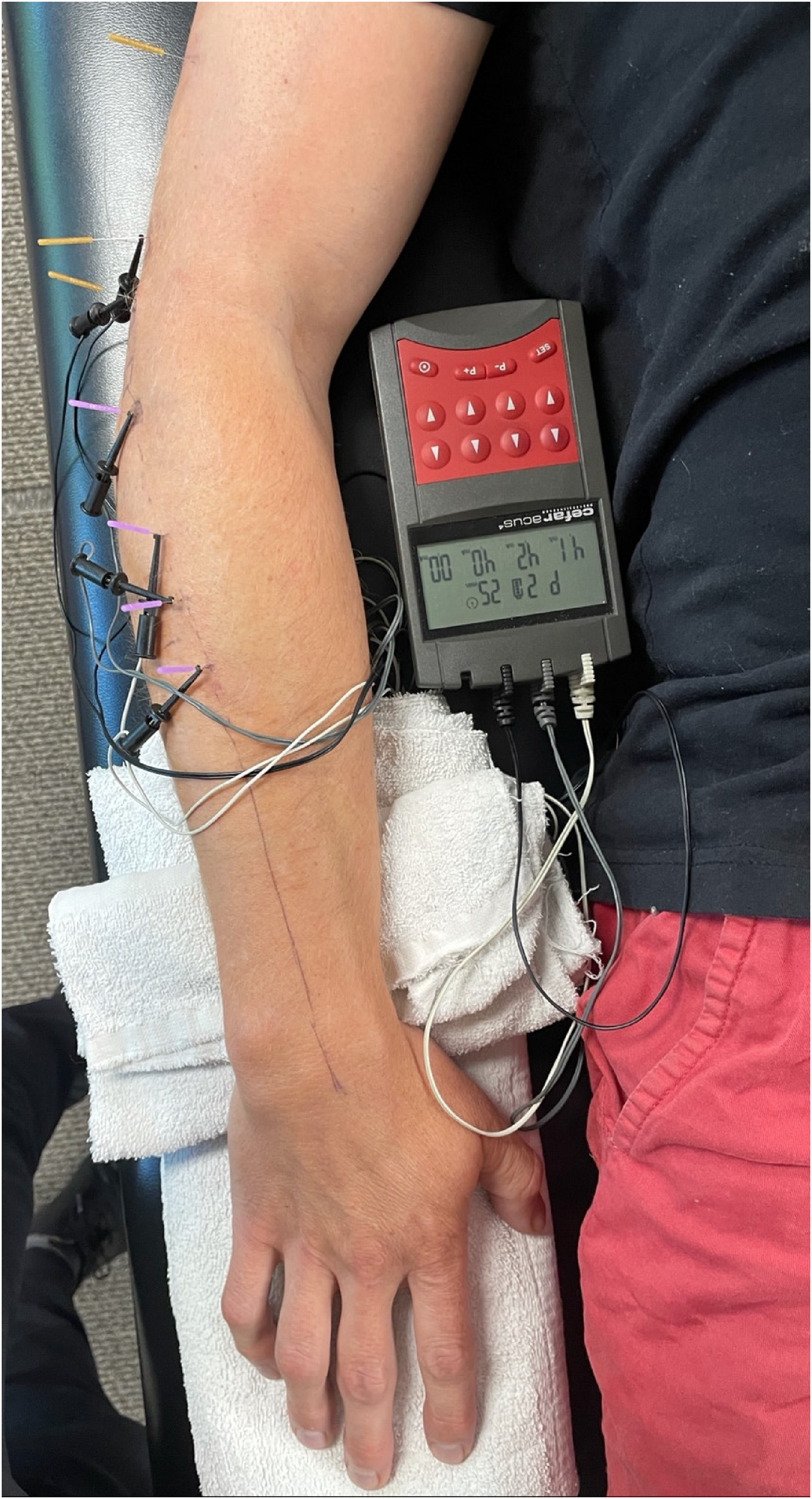
Standardized protocol for percutaneous tendon dry needling for lateral elbow tendinopathy.
Materials
The primary outcome was the Patient-Rated Tennis Elbow Evaluation42,54 assessed at baseline, 1 week, 4 weeks, and 3 months (the primary endpoint). Secondary outcomes included the Numeric Pain Rating Scale55,56 and Tennis Elbow Function Scale 57 assessed at 1 week, 4 weeks, and 3 months. Medication intake was assessed at baseline and 3 months and the Global Rating of Change 58 was assessed 3 months after the first treatment session.
The Patient-Rated Tennis Elbow Evaluation has been found to be both reliable and valid for capturing change in individuals with lateral elbow tendinopathy.42,59–61 The questionnaire includes a section for pain and another section for function. The first section consists of 5 questions scored from 0 (no pain) to 10 (most severe pain). The scores for the 5 pain questions are summed, and a total score out of 50 is reported. The function part of the questionnaire comprises 10 questions, the scores of which are summed and divided by 2, for a total score out of 50. Scores on the pain and function subscales are summed for a total score out of 100. 54 Lower scores indicate improved function. In patients with lateral elbow tendinopathy, the minimum clinically important difference for the Patient-Rated Tennis Elbow Evaluation has been reported to be 11 points. 62
The Numeric Pain-Rating Scale is an 11-point (0, no pain; 10, worst imaginable pain) used to assess the intensity of pain. 56 The Numeric Pain Rating Scale is a reliable and valid instrument to assess pain intensity.55,63,64 The minimum clinically important difference for the Numeric Pain Rating Scale has been shown to be 1.74 in patients with a variety of chronic pain conditions 65 ; thus, a change of 2 points or a 30% decrease in pain from baseline can be considered as the minimum clinically important difference in individuals with chronic musculoskeletal pain.65,66
The Tennis Elbow Function Scale is a 10-item, 5-point response self-report scale designed to measure elbow discomfort during the performance of personal care, household, work, and recreational activities.57,67 The Tennis Elbow Function Scale is a reliable, valid and responsive measure suitable for evaluating patients with lateral elbow tendinopathy. 57 The minimum clinically important difference for the Tennis Elbow Function Scale has not been established.
