
Abstract
Objective
To explore the extent and type of evidence in relation to group-based cardiac telerehabilitation interventions and health outcomes in coronary artery disease patients.
Data sources
A literature search was conducted in August 2022 and July 2023 in databases including PubMed, CINAHL, Scopus and PsycINFO. The search process followed the scoping review methodology guided by the Joanna Briggs Institute for scoping reviews.
Methods
The inclusion criteria were a peer-reviewed journal article published in English between 1 January 2017 and 15 August 2022 and updated to cover until 15 July 2023 concerning group-based cardiac telerehabilitation in adult coronary artery disease patients. All group-based cardiac telerehabilitation interventions and health outcome types were charted and summarized.
Results
The researcher screened a total of 2089 articles, of which 22 were retained with a total of 1596 participants. Group-based cardiac telerehabilitation interventions were particularly useful for patients with multi-faceted technological applications and social support. The patients received guidance regarding cardiovascular disease risk factors. Physical fitness, psychological complaints and quality of life were often measured outcomes in the included studies.
Conclusions
This scoping review indicates the success of various rehabilitation interventions utilizing different technologies for coronary patients. Coronary patients were guided in making lifestyle changes, and positive findings were observed in the health outcomes measured after the telerehabilitation intervention. The findings of this review can provide valuable guidance for developing and evaluating sustainable group-based cardiac telerehabilitation programs that aim to benefit coronary patients.
Introduction
Coronary artery disease causes the most morbidity and deaths in the world.1,2 After an acute cardiac event, the prevention of new cardiac events is essential and reduces suffering. 3 This secondary prevention includes the methods used to prevent the progression of coronary disease in a patient who is already ill. 4 Evidence-based prevention includes medication optimization, risk factor management and lifestyle changes.5,6 The recommendation for cardiac rehabilitation spread to different countries, putting emphasis on the provision of rehabilitation guidance and secondary prevention in the treatment process of cardiac patients. 7 Telerehabilitation is the purposeful use of applications that utilize digital technology in rehabilitation. 8 Rehabilitation groups serve various purposes, such as educating patients, practicing skills and strategies, and providing opportunities for peer support. 9
The goal of rehabilitation is disease management 10 which means the improvement of the patient's physical, psychological, social and overall life situation by means of rehabilitation. Death statistics have traditionally been used as outcome variables, 11 but more recently, changes in risk factors and quality of life have also been included as outcome variables. 10 While the effects of telerehabilitation interventions on cardiac patients have been studied earlier,12–14 there is still a lack of a comprehensive overview of interventions and the different outcomes of telerehabilitation groups. The findings of this review are expected to provide a broad view of evidence-based information available on group-based cardiac telerehabilitation. The aim of this scoping review was to explore the extent and type of evidence related to group-based cardiac telerehabilitation interventions and health outcomes in coronary artery disease patients. The research questions that guided this scoping review were: (1) What kinds of group-based cardiac telerehabilitation interventions have been used in coronary patients? and (2) What health outcome types have been identified in coronary patients participating in group-based cardiac telerehabilitation interventions?
Methods
We used a scoping review methodology recommended by the Joanna Briggs Institute scoping reviews. 15 This involved carrying out five steps for scoping reviews. 16 The identification of the research question (step 1) was presented in the introduction. The identification of potential studies, inclusion/exclusion review and data charting (steps 2–4) are summarized in this section. This is followed by findings/recommendations (step 5) presented in the results and discussion section.
The inclusion criteria applied to the database search were defined according to the aim of the review and the review questions. A literature search was conducted in August 2022 and updated in July 2023 in the PubMed, CINAHL, Scopus, and PsycINFO databases. The authors developed a valid research strategy and comprehensive list of search terms in consultation with a university librarian. The databases were thoroughly searched for topics relevant to group-based cardiac telerehabilitation using the following general terms: “cardiac,” “coronary,” “cardiovascular,” “rehabilitation,” “virtual,” “mobile,” “mobile apps,” “smartphone,” “telenursing,” “telemedicine,” and “ehealth.” The limits applied to the database search were publication in English and studies published from 1 January 2017 to 15 August 2022 and, in the updated search, from 1 August 2022 to 15 July 2023 (Supplemental Material Table 1). This yielded 2089 articles retrieved from the data sources described previously.
