
Abstract
Objective
To investigate cardiac rehabilitation utilisation and effectiveness, factors, needs and barriers associated with non-completion.
Design
We used the mixed-methods design with concurrent triangulation of a retrospective cohort and a qualitative study.
Setting
Economically disadvantaged areas in rural Australia.
Participants
Patients (≥18 years) referred to cardiac rehabilitation through a central referral system and living in rural areas of low socioeconomic status.
Main measures
A Cox survival model balanced by inverse probability weighting was used to assess the association between cardiac rehabilitation utilization and 12-month mortality/cardiovascular readmissions. Associations with non-completion were tested by logistic regression. Barriers and needs to cardiac rehabilitation completion were investigated through a thematic analysis of semi-structured interviews and focus groups (n = 28).
Results
Among 16,159 eligible separations, 44.3% were referred, and 11.2% completed cardiac rehabilitation. Completing programme (HR 0.65; 95%CI 0.57–0.74; p < 0.001) led to a lower risk of cardiovascular readmission/death. Living alone (OR 1.38; 95%CI 1.00–1.89; p = 0.048), having diabetes (OR 1.48; 95%CI 1.02–2.13; p = 0.037), or having depression (OR 1.54; 95%CI 1.14–2.08; p = 0.005), were associated with a higher risk of non-completion whereas enrolment in a telehealth programme was associated with a lower risk of non-completion (OR 0.26; 95%CI 0.18–0.38; p < 0.001). Themes related to logistic issues, social support, transition of care challenges, lack of care integration, and of person-centeredness emerged as barriers to completion.
Conclusions
Cardiac rehabilitation completion was low but effective in reducing mortality/cardiovascular readmissions. Understanding and addressing barriers and needs through mixed methods can help tailor cardiac rehabilitation programmes to vulnerable populations and improve completion and outcomes.
Keywords
Introduction
Low socioeconomic status is associated with poor cardiovascular outcomes. 1 Compared to high socioeconomic areas, the cardiovascular death rate in low socioeconomic areas is 1.3 times higher for males and 1.5 times higher for females. 2 Economic stability, neighbourhood-built environment, education and health care access, social and community relationships can be sources of chronic psychosocial stress. These stressors can activate biological responses that lead to autonomic dysfunction and chronic inflammation. 3 All these processes contribute to an increased cardiovascular risk and explain why psychosocial risk factors (e.g. low socioeconomic status, low social support, depression, anxiety) tend to cluster together and co-occur with traditional risk factors (e.g. smoking, obesity, diabetes), ultimately resulting in increased cardiovascular events and mortality. 3
These social determinants of health can be more prominent in rural areas, where 28% of the Australian population live, than in metropolitan areas. 4 Socioeconomic status is typically lower in rural and remote areas relative to metropolitan areas. This, in combination with worse health services access in rural areas, may contribute to poorer cardiovascular outcomes reported for these areas. In Australia, people living in remote areas have a 1.4 times higher age-adjusted hospitalisation rate than those living in major cities. 2 For coronary heart disease, the leading cause of death, age-adjusted death rates are 1.3 times higher in remote areas than in Australia overall. 2
Cardiac rehabilitation is a structured, multidisciplinary programme that includes exercise training and physical activity counselling, education, risk factor modification, diet counselling, and vocational and psychosocial support. 5 Cardiac rehabilitation can improve functional capacity and the control of traditional cardiovascular risk factors which account for much of the association between low socioeconomic status and cardiovascular mortality. 6 Cardiac rehabilitation is guideline-recommended6,7 and effective in reducing mortality and hospital readmission at 12 months post-discharge.8,9 However, globally, only 30–50% of eligible patients are referred, around 30% of the referred attend at least one session, and 10–30% complete the programme. 10
Patients living in low-income areas are less likely to attend or complete cardiac rehabilitation after hospitalisation for a heart attack and to be informed about cardiac rehabilitation while in hospital.11,12 We aimed to evaluate cardiac rehabilitation utilisation and effectiveness on clinical outcomes (readmissions and overall deaths) of patients with low socioeconomic status living in rural South Australia. Additionally, we sought to understand barriers to cardiac rehabilitation completion and the needs of patients with low socioeconomic status residing in rural areas.
Methods
Study design
This mixed-methods study had a concurrent triangulation and convergent parallel design. 13 The quantitative analysis used a retrospective cohort design, including patients admitted for a cardiovascular event from 01 January 2016 to 30 June 2021 in rural South Australia. The qualitative study involved four semi-structured interviews and five focus groups with participants from low socioeconomic status areas in rural South Australia. Factors associated with non-completion and reasons for non-completion retrieved from the quantitative study were compared and related to the themes and sub-themes derived from the thematic analysis of the qualitative study 13 (Figure 1).