The Global Rating of Change is a 15-point questionnaire assessing the patients perceived recovery. This scale ranges from −7 (a very great deal worse) to 0 (about the same) to +7 (a very great deal better). Intermittent descriptors of worsening or improving are assigned values from −1 to −6 and +1 to +6, respectively. Scores of +4 and +5 have typically been indicative of moderate changes in patient status. 68
Patients were asked to report any adverse events. We defined adverse events as a sequelae of 1-week duration with any symptom perceived as distressing and unacceptable to the patient requiring further treatment.69,70 The treating therapists and patients in the treatment group were instructed to pay particular attention to the presence of ecchymosis and postneedling soreness.
Our sample size calculations were based on detecting a between-group moderate effect size16,22,71,72 of 0.57 in elbow-related disability (Patient-Rated Tennis Elbow Evaluation) at 3 months, using a 2-tailed test, an alpha level (α) of 0.05 and a desired power (β) of 90%. The estimated desired sample size was at least 65 participants per group. We anticipated a dropout rate of 10%. Therefore, 70 participants were required for each group.
Statistical Analysis
Statistical analysis was performed using Statistical Package for the Social Sciences software, version 28.0 (Chicago, IL), according to the intention-to-treat principle. Little's Missing Completely at Random test 71 was used to determine whether missing data points associated with dropouts were missing at random or missing for systematic reasons. Intention-to-treat analysis was performed by using expectation-maximization whereby missing data were computed using regression equations. Means, standard deviations and/or 95% confidence intervals were calculated for each variable. The Kolmogorov-Smirnov test revealed a normal distribution of the variables (P > 0.05). Baseline demographic and clinical variables were compared between groups using independent Student t-tests for continuous data and χ2 tests of independence for categorical data.
The effects of treatment on the Patient-Rated Tennis Elbow Evaluation, Numeric Pain Rating Scale, and Tennis Elbow Function Scale were each examined with a 2-by-4 mixed model analysis of covariance with treatment group as the between-subjects factor and time (baseline, 1 week, 4 weeks, and 3 months) as the within-subjects factor. Age and duration of symptoms were entered as covariates. For each analysis of covariance, the main hypothesis of interest was the 2-way interaction (group by time) with a Bonferroni-corrected alpha of 0.0125 (4 time points). We used χ2 tests to compare self-perceived improvement on the Global Rating of Change and changes in medication intake. To enable comparison of between-group effect sizes, Standardised Mean Differences in score were calculated by dividing mean score differences between groups by the pooled standard deviation. Number Needed to Treat was calculated using each definition for a successful outcome (a Global Rating of Change score of 5 or greater 58 at 3 months and a 50% improvement from baseline to 3 months on the Patient-Rated Tennis Elbow Evaluation). 73
Results
Participants
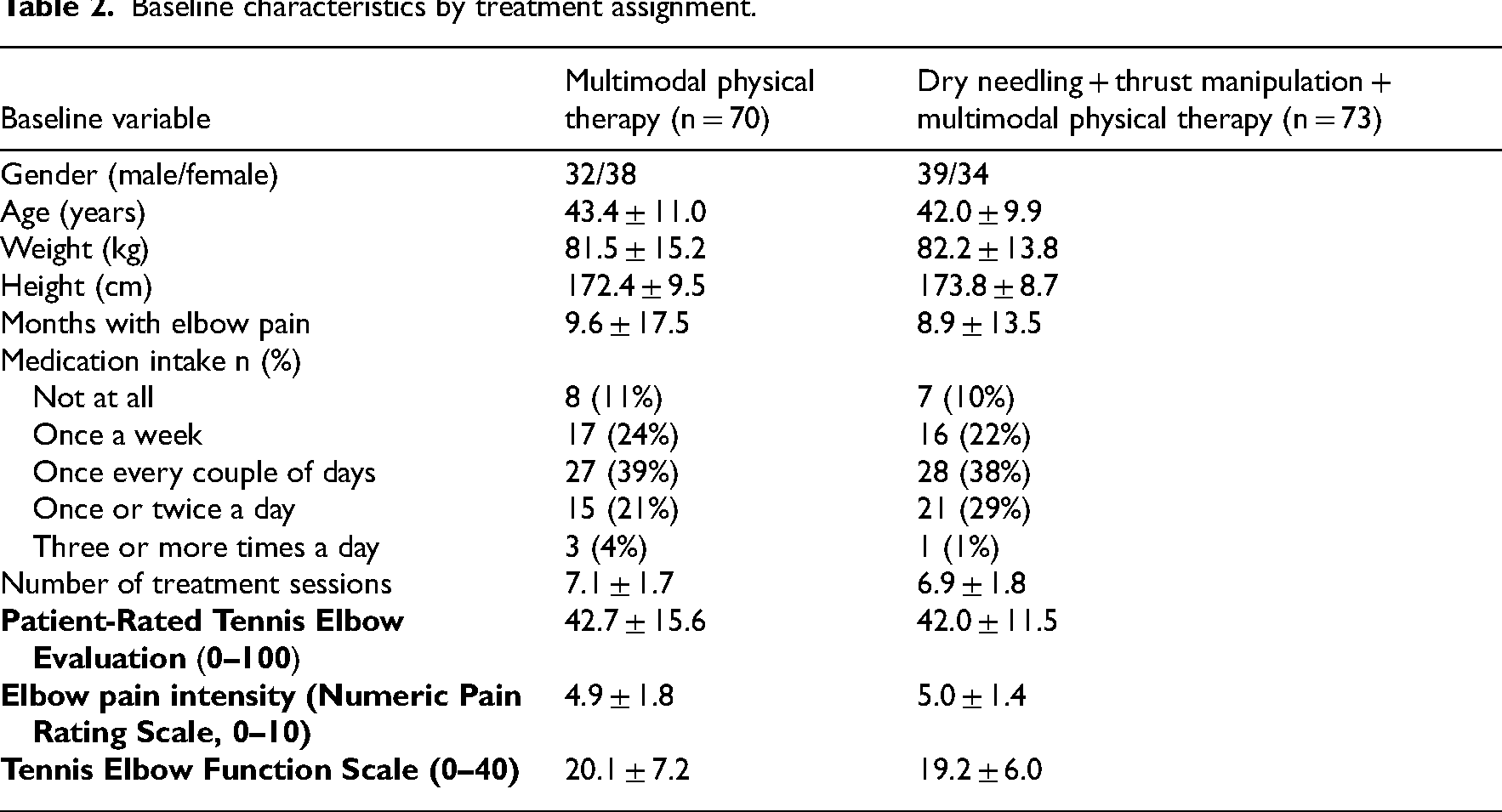
Between June 2017 and March 2021, 248 consecutive patients with lateral elbow tendinopathy were screened for eligibility (Figure 2). One hundred and forty-three (57.7%) satisfied all the inclusion criteria, agreed to participate, and were randomly allocated into the multimodal physical therapy (n = 70) group or the electrical dry needling and thrust manipulation plus multimodal physical therapy (n = 73) group. Randomization resulted in similar baseline characteristics for all variables (Table 2). The reasons for ineligibility are found in Figure 2, which provides a flow diagram of patient recruitment and retention. There was no significant difference (P = 0.473) between the mean number of completed treatment sessions for the dry needling and thrust manipulation group (mean: 6.90 ± 1.83) and the multimodal physical therapy group (mean: 7.11 ± 1.66). In total, 140 of the 143 patients completed all outcome measures through 3 months (98% follow up). Of the 3 patients that dropped out or failed to complete outcome measures, 2 were from the electrical dry needling and thrust manipulation group and 1 was from the multimodal physical therapy group. None of the participants in any group reported receiving other interventions during the study.