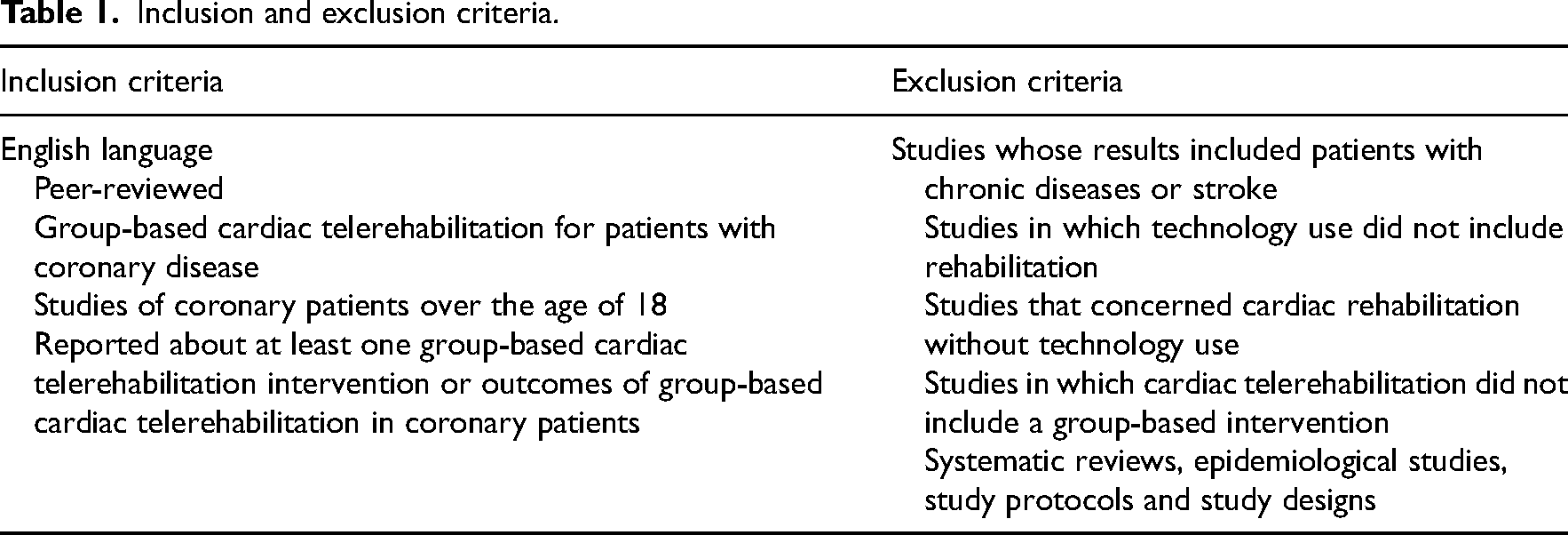
The selection criteria were defined according to the inclusion criteria which followed the Joanna Briggs Institute Manual and the PCC model, wherein P stands for population, C for concept and C for context. 15 In this review, the population of interest comprises studies concerning coronary patients aged over 18 years in rehabilitation groups. The concepts examined in this review are group-based cardiac telerehabilitation interventions and health outcomes. Group-based cardiac telerehabilitation interventions are programs used to increase participants’ levels of self-care, potentially improving their lifestyles. Group-based cardiac telerehabilitation refers to e-technology (telephone, mobile phone, computer, tablet computer and wearables) and includes the use of applications, providing real-time/asynchronous feedback as well as systems that facilitate remote communication with healthcare professionals and their support. 11 The context examined in this review involves remote/digital environments in any healthcare setting where cardiac rehabilitation is provided. The present review includes qualitative, quantitative and mixed-method studies and full-text empirical articles with an abstract available. Systematic reviews, epidemiological studies, and study protocols/designs were excluded (Table 1).
