
Abstract
Objective
There is a large gap between evidence-based recommendations for spatial neglect assessment and clinical practice in stroke rehabilitation. We aimed to describe factors that may contribute to this gap, clinician perceptions of an ideal assessment tool, and potential implementation strategies to change clinical practice in this area.
Design
Qualitative focus group investigation. Focus group questions were mapped to the Theoretical Domains Framework and asked participants to describe their experiences and perceptions of spatial neglect assessment.
Setting
Online stroke rehabilitation educational bootcamp.
Participants
A sample of 23 occupational therapists, three physiotherapists, and one orthoptist that attended the bootcamp.
Intervention
Prior to their focus group, participants watched an hour-long educational session about spatial neglect.
Main measures
A deductive analysis with the Theoretical Domains Framework was used to describe perceived determinants of clinical spatial neglect assessment. An inductive thematic analysis was used to describe perceptions of an ideal assessment tool and practice-change strategies in this area.
Results
Participants reported that their choice of spatial neglect assessment was influenced by a belief that it would positively impact the function of people with stroke. However, a lack of knowledge about spatial neglect assessment appeared to drive low clinical use of standardised functional assessments. Participants recommended open-source online education involving a multidisciplinary team, with live-skill practice for the implementation of spatial neglect assessment tools.
Conclusions
Our results suggest that clinicians prefer functional assessments of spatial neglect, but multiple factors such as knowledge, training, and policy change are required to enable their translation to clinical practice.
Keywords
Introduction
People with spatial neglect typically have impaired attention to stimuli on the side of space opposite to their acquired brain injury and have an impaired experience of the world and a worse rehabilitation prognosis.1,2 People with spatial neglect fall frequently, 3 are unlikely to achieve independent mobility 4 and are more likely to be discharged into institutional care. 5 It is therefore important that clinicians accurately assess spatial neglect to appropriately manage the condition.
Clinicians that aim to assess spatial neglect using evidence-based practice encounter multiple challenges. First, while many stroke guidelines recommend that spatial neglect should be assessed, they commonly do not recommend a specific, best-practice assessment tool (e.g. the Australian Stroke Guidelines recommend that for any person suspected of having spatial neglect, ’a full assessment using validated tools’ should be performed).6,7 Second, the language used to describe spatial neglect in the literature is complex; over 105 different terms are used, and terms such as ‘neglect’, ‘inattention’, and ‘extinction’ are often used interchangeably. 8 Finally, there are almost 300 published assessments of spatial neglect, most of which are specific to one or two ‘sub-types’ of the condition, for example, visual spatial neglect. 8
Given the time constraints of clinical practice and the complexity of assessment choice, a viable strategy is to systematically assess how spatial neglect impacts the activities of daily living of a person with stroke. However, in practice, clinicians typically use informal and non-standardised observations to describe how spatial neglect impacts activities of daily living.9,10 The factors driving these behaviours are currently unclear and could include lack of knowledge, confusing terminology, many assessment choices, lack of specific guidelines, or other unknown influences. The primary aim of this study was to use the Theoretical Domains Framework to describe the factors that influence assessment of spatial neglect in clinical stroke rehabilitation. We also aimed to describe clinicians’ perceptions of an ideal assessment of spatial neglect, and the ideal strategies for its implementation.
Methods
This study was a qualitative investigation that used focus groups with clinician participants to describe their experience of clinical assessment of spatial neglect. Data were collected during a multidisciplinary week-long virtual stroke rehabilitation educational bootcamp in Ulster, Northern Ireland. The bootcamp was open to participants from any country and had six sessions per day, which consisted of seminars and workshops that covered allied health management of stroke rehabilitation. Focus groups were chosen as the method of data collection to provide clinicians with the opportunity to reflect on their experiences as a group, in a way that mimicked the social, team-based context of multidisciplinary clinical stroke rehabilitation. 11 Previous research has reported that many clinicians may not be aware of the complexity of spatial neglect, or the available assessment options.9,12,13 Consequently, prior to their participation in a focus group, participants were provided with an hour-long educational session about spatial neglect. The session aimed to align participants’ knowledge about spatial neglect and the assessment tools that are available and was designed to prompt clinicians to reflect on their clinical practice and potential barriers and facilitators to implementation.