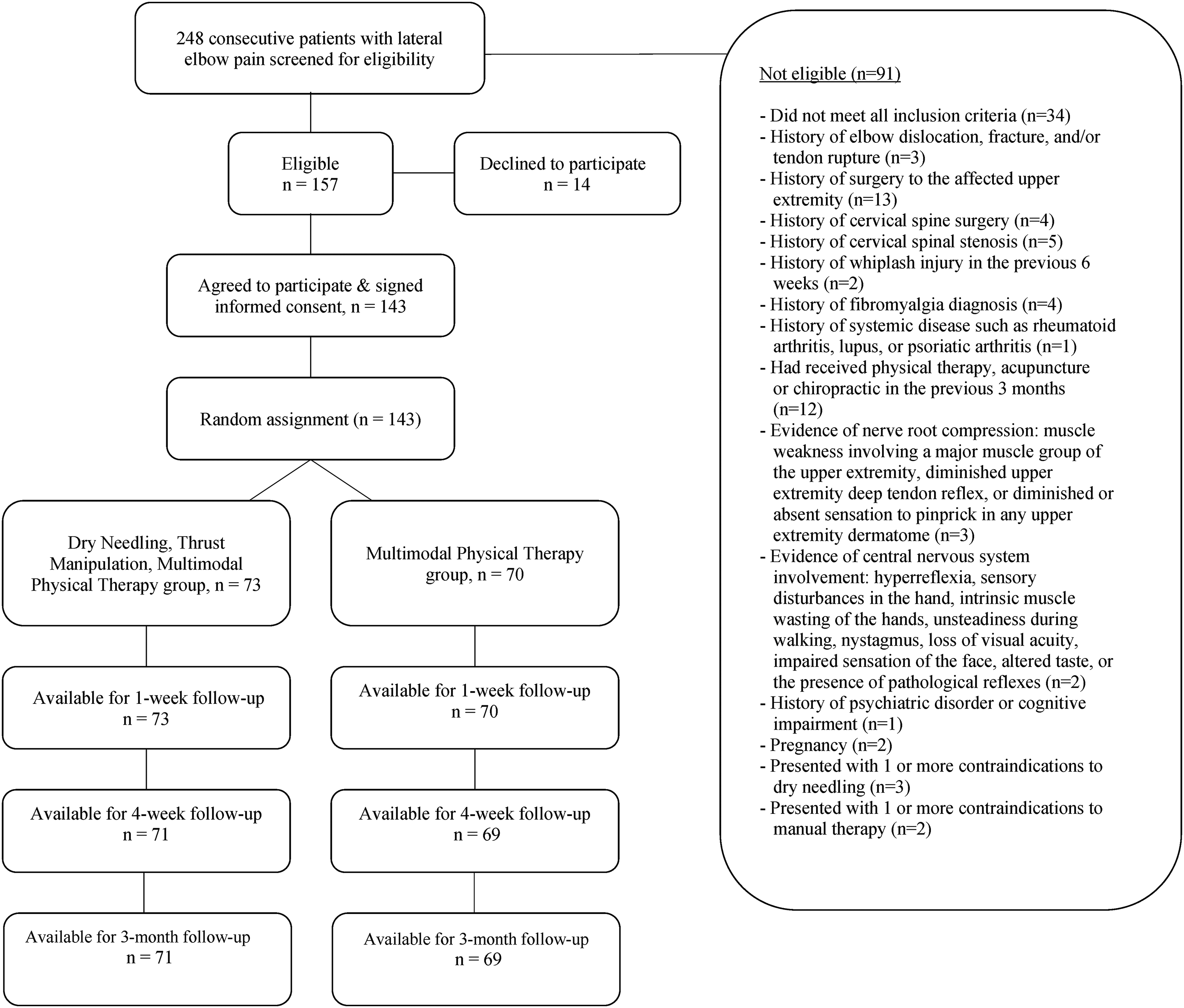
CONSORT flow diagram of patient recruitment and retention.
Baseline characteristics by treatment assignment.
Thirty-two patients assigned to the electrical dry needling and thrust manipulation group (43.8%) experienced postneedling muscle soreness and 13 (17.8%) experienced mild bruising (ecchymosis) which most commonly resolved spontaneously within 48 hours and 2–4 days, respectively. Seven patients (9.6%) in the dry needling and thrust manipulation group experienced bruising that lasted 5–7 days before spontaneously resolving. Two patients (2.7%) in the electrical dry needling and thrust manipulation group experienced drowsiness, headache, or nausea, which spontaneously resolved within several hours. No major adverse events were reported in the dry needling and thrust manipulation group.