Inclusion and exclusion criteria.
The review followed the PRISMA-ScR (preferred reporting items for systematic reviews and meta-analyses for scoping reviews) guidelines. 17 The database search identified a total of 2089 documents. After removing duplicates, two authors (RJJ and JK) independently screened 1475 articles identified in the literature search based on their titles/abstracts. This was followed by a full-text assessment of 44 articles, which involved assessing each article regarding whether it fulfilled the inclusion or exclusion criteria. Those articles that met the inclusion criteria were selected for inclusion in the study. Any disagreements were discussed between the two researchers (RJJ and JK) or a third researcher was consulted (AO) until a consensus was reached. The final selection of relevant articles comprised 22 articles (Supplemental Material Figure 1). A data charting table was developed by the author. 1 Information was recorded as follows: author(s), year of publication, study location, study population and sample, aim, method, intervention type, intervention setting, outcome measures, follow-up time, and health outcome(s) (Appendix 1). Covidence® software was used for screening and data extraction.
Results
Characteristics of the studies
A total of N = 22 articles were included in this review.18–39 The studies varied in research designs, including 11 randomized controlled trials,18–20,23,26,27,30–33,35 five pilot studies,21,24,25,28,36 two observational studies,29,34 one case study, 22 one qualitative study, 37 one mixed-method study, 38 and one cross-sectional study. 39 The studies had been conducted in different locations: 11 of them in Europe,18–20,22,28,31,33–36,39 six in Asia,23,24,29,30,32,37 three in Australia,25–27 and two in North America.21,38 The target population of 21 of the studies was coronary artery disease patients with heart failure and in one study coronary artery disease patients and the patients’ partners. 22 All patients participated in the studies after percutaneous coronary revascularization or coronary artery bypass graft. The study samples ranged from 8 21 to 335 29 coronary artery disease patients.
Intervention types
The participants took part in education sessions delivered by expert health professionals. In the 22 studies, the health professionals were mostly nurses22,30–32,34,37–39 and physiotherapists,20,26,27,30,35,39 and a minority were cardiologists and doctors,20,26,27 clinicians, 26 cardiovascular disease specialists, dietitians or technical staff.21,34,35,38 Out of the 22 studies, 19 described technology-based coaching and feedback provided by healthcare professionals.18,21,23–35,37–39 In the most recently published studies, motivational messages and feedback had been included and were produced by technology by coding these to the used electronic platform.32,35,37 Only six of the studies clearly described group interactions and social support interactions.22,24,26,30,35,38
The duration of the cardiac telerehabilitation interventions ranged from 6 weeks 32 to 12 weeks.18,19,21,22,33 A minority of the studies described the process of developing intervention content. The behavioral theory had been used in two of the studies,25,31 learning theory in one study, 22 and the chronic disease model in one study. 27 Many interventions were delivered in a healthcare setting and tracked remotely. The patients participated in the interventions in their homes, receiving a home-based exercise intervention with telemonitoring guidance.18,20,24,28–31,33 Telerehabilitation was particularly useful when patients were not able to access clinical facilities 29 or were motivated by the easy access and reduced travel time enabled by the solutions.24,27
