
Abstract
Background
There is no general theory of rehabilitation, only definitions and descriptions, with the biopsychosocial model of illness as a structure.
Objective
To develop a general theory of rehabilitation that explains how healthcare rehabilitation changes outcomes and to evaluate its validity.
Need
A general rehabilitation theory would help research, improve services, increase understanding, modify resource allocation and explain some anomalies, such as how rehabilitation helps when no natural recovery occurs.
Building blocks
People adapt to change throughout their lives. Illness is a change, and people adapt to their illness. Adaptation's purpose is to maintain an equilibrium in a person's life. The balanced components are related to Maslow's five needs: basic, safety, affiliation, status and self-fulfilment. The general theory of behaviour suggests that a person's behaviours change to maintain balance, regulated by a central homeostatic mechanism.
The theory
Rehabilitation aids adaptation to changes associated with illness through accurate diagnosis and formulation, catalysing adaptation, optimising the environment and assisting the person in making necessary changes by safely practising activities and teaching self-management.
Implications
The theory makes the person the central active agent, emphasises the importance of the environment in facilitating adaptation, explains why all conditions may benefit, including progressive and static conditions, suggests that health can be equated to someone maintaining their equilibrium and explains why a small dose may be very effective.
Conclusion
The general theory of rehabilitation emphasises the catalytic effects of rehabilitation in facilitating and guiding adaptation and suggests areas for research and improvement.
Introduction
Rehabilitation benefits patients, but how? John Whyte reviewed rehabilitation theories in 2008, emphasising the need for a general theory to answer this question. 1 A comprehensive definition of rehabilitation 2 derived from a systematic review of published definitions 3 describes rehabilitation. It is a reiterative problem-solving process constituting assessment, formulation, goal-setting and planning, undertaking interventions and evaluation.4–6 The main effective interventions have been described. 7 Descriptions do not constitute a theory and cannot explain anything.
Theories exist for bits of rehabilitation, such as learning8,9 and goal-setting. 10 The biopsychosocial model of illness is rehabilitation's conceptual, theoretical framework. 11 The World Health Organisation improved this model by adding environmental and personal contexts in the International Classification of Functioning, Disability and Health (WHO ICF).12,13 The addition of time, choice and well-being made the model holistic.14,15 It encompasses the biomedical 14 and social models. 16
What is a theory, and how might it help?
A theory is ‘a supposition or a system of ideas intended to explain something, especially one based on general principles independent of the thing to be explained’ (Oxford English Dictionary (OED)).
Theories comprise concepts and principles; they change the world. A good theory's five essential characteristics
17
are that it is:
Testable, making predictions that can be tested; if the prediction is not upheld, the theory is disconfirmed. Coherent, understandable and logically consistent without contradictions. Economical, with fewer variables than other theories covering the same field. Broadly applicable, covering almost all instances of the phenomenon, not just in restricted circumstances. Explanatory, consistent with all known observations and unexplained or contradictory ones.
A rehabilitation theory should incorporate subsidiary theories, increase understanding of rehabilitation and predict ways to improve it. It should explain how rehabilitation has an effect with a small dose. For example, stroke units have a large effect,
18
yet the contact time is 5–10 h a week.19,20 The dose–response relationship is weak.21–23 Establishing a dose–response relationship is challenging because the content is often missing.
24
The effect may be unrelated to the dose of the intervention being studied.
25
It should also explain how rehabilitation is effective in almost all conditions. 7 Rehabilitation benefits patients with conditions where recovery occurs, such as stroke 18 or progressive conditions, such as multiple sclerosis26,27 or conditions with no recovery, such as complete spinal cord injury.
John Whyte also said, ‘At the level of body structure and function, demand-based adaptation is a pervasive phenomenon’. 1
Adaptation
People adapt to their illnesses. In 1986, David Mechanic said, ‘Illness behaviour arises in response to circumstances that challenge the ongoing homeostasis. People are extraordinarily adaptive, but some changes in the situation, whether arising within the organism or from external factors, induce self-consciousness and appraisal and require assessments about the nature of the problem, its causes and the strategies to be initiated’. 28
In 2004, JT Young made the central role of adaptation explicit, ‘The fact of illness requires that the sick adapt to illness. This adaptation is moulded by society through cultural, social, institutional and biomedical mechanisms of interaction’. 29
To adapt is to ‘become adjusted to new conditions’ (Oxford English Dictionary (OED)).
People encounter new conditions throughout life. Some are minor, such as a change in the weather or the breakdown of a machine and others major, such as the death of a parent or starting a new job. Adaptation occurs throughout life and every day.
Other people assist with adaptation. Parents, siblings and education facilitate changes associated with growth and development from birth to independent adulthood. Adults may seek support from education, employers and others as needed. When someone falls ill, the healthcare system meets physiological and safety needs.