Primary Outcome
Adjusting for baseline outcomes, the mixed model analysis of covariance revealed a significant group-by-time interaction for the primary outcome of elbow pain and disability (Patient-Rated Tennis Elbow Evaluation: F = 19.675; P < 0.001, Table 3). Patients in the electrical dry needling and thrust manipulation group experienced greater reductions in pain and disability at 1 week (Δ −6.1; 95% confidence interval: −9.6, −2.7; P < 0.001), 4 weeks (Δ −7.2; 95% confidence interval: −11.3, −3.2; P < 0.001), and 3 months (Δ −15.0; 95% confidence interval: −19.4, −10.6; P < 0.001) than those receiving multimodal physical therapy alone (Figure 3). For the Patient-Rated Tennis Elbow Evaluation, between-group effect sizes were medium at 1 week (standardized mean difference: 0.58; 95% confidence interval: 0.25, 0.92), medium at 4 weeks (standardized mean difference: 0.60; 95% confidence interval: 0.26, 0.93), and large at 3 months (standardized mean difference: 1.13; 95% confidence interval: 0.78, 1.48) after the first treatment session in favor of the electrical dry needling and thrust manipulation group.
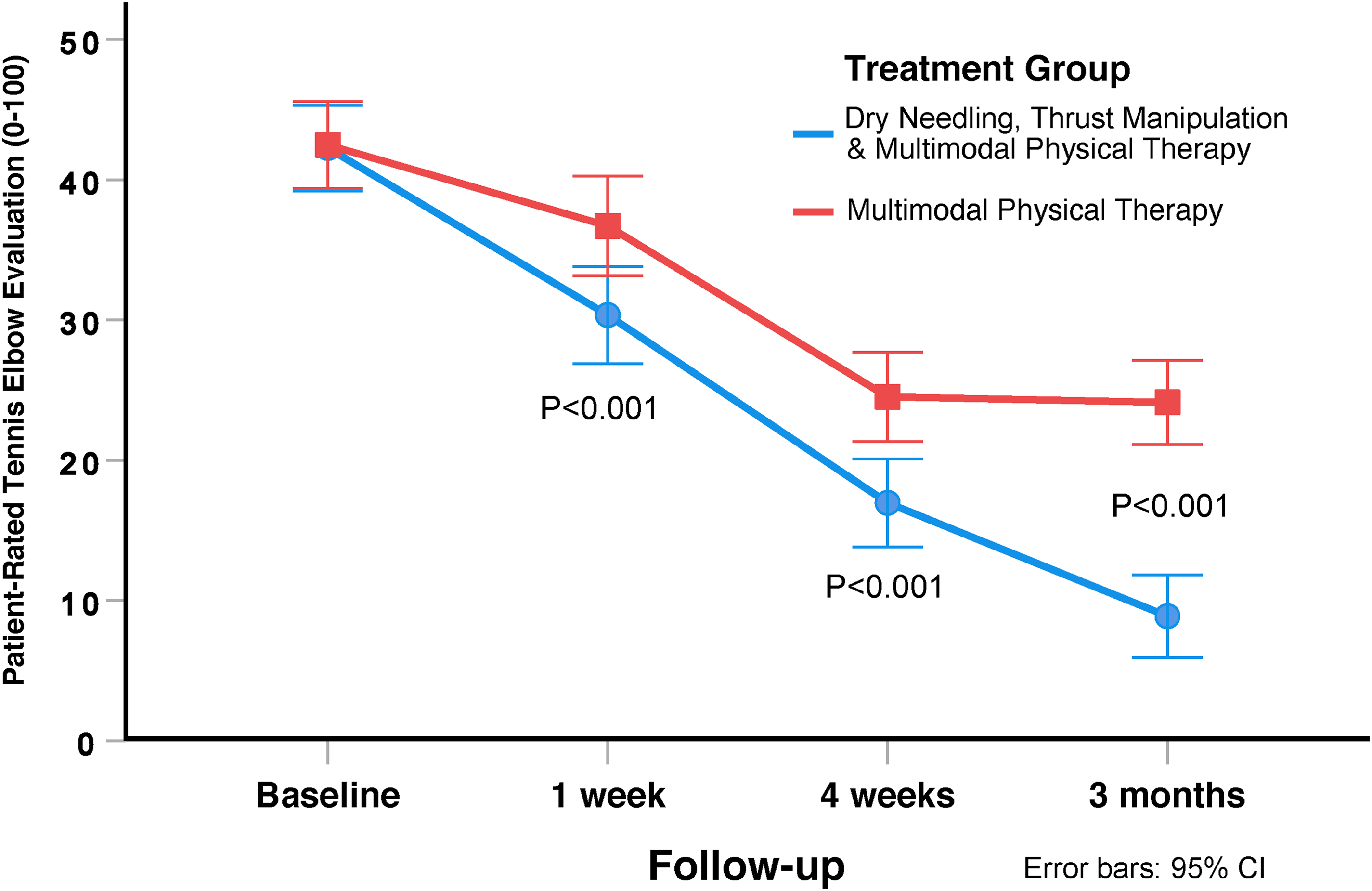
Evolution of elbow pain related disability (Patient-Rated Tennis Elbow Evaluation) throughout the course of the study, stratified by randomized treatment assignment. Values are mean and standard error.
Within-group and between-group mean scores by randomized treatment assignment.