In all the studies, the interventions were computer- or tablet-based. Patients participating in the group-based cardiac telerehabilitation were required to have their own, relevant technological equipment with Internet access (computer, telephone, and mobile connection).18–39 A variety of other devices and applications were also used in the included studies (Supplemental Material Table 3). Out of the 22 studies, a chat feature was primarily utilized as a means of delivering the intervention in 15 studies,21,22,24–27,29–32,34,35,37–39 telemonitoring,18,20,24,28–30,32–37,39 and a virtual platform21–25,28,30–32,34,35,37–39 were used in 14 studies, other mobile connections in 12 studies18,19,23,24,28,29,33–37,39 and video conferencing in nine studies.21,24,26,27,30,34,36,38,39 Using video conferencing at patients’ homes enabled clinicians to observe the participants, provide them with feedback and facilitate peer-support,24,27,38 and this method was used for an exercise and education intervention delivered by healthcare professionals.25–27
Of the 22 studies, five involved physical exercise testing performed using remote telemonitoring devices (e.g. smart watch, digital step counter, blood pressure monitor, and fitness tracker).18,19,34,35,39 Of the 22 studies, four utilized remote patient heart rate monitoring.18,26,33,39 Most of the studies included some elements of self-management resources. These elements aimed to boost behavioral risk factor management in coronary artery disease patients. 25 The behaviors mainly included physical activity and diet.21,25,34,38,39 Only a minority of studies addressed or described risk factors related to smoking or hypertension management20,32,34,37 or other issues most relevant to cardiac rehabilitation (sexuality and heart disease, heart medications). 21 In 11 of the 22 studies, the intervention participants were encouraged to set goals and take action to modify their behavioral risk factors focused on healthy lifestyle changes.18,20,23,25,26,31,32,34,35,37–39 In two of the 22 studies, returning to work had been set as the goal.25,35 Online platforms were used to empower patients to make progress toward their goal34,37,39 and aimed at supporting patients in planning their coping. 21
The used chat feature was commonly text-based and synchronous, using two-way audio–visual communication that enabled interactions between all parties. 26 Many cardiac rehabilitation participants enjoyed the group interactions and social support enabled by such solutions. 26 Participants shared their experiences and pursued their goals together in an online group. 32 Elderly patients were conservative about using online communication. 24 Patients were encouraged to post their questions on the forum to get responses from the nurse and their peers. 32 Healthcare staff also contacted individual participants if a need to discuss their progress was detected. 31 Four studies described the use of telecommunication specifically for the purpose of guiding the participants on how to use technology in rehabilitation. This included activities such as sharing instructional information and operating technical devices.19,21,31,35
Measured health outcome types
