
Abstract
Objective
To describe the development of a goal-directed movement intervention in two medical wards, including recommendations for implementation and evaluation.
Design
Implementation Research.
Setting
Pulmonology and nephrology/gastroenterology wards of the University Medical Centre Utrecht, The Netherlands.
Participants
Seven focus groups were executed including 28 nurses, 7 physical therapists and 15 medical specialists. Patients’ perceptions were repeatedly assessed during the iterative steps of the intervention development.
Intervention
Interventions were targeted to each ward's specific character, following an Intervention Mapping approach using literature and research meetings. Main measures: Intervention components were linked to Behavior Change Techniques and implementation strategies will be selected using the Expert Recommendation Implementing Change tool. Evaluation outcomes like number of patients using the movement intervention will be measured, based on the taxonomy of Proctor.
Results
The developed intervention consists of: insight in patients movement behavior (monitoring & feedback), goal setting (goals & planning) and adjustments to the environment (associations & antecedents). The following implementation strategies are recommended: to conduct educational meetings, prepare & identify champions and audit & provide feedback. To measure service and client outcomes, the mean level of physical activity per ward can be evaluated and the Net Promoter Score can be used.
Conclusion(s)
This study shows the development of a goal-directed movement intervention aligned with the needs of healthcare professionals. This resulted in an intervention consisting of feedback & monitoring of movement behavior, goal setting and adjustments in the environment. Using a step-by-step iterative implementation model to guide development and implementation is recommended.
Introduction
In the Netherlands, annually more than 1.6 million patients are admitted to a hospital. Patients admitted to a hospital spend an average of 55–100% of the time being inactive or in bed.1–4 In-hospital inactivity is associated with an increased length of stay and a decline in daily functioning after hospitalization. 5 Despite knowing the adverse consequences of inactivity, physical activity is still not considered a structural part of hospital care for both patients and healthcare professionals. 6
Multiple studies highlighted the complexity of improving movement behavior during hospital stay and the need for a tailored intervention.4,7,8 Goal setting and self-monitoring have been shown to be important strategies to improve physical activity. 9 Goal setting is effective when the selected goal is challenging but attainable. 10 Interventions using movement sensors during or after an inpatient period have the potential to increase the level of physical activity across a wide range of surgical and nonsurgical populations on nursing wards. 11
Previous research looked into barriers and facilitators of patients' physical activity, from patients' and healthcare professionals' perspective.12,13 They suggested that physical activity is influenced by patients' knowledge, awareness and attitudes. Encouragement from healthcare professionals positively affects physical activity. For healthcare professionals, it is stated to be important that they have clear roles and team collaboration. In general, an attractive ward was found to be motivated to increase physical activity.12,13
The preliminary effectiveness of self-monitoring of patients' physical activity, setting daily movement goals and posters with exercises and walking routes is tested in our pre–post design study. 14 Results showed physical activity increased with 32% after implementation of this intervention. 14 This intervention was accompanied by implementation strategies and evaluation outcomes. These were selected following a planned approach, Intervention Mapping, which might increase the effectiveness and is, therefore, recommended to develop interventions aiming to increase inpatients’ physical activity.15,16
