
Abstract
Objective
People exhibiting post-stroke lateropulsion actively push their body across the midline to the more affected side and/or resist weight shift toward the less affected side. Despite its prevalence and associated negative rehabilitation outcomes, no clinical practice guidelines exist for the rehabilitation of post-stroke lateropulsion. We aimed to develop consensus-based clinical practice recommendations for managing post-stroke lateropulsion using an international expert panel.
Design
This Delphi panel process conformed with Guidance on Conducting and Reporting Delphi Studies recommendations.
Participants
Panel members had demonstrated clinical and/or scientific background in the rehabilitation of people with post-stroke lateropulsion.
Main Measures
The process consisted of four electronic survey rounds. Round One consisted of 13 open questions. Subsequent rounds ascertained levels of agreement with statements derived from Round One. Consensus was defined a priori as ≥75% agreement (agree or strongly agree), or ≥70% agreement after excluding ‘unsure’ responses.
Results
Twenty participants completed all four rounds. Consensus was achieved regarding a total of 119 recommendations for rehabilitation approaches and considerations for rehabilitation delivery, positioning, managing fear of falling and fatigue, optimal therapy dose, and discharge planning. Statements for which ‘some agreement’ (50%–74% agreement) was achieved and those for which recommendations remain to be clarified were recorded.
Conclusions
These recommendations build on existing evidence to guide the selection of interventions for post-stroke lateropulsion. Future research is required to elaborate specific rehabilitation strategies, consider the impact of additional cognitive and perceptual impairments, describe positioning options, and detail optimal therapy dose for people with lateropulsion.
Introduction
The phenomenon of actively pushing the body across the midline toward the more affected side, and/or actively resisting weight shift toward the less affected side is prevalent among people who require rehabilitation after stroke. 1 While the terms ‘pusher behaviour’, ‘pusher syndrome’ and ‘contraversive pushing’ have previously been used to describe this phenomenon, the term ‘lateropulsion’ is currently recommended.2,3 The presence of lateropulsion after stroke is associated with a need for longer rehabilitation length of stay, poorer functional outcomes, and reduced likelihood of home discharge.4,5 Despite the prevalence of lateropulsion after stroke, 1 research evidence for the efficacy of any particular therapeutic approach is limited. No clinical practice guidelines for the physical rehabilitation of post-stroke lateropulsion currently exist.
In addition to providing the initial description of ‘pusher syndrome’, Davies 6 proposed an approach to rehabilitation. The main aims of rehabilitation of ‘pusher syndrome’ were to: restore head control, stimulate activity in the lateral trunk flexors on the more affected side, regain midline in standing and walking, and regain the ability to safely climb stairs. Davies 6 recommended a forward lean position in the wheelchair, with the armrest on the unaffected side removed so that the patient cannot push on it. Broetz and Karnath 7 subsequently published recommendations for the rehabilitation of people with lateropulsion, including treating people in an ‘earth-vertical’ position and leveraging visual feedback of vertical position. However, Paci and Rinaldi 8 noted that some people with lateropulsion are unable to use visual input to align with their surroundings. More recent findings 9 have shown lateropulsion to be associated with neglect and impaired perception of visual vertical, which suggests difficulty exploring the spatial environment. Consequently, treatment based on visual cues alone may not be fully effective. 8 Multimodal rehabilitation approaches show some promise. 10
Evidence for the effect of different approaches to rehabilitation on lateropulsion is lacking. A recent scoping review investigating the evidence for treatment approaches for lateropulsion reported only five small randomised controlled trials (n = 12–36) from 31 included studies. 11 The authors reported ‘promising results’ in studies investigating somatosensory cues and visual-somatosensory integration, while approaches based on visual feedback alone were less effective. 11 They suggested further research to investigate the value of non-invasive brain stimulation (NIBS) in influencing lateropulsion. 11
This study examined consensus among an international Delphi panel of experts tasked with developing clinical practice recommendations for managing lateropulsion after stroke, using resources that are readily available in the majority of clinical settings. Recommendations regarding the definition of lateropulsion and preferred terminology to describe the condition were also developed and are published elsewhere. 3 The focus was primarily on physical rehabilitation although it is acknowledged that post-stroke lateropulsion is a complex phenomenon.
Methods
Design
This Delphi Panel Process conformed with the Guidance on Conducting and Reporting Delphi Studies 12 recommendations. The Process was registered via Open Science Framework at https://doi.org/10.17605/OSF.IO/KN3JT 13 and consisted of two sections: The first aiming to provide recommendations regarding terminology, 3 and the second to provide recommendations regarding rehabilitation for post-stroke lateropulsion. This paper addresses recommendations for rehabilitation of lateropulsion.