Study participants were a convenience sample of allied health professionals that attended the educational bootcamp and were working in stroke rehabilitation. In the welcome session of each day of the bootcamp, all clinician attendees were invited to participate in the study and were provided with an online link to the study information. To be eligible to participate, clinicians needed to (a) be a registered allied health professional, (b) be employed in a rehabilitation setting that provided stroke rehabilitation services, (c) have at least 6 months previous experience in neurological rehabilitation, and (d) be able to provide written, informed consent to participate in the study. The study was approved by the University of Technology Human Research Ethics Committee (ETH 21-6132) and ratified by the Ulster University Research Governance (NT21-301121-05).
Study Procedure
After providing informed consent, participants selected one of eight focus group sessions to attend. Prior to the focus group, participants were provided with a link to an online, 1-hour long educational session about available standardised assessments of spatial neglect in stroke. Participants could watch the video at any time prior to their participation in the focus groups, however, were required to have watched the video before the start of their focus group.
The educational session was presented by a member of the research team (DK) in a pre-recorded video. The video provided an overview of the pathophysiology and clinical impact of spatial neglect, and then presented a total of 12 different standardised assessments, with different levels of evidence, to not bias participants towards a particular assessment tool. These assessments were selected from a recent review of spatial neglect assessment (see Supplemental material 1). 10
The online focus groups were held for approximately 1 hour each using the Zoom platform 14 and were video and audio recorded. The maximum possible focus group size was six participants to ensure that all participants would have a chance to express their ideas. Focus group questions were developed a priori by the research team. The first set of questions (1–9) was based on the 14 domains of the Theoretical Domains Framework 15 : Knowledge, Skills, Social/professional role and identity, Beliefs about capabilities, Optimism, Beliefs about consequences, Reinforcement, Intentions, Goals, Memory, attention and decision processes, Environmental context and resources, Social influences, Emotion, and Behavioural regulation. An explanation of these domains is detailed in Supplemental Material 2. The second set of questions (10–13) was general and asked participants to describe a hypothetical ideal assessment of spatial neglect and strategies for its implementation. These questions were piloted in two groups of Australian inpatient (n = 4) and community-based (n = 6) physiotherapists and occupational therapists. Based on the pilot and clinician feedback, the focus group questions were refined to their final version (see Supplemental material 1).
Each focus group was conducted by three members of the research team, one primary facilitator, and two co-facilitators that took notes and provided prompts as needed. Each member of the research team conducted between two and three focus groups. One member of the research team (DK) facilitated the first two focus groups and then observed all others to ensure consistency. All research team members had undertaken training in focus group facilitation. At the beginning of each focus group, the facilitators provided a brief overview of their clinical and research experience and informed the participants that the goal of the research was to understand the clinical reasoning processes of allied health professionals that worked in stroke rehabilitation. The facilitators also confirmed that each participant had watched the educational video. If a participant had not, they were asked to leave the group and attend another focus group after they had watched the video. The primary facilitator made an effort to set an informal atmosphere and clearly stated that different perspectives were expected, and that all ideas were welcome. No study participant had a pre-existing relationship with the primary group facilitators, but several co-facilitators knew study participants in a professional capacity. At the start of each focus group, the primary facilitator obtained the profession, experience in stroke rehabilitation, practice setting, and geographic location of each participant.
This study was designed according the Consolidated Criteria for Reporting Qualitative Research 16 and is also reported according to these criteria (Supplemental Material 3). The research team was made up of three researcher physiotherapists (one male, two female), six practising occupational therapists (all female), one female researcher occupational therapist, one female researcher speech pathologist, one male researcher neuropsychologist, and one male who was both a researcher physiotherapist and an exercise physiologist. Team members were based in Australia, Ireland, and the United Kingdom; however, their countries of origin also included the United States of America, Brazil, and New Zealand. The focus groups were conducted by team members from at least two different professional and national backgrounds. Data analysis was conducted by three Australian-based researcher physiotherapists with a research focus in neurological rehabilitation; one with a particular interest in spatial neglect and implementation research, one with an interest in research methods and emerging technologies, and another with a broad interest in neurological rehabilitation.