In this context, health outcome types refer to changes in the coronary artery patients’ health status and to patient-reported outcomes. Health outcomes were collected at baseline in all the studies as well as at post-intervention measurement points from 6 weeks 32 to 4 33 years after the intervention (Table 2). Out of the 22 studies, the health outcome measurement point was 6 weeks in five studies20,23–25,30 but in most of the studies, this was set at 12 weeks.18,19,21–23,26,27,29,31,33 In total, 11 studies used longer follow-up times. These included four studies with measurement points set at 6 months,26,27,30,34 five studies with measurement points at 1 year,18,19,29,31,33 one study with a measurement point at 2 years 29 and one study at 4 years. 33
Summary of the health outcomes of the group-based cardiac telerehabilitation interventions in the included studies.
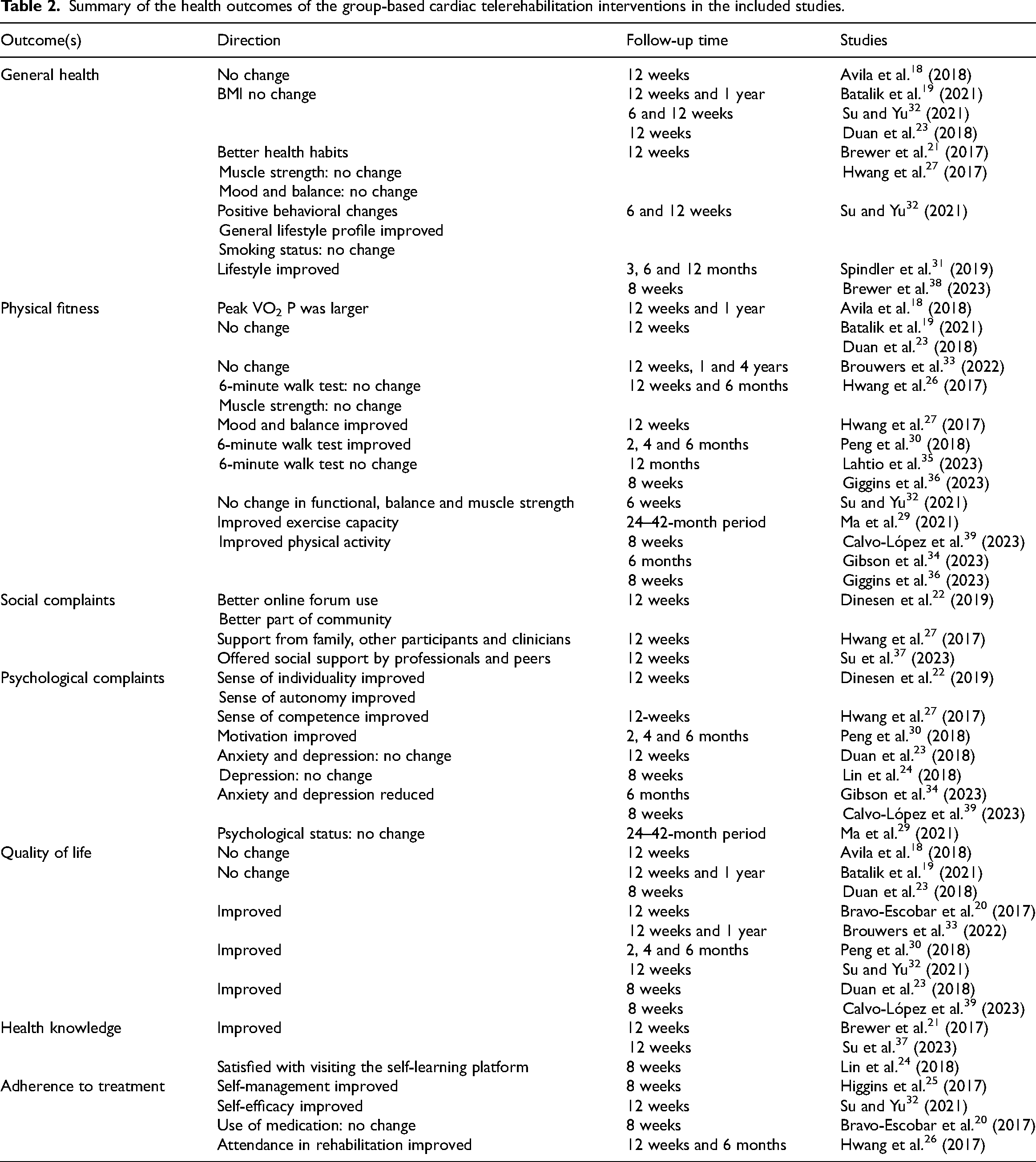
Common strategies used to promote a healthy lifestyle included promoting behavioral changes.21,23,32,34,38,39 Among those with a healthy lifestyle at the start of the intervention, all the patients in the cardiac telerehabilitation group continued to maintain their healthy lifestyle throughout the treatment. 23 Early recovery prior to the return to work increased motivation for change and supported sustaining long-term self-management. 25 The return to work and its significance were not measured in other studies. In 22 of the studies, nine measured traditional risk factors and showed no significant differences in anthropometric characteristics or traditional cardiovascular risk factors,18,19,23,29,32,35,36,38,39 although clinically relevant trends were noted in some studies.38,39 Several studies describe that patients have many risk factors. 38 In one study, the majority were smokers, and about half of the participants reached the targeted blood pressure. 29 One study reported improvement in diet, 34 but most of the studies reported no significant improvements in the patients’ dietary or smoking status. 32 Body mass index associated with risk factors was calculated using the formula BMI = weight/height in five of the 22 studies. After a 6–12-week period19,23,32,34,36 and a 1-year follow-up, 19 the participants’ BMIs continued to be similar. Only one study showed reductions in mean weight in a 6-month follow-up. 38 A 42-month follow-up showed better control of risk factors regarding LDL-C and systolic blood pressure. 29 The use of prescription medications was measured in one study. 20
In total, nine studies included physical fitness tests. Physical fitness was tested based on a functional capacity test,27,34–36 oxygen uptake, 18 pVO2,19,33 the number of steps 32 and a 6-minute walk test.27,30,35 In total, in eight of the nine studies, the participants’ physical fitness increased. Oxygen uptake at the first and second ventilatory thresholds increased more in the 12-week follow-up. 18 Functional exercise capacity increased 4 months after the post-test in an 8-week cardiac telerehabilitation program. 30 The average peak of pVO2 was higher after 1-year follow-up. 19 One study showed improvement in the number of steps per day. 32 Muscle strength, mood and balance were improved. 27 After 1-year follow-up, a cardiac telerehabilitation had improved the participants’ physical activity, but a long-term follow-up 4-years after the cardiac telerehabilitation showed that the intervention had not prevented a relapse in physical activity. 33 However, it conveys that in all the studies analyzed, there was no association or correlation found between telerehabilitation and improvement in physical activity.27,32,33