The current study describes the iterative steps toward the GOAL-intervention. The intervention contains a goal-directed movement intervention aimed to improve physical activity in hospitalized patients, including the recommendation for implementation strategies and evaluation outcomes.
Methods
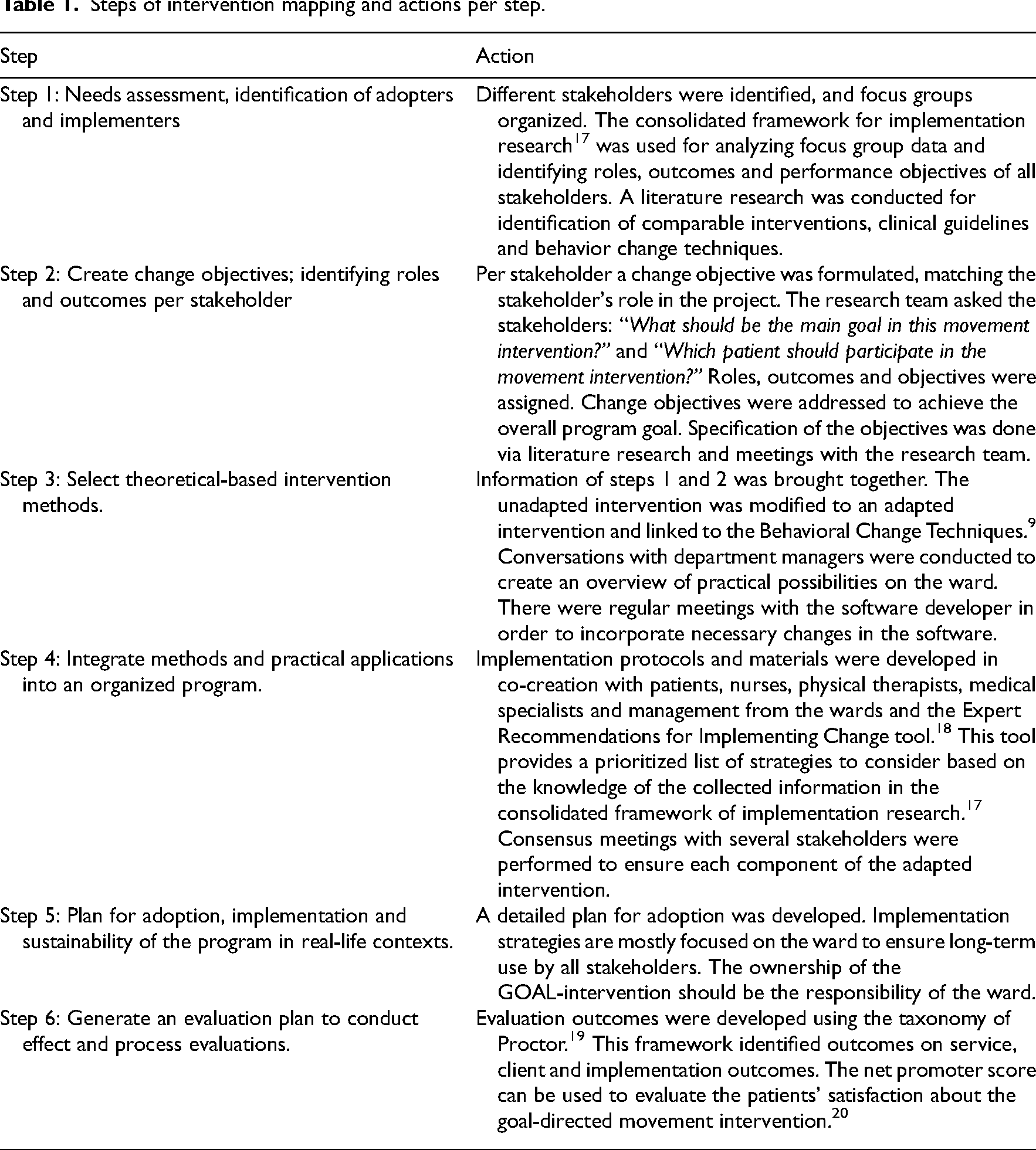
For this implementation research, the intervention mapping approach was used. The intervention mapping approach specifies the six steps used to develop the GOAL-intervention at two nursing wards (pulmonology and nephrology/gastroenterology wards of the University Medical Centre Utrecht (UMC Utrecht)) (see Table 1).
Steps of intervention mapping and actions per step.
The study was performed between February 2022 and January 2023. The study protocol was assessed and approved by the medical ethics committee of the UMC Utrecht (study protocol number 22–537).
Before the start of this study, a movement sensor was used by healthcare professionals working in the surgical oncology ward of the UMC Utrecht; however, it was new to the pulmonology and nephrology/gastroenterology wards. Therefore, we defined the availability of the movement sensor as “the unadapted intervention” according to the consolidated framework of implementation research. 17
To develop the GOAL-intervention the physical activity monitor (PAM) (Pam, Oosterbeek, The Netherlands, version AM400) movement sensor was used. This ankle-worn accelerometer registers physical activity of 1.4 METs or higher, defined as “active minutes.” The concurrent validity of the PAM AM400 was found to be good, demonstrated by a strong level of agreement (ICC = 0.955) with the ActiGraph GT9X Link.21–23
At the UMC Utrecht, physical activity data of the PAM AM400 is visualized in the electronic patient record. Furthermore, healthcare professionals can set movement goals within the electronic patient record. If patients provide permission, their level of physical activity can also be made visible on a public screen on the ward. Additionally, patients can download a mobile application so that they can monitor their own physical activity.
To develop a tailored intervention per ward including the movement sensor, the six steps of intervention mapping were followed and described in this study.
For the needs assessment (step 1 of Table 1), several focus groups were organized. Healthcare professionals were approached to participate in the focus groups by JvG after consultation of a senior nurse at the wards. The focus groups for nurses were planned between shifts, so that most of the nurses could join. Focus groups for physical therapists and medical specialists were conducted as part of scheduled meetings during their shift. Focus groups took place at the ward or physical therapy department and continued until theoretical saturation was reached. One focus group was organized per ward and per profession. Focus groups were directed by PB and JvG, both researchers and physical therapists, to guarantee quality and consistency. An experienced researcher in this topic (PB) led the conversation and JvG was responsible for observations and the informed consent procedure. Due to availability of the researchers, two focus groups were directed by JvG and JN, and JvG and MV. Each focus group was made sure that the leading researcher was not related to the specific ward. During the focus groups participants were encouraged to have in-depth discussions. Hereafter, participants received information on the current ideas and possibilities of the intervention and were asked to discuss the potential to implement in usual care. Participants were asked to share their perspectives on aspects they thought important to the use of the intervention and adjustments needed to implement the intervention on their ward. All focus groups took place face-to-face and were audio- and video-recorded. In addition, characteristics (i.e., age, years of work experience) were collected. We refer to the supplementary materials for the topic guide.