Adaptation is a feature of all life. It is the mechanism underlying evolution and the survival of a species. Over short periods, adaptation's purpose is to promote the survival of the individual by maintaining a balance; 30 it is a homeostatic mechanism. Adaptation to maintain equilibrium applies as much to a person as it does to the body or group.
Biopsychosocial adaptation
The body maintains a physiological (biological) balance. 31 This is called homeostasis, a word coined by WB Cannon in 1926, meaning ‘the tendency towards a relatively stable equilibrium between interdependent elements, especially as maintained by physiological processes’ (Oxford English Dictionary (OED)).
A person will also balance non-biological parameters; the biopsychosocial model suggests these may be psychological and social and will be determined by the person.
Personhood is discussed extensively in philosophy.32,33 The Oxford English Dictionary [OED] describes it as ‘the quality or condition of being an individual person’; it is the person's essence. The person has a narrative identity: how they recall and interpret their life 34 and decide on goals.35,36
The person is central to the general theory of behaviour, 37 which stresses that people have a purpose as part of their identity, 38 working towards meaningful goals, which can be identified in rehabilitation.39,40
The person is central to healthcare. William Osler (1849–1919) summarised this in an aphorism, ‘Ask not what disease the person has, but rather what person the disease has’. His implied contrast between the bodily focus of biomedical healthcare 14 and person-centred healthcare is illustrated vividly in Figures 4 and 5 of chapter three of the White Book. 41 The person is central to the biopsychosocial model of illness.42,43 Being person-centred 44 follows naturally from using the biopsychosocial framework.45,46
The person's equilibrium
What factors are balanced? The General Theory of Behaviour suggests that ‘human thriving is dependent upon an intrinsic homeostasis system with purpose, desire and intentionality striving to maintain equilibrium’. 47 Figure 1 of a recent paper 48 illustrates how psychological homeostasis might be maintained in response to change through a behavioural homeostatic process, the reset equilibrium function. 37
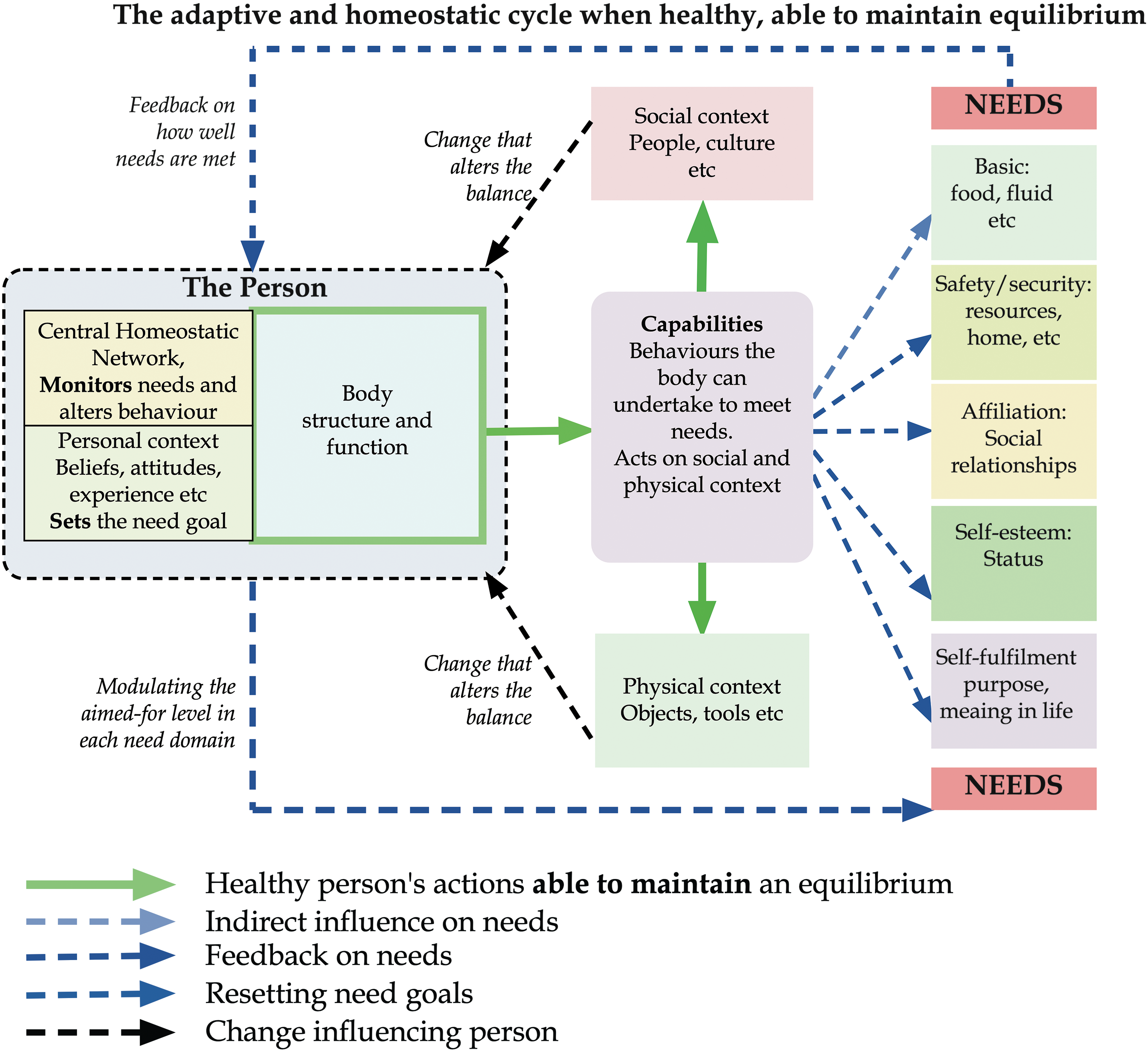
The adaptive and homeostatic cycle when healthy, able to maintain equilibrium.