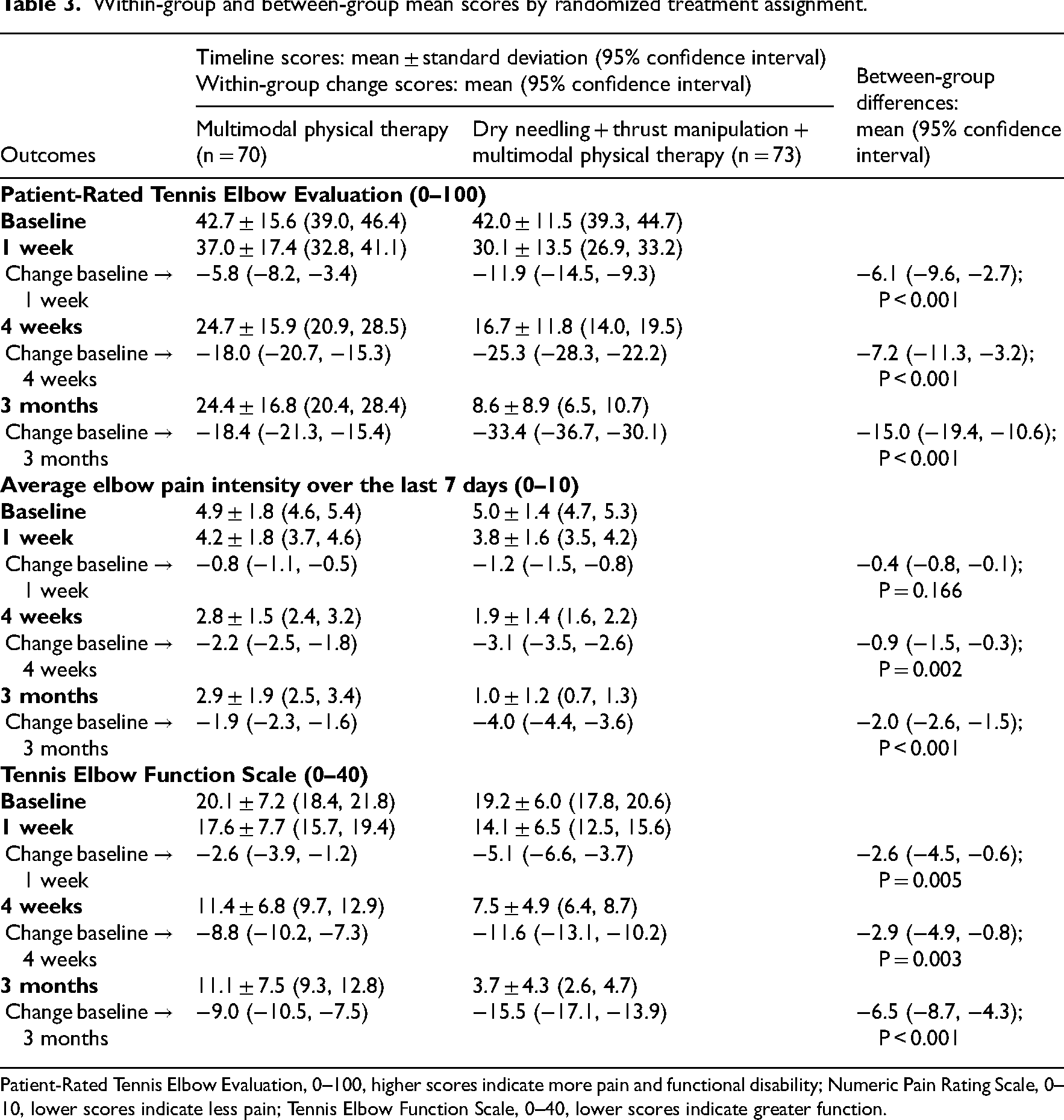
Patient-Rated Tennis Elbow Evaluation, 0–100, higher scores indicate more pain and functional disability; Numeric Pain Rating Scale, 0–10, lower scores indicate less pain; Tennis Elbow Function Scale, 0–40, lower scores indicate greater function.
Secondary Outcomes
The intention-to-treat analysis also revealed a significant group-by-time interaction for average elbow pain intensity over the last 7 days (Numeric Pain Rating Scale: F = 22.769; P < 0.001, Figure 4) in favor of the electrical dry needling and thrust manipulation group (Table 3). For average elbow pain intensity over the last 7 days (Numeric Pain Rating Scale), between-group effect sizes were small at 1 week (standardized mean difference: 0.23; 95% confidence interval: −0.10, 0.56), medium at 4 weeks (standardized mean difference: 0.54; 95% confidence interval: 0.21, 0.87), and large at 3 months (standardised mean difference: 1.19; 95% confidence interval: 0.84, 1.55) after the first treatment session in favor of the electrical dry needling and thrust manipulation group.