Patients’ opinion is repeatedly assessed during the iterative steps of this intervention development. Patients did not participate in focus groups because of the novelty of the intervention. The intervention was completely new for the included wards at the start of this project, which made it difficult to ask patients’ opinions. Therefore, patients were asked to give their opinion about intervention materials such as flyers and posters and two questions about user-friendliness of the movement sensor. In addition, patients from a different ward were the movement sensor was already used in daily care were asked about their experiences. For the methods of steps 2–6, we refer to Table 1.
Quantitative data such as age, gender and years of work experience are presented as median and range for not normally distributed values. Qualitative data were analyzed using NVivo qualitative data analysis software; QSR International Pty Ltd Version 12, 2018 (Table 1, step 1). All focus groups were transcribed verbatim by JvG. The transcript of the first focus group was analyzed by PB and JvG and codes were selected following thematic analysis. 24 PB and JvG independently identified categories and discussed them in a consensus meeting, JvG analyzed the following transcripts. When all transcripts were analyzed, PB and JvG discussed and checked the categories and themes. A third researcher (KV) was involved to check the final categories and themes to ensure consistency of the outcomes. The final categories were organized in the consolidated framework of implementation research by PB, JvG and KV. 17 This framework provides a menu of constructs arranged across five domains, providing a detailed understanding of the problem. Finally, a member check was carried out. All participants received the transcript of their own focus group via e-mail and were asked if there were any uncertainties and if the transcript was in line with their contribution to the focus groups.
Results
Steps 1–3 describe the conducted steps of the development towards the adapted GOAL-intervention. Steps 4–6 describe recommendations for implementation strategies and an evaluation plan.
Step 1: Needs assessment, identification of adopters and implementers
In total, seven focus groups were executed including 28 nurses, 7 physical therapists and 15 medical specialists. The duration ranged from 22 to 42 min per focus group. Table 2 shows the characteristics of the participants.
Characteristics participants focus groups.
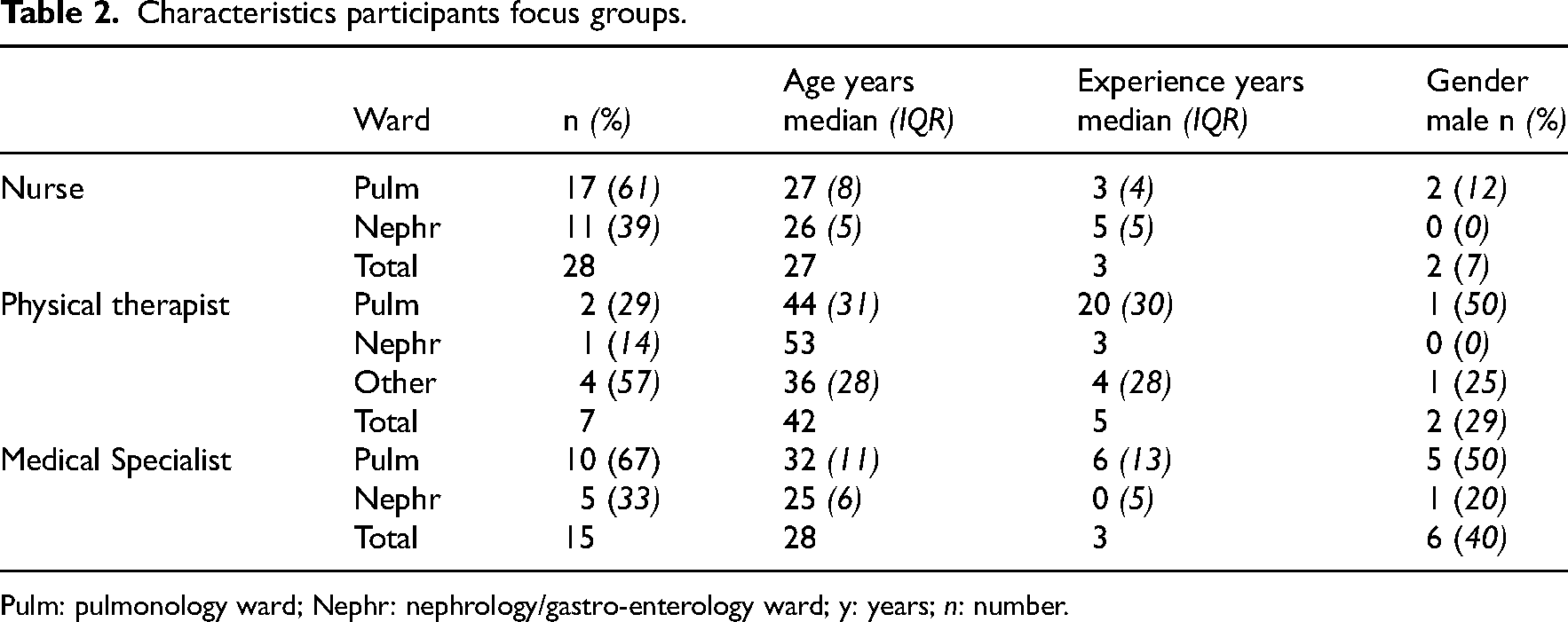
Pulm: pulmonology ward; Nephr: nephrology/gastro-enterology ward; y: years; n: number.