Data Analysis
The focus group recordings were de-identified and transcribed verbatim by a single researcher (MC). Three members of the research team (GF, CQ, PS) independently extracted and coded data from transcripts in pairs using the process of analysis recommended by Gale et al. 17 Disagreements were resolved through consensus with a fourth member of the research team (DK). The NVivo program 18 was used to code focus group transcriptions. Transcripts were analysed using two methods. A deductive framework analysis was used on focus group questions 1 to 9, where data was mapped to the Theoretical Domains Framework 15 to describe the barriers and facilitators to standardised functional assessment of spatial neglect. The analysis included an additional category of ‘Other’ to allow additional codes for relevant data that did not fit within the Framework. After data had been coded into the Theoretical Domains Framework domains and sub-themes, raw counts of the frequency of each sub-theme were calculated. An inductive content analysis 19 was used for focus group questions 10 to 13, to examine participants’ perceptions about an ideal assessment of spatial neglect, and their suggestions on strategies to implement it into clinical practice. After data extraction was finalised, one member of the research team (GF) selected quotations that were representative of each framework item, and each sub-theme that was generated in the thematic analysis. These quotations were reviewed and approved by all members of the research team.
Results
A total of 399 clinicians attended the educational bootcamp, of whom, 395 were from the United Kingdom or Ireland. Seventy-four clinicians expressed interest to participate in the study and were screened against the study eligibility criteria. A total of 27 clinicians elected to participate in the study. Each focus group had an average of three clinicians (range 2–4). Participants included 23 occupational therapists, three physiotherapists, and one orthoptist with a mean of 11 (range 2–20+) years of clinical experience. Two participants worked in hyperacute stroke wards (0 to ∼72 hours post-stroke), 10 in acute inpatient wards (∼3 to ∼7 days post-stroke), six in sub-acute inpatient wards (∼7 + days post-stroke), seven in community settings, and two in outpatient clinics. Most clinicians were from Northern Ireland (n = 20) with six from the Republic of Ireland and one from Scotland. One participant did not watch the educational video before participating in a focus group; this participant was unable to attend any other session and so was permitted to participate in the focus group without having viewed the video.
Primary Determinants of Assessment of Spatial Neglect in Clinical Stroke Rehabilitation
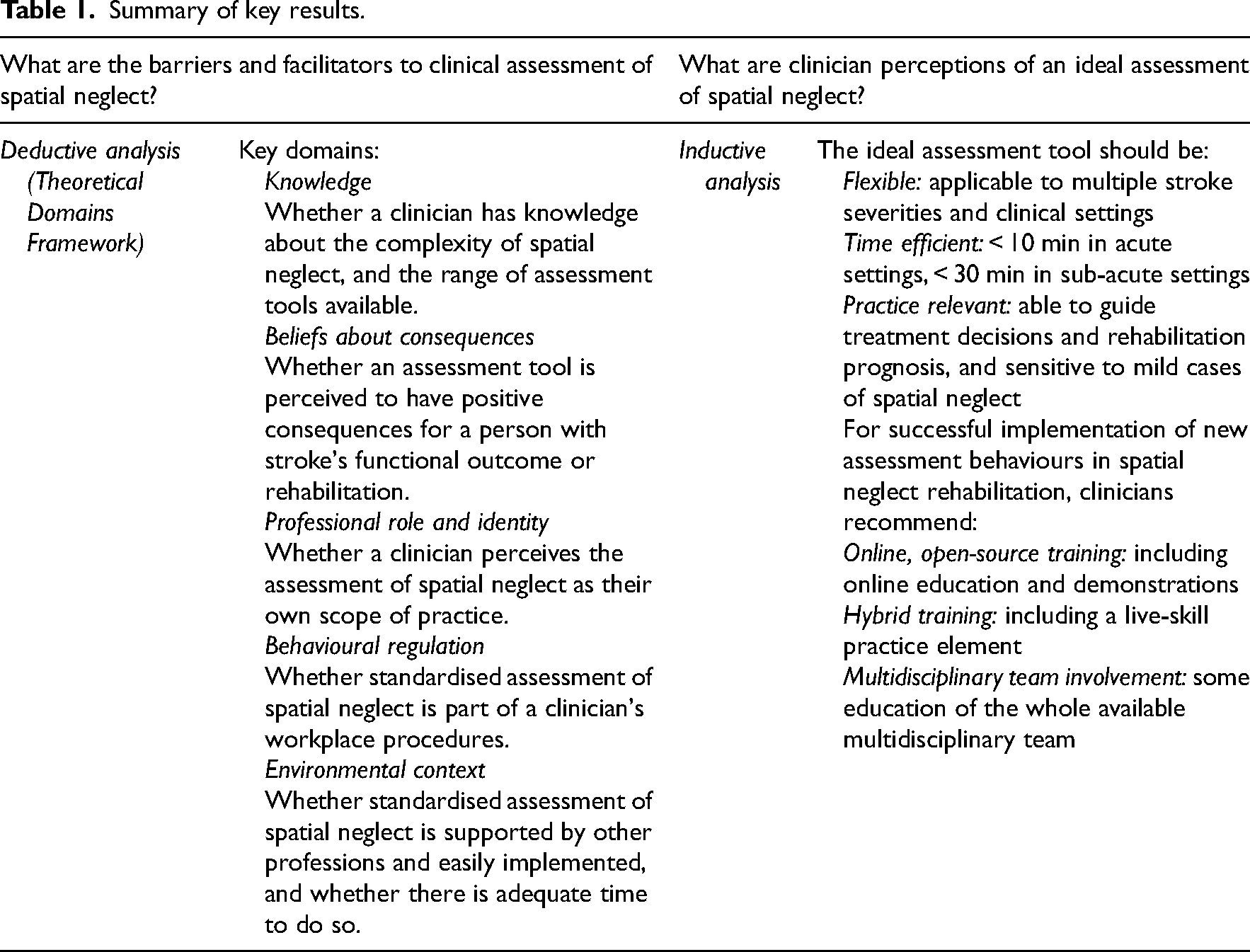