Social complaints were measured in a total of four studies. Group-based cardiac telerehabilitation improved social support when patients received support from healthcare professionals20,22,27,37 and peer support from other participants.22,25,27,37 Healthcare workers coached patients to return to their everyday lives. 22 Support from family was improved during cardiac telerehabilitation, with participants spending more time with their families and carrying out the same exercises. 26 Opportunities to interact with other cardiac patients online were clearly desired by patients. The rehabilitation programs provided emotional support through shared experiences.20,25 The online sessions promoted group cohesion and a sense of universality. The participants acknowledged that they were communicating with real people, which shortened the psychological distance between group members despite their physical distance. 24
Psychological complaints were measured in 11 of the 22 studies.22,23,25,27,31–34,37–39 Anxiety and depression were measured in six studies, and most of them found no differences in the scores for anxiety and depression23,24,29,30,34,38 except one study. 34 The participants’ sense of individuality, autonomy, capability and motivation improved. 22 In one study, improvement was only found in subscales between the 1- and 4-year follow-up in the control group but not in the telerehabilitation intervention group. 33 An initial increase was observed in autonomous motivation but this positive change in motivation did not last over time. 31 High motivation to use the self-learning platform and participate in video conferences indicated that a group-based cardiac telerehabilitation program is feasible and acceptable for the psychosocial rehabilitation of patients with coronary artery disease.24,37
In total, seven of the 22 studies measured health-related quality of life. None of these studies found significant differences in the quality of life between control and intervention groups.18,19,23,30–32,35 Quality of life seems to improve over time in a 4-month to 1-year follow-up.30,32 Apparently, an exercise training program improved participants’ quality of life after the start of the cardiac telerehabilitation. 30
In total, five of the 22 studies included a health knowledge measurement.21,25,31,37,38 In one study, most of the participants reported that the program had improved their health knowledge and helped them maintain better health habits. 21 The patients believed that the online cardiac rehabilitation program would be more appropriate for patients with lower health literacy than those participating in the rehabilitation. 25 While satisfaction with the rehabilitation was measured in the studies, health knowledge improvement was not measured in connection with rehabilitation. 24
Only three of the 22 studies measured self-management and self-efficacy.25,32,37 A 12-week empowerment-based telerehabilitation program was found to improve patients’ self-efficacy and was seen to support self-management in patients ready and willing to implement it. 32 Self-efficacy emerged as an increased activity in carrying out lifestyle changes and coping plans.25,35 A total of two studies measured motivation.24,27 The participants were highly motivated and satisfied with using the self-learning platform and the video conference feature. 24 Improved motivation influenced health outcomes and access to care. 27
Discussion
The aim of this scoping review was to examine the different types of interventions and health outcomes targeted at coronary patients. This review may clarify definitions and provide contextual information on telerehabilitation phenomena. To our knowledge, this is the first scoping review of group-based cardiac telerehabilitation. Most of the earlier studies focus on individual telerehabilitation without a group-based context.