Table 3 gives an overview of the outcomes of the focus groups per construct of the consolidated framework of implementation research. 17 The results of the focus groups show the importance of goal setting and feedback (characteristics of the intervention) and a multidisciplinary approach (inner setting). Healthcare professionals highlighted the role for patients (individuals involved), healthcare professionals and supporting staff from the ward (inner setting) and the importance assigning an implementation champion who disseminates the intervention (implementation process).
Results of the focus groups per construct of the consolidated framework of implementation research.
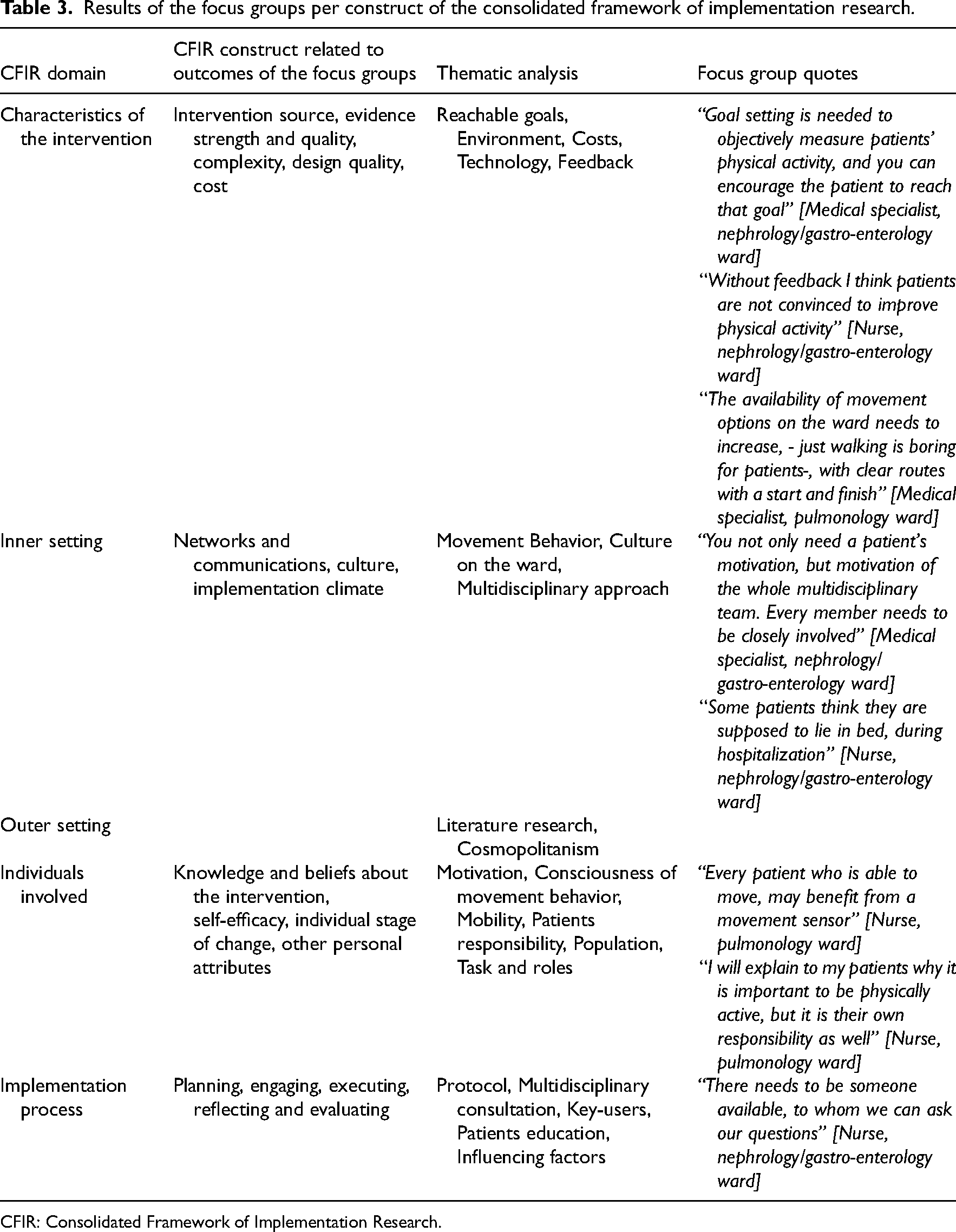
CFIR: Consolidated Framework of Implementation Research.