The biopsychosocial model of illness suggests that a person will balance physiological (i.e., biological), psychological, and social parameters. Physiological balance was confirmed over a century ago. 31 Psychological homeostasis was first suggested in 1942 49 and was listed as one of ten areas of human homeostasis in 1966. 50
Social homeostasis in rodents is maintained by neural mechanisms that counter a lack of social contact to avoid loneliness. 51 Research has also identified neural control of a balanced level of social contact52,53 and that people maintain their subjective well-being around a set point, 54 a mechanism underlying resilience. 55
A person's complex mix of parameters can be analysed using Maslow's hierarchy of needs, 56 which applies in most countries and cultures. Satisfaction with these needs is associated with higher subjective well-being, 57 equivalent to their quality of life. 58
Thus, in addition to their bodily physiological parameters, a person will balance the five needs Maslow identified:
basic physiological needs (hunger, thirst, etc.), safety and security (self-protection), love and social support (affiliation with others, social contact), self-esteem and respect (status in society), self-actualisation and autonomy (self-fulfilment)
They will determine the expectation and the weight given to each need. However, the more fundamental needs, such as physiological and safety, will typically have a higher priority if unmet.
Behaviour and homeostasis
The general theory of behaviour suggests a central homeostatic network 59 maintains non-physiological balance by altering a person's behaviour. 37 Central neural homeostatic mechanisms may underlie adaptive response to trauma 60 and making adaptive decisions. 61
Maintaining equilibrium is an automatic process. The brain has many networks that control complex automatic behaviours such as driving to work or responding to someone saying, ‘Good Morning. How are you’? These networks allow the person to think of other matters, but they can be controlled and altered consciously. Networks controlling adaptive mechanisms have been identified.51–54 Figure 1 illustrates the general mechanism.
Adapting to illness adds challenges not faced with other changes. Suppose the person's bodily structures and functions are affected. In that case, the behaviours available may be reduced, limiting the adaptive response, and if their brain is affected, their intrinsic adaptive abilities may be reduced. Figure 2 illustrates this; the illness limits the ability to maintain equilibrium, as the red arrows show.
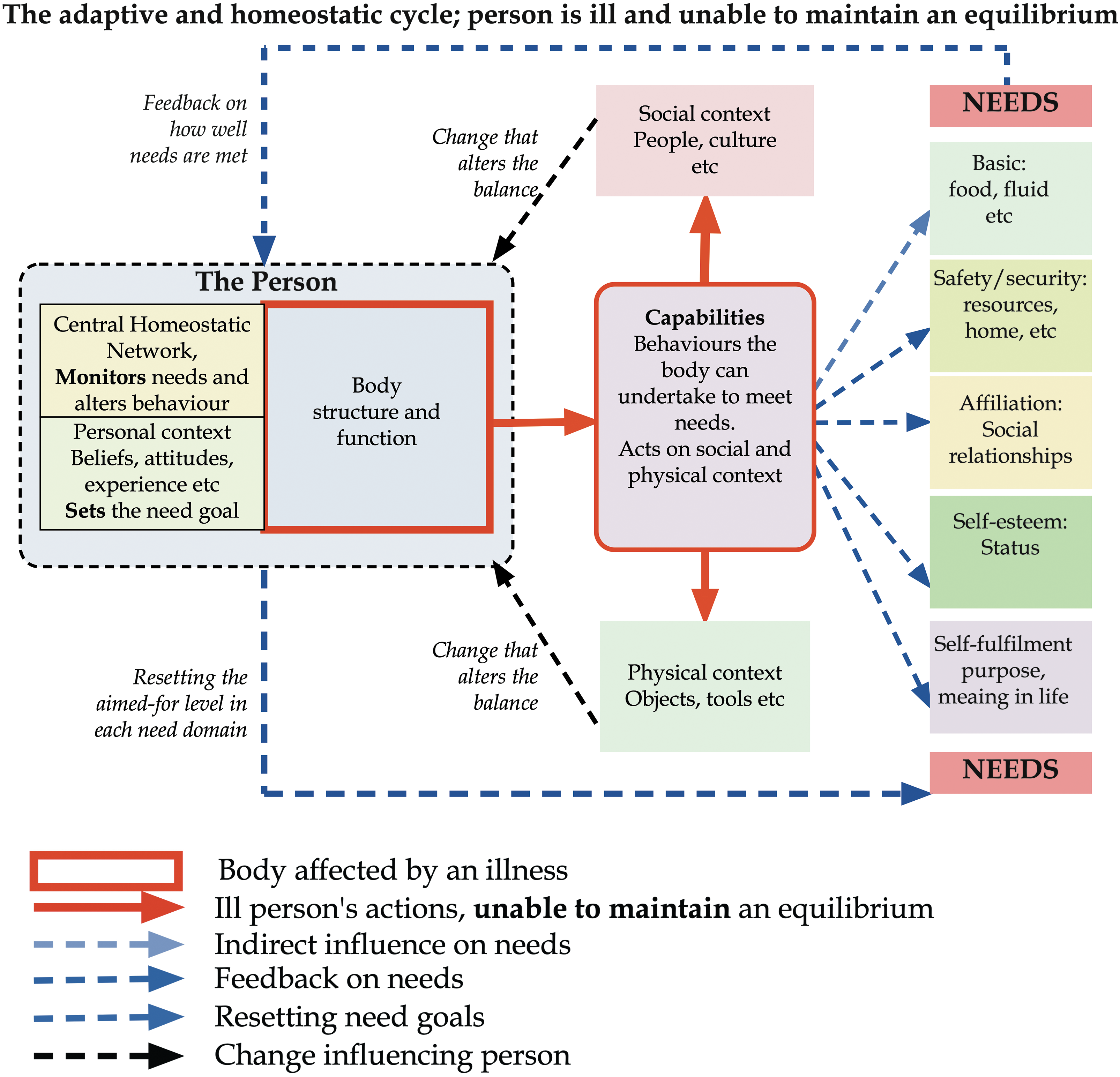
The adaptive and homeostatic cycle; person is ill and unable to maintain an equilibrium.