The five most reported sub-themes occurred in the Theoretical Domains Framework domains of Knowledge, Beliefs about Consequences, Professional Role and Identity, Behavioural Regulation, and Environmental Context and Resources. These are detailed in Table 1.
Summary of key results.
A frequent factor that appeared to influence functional spatial neglect assessment was lack of Knowledge, which included a lack of knowledge about spatial neglect (n = 31 quotations), and a lack of knowledge about assessment tools (n = 31 quotations). … ‘ [the online educational session] helped me to think neglect is not just visual, it's auditory, sensory, you know as well, and remind me of the personal, peri-personal, and extra-personal spaces’ (ACUTE_OT_20) ‘I wasn't aware of a lot of these tests either so it was really good to learn about different ways to assess for neglect [in the video]’ (COMMUNITY_OT_11)
‘… we would take patients off the corridor and get them to point out coloured objects on either side … but I hadn't realised there was an actual you know assessment [the Dublin Extrapersonal Neglect Assessment] for that’ (ACUTE_OT_1)
Clinicians reported being more likely to use an assessment of spatial neglect in practice when there was a strong, positive Beliefs about Consequences for the functional outcome and goals of a person with stroke (n = 28). They also reported that they were more likely to use an assessment that they perceived would have a positive impact on the experience of a person with stroke, for example, an assessment that would make their rehabilitation goals clearer.
‘[Functional assessment] is something that … would be able to help you in your practice to recognise some additional things that might need to be addressed for someone to go home’ (HYPERACUTE_OT_10)
Clinicians also reported that they were more likely to choose an assessment of spatial neglect that they could use to develop insight in people with stroke and their families (n = 16).
‘We've had instances of families wanting to take patients home that have quite significant deficits including neglect, and you're trying to explain you know, what the care needs are and how the neglect in particular impacts on [going home] and it [assessment] might be a really helpful way of you know, helping them to understand what it [going home] actually looks like.’ (ACUTE_OT_24)
A participant's Professional Role and Identity played a key part in their clinical assessment of spatial neglect. The perception of spatial neglect assessment as being part of one's own professional scope of practice likely facilitated the use of standardised assessments. Perception of assessment as another profession's scope of practice may have hindered the use of standardised spatial neglect assessment. The assessment of spatial neglect was predominately perceived to be in the scope of practice of occupational therapists (n = 24 quotations).