Step 2: Create change objectives; identifying roles and outcomes per stakeholder
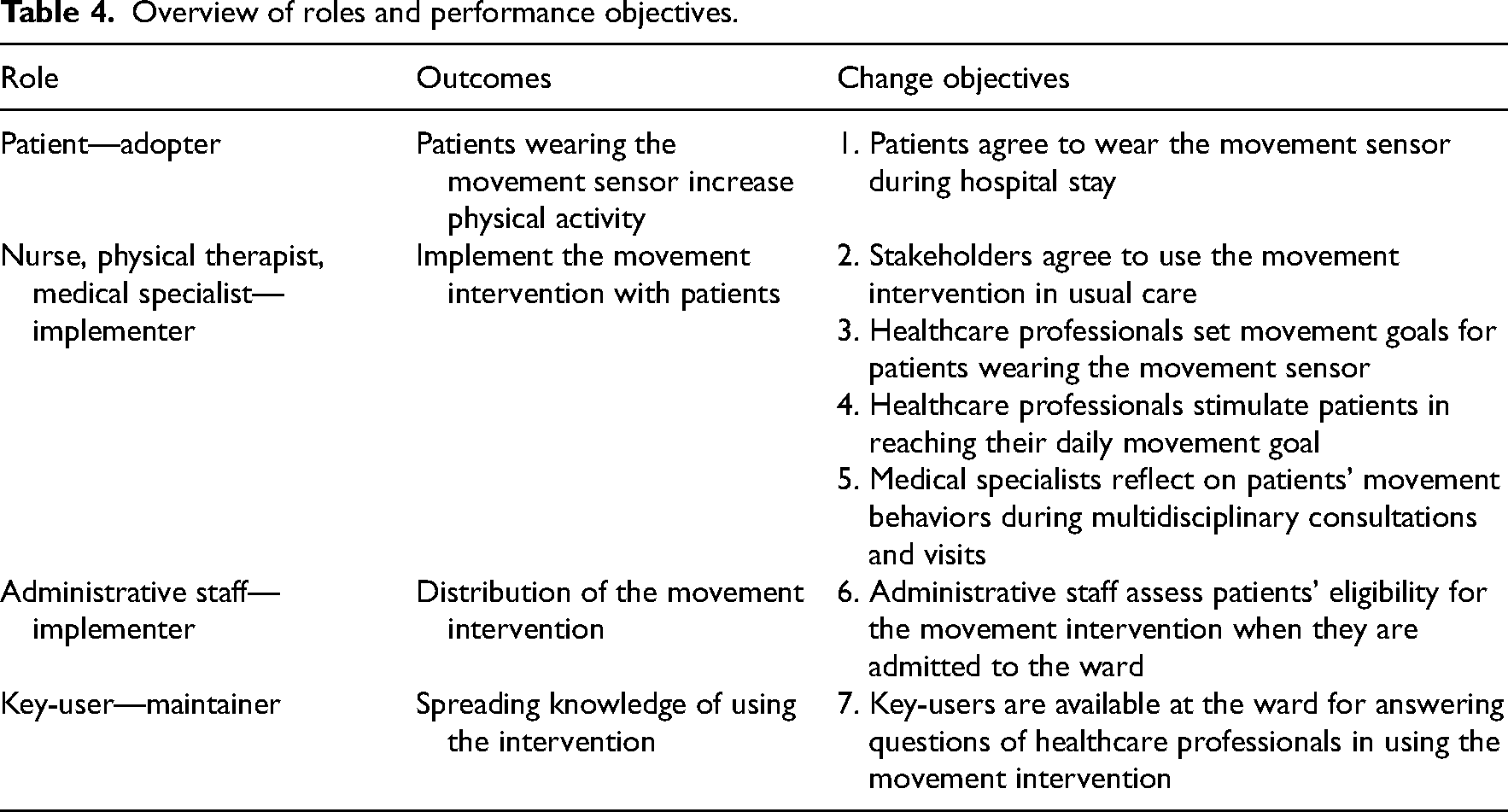
Following step 1, change objectives were defined for the different roles per stakeholder based on conversations with stakeholders and discussions with the research team (see Table 4).
Overview of roles and performance objectives.
Step 3: Select theoretical-based intervention methods.
Outcomes of the focus groups from step 1 (availability of feedback, an attractive surrounding of the ward and development of movement goals) were incorporated in the intervention design of the adapted intervention. The adapted intervention contains three behavioral change techniques (see also Table 5):
Adapted GOAL-intervention.