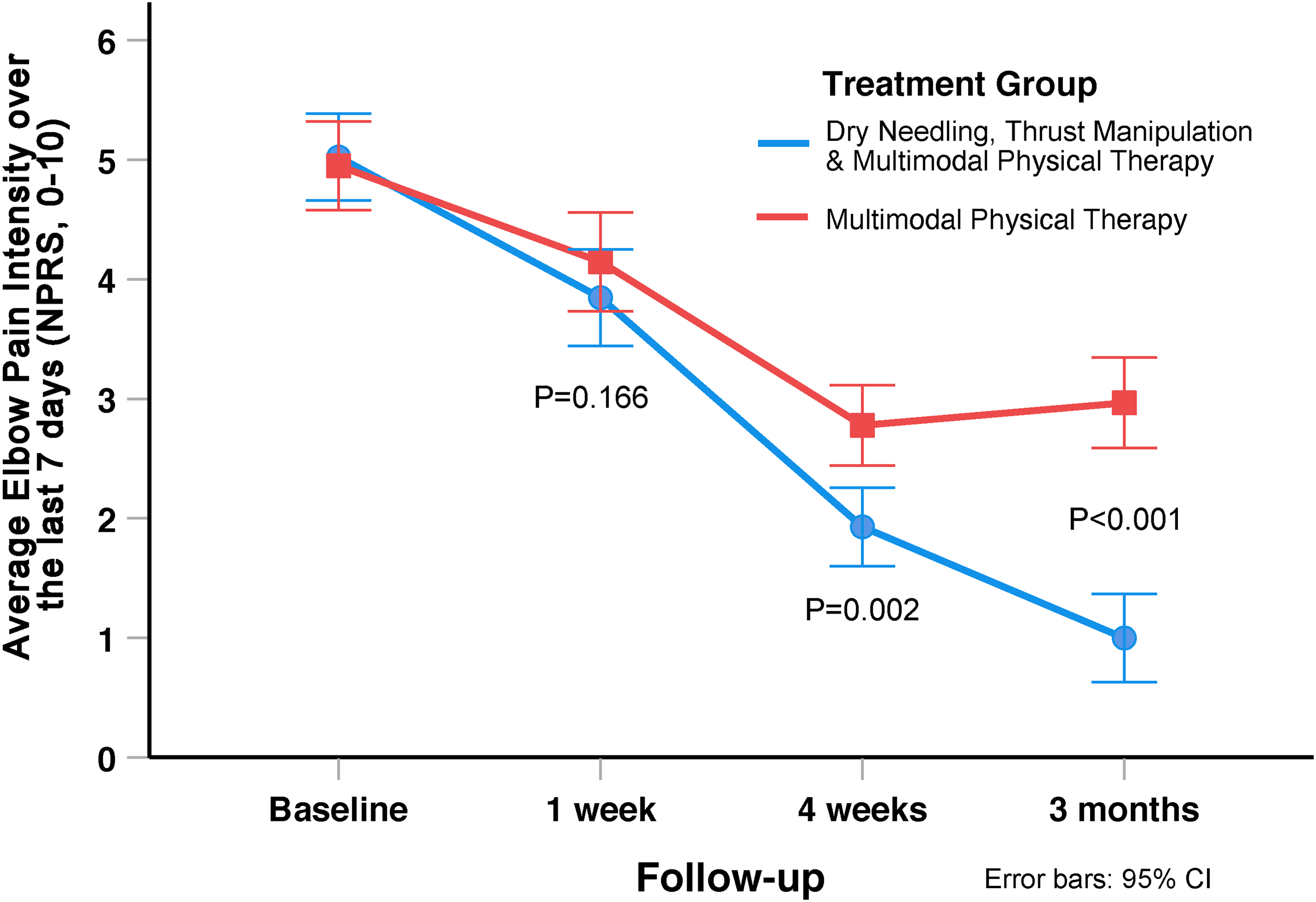
Evolution of elbow pain intensity (Numeric Pain Rating Scale) throughout the course of the study, stratified by randomized treatment assignment. Values are mean and standard error.
There was a significant group-by-time interaction for elbow function (Tennis Elbow Function Scale: F = 13.269; P < 0.001, Figure 5) in favor of the electrical dry needling and thrust manipulation group (Table 3). Between-group effect sizes for elbow function (Tennis Elbow Function Scale) were small at 1 week (standardised mean difference: 0.43; 95% confidence interval: 0.10, 0.76), medium at 4 weeks (standardised mean difference: 0.47; 95% confidence interval: 0.13, 0.79), and large at 3 months (standardised mean difference: 0.98; 95% confidence interval: 0.63, 1.33) after the first treatment session in favor of the electrical dry needling and thrust manipulation group.
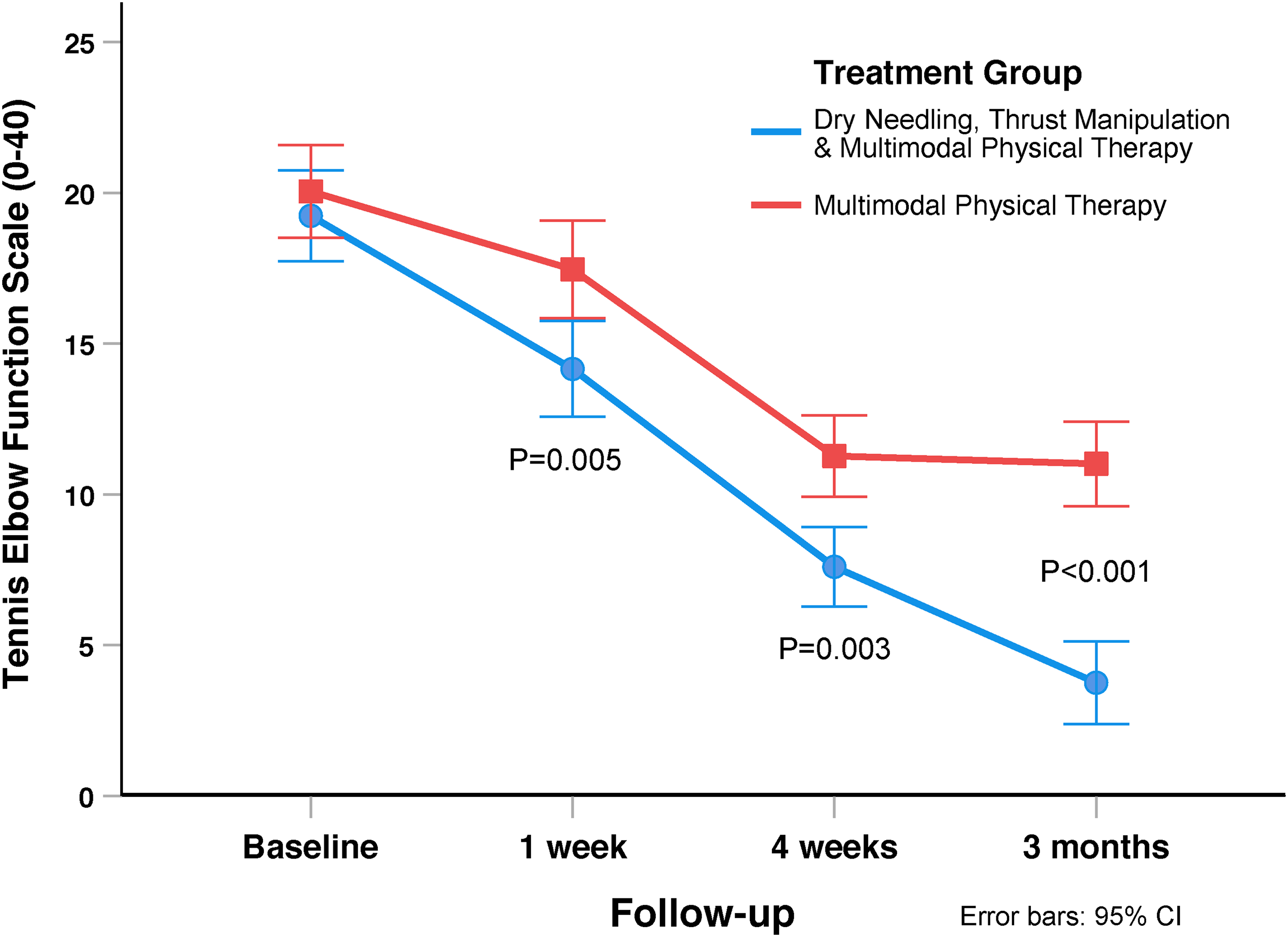
Evolution of elbow function (Tennis Elbow Function Scale) throughout the course of the study, stratified by randomized treatment assignment. Values are mean and standard error.