‘I suppose coming from a physio background I probably would have felt we maybe had slightly less of a role to play in the more in-depth assessment of neglect’ (SUBACUTE_PT_5)
‘I think [spatial neglect assessment] does sit comfortably with within occupational therapy because of our remit [and] because of our ethos of doing functional tasks’ (COMMUNITY_OT_2)
Clinicians reported that standard workplace protocols were an important component of Behavioural Regulation in spatial neglect assessment (n = 20 quotations). Because of these protocols, many clinicians used a pen-and-paper test as a screening tool to indicate the need for further assessment and then used functional assessments in their practice.
‘… in Northern Ireland we have a regional neurological assessment tool and some of the pen and paper tests are on it and that's generally our go to’ (ACUTE_OT_20)
Environmental context and resources were unsurprisingly influential in clinical implementation. In the environmental context, COVID-19 restrictions were a barrier to functional assessment, mainly due to equipment cleaning requirements and limited access to group rehabilitation settings (n = 11 quotations).
‘Well at the minute I haven't had an OT department for a year because of COVID, all our assessments are entirely ward based because we're not allowed to bring the patients anywhere else’ (ACUTE_OT_20)
Participants described barriers associated with early acute stages of the continuum of care, where the severity of impairments (n = 12 quotations) and short length of stay (n = 12 quotations) limited the ability of clinicians to implement a more functional spatial neglect assessment.
‘It depends on the stage of the patient; I think working in a very very sick patient in acute or hyper acute stroke units … some of our patients will not be able [to do] any of those assessments’ (ACUTE_OT_18)
‘[Pen and paper assessments] would be our kind of go-to ones at first because they are quick to use [because with] acute patients there's quite a quick turnaround’ (ACUTE_OT_1)
An engaging, salient environment increased the perceived sensitivity of functional assessment tools and facilitated their use, while conversely, a controlled clinical environment did the opposite (n = 5 quotations).
‘… being in an outpatient setting and the bit that's maybe missing … is observing how they're functioning within the context of the home environment at that point’ (OUTPATIENT_OT_7)
When it came to resources, therapists reported that the cost (n = 5 quotations), and the number of required items of equipment (n = 6 quotations) were barriers to assessment use. Additionally, time was another barrier that impacted on assessment implementation in multiple ways, including the amount of time needed to perform the assessment (n = 10 quotations), the length or number of sessions with a person with stroke (n = 6 quotations), and the time required to learn a new assessment (n = 4 quotations).
‘One of the upper limb tools we use here … there's so many things you have to gather before you can even start it and that just puts people off using it’ (ACUTE_OT_27)
‘I have been aware of [the Catherine Bergego Scale] … but again it's something I just haven't got time to get into and to look into more depth and to implement in our workplace’ (ACUTE_OT_20)
Clinicians also reported having varied access to a full multidisciplinary team to assess spatial neglect, or to clinical specialities in the area (n = 19 quotations). For example, some clinicians reported that they felt well supported by psychologists and ophthalmologists, others reported that these professions were part of their multidisciplinary team but hard to access due to their part-time hours or locations in separate clinics, and still others reported no access at all.
‘We have access here to orthoptics at the hospital has one and we also have access to a neuropsychologist, a neuropsychologist is with us only half the week’ (ACUTE_OT_20)
‘From our point of view from our team um the neuropsychologist and orthoptist would be something that would come along in a couple of weeks’ time, it wouldn't be like the instant review that we would be under pressure to see people sooner’ (COMMUNITY_OT_22)
Other Determinants of Spatial Neglect Assessment
Most clinicians reported that their Decision-Making Processes involved using assessments that they were familiar with, or that could be incorporated into other tasks they frequently completed in their clinical practice (n = 17 quotations). ‘I think another barrier can just be implementing any change … if people are used to certain tools, um, you know they might be of the opinion “why do we need to change?”’ (ACUTE_OT_27)
Optimism towards the clinical utility, ease of implementation, and the positive outcomes of a functional assessment for people with stroke and their families increased willingness to assess spatial neglect (n = 19 quotations).