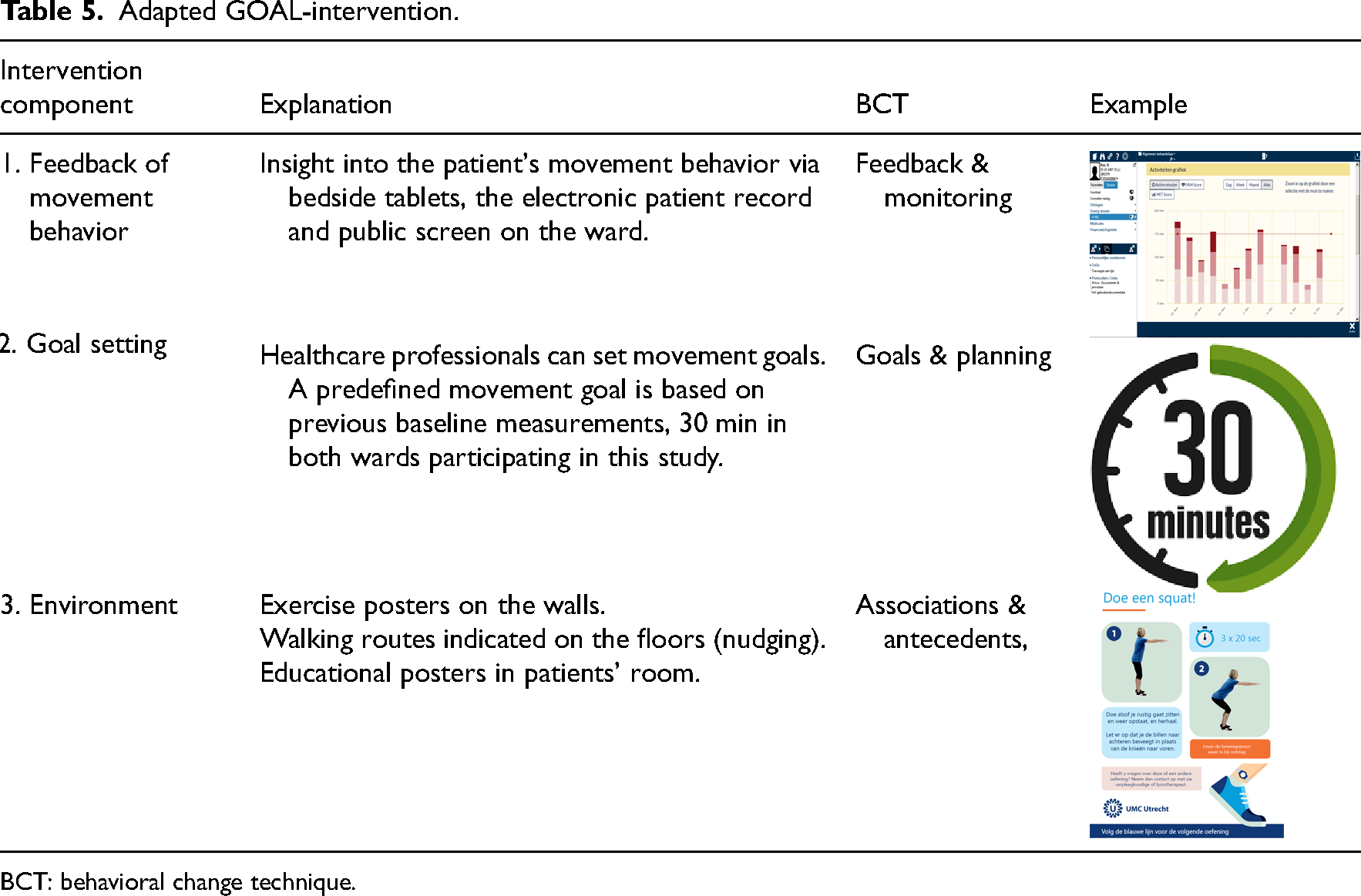
BCT: behavioral change technique.
1) Feedback of movement behavior: Stakeholders agreed that patients who wear a movement sensor should be provided with feedback on their physical activity via patients’ bedside tablets/mobile phone and/or a public screen in the reception area of the ward. Healthcare professionals can monitor patients’ physical activity via the electronic patient record. Behavioral change techniques are feedback & monitoring.
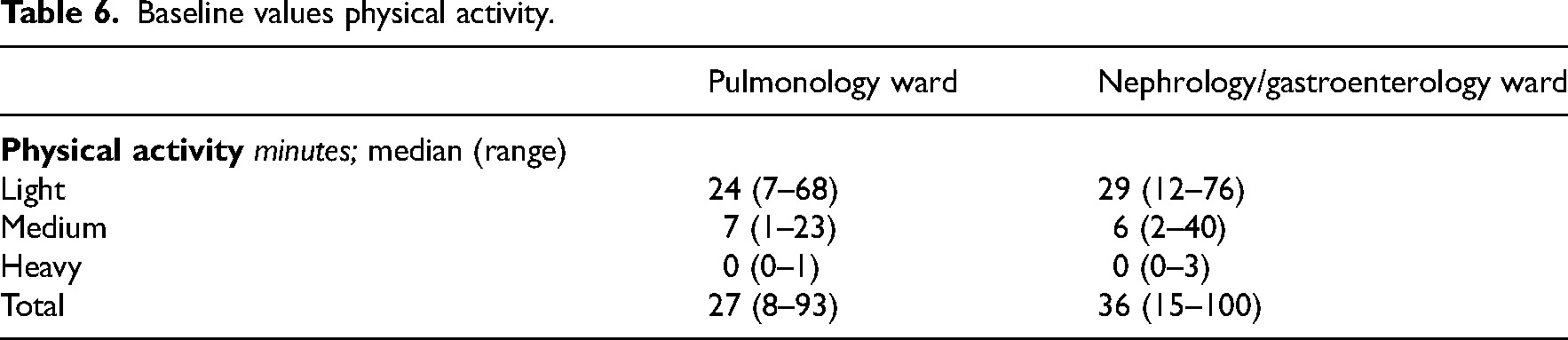
2) Goal setting: Administrative staff and healthcare professionals determined one movement goal per day for each patient. This movement goal was set at 30 min per day for patients admitted to the pulmonology- and nephrology/gastroenterology wards. This was based on preimplementation measurements (see Table 6) and adjusted by the healthcare professional if needed. Daily movement time was increased with 5–10 min per day as goals were reached, based on healthcare professionals’ judgment and patients’ capabilities. This increase is based on previous research in a surgical population. 1 Behavioral change techniques are goals & planning.