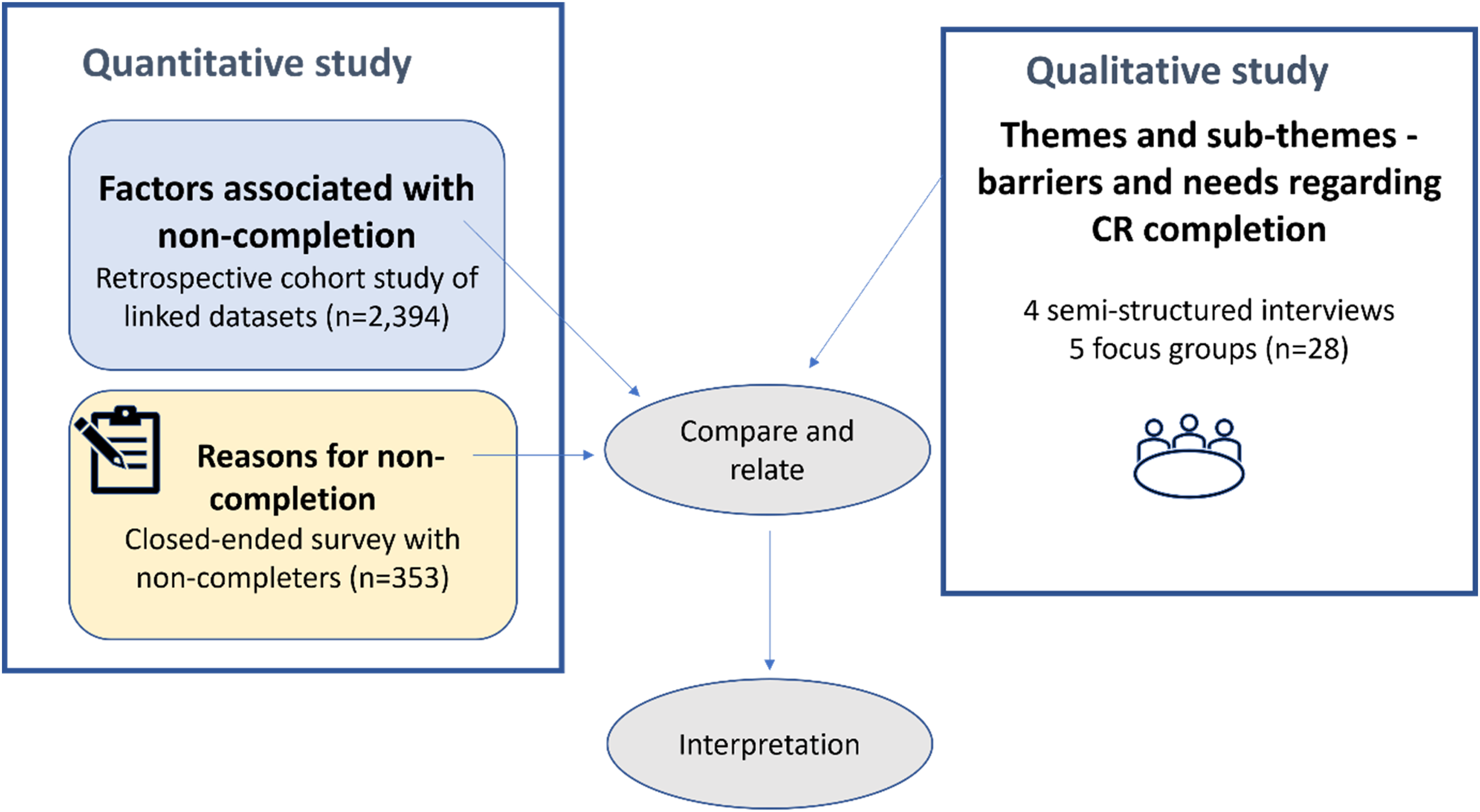
Mixed-methods study diagram.
Definitions
Low socioeconomic status was defined as an Index of Relative Socioeconomic Advantage and Disadvantage score within the two lowest deciles. The Index of Relative Socioeconomic Advantage and Disadvantage measures high and low income, degree of house mortgage, size of home, educational level, qualifications or none, employed as a professional, a manager, low skilled worker, machinery operator or laborer, high rent, number of cars or none, overcrowding, divorced, low rent, disability, unemployed, single parent family, no internet access and jobless parents from the Australian Census. 14
Rural areas were defined as those outside metropolitan areas according to the Modified Monash Model which also considers distance to services to classify as rural (also named regional in Australia) according to its remoteness (inner regional, outer regional, remote, and very remote areas). 4
Setting
All South Australian public hospitals and the 15 public cardiac rehabilitation programmes in rural areas, including the one delivered exclusively via telephone, were involved. All cardiac rehabilitation programmes receive referrals from metropolitan and regional hospitals via a central referral system. All programmes comprised the following core components: referral and access to services, clinical assessment and short-term monitoring, recovery and long-term maintenance, lifestyle/behavioral modification and medication adherence, and evaluation and quality improvement. 15
Quantitative study
Participants
Eligible patients were adults (≥18 years); living in rural areas of South Australia with a low socioeconomic status; discharged alive from a hospital separation with a primary or secondary cardiac-related diagnostic code, with or without an interventional procedure, including acute coronary syndrome, heart failure, atrial fibrillation, acute myocardial infarction, percutaneous coronary intervention, coronary artery bypass graft, aortic or mitral valve replacements, automatic implantable cardioverter-defibrillator or permanent pacemaker.
A hospital separation was defined as from the beginning of admission to discharge. Separations across multiple hospitals, transfers, and readmissions within 24 hours were merged into one event. All the separations eligible to cardiac rehabilitation from the South Australian Department of Health Admitted Patient Care database between January 2016 and June 2021 (5.5 years) were included.
Variables/outcomes
The primary outcome was cardiac rehabilitation utilisation measured across three categories: did not receive cardiac rehabilitation (not referred or declined), commenced but did not complete cardiac rehabilitation, and completed cardiac rehabilitation. Referrals were defined by a health professional assessment and recorded in the South Australian cardiac rehabilitation programme database. Commencement (≥1 session) and completion as defined by a clinician were also characterised by a health professional involved in the patient care.
Secondary outcomes included a composite endpoint of all-cause mortality or admission for new/re-myocardial infarction, heart failure, atrial fibrillation, or stroke within 12 months of the index admission.
Data sources/measurements and linkage process.
The public hospital's database (South Australian Admitted Patient Care), the Emergency Department Data Collection, the South Australian Births, Death and Marriages, and the South Australian cardiac rehabilitation datasets were linked through deterministic linkages based on 11 identifying variables (client identification number, last name, first name, other names, date of birth, sex, date of death, weight at birth, street address, suburb, and postcode). Records not linked deterministically were analysed by probabilistic linkage and subsequently underwent clerical review if still unmatched.
The South Australian Cardiac Rehabilitation database (Country Access to Cardiac Health - CATCH database) captured dates of referrals, commencements, and completions; pre, post, 6- and 12-month cardiovascular risk factors, depression screening through Patient Health Questionnaire (PHQ)-2 and PHQ-9 16 ; self-reported smoking and medication adherence; and exercise capacity. Additionally, it captures close-ended questions with a list of possible reasons for non-completion prompted by the clinicians to patients commencing but not completing cardiac rehabilitation.
Statistical methods
We used an inverse probability weighting model adjusted for age, gender, primary diagnosis, Charlson Comorbidity Index, 17 prior heart failure, coronary disease, atrial fibrillation, revascularisation, malignancy, and socioeconomic disadvantage measured by the Index of Relative Socioeconomic Advantage and Disadvantage 14 to account for the selection bias and unequal probabilities of cardiac rehabilitation completion. The balance of the inverse probability weighting model was tested by comparing the standardised difference (<10%) of the probabilities between the group that did not receive cardiac rehabilitation (was not referred or declined cardiac rehabilitation) versus those who commenced but did not complete and those who completed cardiac rehabilitation (Supplementary Table 1). As a prior diagnosis of dementia was not balanced across the groups in the weighted model (i.e. standardised difference ≥10%), we excluded patients with dementia (n = 135).