There is limited literature describing the use of group-based chats or video conferencing as a part of cardiac rehabilitation. Most interventions included online meetings between groups and healthcare professionals and these meetings enabled support and communication. The most recent studies showed an increase in technology-based motivational messages in addition to interpersonal communication. Using artificial intelligence-based communication for support has not been studied much in the context of rehabilitation, and there is no clear evidence regarding the current understanding of patients’ views and preparedness to use artificial intelligence in their practices. 40 A positive finding in this study is the support and guidance provided by healthcare professionals to patients. Although physiotherapists and nurses play a significant role and accompany patients during rehabilitation, this aspect was not clearly described in the studies. The role of cardiac nurses is very important in overall cardiac rehabilitation leading to an improvement in the patient's well-being and recovery. 41 In the future, the role of nurses in interventions should be described in greater depth and with more precision. Our findings support the assumption that group-based social support can be used in rehabilitation groups to provide opportunities for peer support 9 ; indeed, geographically isolated patients were found to benefit the most from the communication included in the rehabilitation. 24 Telemedicine was particularly useful when patients were unable to access clinic facilities 29 or were motivated by easy access and reduced travel time.24,27
This scoping review demonstrated that the interventions utilized different digital tools and platforms. Various applications and digital devices were used significantly differently throughout the interventions. We suggest that telerehabilitation interventions can be implemented with a wide variety of devices and communication applications. The elderly population exhibited reduced levels of participation in communication. 24 This finding was in line with previous studies on telerehabilitation, which observed challenges related to the use of technology, especially among older users. 42 To conclude, the digital devices available to elderly coronary patients and their knowledge of using them need to be reviewed. As a result, there is a clear demand for further investigation of telerehabilitation programs targeted at elderly coronary patients. In the future, it would be relevant to investigate clear instructions for patient-friendly and patient-centered digital and communication tools, and standardized remote methods are essential for clinical practice.
Long-term outcomes were not addressed in the included studies, which typically contained follow-up times of 6, 8 and 12 weeks. This was also identified by a previous review on telerehabilitation, in which the included studies did not address any long-term outcomes. 42 Further studies will provide insight into the long-term impacts of group-based cardiac telerehabilitation. The studies did not measure the most useful time to start rehabilitation after a cardiac event. This is significant to internal psychological resources (high intention and good self-regulation capability) as a central variable and should especially be considered in health promotion aimed at cardiac patients. 23
In this review, we were primarily interested in the types of interventions and outcomes reported in the studies. The achieved outcomes and results showed improvement in patients’ general health, physical capacity, psychological well-being, quality of life and self-effectiveness. A personalized approach to risk stratification and invasive procedures combined with optimal medical therapy improved finding an effective solution for the prevention of new cardiac events in the patients. 3 Patients had an interest in optimizing their medication, and while this was a topic of guidance and education, its effect was not measured in the included studies. As a result, future research should pay attention to adherence to medication. Smoking cessation, as an outcome variable, was also almost absent in the studies. 32 However, smoking cessation is recommended as an important goal in cardiac rehabilitation because smoking is a modifiable risk factor that should be pursued in every secondary cardiac rehabilitation program. International and European guidelines recommend that coronary artery disease patients should be encouraged to stop smoking permanently. 13 In the future, it would be relevant to investigate how to support patients in smoking cessation and what methods can be used in technology-based rehabilitation.
Sample sizes in the included studies were small; in most of the studies, the sample comprised less than 50 patients. In most of the studies, all patients had been recruited from a single clinic. Based on the recommendation for normally distributed outcomes, the relative gain in precision of the pooled standard deviation (SDp) is less than 10% with a total sample size of 70 and 5% with a pilot sample size of 60. If the event rate in an intervention group needs to be estimated by a pilot, a total of 60–100 patients is required in the pilot trial, and for a primary outcome, a total of at least 120 subjects (60 in each group) may be required. 43 More reliable and significant results will be obtained in the future when larger sample sizes are used.