Under these circumstances, four broad responses are available:
alter the levels aimed for in one or more areas of need to a level that can be achieved, alter the activities (behaviours) used to achieve the needs, learn new ways to perform previous activities or new activities to satisfy the needs, change the social or physical environment so that the requirements can still be satisfied. reduce the level of need aimed for.
People facing challenges they cannot overcome typically seek help, an adaptive response. For example, someone who loses a job may seek help from an employment advisor, friends, or the Internet. They might seek a different position and educational or vocational training resources to help them. People who develop an illness will also seek advice and support. When ill, they may approach healthcare.
Rehabilitation's role
Healthcare supports ill people. Biomedical healthcare helps maintain their bodily physiological balance, for example, in an intensive care unit or by giving insulin or anti-hypertensive medication, and their function in the short term by helping with personal care activities.
The need to offer civilians rehabilitation was recognised as early as 1918.
62
The recognised roles of rehabilitation can be summarised as undertaking:
a holistic assessment and formulation, including a prognosis planning how to achieve self-identified or negotiated goals, specific actions that the patient needs, such as
Helping the person relearn activities or learn new activities, Teaching the person how to manage their condition, Assisting the person in setting goals, Advising on and sometimes providing aids, adaptations, housing, equipment etc., Advising on and sometimes providing care and support.
Most of these actions will facilitate and sometimes guide the person's adaptation. They depend upon expert knowledge and skills the person is unlikely to have. Most rehabilitation input will facilitate adaptation.
Rehabilitation's effect is thus indirect and can best be considered catalytic. A catalyst is ‘a substance that increases the rate of a chemical reaction without itself undergoing any permanent chemical change’ with a subsidiary description, ‘a person or thing that precipitates an event’ (Oxford English Dictionary (OED)). Rehabilitation catalyses a person's adaptation.
Rehabilitation comprises many actions and is not a single catalyst. Effective rehabilitation is a systematically organised series of catalytic activities, often interdependent and only effective in combination. The rehabilitation team is analogous to a cell's endoplasmic reticulum; 63 it may catalyse many actions, some in series and some in parallel. The activities must be coordinated and often undertaken in a specific order and with others.