We compared patients’ demographics, clinical, and social characteristics across the cardiac rehabilitation utilisation categories through Kruskal–Wallis (for continuous variables described by median and interquartile range) and Chi-square tests (for categorical variables defined by proportions). The Shapiro–Wilk test was used to test the normality distribution of the data. Cardiac rehabilitation utilisation was reported as ratios, measured as proportions (%).
To assess the association of the secondary outcome (composite of cardiovascular readmission due to myocardial infarction, heart failure, atrial fibrillation, or stroke and all-cause mortality) and cardiac rehabilitation utilisation (three groups), we performed Cox proportional hazard models applied to the weighted population after testing for the proportional hazard assumption. The models were adjusted by age, gender, remoteness, primary cardiac diagnosis, referring hospital, and the Charlson Comorbidity Index. 17 A p value of <0.05 was statistically significant, and Stata 15.0 was used for the analysis. 18
For the sub-cohort of separations receiving cardiac rehabilitation, we investigated the association of non-completion (independent variable) with sociodemographic and clinical factors by adjusting binary logistic models for age, gender, remoteness (inner regional, outer regional, remote, and very remote), living alone, English as a second language, index separation characteristics pre or during the COVID-19 pandemic, the reason for referral (acute myocardial infarction, heart failure, atrial fibrillation, coronary artery bypass graft, percutaneous coronary intervention, valve procedures, implantable device procedures), Charlson Comorbidity Index, and history of comorbidities (diabetes, obesity, hypertension, depression), and the waiting time to commence cardiac rehabilitation from hospital separation.
Qualitative study
Qualitative data from 28 participants were collected through four semi-structured interviews and five focus groups, using the Experience Based Co-Design – A toolkit for Australia 19 as a framework to engage with the participants through accessible, tangible ways (e.g. visual communication, scenarios, and personas). This approach helps patients with low literacy levels convey ideas and design better service experiences. 19
Perceived barriers and needs from hospital discharge/referral to (non) attendance/completion of cardiac rehabilitation were explored through interviews and focus groups. The research questions and target groups in this phase were specific, and the sample size generated sufficient information for an in-depth analysis of the narratives. 20
The cardiac rehabilitation nurse recruited participants; the inclusion criteria were: being adults (≥18 years), referred to a cardiac rehabilitation programme in rural South Australia, and living in an area of low socioeconomic status. Cognitive impairment (Mini-mental short scale <20) was an exclusion criterion.
Interviews and focus group interviews’ audio recordings were transcribed verbatim by a professional transcription company. The de-identified transcripts were analysed using Braun and Clark inductive thematic analysis. 21 Familiarisation with the topic was established through individual organic and subjective coding by AB and HD. Nodes were established independently and then examined collaboratively by AB, HD, CH, and MAPP after identifying recurrent themes to confirm final themes. Verbatim quotes were extracted to illustrate themes and sub-themes.
Reporting bias was mitigated by involving researchers from different disciplines and backgrounds (medicine, nursing, health economics, and public health) in the analysis. Additionally, these researchers were not involved in data collection. To reduce selection bias, we offered options for out-of-hours participation, and in-person or virtual/phone attendance. Participants were reimbursed for travel and participation time.
Ethics
The quantitative study received approval from the South Australian Department for Health and Wellbeing Human Research Ethics Committee (2021/HRE00270) for the use of linked data. A waiver of consent was granted to the project by the Department for Health and Wellbeing Ethics Committee. The qualitative study was approved by the Southern Adelaide Clinical Human Research Ethics Committee (LNR/22/SAC/71).
Results
Quantitative study
There were 16,159 separations eligible to this analysis after exclusion of patients with dementia (Figure 2). Participants’ median age was 71 (IQR 60-79) years, and 40.9% (n = 6,610) were female; acute myocardial infarction (n = 1773; 11.0%) and percutaneous coronary intervention (n=806; 4.9%) were the most frequent index admission single diagnosis and procedure, respectively. A referral was received by 7,159/16,159 (44.3%). Among the 7,159 who received a referral, 2,394 (33.4%) commenced cardiac rehabilitation, and among those commencing, 1,806 (75.4%) completed the programme. When assessed among the eligible, the completion rate was 11.2%. Characteristics of patients across the cardiac rehabilitation utilisation groups are displayed in Table 1.