‘I found that the Catherine Bergego Scale was more relevant to [my practice] and I like the way that it covers so many areas and yeah, so I think I’ll be using that one in the future’ (COMMUNITY_OT_11)
Clinicians reported that their Beliefs about Capabilities in using an assessment tool were an important factor for its use. Clinicians that felt that they were capable to implement assessments correctly were more likely to attempt to do so (n = 17 quotations).
‘I think it's the [clinician's] confidence … it can really affect confidence if you don't feel that you're doing it right and you don't get the full benefit from it’ (COMMUNITY_OT_11)
The Social Influences of the care team were important, where clinicians working in supportive social environments were more likely to trial new, evidence-based assessments (n = 11 quotations).
‘My senior's been very good at sitting down informally … and being pretty proactive in supporting you in innovative ways of working or assessing’ (HYPERACUTE_PT_15)
Finally, negative Emotions such as anxiety about consequences and embarrassment about capability were motivators to learn more about functional assessment of spatial neglect (n = 5 quotations).
‘I’d be terribly worried if a person had fallen through the net and was actually already back driving, that would terrify me’ (OUTPATIENT_OT_7)
Clinician Perceptions About an Ideal Assessment of Spatial Neglect
The inductive analysis of interview questions 10 to 13 examined participants’ perceptions about an ideal assessment of spatial neglect and revealed two main themes. First, the ideal assessment tool should be time efficient and cater to complex stroke presentations in all clinical settings. Second, training, online resources and the involvement of a multidisciplinary team were perceived as desirable for successful implementation of new assessments of neglect. These themes are summarised in Table 1.
The ideal assessment tool should be time efficient, functional, and sensitive to different severities of unilateral neglect in all clinical settings.
Clinicians indicated that any assessment tool needed to be time efficient and completed in under 30 min. However, the ideal assessment time differed between settings and the continuum of care. Clinicians in the acute setting reported that the tool should be completed in under 10 min, whereas clinicians in the sub-acute setting reported 15 to 30 min as a reasonable time for completion. Clinicians agreed that any assessment tool should be able to detect spatial neglect in individuals with more complex needs; for example, those with aphasia, cognitive impairment, or significant fatigue. ‘I think the speech is a big issue, the aphasic stroke patient is a very difficult patient to assess generally for perception and cognition, um, so I think some elements of it may need to be by demonstration’ (OUTPATIENT_OT_16)
‘…if it's a comprehensive functional assessment … that can have an impact on your recommendations for your rehab and your follow-on to educating family members as well about the functional implications of the neglect’ (ACUTE_OT_3)
Despite acknowledgement of differing needs in different settings, clinicians also perceived that the tool should be applicable to multiple clinical settings to facilitate continuity of care for people with stroke.
‘Something that often comes up you know in acute is … we're using different tools [to rehabilitation settings] … so if there was a way of saying well you know this is the first section of the screening that you might do in acute hospital and then that is continued on in rehab, like a like an extension of it, so that the work you're doing the acute actually feeds into … rehab’ (ACUTE_OT_27)
Training, online resources and the involvement of a multidisciplinary team are desirable for successful implementation of new assessments of neglect.