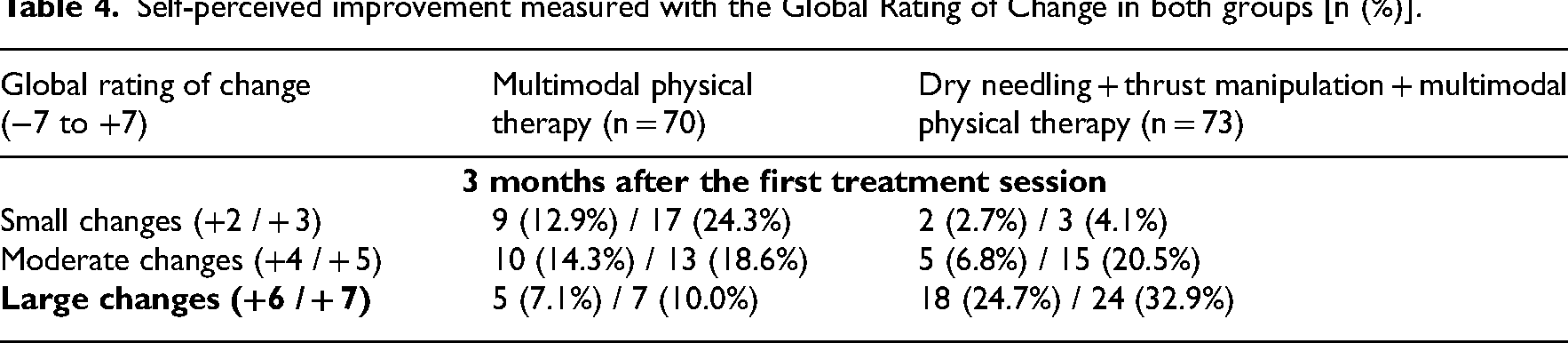
Significantly (X2 = 16.791; P < 0.001) more patients in the thrust manipulation and electrical dry needling group (n = 53, 72.6%) completely stopped taking medication for their pain compared to the multimodal physical therapy group (n = 27, 38.6%) at 3 months. In addition, based on the cutoff score of ≥+5 on the Global Rating of Change, 58 significantly (X2 = 26.223; P < 0.001) more patients (n = 57, 78%) within the electrical dry needling and thrust manipulation group achieved a successful outcome compared to the multimodal physical therapy group (n = 25, 36%) at 3 months follow up (Table 4). Therefore, based on the cutoff score of ≥+5 on the Global Rating of Change, the Number Needed to Treat was 2.4 (95% confidence interval: 1.8, 3.6) in favor of the dry needling and thrust manipulation group at 3-month follow up. Likewise, based on a 50% improvement from baseline to 3 months in pain and disability on the Patient-Rated Tennis Elbow Evaluation, the Number Needed to Treat was 1.9 (95% confidence interval: 1.5, 2.5) in favor of the dry needling and thrust manipulation group at 3-month follow up.
Self-perceived improvement measured with the Global Rating of Change in both groups [n (%)].
Discussion
The inclusion of dry needling and thrust manipulation into a program of exercise, mobilization, and ultrasound was more effective for improving pain, disability, and function than the application of exercise, mobilization, and ultrasound alone in individuals with lateral elbow tendinopathy. For the primary outcome of elbow pain and disability (Patient-Rated Tennis Elbow Evaluation), effect sizes were moderate and large at 4 weeks and 3 months, respectively, in favor of the electrical dry needling and thrust manipulation group. The between-group difference for change in elbow pain and disability at 3 months, as measured by the Patient-Rated Tennis Elbow Evaluation, was also large (−15.0 points; 95% confidence interval: −19.4, −10.6) and exceeded the minimum clinically important difference for that instrument (11 points). 62
The current study has similar outcomes to previous trials that have utilized dry needling in comparison with other nonsurgical interventions in patients with lateral elbow tendinopathy. Uygur et al. 20 reported dry needling to the lateral epicondyle (targeting the bone) was significantly more effective at improving pain and function than nonsteroidal anti-inflammatory drugs and proximal forearm bracing. Notably, two randomized clinical trials that directly compared dry needling (multiple needles to bone depth) to corticosteroid injections (single injection with 21 and without 19 periosteal pecking) found significantly greater improvements in pain and function in the dry needling group at the short-term19,21 and long-term 21 follow up. In addition, direct comparison of dry needling (single needle with periosteal pecking) to corticosteroid injection (single injection) and platelet-rich plasma (single injection), demonstrated that dry needling was safe and equally effective in pain reduction as corticosteroid injection and platelet-rich plasma at the 3-week and 3-month follow up. 23 Although the aforementioned clinical trials and systematic reviews74,75 appear to support the use of dry needling in the management of lateral elbow tendinopathy, a recent guideline 76 from the British Elbow and Shoulder Society does not recommend dry needling. More specifically, the analysis of patient-focused outcomes in 8 identified randomized clinical trials “demonstrated a large positive effect size (SMD) for improvement in pain and function from dry needling over the short (weeks) and medium term (6 months)” 76 ; however, Singh and Watts concluded that “there is no evidence of benefit compared to placebo” due to the differential application of the dry needling techniques and the significant heterogeneity in the outcome measure choice, outcome interval, and comparator groups. 76
There are several prior clinical trials that support the use of the manual therapy and exercise interventions used in the current study. Soft tissue mobilization,2,77,78 joint mobilization,2,79 and exercise2,80,81 have been found to improve clinical outcomes in patients with lateral elbow tendinopathy, either individually, or as a part of a multimodal treatment program. Notably, in patients with lateral elbow tendinopathy, local thrust manipulation targeting the radial head (Mill's manipulation)82,83 has been found to improve pain and function in the short term.2,77,79 Additionally, regional thrust manipulation and/or mobilization of the scaphoid84,85 and cervical spine18,86,87 have been reported to improve pain, function, and grip strength in patients with lateral elbow tendinopathy.2,79