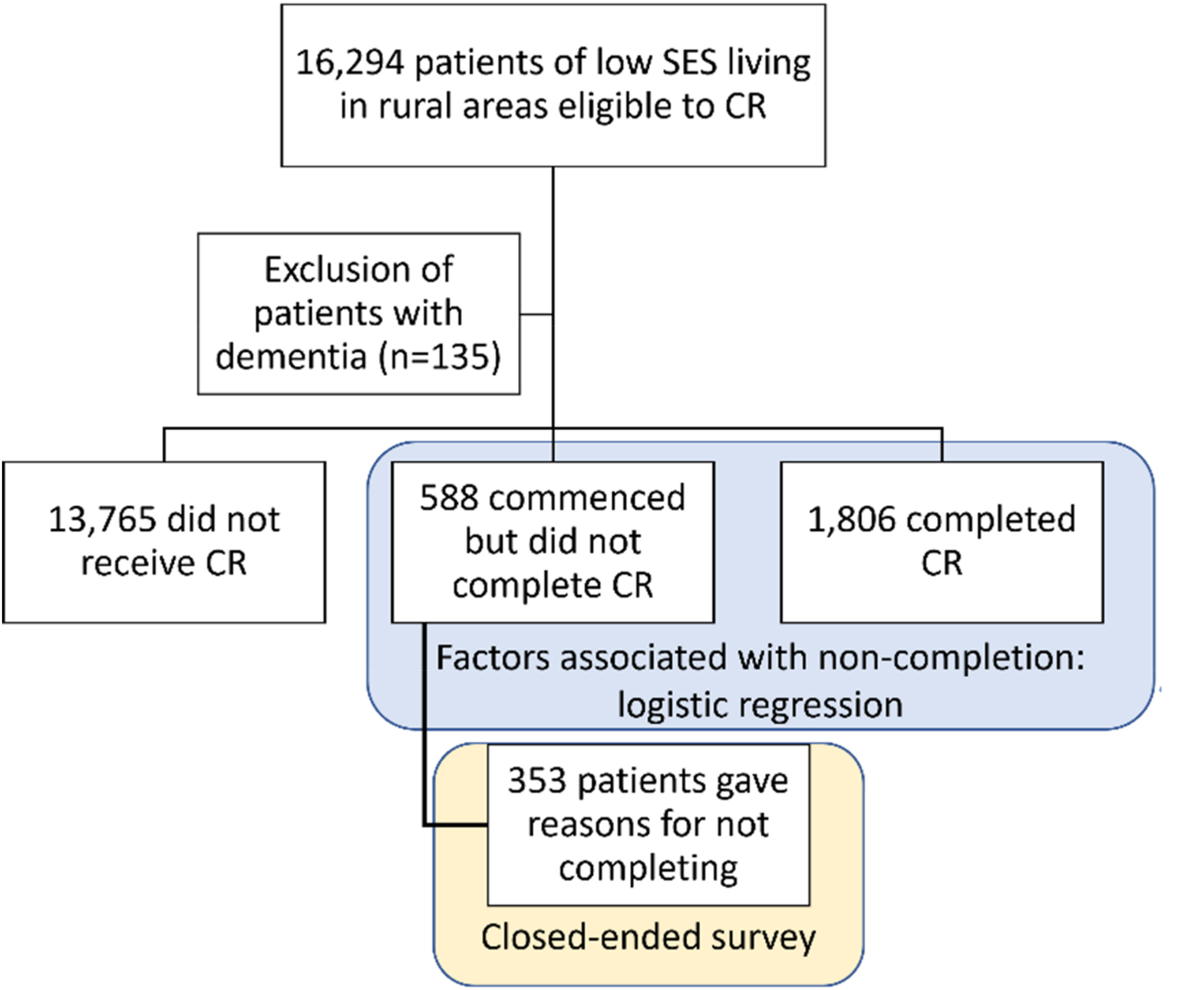
Quantitative study flow diagram.
Characteristics of the patients across groups of cardiac rehabilitation utilisation for the non-weighted population.
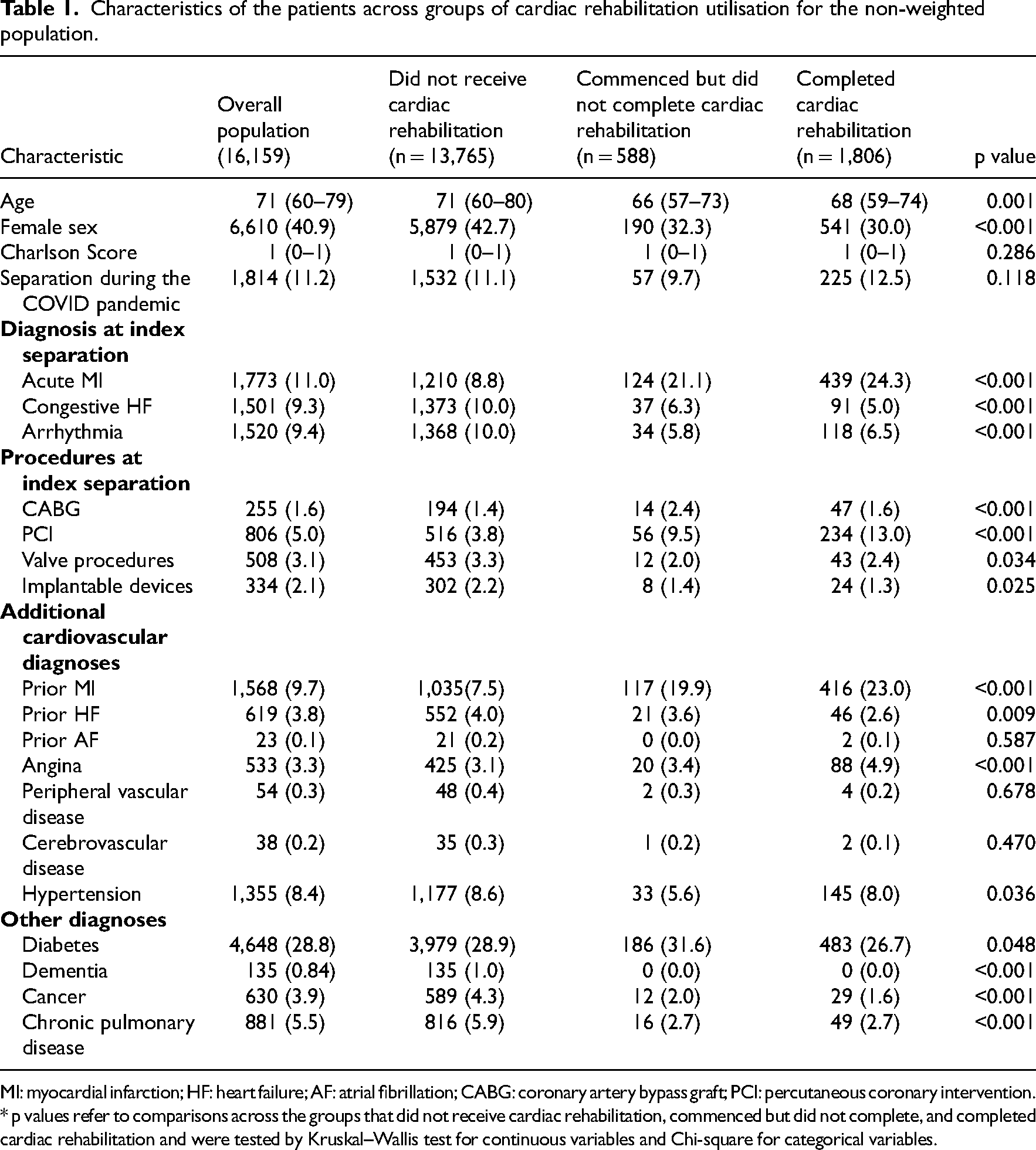
MI: myocardial infarction; HF: heart failure; AF: atrial fibrillation; CABG: coronary artery bypass graft; PCI: percutaneous coronary intervention. * p values refer to comparisons across the groups that did not receive cardiac rehabilitation, commenced but did not complete, and completed cardiac rehabilitation and were tested by Kruskal–Wallis test for continuous variables and Chi-square for categorical variables.