When it came to implementing a new evidence-based assessment of spatial neglect, clinicians indicated a preference for online, open-access to training resources and demonstrations. They also recommended a hybrid training format, with a live-skill practice element that could be in person or facilitated online. ‘Examples are good as part of an online training where you actually see an example of a patient and maybe them completing [the assessment] and you have to try and score it … so you know the practical [training], not just listening to somebody talking about the assessment’ (ACUTE_OT_3) ‘Online training and then as well maybe just practising on each other as therapists … before doing it with patients just so we're familiar and confident with it’ (ACUTE_OT_1)
Most participants (n = 11) supported the involvement of the entire multidisciplinary team in the implementation of assessments for neglect, while a portion of clinicians were supportive of implementation led primarily by physiotherapists and occupational therapists (n = 8). ‘I think it's got to be a multidisciplinary team approach both in the assessment and the intervention because everyone's got to be working with a common goal’ (OUTPATIENT_OT_7) ‘I agree with HYPERACUTE_PT_15 in terms of I think … ideally both occupational therapists and physiotherapists should both be assessing for neglect’ (ACUTE_OT_13)
Discussion
Spatial neglect negatively impacts the functional outcomes and prognosis of many people with stroke.5,20 However, in rehabilitation settings, clinicians rarely use standardised assessments that evaluate the impact of spatial neglect on functional outcomes.9,10 In our deductive analysis using the Theoretical Domains Framework, 15 many clinicians reported that they lacked knowledge on the variety of ways that spatial neglect can present after stroke, which influenced clinician beliefs and choices about assessments for spatial neglect. Our inductive analysis showed that clinicians believed that an ideal assessment of spatial neglect needed to be flexible to both their own and the needs of people with stroke, time efficient, and relevant to their clinical practice, attributes that they perceived were lacking in many current assessment tools. To change their assessment practice behaviours, clinicians recommended open-source, online education and training that included at least some live-skill practice, and that was offered to all members of the multidisciplinary team.
Many participants in the present study understood spatial neglect predominately as a disorder of visual attention, rather than a disorder of multisensory processing. 21 Similar results were reported in a recent survey of clinicians in the United Kingdom about their knowledge of visual perceptual deficits in people with stroke. 22 These beliefs likely reflect the visual emphasis of the literature on spatial neglect. For example, there are 90 published assessments specific to visual neglect, compared to nine assessments specific to motor neglect, and six assessments specific to auditory neglect. 8 In the context of the International Classification of Function model, 23 only 18% of the spatial neglect assessments evaluate activity limitations and only 1.7% evaluate participation restrictions. 8 Many participants in the present study preferred assessments that were related to function, but lacked knowledge about standardised, published functional assessments of spatial neglect. It is understandable that clinicians would use the standardised assessments at the impairment level that they were aware of, and then attempt to supplement these with unstandardised observation of activity limitations and participation restrictions.
In stroke rehabilitation, impairments are often arbitrarily divided into defined ‘scopes of practice’ of multiple clinical specialties. 24 Assessment of visual perceptual deficits is considered the scope of practice of occupational therapists, neuropsychologists, and orthoptists. If clinicians understand spatial neglect to be primarily a disorder of visual perception, they would naturally ascribe standardised assessment of the condition to these professions, which was indeed reflected in the present study, and in previous investigations.10,22 Importantly, many clinical rehabilitation settings lack consistent access to orthoptists and neuropsychologists (e.g. ref 25 ), and as such, clinical assessment of spatial neglect often falls to occupational therapists. 10 However, the impact of spatial neglect spans multiple sensory modalities, and there is scope for multiple professions in the rehabilitation team to be involved in the assessment and management of spatial neglect, including physiotherapists and nursing staff. The impact of spatial neglect is also context dependent; the severity of a person's presentation can fluctuate based on multiple factors including the environment, fatigue, stress, and the number of distractions present.26,27 If spatial neglect is assessed by a single profession at a single timepoint, the total impact of spatial neglect on a person with the condition is difficult to estimate and can be misjudged. 28
Clinician education and training about spatial neglect as a multisensory disorder and the available standardised functional assessments, as well as training in their use, is likely an important step towards evidence-based practice in this area, and should include education of multiple members of the multidisciplinary team. Support for implementation could be provided by a clinical champion, an established strategy in practice-change interventions in stroke rehabilitation in which a team member is nominated to motivate others and facilitate change in a particular component of clinical practice. 29 Changes to healthcare and education delivery in the COVID-19 pandemic and its associated lockdowns and restrictions mean that many clinicians have adapted to online-only or hybrid formats for both service delivery and ongoing education, and thus the development of open-source, online education and training resources for clinicians is an important future direction in this area.