Baseline values physical activity.
3) Environment: In one of the focus groups, a nurse mentioned “Sometimes patients ask me; am I allowed to walk in the ward? [Nurse, pulmonary ward].” Patients were given the impression that they are getting in the way of the staff if they walk on the ward. Therefore, we decided to indicate walking routes on the floors of the wards and place leaflets with exercise instructions on the walls. Additionally, educational posters were placed in patients’ rooms. Behavioral change techniques are associations & antecedents.
Step 4: Integrate methods and practical applications into an organized program.
To facilitate successful implementation of the adapted intervention (step 3), implementation strategies were selected based on the outcomes of the focus groups and the Expert Recommendations for Implementing Change tool, 18 part of the consolidated framework of implementation research. 17
First, champions (key-users) should be identified and prepared. 18 “There needs to be a person who disseminates the idea, like an ambassador [Medical specialist, pulmonology ward].” Therefore, every ward needs to appoint at least one person, preferably a nurse, as key-user who is in close contact with all stakeholders in the project. Additionally, for nursing staff, pop-up notifications need to be added within standard text formats in the electronic patient files, to remind them of the intervention.
Second, educational meetings should be conducted. 18 Healthcare professionals frequently reported that they felt they lacked knowledge about movement goals (“I will cooperate in this project, but at this moment, my knowledge about setting movement goals is limited [Nurse, nephrology/gastroenterology ward]”). To effectively use the intervention, protocols about the use of the intervention and how to set movement goals need to be developed for the involved healthcare staff. Furthermore, clinical sessions on the application of the intervention as part of the usual care need to be organized.
Third, an audit and provision of feedback should be part of daily care. 18 Patients’ physical activity should be a standard topic at every meeting at the start of a shift. Furthermore, wards need to be encouraged to increase their “total active minutes” each week. Sharing these successes will remind healthcare professionals to use the intervention in daily care. Key-users need to provide an overview of the total number of patients who have worn the movement sensor at the end of the week. These numbers must be shared as feedback and monitoring for implementation outcomes. Thereby, we recommend to discuss the levels of patients’ physical activity during the medical specialist's visit, and to discuss the movement goals with patients and between disciplines.
Step 5: Plan for adoption, implementation and sustainability of the program in real-life contexts.
To ensure embedding in usual care, the wards need to be responsible for the implementation of the adapted intervention. A group of key-users need to be formed at each ward to create a guiding coalition. Key-users will be made responsible for repeating clinical instruction sessions and training regarding the setting of movement goals, whenever new staff was hired. We recommend that the intervention and its implementation are discussed in monthly team meetings and are incorporated in the annual action plans of the wards in which key performance indicators (see step 6) will be monitored.
Step 6: Generate an evaluation plan to conduct effect and process evaluations.
Specific key performance indicators will be defined on implementation service, and client outcomes, following the taxonomy of Proctor. 19
Implementation outcomes: Adoption is defined as the number of patients wearing the movement sensor in the ward and is evaluated monthly. When less than 70% of the patients wear the movement sensor during two consecutive months, key-users need to consult the ward management to investigate what is needed to increase the number of patients wearing the movement sensor. Furthermore, adoption needs to be evaluated by the number of patients with a set movement goal. For example, when less than 50% of the patients has a movement goal during two consecutive months, the key-users will investigate the problem and undertake activities to solve this.
Service outcomes: To evaluate the effect of the implementation on movement behavior during hospitalization, the average amount of physical activity per ward can be evaluated by the key-users. Key-users can share outcomes of movement behavior with their colleagues on the ward. When the total time of physical activity is decreasing. We recommend to undertake actions to correct this. This action plan can consist of the implementation strategies such as clinical instruction sessions.
Furthermore, safety of the intervention can be monitored through the number of adverse events related to the intervention. Each adverse event can be evaluated by the management of the ward.
Client outcomes: To monitor satisfaction of patients and healthcare professionals, the net promoter score can be used to evaluate the acceptation of the intervention. 20 When the net promoter score drops below 7 the key-user can prepare a meeting with the management of the ward to further investigate this score. It is recommended to score the net promoter annually by the key-users.
Discussion
In this study, we have described the development of the GOAL-intervention using a movement sensor for hospitalized patients in co-creation with healthcare professionals and patients following the steps of intervention mapping. For an efficient use of the intervention, we found that the application of the movement sensor should be accompanied with multiple intervention components: feedback of movement behavior, goal setting and environment. For successful implementation of the intervention, the following strategies are recommended: prepare & identify champions, conduct educational meetings and audit and provide feedback.