Thus, my central hypothesis is that rehabilitation aids natural adaptation to the changes associated with illness primarily through a systematic series of catalytic actions, identifying or facilitating changes the person can make. This is illustrated in Figure 3.
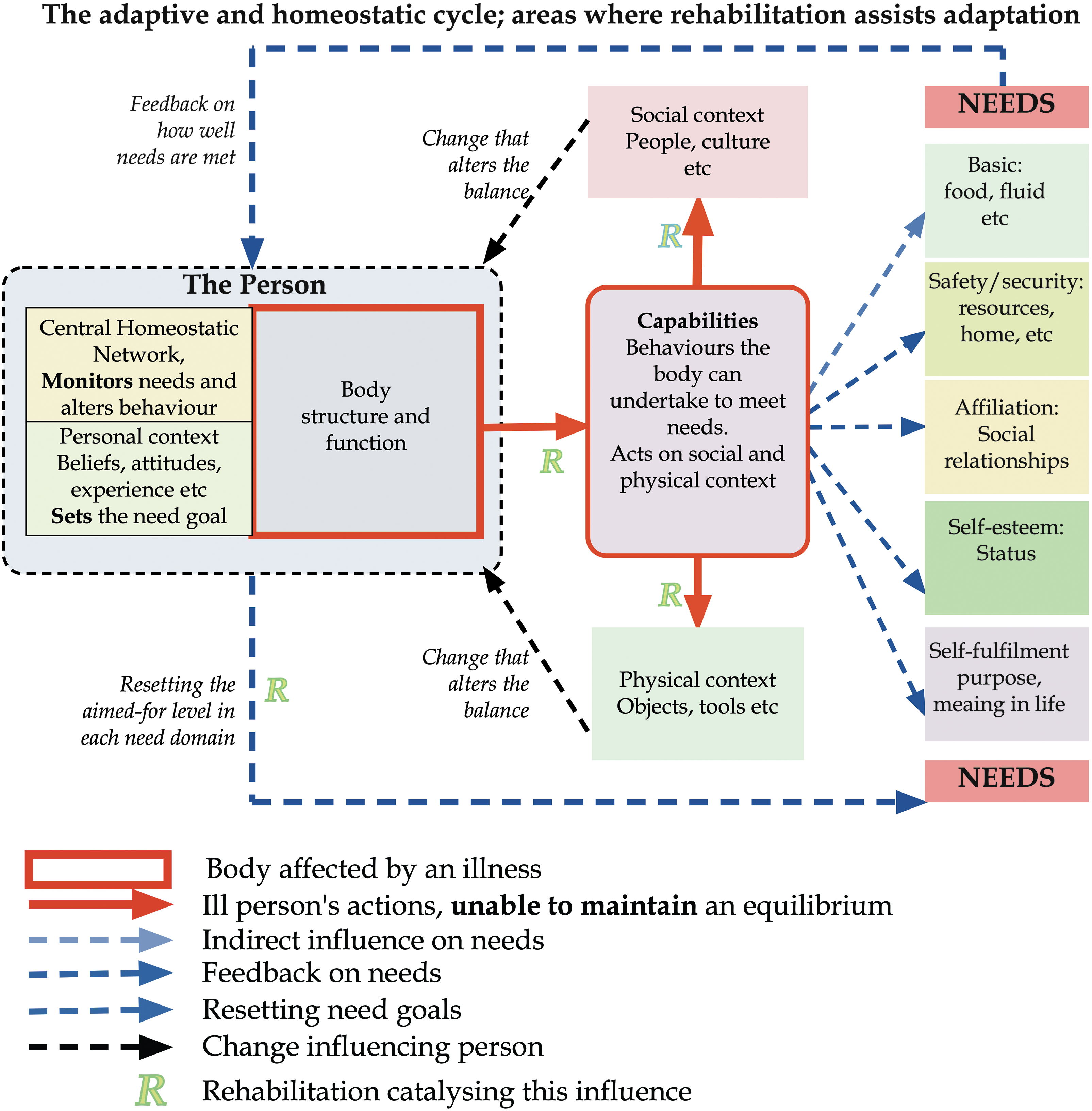
The adaptive and homeostatic cycle; areas where rehabilitation assists adaptation.