There were several strengths of the design and methods of this study. First, the use of the Theoretical Domains Framework allowed determinants of clinician behaviour to be described in a comprehensive, theory-informed approach. Second, the online delivery of the study meant that a sample of clinicians from a wide range of health organisations and clinical settings were able to participate in the study. Finally, while focus group questions were pre-defined, the use of different moderators meant that groups were not biased towards the perspective of a particular member of the research team. However, the member of the research team that provided the education session (DK) observed each focus group, and moderated two groups, which could have positively biased clinician responses. While the bootcamp from which study participants were recruited was open to all types of allied health clinicians from any country, the clinicians in this study were almost all occupational therapists from the United Kingdom and the Republic of Ireland. As such, the results are less generalisable to other allied health professions in stroke rehabilitation, and the health services of other countries, especially low-income countries. A second limitation was the use of an educational session prior to the focus group sessions; this is a potential behaviour change strategy and risked pre-empting or biasing the study results by providing knowledge to participants. It also may have influenced the type of clinicians in the study sample, as those who felt that they had adequate knowledge about spatial neglect may have declined to participate.
Based on this foundational investigation, future research could use theory-informed behaviour change approaches such as the Theoretical Domains Framework with the Behaviour Change Wheel to further refine knowledge of the key barriers and facilitators in other groups and healthcare settings. 30 This would facilitate the development of tailored behaviour change interventions, which could be implemented at scale to increase the use of standardised assessment of spatial neglect in clinical practice.
Spatial neglect has a significant impact on the function of people with stroke; however, clinicians do not commonly use validated functional assessments for the condition. The results of our study suggested that this pattern of clinical behaviour is due to clinicians’ lack of knowledge about unilateral neglect as a multisensory disorder, and about available assessment tools.
Clinical messages
Clinicians should use standardised assessments for spatial neglect that include functional tasks.
All multidisciplinary team members should understand assessments of spatial neglect that are in use and be able to interpret their results.
To change practice in this area, clinicians should use evidence-based strategies for behaviour change.
Supplemental Material
sj-docx-1-cre-10.1177_02692155241230270 - Supplemental material for Spatial Neglect: An Exploration of Clinical Assessment Behaviour in Stroke Rehabilitation
Supplemental material, sj-docx-1-cre-10.1177_02692155241230270 for Spatial Neglect: An Exploration of Clinical Assessment Behaviour in Stroke Rehabilitation by Georgia Fisher, Camila Quel de Oliveira, Peter W. Stubbs, Emma Power, Matthew Checketts, Alison Porter-Armstrong and David S. Kennedy in Clinical Rehabilitation
Supplemental Material
sj-docx-2-cre-10.1177_02692155241230270 - Supplemental material for Spatial Neglect: An Exploration of Clinical Assessment Behaviour in Stroke Rehabilitation
Supplemental material, sj-docx-2-cre-10.1177_02692155241230270 for Spatial Neglect: An Exploration of Clinical Assessment Behaviour in Stroke Rehabilitation by Georgia Fisher, Camila Quel de Oliveira, Peter W. Stubbs, Emma Power, Matthew Checketts, Alison Porter-Armstrong and David S. Kennedy in Clinical Rehabilitation
Supplemental Material
sj-docx-3-cre-10.1177_02692155241230270 - Supplemental material for Spatial Neglect: An Exploration of Clinical Assessment Behaviour in Stroke Rehabilitation
Supplemental material, sj-docx-3-cre-10.1177_02692155241230270 for Spatial Neglect: An Exploration of Clinical Assessment Behaviour in Stroke Rehabilitation by Georgia Fisher, Camila Quel de Oliveira, Peter W. Stubbs, Emma Power, Matthew Checketts, Alison Porter-Armstrong and David S. Kennedy in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors would like to acknowledge the assistance of the REfLECTS Team (Patricia McIlwaine, Lourene Abbi, Leona Robinson, Fiona Morrow, Beverley Turtle, May Stinson) in conducting the study focus groups.
Author Contributions
DK and GF conceived the study, and all authors designed the study and collected data. GF, PS, and CQ analysed data. GF completed the first draft of the manuscript which was then critically reviewed by all authors. APA obtained the funding for the bootcamp from which the study was conducted.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The bootcamp was free to attend for all participants and was funded through the CHITIN portfolio (Department of Health NI and the Health Service Executive (ROI)) from the EU's INTERREG VA Programme which is managed by the Special EU Programmes Body (SEUPB).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.