Most of the included studies were from Europe and Asia, and several of them were from Australia. Only one of the European studies was from the Nordic countries, 35 even though the prevalence of heart disease is high in the Nordic countries. Most of the European coronary patients have a less than optimal management of LDL-C and lifestyle changes are needed.5,44 In a previous study, it was discovered that the majority of coronary patients did not have their blood pressure, low-density lipoprotein cholesterol and glucose targets under control. 44 Cardiovascular disorders are largely preventable, which provides grounds for optimism that the spread of favorable mortality trends in the high-income countries of Western Europe will continue, as inequalities in prevention and treatment are diminishing. 45 Our review demonstrates that providing groups with remote support through technology can lead to positive lifestyle changes among coronary patients. Results from the European Society of Cardiology EUROASPIRE V registry indicate that cardiovascular prevention requires introducing a modern preventive cardiology program delivered by interdisciplinary teams of healthcare professionals addressing all aspects of lifestyle and risk factor management to reduce the risk of recurrent cardiovascular events. 44 For this reason, this scoping review showed that the included interventions likely resulted in improvements in the quality of life, physical activity and psychological well-being of coronary patients. However, while the patients received guidance in controlling risk factors, the risk factors were not sufficiently and comprehensively measured at the follow-ups.
This scoping review highlights the success of various rehabilitation interventions utilizing different technologies for coronary patients. The coronary artery disease patients were guided and supported in making lifestyle changes, but changes in cardiovascular disease risk factors, lifestyle or medication were often not measured in the included studies. The conclusion is that there is a need for a comprehensive assessment of the outcomes of the intervention on a full range of secondary prevention measures such as cardiovascular disease risk factor modifications, psychosocial complaints, adherence to treatment, rehospitalizations and adherence to medication along with lifestyle changes. Group-based cardiac telerehabilitation should be delivered by multidisciplinary teams addressing all relevant aspects and the means of managing risk factors to reduce the risk of recurrent cardiovascular events. Telerehabilitation should be promoted by health policy and healthcare management due to its potential for reducing inequality. By enabling participation in rehabilitation whatever their clinical facilities and regardless of geographical distance, telerehabilitation can help bridge the gap in healthcare access and promote equity among patients. In clinical practice, technological tools can be harnessed to guide, monitor and actively involve patients in their treatment process. In the future, it is suggested that interventions should be designed to promote long-term adherence to healthy lifestyles and sustainable changes in coronary patients.
Based on the results, it can be suggested that nurses and other healthcare professionals can effectively utilize group-based telerehabilitation models to assist cardiac patients in establishing and achieving healthier lifestyles. Group-based cardiac telerehabilitation enables peer support from other participants, group interaction and social support. Different technological interventions can be used in cardiac rehabilitation for patients who are geographically isolated, and clinical facilities for rehabilitation are limited.Clinical messages
Supplemental Material
sj-docx-1-cre-10.1177_02692155231202855 - Supplemental material for Group-based cardiac telerehabilitation interventions and health outcomes in coronary patients: A scoping review
Supplemental material, sj-docx-1-cre-10.1177_02692155231202855 for Group-based cardiac telerehabilitation interventions and health outcomes in coronary patients: A scoping review by Renuka J Jacobsson, Anne Oikarinen, Jenni Krogell and Päivi Kankkunen in Clinical Rehabilitation
Supplemental Material
sj-docx-2-cre-10.1177_02692155231202855 - Supplemental material for Group-based cardiac telerehabilitation interventions and health outcomes in coronary patients: A scoping review
Supplemental material, sj-docx-2-cre-10.1177_02692155231202855 for Group-based cardiac telerehabilitation interventions and health outcomes in coronary patients: A scoping review by Renuka J Jacobsson, Anne Oikarinen, Jenni Krogell and Päivi Kankkunen in Clinical Rehabilitation
Supplemental Material
sj-docx-3-cre-10.1177_02692155231202855 - Supplemental material for Group-based cardiac telerehabilitation interventions and health outcomes in coronary patients: A scoping review
Supplemental material, sj-docx-3-cre-10.1177_02692155231202855 for Group-based cardiac telerehabilitation interventions and health outcomes in coronary patients: A scoping review by Renuka J Jacobsson, Anne Oikarinen, Jenni Krogell and Päivi Kankkunen in Clinical Rehabilitation
Footnotes
Author contributions
RJJ designed and drafted the manuscript; RJJ, JK, and AO screened the studies and assessed the quality of the outcomes; JJ extracted the data; AO and PK provided guidance. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Central Finland Heart Association (grant number 18.4.2023).
Supplemental material
Supplemental material for this article is available online.
Appendix 1
See Table A1.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.