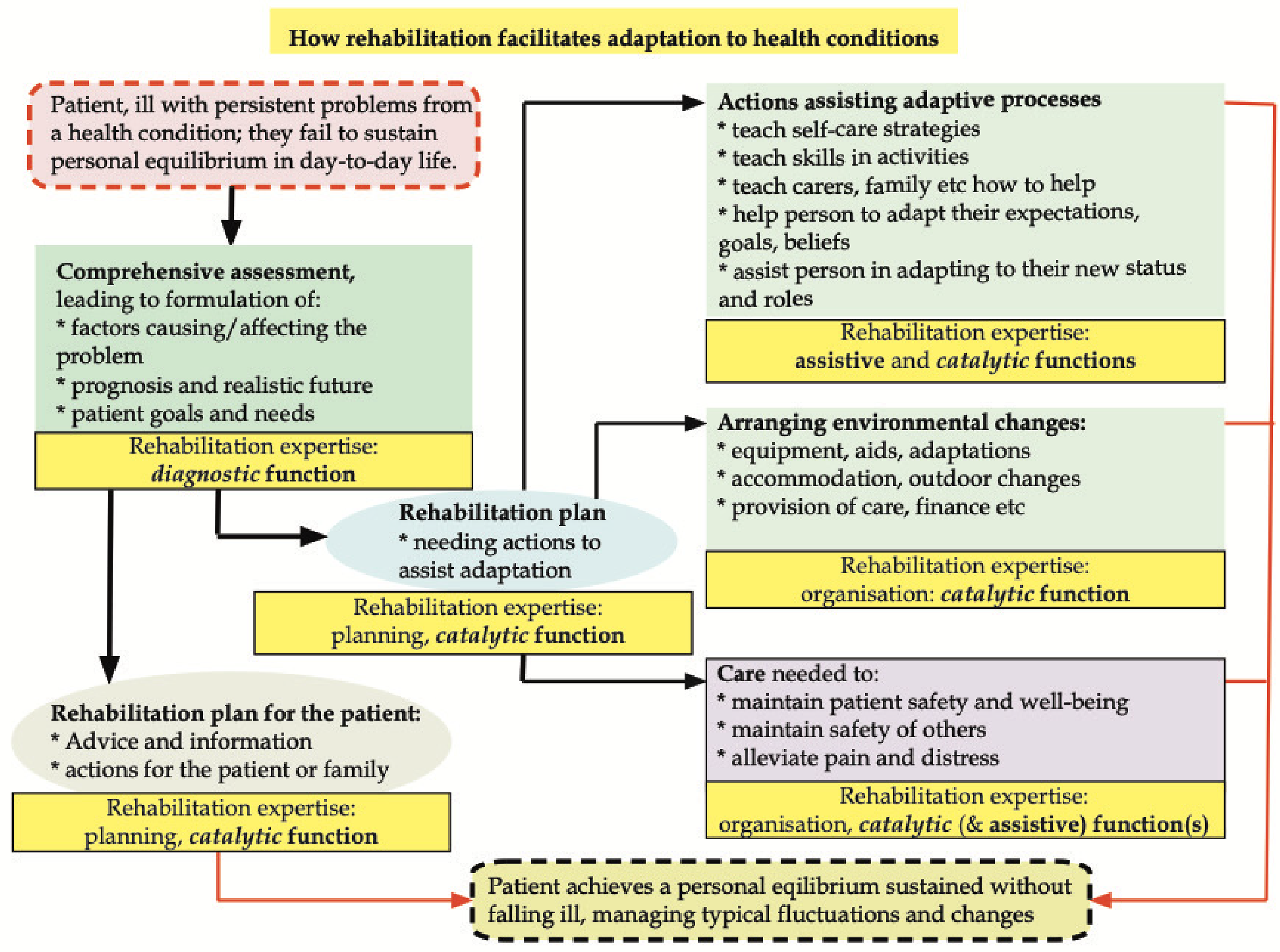
How rehabilitation facilitates adaptation to health conditions.
Discussion
The paper combines three theories into a single general theory of rehabilitation centred on adaptation: It reframes rehabilitation as a systematic series of assistive and catalytic interventions guiding the natural adaptation process, enabling the person to achieve and maintain their psychosocial equilibrium against set points in each domain of need.
From passive to active
This theory makes the patient the central, active agent in rehabilitation, not the passive recipient presupposed in biomedical healthcare.
The theory requires services to be person-centred, 44 often proclaimed but not well practised, 64 because, when adapting, the person explores and learns new ways to achieve their goals. The person must be an active learner engaged in the process.65,66 Because the patient is seeking expertise rather than the professional giving it, power transfers from the professionals to the patient, which is challenging for some professionals. An active patient naturally undertakes self-management. 7
Acknowledging the person's active role in rehabilitation should encourage the following:
more research into and resources for teaching life-long self-management, professionals and organisations to relinquish some control, organisations to become person-centred.
The environment
The vital role of the environment in learning and adaptation was demonstrated by Hubel and Wiesel, who discovered the catastrophic effect of absent early visual input on the development of vision. 67 Conversely, an enriched environment after stroke can lead to structural and behavioural benefits in mice. 68
The importance of a rehabilitative (or adaptive) environment for people after a stroke is apparent: ‘People with stroke who receive organised inpatient (stroke unit) care are more likely to be alive, living at home, and independent in looking after themselves one year after their stroke’.