The dry needling protocol of the current trial utilized bilateral and/or unilateral rotation manipulation88,89 of multiple needles 90 left in situ, combined with electrical stimulation53,91–93 to intramuscular, musculotendinous, teno-osseous, periosteal, and peri-articular tissues of the elbow complex.16,45,94,95 Although the terminology, theoretical constructs, and philosophies of “dry needling” and “acupuncture” differ, they are often considered to be in the same category of intervention,96–99 as both use thin monofilament needles without injectate to treat neuromusculoskeletal conditions.43,45,98,99 We chose to include “electrical dry needling” as part of the experimental group, as opposed to “dry needling” alone, because there may be superior analgesia obtained when treating pain with electroacupuncture compared to manual acupuncture alone.53,91,92,100 Neurophysiological mechanisms that may explain the superior analgesic effects of electroacupuncture include greater activation of the anterior middle cingulate cortex, 52 blocking the local release of inflammatory cytokines in the synovia of joints, 101 and blocking the systemic release of inflammatory factors in the periaqueductal gray of the brain stem. 102
The addition of cervical spine thrust manipulation has been used in prior trials on patients with subacromial pain syndrome16,103,104 and lateral elbow tendinopathy.17,18 Thrust manipulation to the cervical spine seems to produce an analgesic effect on the lateral elbow, resulting in increased pressure pain thresholds,17,18,105 an excitatory effect in resting electromyographic activity of segmentally associated muscles of the upper limb, 106 and an increase in pain-free grip strength in patients with lateral elbow tendinopathy.17,18 Plausible neurophysiological mechanisms may include stimulation of larger-diameter low-threshold mechanoreceptors at the spinal cord,107–109 a decrease in joint afferent activity, 110 and production of an adequate stimulus to activate descending inhibitory pain systems.111–113
There are important limitations to our trial. First, we only assessed short-term follow up (i.e. 3 months). Second, we did not use a placebo-needling or control group; however, trials measure relative efficacy of a treatment compared to a control, placebo, or usual care.
114
Third, there is a risk of treatment bias secondary to all treating therapists being associated with the same postgraduate fellowship program in orthopedic manual physical therapy.
The inclusion dry needling and thrust manipulation into a multimodal program of exercise, mobilization, and ultrasound were more effective for improving pain, disability, and function than the application of exercise, mobilization, and ultrasound alone in individuals with lateral elbow tendinopathy.Clinical messages
Supplemental Material
sj-docx-1-cre-10.1177_02692155241249968 - Supplemental material for Percutaneous tendon dry needling and thrust manipulation as an adjunct to multimodal physical therapy in patients with lateral elbow tendinopathy: A multicenter randomized clinical trial
Supplemental material, sj-docx-1-cre-10.1177_02692155241249968 for Percutaneous tendon dry needling and thrust manipulation as an adjunct to multimodal physical therapy in patients with lateral elbow tendinopathy: A multicenter randomized clinical trial by James Dunning, Firas Mourad, Paul Bliton, Casey Charlebois, Patrick Gorby, Noah Zacharko, Brus Layson, Filippo Maselli, Ian Young and César Fernández-de-las-Peñas in Clinical Rehabilitation
Supplemental Material
sj-doc-2-cre-10.1177_02692155241249968 - Supplemental material for Percutaneous tendon dry needling and thrust manipulation as an adjunct to multimodal physical therapy in patients with lateral elbow tendinopathy: A multicenter randomized clinical trial
Supplemental material, sj-doc-2-cre-10.1177_02692155241249968 for Percutaneous tendon dry needling and thrust manipulation as an adjunct to multimodal physical therapy in patients with lateral elbow tendinopathy: A multicenter randomized clinical trial by James Dunning, Firas Mourad, Paul Bliton, Casey Charlebois, Patrick Gorby, Noah Zacharko, Brus Layson, Filippo Maselli, Ian Young and César Fernández-de-las-Peñas in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors thank all the participants of the study.
Author Contributions
JD, FMo, and CF participated in the conception, design, data acquisition, statistical analyses, data interpretation, drafting, and revision of the manuscript. PB, IY, BL, and PG were involved in data acquisition, data interpretation, drafting, and revision of the manuscript. NZ, CC, and FMa were involved in data interpretation and revision of the manuscript. All authors read and approved the final version of the manuscript.
Declaration of Conflicting Interests
J.D. is the Director of the American Academy of Manipulative Therapy Fellowship in Orthopaedic Manual Physical Therapy. The American Academy of Manipulative Therapy provides postgraduate training programs in musculoskeletal sonography, vestibular rehabilitation, spinal manipulation, spinal mobilization, dry needling, extremity manipulation, extremity mobilization, instrument-assisted soft-tissue mobilization, therapeutic exercise, and differential diagnosis to licensed physical therapists, dentists, osteopaths, and medical doctors. J.D., I.Y., P.B., P.G., and N.Z. are senior faculty of the American Academy of Manipulative Therapy Fellowship. None of the authors were directly involved with subject recruitment, treatment sessions, or data collection. None of the treating therapists were reimbursed in any way for subject recruitment, treatment sessions, or data collection. The other authors declare that they have no competing interests.
Funding
None of the authors received any funding for this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.