The median time from discharge to commencement of a cardiac rehabilitation programme was 31 (IQR 18–51) days, and the median duration of the cardiac rehabilitation programme was 42 (IQR 30–61) days.
Living alone (OR 1.38; 95% CI 1.00–1.89; p = 0.048), having diabetes (OR 1.48; 95% CI 1.02–2.13; p = 0.037) or depression at baseline (OR 1.54; 95% CI 1.14–2.08; p = 0.005), and being enrolled in the telephone programme compared to a face-to-face programme (OR 0.26; 95% CI 0.18–0.38; p < 0.001) were associated with non-completion of cardiac rehabilitation.
Patient-related (not interested, n = 109; feeling unwell, n = 104; did not like or see value in the programme, n = 9), service-related (preferring to follow-up with the general practitioner, n = 46; cardiac rehabilitation programme time unsuitable, n = 8); and work/social circumstances-related (return to work, n = 42; transport/distance, n = 34; cost, n = 1) were reported as reasons for non-completion by 353 patients.
There were 4,066 composite events of all-cause death or admission for new/re-myocardial infarction, heart failure, atrial fibrillation or stroke) within the 12 months of follow-up after hospital discharge. After adjustment for sociodemographic and clinical factors, completing cardiac rehabilitation (HR 0.65; 95% CI 0.57–0.74; p < 0.001) was associated with a lower risk of cardiovascular readmission/death. Commencing but not completing cardiac rehabilitation was not significantly associated with the composite outcome (HR 0.94; 95% CI 0.78–1.13; p = 0.478) – Figure 3.
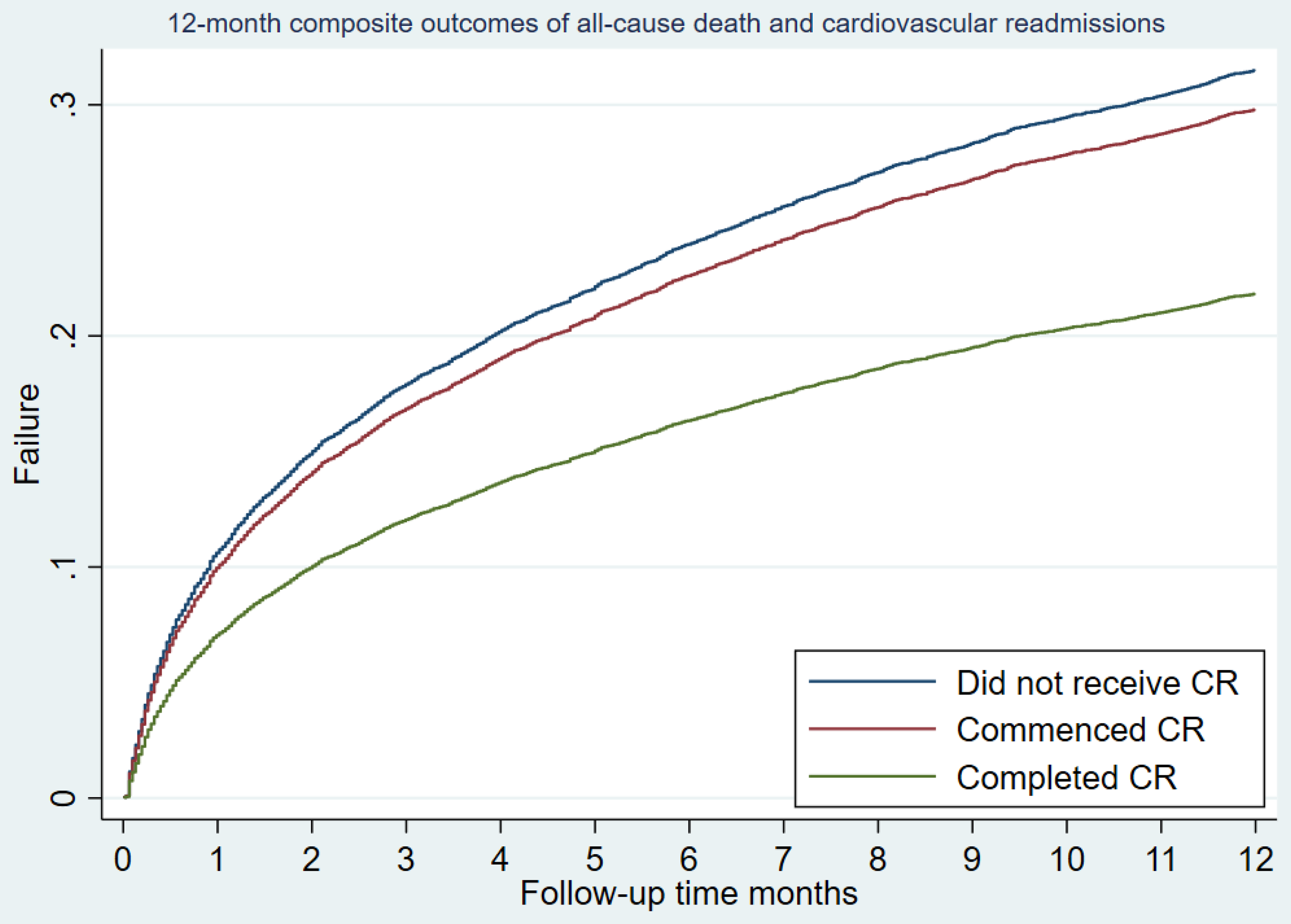
Adjusted all-cause mortality/cardiovascular readmission rates within 12 months after the index hospitalisation.