Self-monitoring for patients in this intervention is available using an app on the patients’ mobile device and a public screen on the ward in the reception area. Healthcare professionals stated that if the amount of physical activity is visible for both patients and professionals, this contributes to improved physical activity. This is supported by literature, as self-monitoring has the potential to reduce sedentary behavior in healthy adults. 25
Goal setting is stated to be effective in improving physical activity in both hospitalized and nonhospitalized populations. 11 A previous review stated that the use of a movement sensor with a step goal is associated with a significant increase in physical activity. 26 In our study, patients received a movement sensor with a predefined movement goal based on preimplementation measurements of activity levels. When this goal was reached by an individual patient, it was adjusted by healthcare professionals. This allows for tailoring and personalization of activity goals for patients. A downside of a predefined goal is that for some patients it can be unattainable or not challenging enough. To overcome this, movement goals should be monitored daily and can be adjusted if needed.
Walking routes were indicated with arrows on the floors, and leaflets with exercises instructions on the walls were developed within the component “adaptations in the built environment.” 27 The environment of the ward is part of the immobilizing hospital culture, which needs to be changed into a culture which invites patients to be physically active. 28 This can be supported by adding nudges in the environment, which are factors that can significantly alter behavior. 27
The multidisciplinary approach in this intervention is guaranteed by the engagement of healthcare professionals and the embedding in daily routine tasks. The pop-up notifications for nurses, insight in physical activity data and mentioning physical activity in the multidisciplinary consultation meetings keep the primary care taking staff engaged.28,29 Multidisciplinary engagement for stimulating patients’ physical activity during hospital admission seems important to change the culture of inactivity within the hospital. The involvement of the entire medical team stimulating the importance of improving physical activity will strengthen the message. 6
The most prominent implementation strategy we recommend is to identify and prepare champions (key-users). This strategy addresses barriers in the inner setting (i.e., culture on the ward), individuals involved (users of the intervention) and the implementation process (distribution of knowledge and protocols, engaging all healthcare professionals). The role of champions is also mentioned in previous literature, showing the importance of key-users to change movement behavior in a hospital setting. 29 Key-users can overcome staff members’ resistance by actively supporting the intervention during implementation. 29 Literature describes three roles a key user should play: initiating, facilitating and implementing. 30
This study distinguishes itself from other studies through the comprehensive needs assessment in step 1 of intervention mapping, ensuring valuable participation of a diverse group of healthcare professionals. The outcomes of this needs assessment provided valuable insights into which components were needed when implementing the intervention to increase inpatient physical activity. There were also some limitations in this study. First, patients were limitedly involved in this study. Because of the novelty of the intervention, it was difficult to ask their input during intervention development. Some patients with previous experience with a movement intervention in a different ward were asked for their opinion and experience. Therefore, in our effectiveness study, patients’ opinion is thoroughly evaluated, and the intervention is adjusted based on patient feedback, if needed. 14 Second, the goal of 30 min per day is based on relatively low sample-size baseline measurements on the specific wards and previous literature. 31 This predefined goal was set preimplementation and could be an underestimation of physical activity in the ward. It might be necessary to adjust these movement goals over time. If this goal is applicable on various other wards needs to be investigated.
Practical considerations should be considered. The main components used in this intervention are crucial and therefore recommended to use in an intervention to improve inpatients physical activity. 11 Nevertheless, each ward has its own culture, necessitating adjustments to the intervention and its implementation.29,32 Therefore, we recommend that other hospitals that seek to implement a goal-directed movement intervention follow a similar process of intervention mapping, enabling them to tailor the intervention to their specific environment. It is crucial to recognize the importance of fostering ownership and creating support from the ward to effectively adopt the intervention. By engaging stakeholders and thoroughly executing each iterative step of intervention mapping, the chances of successfully developing and implementing an intervention that is both effective and sustainable are significantly enhanced.32–34
Clinical messages
The use of a step-by-step iterative implementation model is recommended to guide the development and implementation of interventions aimed to promote physical activity during a hospital stay.
To ensure sustainable changes in physical activity levels of hospitalized patients, it is crucial to foster a sense of ownership and responsibility among the intervention users within the ward.
Supplemental Material
sj-docx-1-cet-10.1177_02692155231198173 - Supplemental material for Development of a goal-directed movement intervention (GOAL) using a movement sensor for hospitalized patients: An intervention mapping approach
Supplemental material, sj-docx-1-cet-10.1177_02692155231198173 for Development of a goal-directed movement intervention (GOAL) using a movement sensor for hospitalized patients: An intervention mapping approach by JWM van Grootel, P Bor, C Veenhof, and K Valkenet in Clinical Rehabilitation
Footnotes
Acknowledgements/Authors’ contributions
JvG and PB conducted most of the focus groups. Jolien Netjes (JN) and Miriam van de Velde (MV) were present at two focus groups. JvG, PB, KV and CV supported the writing process.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by Nationaal Regieorgaan Praktijkgericht Onderzoek SIA, (grant number (KIEM K21.01.037)).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.