18
The broad nature of the facilitative environment is illustrated by the essential features of stroke unit care:69,70
Structured assessment procedures Policies on early stages of management of common problems Policy on the ongoing rehabilitation Expertise in stroke management and rehabilitation with regular team education Multidisciplinary teamwork with regular planned team meetings Involvement of patients and families Planned changes in the physical environment alter the behaviour of patients, increasing their activities.71–74 Social factors influence adaptation; for example, after a stroke, community activity is influenced by social networks
75
and being with other people is associated with more movement of the affected arm.
76
Other studies have shown that:
The harm caused by inappropriate environments is also clear. In a hospital, adaptation is prevented by physical constraints, such as beds that are difficult to get out of, a cluttered, noisy environment, and, more powerfully, by cultural and organisational factors, such as risk avoidance and an expectation of delivering care rather than encouraging independence. Inactivity leads to dependence upon carers, loss of confidence, self-esteem, and muscle bulk.77–79
This theory emphasises the crucial need for all healthcare environments to facilitate adaptation after acute loss and maintenance of skills when admitted with any disability. Moreover, it highlights the risk of a poor, unenriched environment, with patients missing the opportunity to recover through loss of confidence, muscle wasting, or becoming psychologically dependent on care.
It should encourage research into improving all healthcare environments, primarily physical and cultural aspects of hospital environments, to facilitate adaptation to illness and prevent loss of skills and abilities.
Resetting psychosocial equilibrium set points
People with marked changes in their capabilities may need to reset their psychological, social or self-fulfilment set points to achieve psychosocial equilibrium. 37
Research has described coping strategies associated with long-term disabling conditions and suggests therapies, such as increasing a person's empowerment or self-management skills and using peer support. Goal adjustment has been described in people with long-term conditions, 80 including cancers. 81
This theory suggests research is needed to assist people to adapt their long-term aspirations, accounting for their altered abilities. I have yet to find significant studies on how and when to help patients adjust their goals.
Rehabilitation services
Adaptation is a continuous process, active from the outset. It is not limited to therapy sessions or any phase of an illness. The general theory of rehabilitation highlights the central role of assessment, formulation and planning in giving advice and suggesting specific interventions. Consequently, expert rehabilitation input must be available in all healthcare settings, especially in acute hospital inpatient settings, including intensive care. Rehabilitation should supplement biomedical healthcare as a parallel service.
The continuous nature of adaptation also means there should be no boundaries between the many services a person needs. Not all are health services, but there should be no barriers between them.
The solution is to ‘establish a local provider rehabilitation network to include primary, secondary, tertiary health care, mental health, social care, independent and third sector providers’.82,83 The crucial common feature linking rehabilitation services is assisting adaptation.
The theory suggests research into how rehabilitation services can form effective networks might significantly improve the use of resources.
Normality and health
Many professionals and patients strive for normality. Georges Canguilhem showed that defining normal is impossible. 84 Normal is particularly misused in rehabilitation. 85 Some rehabilitation professionals and some relatives want the patient to achieve the performance of tasks normally, especially without using ‘compensatory’ movements. 86
Compensatory movements are usually appropriate adaptive movements, which may be best for a patient.87,88 Children with congenital disorders such as phocomelia, cerebral palsy or cleft palate will adapt naturally as they grow; their way of undertaking activities is the best way for them. People with slowly progressive conditions such as muscular dystrophy, Huntington's disease or inflammatory arthritis often adapt without assistance.
Two books by a philosopher with a long-term lung condition, Havi Carel, have explored the concept of health in people with disabling conditions.89,90 In the first, Illness, she refers to ‘… the ability to adapt to new, more limited capacities and the creativity that emerges …’. She prefers the word adaptability to ‘… refer to the behavioural flexibility of ill or disabled people adjusting their behaviour in response to their condition’. She thinks that these approaches enable someone to be healthy within an illness. 89
In her second, Phenomenology of Illness, she notes that many people with even quite severe limitations are as happy and report their sense of well-being at similar levels to people considered to be healthy. She says, ‘Rather, cultivating well-being within illness and learning to live well with physical and mental constraints requires effort and is an achievement …’. 90
The General Theory of Rehabilitation suggests that a person could be considered healthy when they have regained the capacity to maintain physiological and psychosocial balance in the face of typical changes in their circumstances and can focus on their self-fulfilment goals.
Rehabilitation: Roles and resources
This theory focuses rehabilitation on achieving the best adaptation possible. Consequently, recovery from tissue damage is not essential, a return to a previous state is not expected, and adaptation occurs at any stage of life or an illness. Adaptation will be judged by social integration.
The various roles of expert rehabilitation are illustrated in Figure 4: diagnosis, planning, catalysis (including organisation), and assistance. Note that the provision of care is not a direct rehabilitation responsibility.