Qualitative study
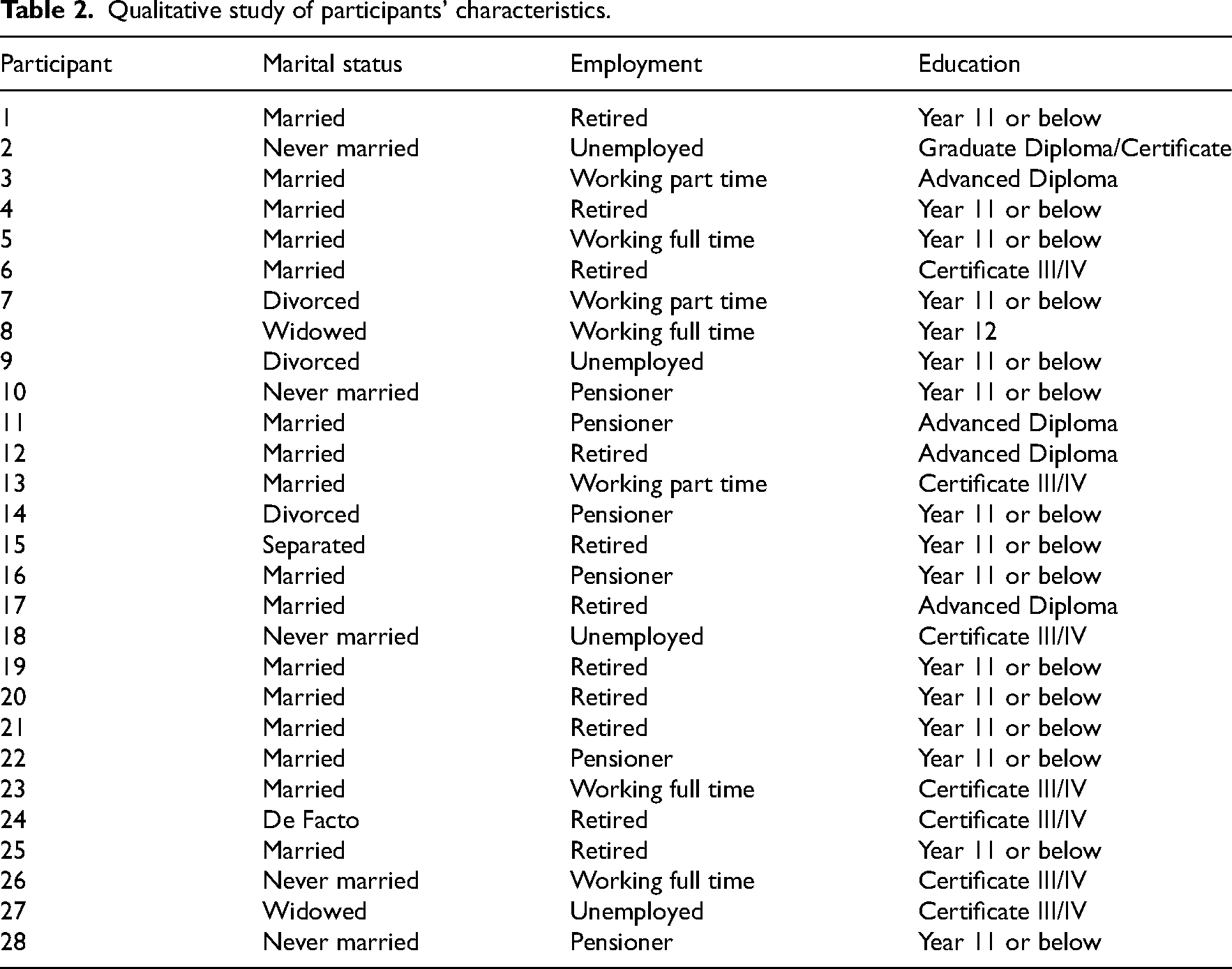
There were 28 participants in the qualitative study (24 participants from the five workshop focus group interviews and four patients’ individual interviews). Participants’ median age was 68 years (range 62–75), and six (21.4%) were women. All had English as a first language, and none were of Aboriginal and Torres Strait Islander heritage. Ten (35.7%) participants lived alone, and one participant reported having a carer. Two did not have access to the internet. Twelve (43%) were enrolled in a face-to-face programme and 16 (57%) in the telephone programme. Characteristics of the qualitative study participants are shown in Table 2.
Qualitative study of participants’ characteristics.
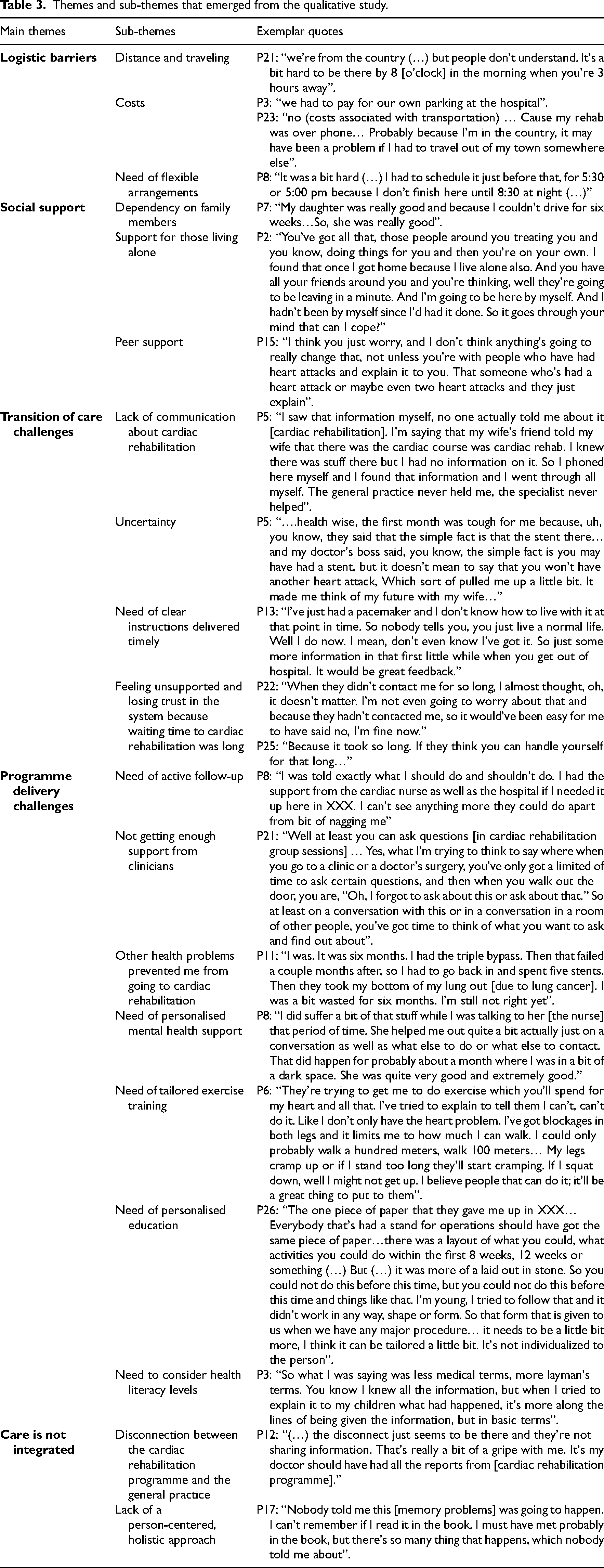
Five overarching themes (logistic barriers, social support, transition of care, programme delivery, and care integration) and 19 sub-themes emerged from this study (Table 3).
Themes and sub-themes that emerged from the qualitative study.
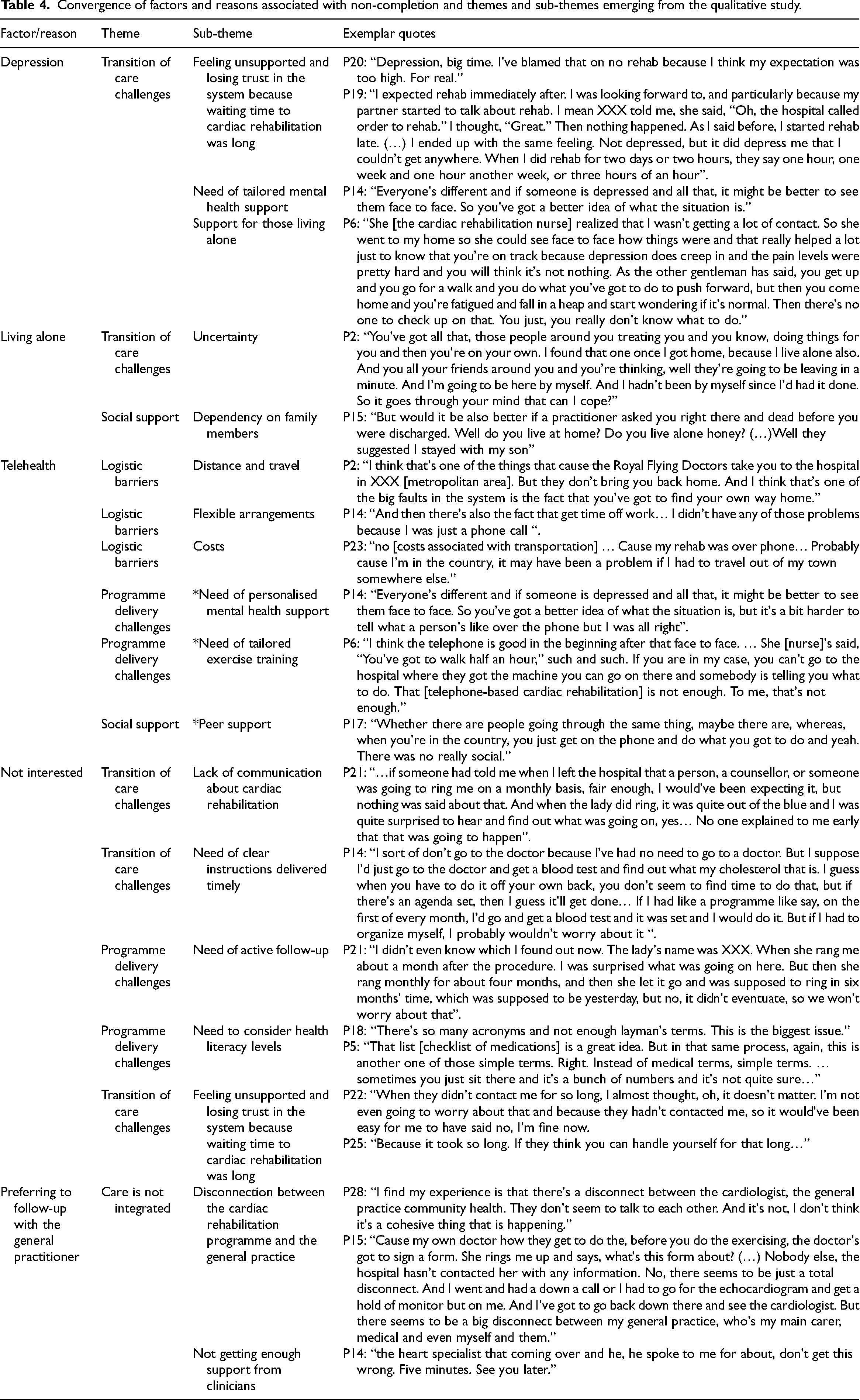
We found convergence between the factors and reasons found in the quantitative analysis and the barriers and needs that emerged in the qualitative study (Table 4). However, for telehealth that was associated with lower chance of non-completion (i.e., patients receiving telehealth were more likely to complete cardiac rehabiliation), we found some divergence between the themes. Whereas the theme “logistic barriers” converged with the findings of telehealth increasing cardiac rehabilitation participation; in the qualitative study the emerging sub-themes “need of personalized mental health support”, “need of tailored exercise training”, and “(lack) peer support” were reported as barriers associated with telehealth.
Convergence of factors and reasons associated with non-completion and themes and sub-themes emerging from the qualitative study.
Discussion
This study showed low utilisation rates of cardiac rehabilitation by people of low socioeconomic status living in rural Australia. On the other hand, completing the programme was associated with a 35% reduction in the risk of death or hospital admission; attending the programme without completing it was not associated with a risk reduction in this population living in rural low socioeconomic areas. The main reasons for non-completion were lack of interest, being unwell and preferring follow-up within primary care only. Living alone and having diabetes or depression increased the risk of non-completion, but being enrolled in a telehealth programme decreased the risk of not completing. There was convergence of the factors/reasons with the themes emerging from the qualitative study except for needs around telehealth-delivered cardiac rehabilitation.
Lemstra et al. (2013) showed lower cardiac rehabilitation attendance and completion rates (6.4% versus 14.8% in our study and 37.9% versus 75.4%, respectively) and higher waiting times (123 days versus 31 days) among people living in low-income neighbourhoods in Canada after hospitalisation for ischemic heart disease or revascularisation procedure. 11 Conversely, completion rates among those who started cardiac rehabilitation were higher in a Danish study than in ours (97.7% versus 75.4%, respectively). 22 Their model of care included an extra number of cardiac rehabilitation sessions, telephone follow-up, and involvement of general practices and patient associations in the maintenance phase for their socially vulnerable group.