The crucial first step is a diagnostic assessment, such as a comprehensive geriatric assessment 91 or a person-centred rehabilitation assessment. 46 The theory suggests that a formulation based on the biopsychosocial model of illness can lead to well-informed advice and well-targeted actions while avoiding wasteful activities. We can only select who will benefit from sound advice and guidance once they are seen. 92
Some patients will need environmental changes. The rehabilitation service will need to assess what equipment, ensure it is suitable, and teach patients and carers how to use it. The equipment is essential for successful adaptation; this extends to altering living accommodations and the wider environment. These costs are not rehabilitation costs but societal costs associated with helping a person adapt.
Most patients will need advice on problem-solving and on what and how to learn. Learning goals are effective at achieving change. 93 Many patients require only brief, specific expert rehabilitation input. A few patients with severe or complex losses or difficulty in learning and adapting will need significant, sometimes substantial, ongoing input. This will typically focus on learning skills where the risk or the need for active feedback requires an expert to help.
Thus, people based in specialist inpatient rehabilitation units must not be concerned that their work is undervalued, nor should commissioners consider they are paying for unnecessary high-cost services. Further, the costs of care, which may be great, arise wherever the patient is; they are not a rehabilitation cost, though rehabilitation services may have to provide care.
Evaluation of the theory
I will evaluate this hypothesis against the criteria of a good theory. 17
This paper has suggested some testable changes in rehabilitation that, if found effective, will validate it. They include:
Discussing and assisting with goal adjustment. Increasing emphasis on teaching self-management. Educating patients, carers, and professionals that rehabilitation is usually a facilitating and catalytic service, not a dose-dependent assistive service. Using teams with more expertise in the initial analysis, formulation, and planning is likely more effective than teams with less expertise. Developing cross-agency and cross-organisation networks to increase collaboration and cooperation between the many services involved.
It is coherent, combining ideas and theories consistent with the central hypothesis.
It is economical, building on three ideas:
People adapt to illness. An advisory, educational expert service can guide and facilitate adaptation. Rehabilitation's goal is to facilitate a person in achieving equilibrium between the social, psychological, and self-fulfilment aspects of their life.
It is broadly applicable, encompassing all areas of healthcare rehabilitation in people of all ages and with all types of illness.
It has considerable explanatory power:
Rehabilitation acts on the adaptive process, not the person. This explains its effectiveness across almost all conditions, regardless of prognosis, age, duration, and the underlying condition, Catalysts alter the ease of a process and do so at minimal levels. This explains how low doses of rehabilitation input may have a detectable effect and why it is difficult to find an apparent dose–response relationship, Natural recovery is adaptation without input from a recognised expert rehabilitation team. This explanation recognises that adaptation includes seeking and receiving help from others. No rehabilitation refers to the absence of expert rehabilitation services’ assessment, advice, and interventions. Adaptation may involve every domain of life and many organisations. This explains why a healthcare service undertaking the catalytic process must draw on help from almost anyone, a marked contrast to biomedical healthcare.
Last, this theory explains one otherwise startling observation. In 1935, a person with a spinal cord injury could expect to remain physically and socially dependent, with an early death. Now, they can expect a near-normal life span and full social participation. Rehabilitation has transformed lives despite the lack of any recovery in motor control or sensory function. Rehabilitation services were developed to assist adaptation, focusing on social integration, teaching patients how to care for themselves, providing and teaching them to use equipment, and advocating for society to adapt to their needs.
Weaknesses
This theory has weaknesses. It is untested. It gives an overview and can suggest ways to improve rehabilitation, but it does not provide details on how those improvements can be undertaken. It does not tell the professional faced by a patient what to do.
On the other hand, it is a development of ideas that have been around for many years, and it tells the person facing a patient how they should think about the situation. It sets out a general framework, comparable to the biopsychosocial framework, that encompasses many more detailed theories and places them in a greater context.
Finally, a theory is neither right nor wrong; its influence must judge it. A theory that improves understanding and promotes new or better ways of helping patients is an advance on earlier ideas. This theory should be tested by use. I expect it will be improved, particularly by increasing details; it may eventually be replaced.
Clinical messages
Rehabilitation facilitates a person's adaptation to their illness.
Its central role is as a catalyst, formulating a rehabilitation plan.
Its other leading role is to help a person learn new skills, especially in self-management;
It provides direct assistance in learning and practising activities for patients with complex or severe losses.
Footnotes
Acknowledgments
I am incredibly grateful to Professor Stefano Negrini for his excellent, insightful criticism of my initial submission, which was a poor paper; he gave invaluable feedback and advice. The article is vastly improved. I also thank Professor Diane Playford for asking me to give a talk on “recovery and rehabilitation,” which led to this idea, and the many people who have asked me what rehabilitation does. I have at last discovered!
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.