Living alone was associated with a higher risk of not completing cardiac rehabilitation by our quantitative study and reported as a barrier to cardiac rehabilitation participation in our qualitative study. Living alone was related to feelings of being unsupported which coincides with findings that it is a proxy of low social support and worse clinical outcomes. 23
Long waiting times were reported as a contributing factor to feeling depressed, and being unsupported leads to a decreased interest in cardiac rehabilitation. Likewise, lack of or unclear communication about cardiac rehabilitation during the hospital stay and transition of care period were referred as sources of low interest in cardiac rehabilitation which relates to the evidence that physician endorsement 24 and enrolment by a nurse or allied health professional increase cardiac rehabilitation participation. 10
Another factor that could be leading to disinterest in cardiac rehabilitation is clinician communication occurring at a health literacy level that was not appropriate as reported in our qualitative study. As health literacy may influence both patient satisfaction and self-management of risk factors, 25 programmes should consider evaluating health literacy and addressing the patient's needs. This may involve helping patients with (i) finding and (ii) appraising health information, (iii) navigating the health care system, and (iv) engaging with health care providers. 26
The perception that the general practitioner was not involved with cardiac rehabilitation may reduce the programme value to patients leading to low participation. Ensuring that intake and discharge transition records are shared with the primary care provider can improve integration of care. However, <50% of the general practices receive an intake transition record from the cardiac rehabilitation programme. 27
Cardiac rehabilitation delivered via telehealth was independently associated with cardiac rehabilitation completion, which can be explained by telehealth increasing access to care by minimising logistic barriers such as distance and travelling, costs and scheduling flexibility. 28 However, participants highlighted that mental health support, exercise training, and peer support were weaknesses of the telehealth program. Tailoring these components to the needs of special subgroups rather than a one-size fits all approach may help to improve the quality of telehealth delivery, increase completion and clinical and patient-reported outcomes. For example, programme tailoring to women's needs has been associated with gains in health-related quality of life during cardiac rehabilitation. 29 Moreover, offering alternative forms of exercise, such as yoga and Tai Chi Chuan, could facilitate personalisation and lead to improvements in cardiac rehabilitation adherence and participation particularly among women. 30
As limitations of our study, we acknowledge that its observational design limits generalisability and that, despite the use of the inverse probability weighting and extensive model adjustment, selection bias and residual confounding may still have occurred despite adjustment for clinical and sociodemographic factors. Additionally, it is likely that women, people with English as a second language and Aboriginal and Torres Strait Islander peoples were underrepresented in the qualitative study which may have impacted the emergence of the themes.
As a message to clinical practice, we would highlight that, as programme completion was key to reduce the risk of hospitalisation and death among people of low socioeconomic status living in rural areas, it would be advisable to concentrate on cardiac rehabilitation quality improvement initiatives around issues that may lead to improved completion. These may include: (i) identifying patients who live alone and providing them with social support; (ii) reducing waiting time; (iii) communicating the benefits of cardiac rehabilitation timely and at an appropriate health literacy level; (iv) integrating cardiac rehabilitation with primary care; (iv) offering telehealth as an option of cardiac rehabilitation delivery and designing telehealth models that enable tailored mental health support, exercise training, and peer support; (v) personalising mental health support and exercise programme.
In conclusion, our findings reinforce that completion of cardiac rehabilitation is paramount to the achievement of clinical benefits in patients with low socioeconomic status living in rural areas. However, completion remains low. Addressing barriers and needs related to logistics, social support particularly to those living alone, transition of care, care integration, and lack of person-centredness of the programmes especially through telehealth-enabled models of care may increase the interest and value of patients with socioeconomic disadvantaged leading to improved participation and clinical outcomes.
Programme completion reduces the risk of hospitalisation and death among people of low socioeconomic status living in rural areas. Focus cardiac rehabilitation initiatives on:
(ι) identifying and supporting patients living alone (ii) reducing waiting time (ιιι) offering telehealth as an option of programme delivery, personalising, and improving mental health support, exercise, and peer support.Clinical messages
Supplemental Material
sj-docx-1-cre-10.1177_02692155241236998 - Supplemental material for Clinical effectiveness of cardiac rehabilitation and barriers to completion in patients of low socioeconomic status in rural areas: A mixed-methods study
Supplemental material, sj-docx-1-cre-10.1177_02692155241236998 for Clinical effectiveness of cardiac rehabilitation and barriers to completion in patients of low socioeconomic status in rural areas: A mixed-methods study by Alline Beleigoli, Hila Ariela Dafny, Maria Alejandra Pinero de Plaza, Claire Hutchinson, Tania Marin, Joyce S. Ramos, Orathai Suebkinorn, Lemlem G. Gebremichael, Norma B. Bulamu, Wendy Keech, Marie Ludlow, Jeroen Hendriks, Vincent Versace and Robyn A. Clark in Clinical Rehabilitation
Footnotes
Acknowledgements
We acknowledge the contribution of the cardiac rehabilitation patients, South Australian public health cardiac rehabilitation service providers, and the Heads of Unit across the Department of Health Local Health Networks, and the SA/NT Datalink consortium for providing the data linkage and the Integrated Cardiovascular Clinical Network, Rural Support Service, South Australiaa especially Dr Philip Tideman (in memoriam) and Rosy Tirimacco.
Author Contributions
The study was conceived and designed by AB and RC. AB, MAPP, CH, RC, WK, ML, PT, and JH secured funds for the study. AB analysed the quantitative data. AB and HD analysed the qualitative data with input from MAPP and CH. JSR, OS, and TM collected the qualitative data. The first draft of the paper was written by AB with input from all co-authors. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by a Flinders Foundation Health Seeding Grant and by the Country Heart Attack Prevention (CHAP) project, a peer-reviewed National Health and Medical Research Council (NHMRC Partnership Grant GNT1169893). VV is funded by the Rural Health Multidisciplinary Training (RHMT) programme (Australian Government Department of Health and Aged Care).
Author's note
Robyn A. Clark, Department of Health, Southern Adelaide Local Health Network, South Australia, Australia.
Data Availability Statement
The data underlying this article cannot be shared publicly due to SA Health policy for data linkage privacy. The data will be shared on reasonable request to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.