Participants
Identified experts were invited via email to participate in the panel. Written informed consent to participate was obtained. Participants had demonstrated clinical and/or scientific background in the rehabilitation of people with post-stroke lateropulsion. Invited participants met any of the following criteria: first or senior author of a published journal article (English language) reporting on rehabilitation of lateropulsion (2010–2020), identified via a search of Medline and CINAHL databases conducted in May 2020, using the terms, ‘lateropulsion or contraversive pushing’ AND ‘stroke or cerebrovascular accident or CVA’ AND ‘rehabilitation or therapy or treatment or intervention’ (authors of publication reports on lateral medullary syndrome only were excluded); and/or member of the Scale for Lateropulsion 14 development expert panel; and/or presented on lateropulsion at ‘Symposium on Human Perception of Verticality: Lateropulsion and Retropulsion in Neurological Disorders’ in May 2019; and able to complete the survey and communicate about the process in English.
To minimise the risk of selection bias, when multiple representatives from one institution expressed interest in participating, they were asked to select a maximum of two representatives to join the panel. This meant that bias toward the accepted practices at one institution could be avoided in developing consensus.
Procedures
The Delphi Process consisted of four online survey rounds conducted in English via the Qualtrics XM programme. 15 Participants were advised upon recruitment that the process would be ceased after a maximum of four rounds. During an optional introductory video conference meeting (via Zoom) prior to Round One, panellists discussed the potential need for future meetings between rounds. A second meeting was held between the second and third rounds, during which definitions of consensus and management of recommendations relevant to all people after stroke, as opposed to those of particular importance to those with lateropulsion, were discussed and agreed upon.
The Round One survey consisted of 13 open questions designed to establish themes and opinions of panel members regarding elements of rehabilitation of lateropulsion and priorities for discussion:
What term(s) should be used to describe the phenomenon of active pushing of the body across the midline toward the more affected side, or actively resisting weight shift toward the less affected side? (Results of this component of the study are published elsewhere.
3
) Please outline the most important components of the education about lateropulsion, which should be provided to affected people after stroke and their families/carers. Does the management of people with post-stroke lateropulsion vary according to assessment findings and/or presence of additional effects of stroke? Yes/No Please outline the factors that determine management strategies, and the ways in which these factors relate to management of the affected person. Please list the most important elements of rehabilitation for a person with post-stroke lateropulsion. Is the fear of falling an issue in people with post-stroke lateropulsion? Yes/No If it is an issue, how should this fear be addressed? Please outline the role of positioning (in bed and in sitting) in the management of lateropulsion. Which disciplines are essential in an ideal multidisciplinary team managing people with post-stroke lateropulsion, and what are their roles? What is the optimal ‘dose’ of therapy for a person with post-stroke lateropulsion? (Please refer to attached – Hayward, Churilov
16
) Please describe strategies that should be used to achieve this dose of therapy. Does fatigue usually affect performance of people with post-stroke lateropulsion? Yes/No If you believe that fatigue is often a problem, what strategies should be employed to manage fatigue, in rehabilitation of a person with post-stroke lateropulsion? How long should rehabilitation (inpatient, community and/or outpatient rehabilitation) for a person with post-stroke lateropulsion continue? Please list the factors that influence the decision to discontinue rehabilitation. Please outline considerations that should be made and steps that should be undertaken when discharging a person with post-stroke lateropulsion from the inpatient setting to:
Home or a private residence; and Residential care. What do you see as the top three priorities for future research in post-stroke lateropulsion? (Results of this component of the study are published elsewhere.
3
)
Two representatives with lived experience of lateropulsion after stroke (one person with stroke and one caregiver) provided input into development of the first round of survey questions to ensure that consumer priorities were included in the topic areas considered in the process. Subsequent rounds ascertained levels of agreement with statements derived from Round One. Levels of agreement were set a priori.
12
‘Consensus’ was defined as ≥75% agreement (agree or strongly agree) or ≥70% agreement after excluding ‘unsure’ responses. ‘Some agreement’ was defined as 50%–74% agree or strongly agree, or 75% agreement reached after excluding both ‘unsure’ and ‘neutral’ responses, but <70% agreement when excluding ‘unsure’ responses only. Statements with no clear agreement were labelled ‘remains to be clarified’, with recommendation for additional research. Areas with clear disagreement (majority of panel disagreed or strongly disagreed) were to be reported but not included in the recommendations.
When consensus was reached, that statement was not represented in subsequent rounds. Overall results of each round were provided to panel members before commencement of the subsequent round. Where prior research on rehabilitation of lateropulsion was available, relevant studies were embedded in the survey for reference, however the process did not include a critical literature review. Links to the Australian, 17 American, 18 Canadian, 19 and United Kingdom 20 Stroke Guidelines referring to the amount of rehabilitation were also included in the survey questions regarding optimal therapy dose.
Data analysis
Quantitative data were reported using descriptive statistics with percentages and frequency counts. Content analysis of data from Round One using the NVivo programme 21 informed the development of subsequent rounds. Agreed elements of lateropulsion rehabilitation were prioritised and ranked. Levels of the agreement for all statements were calculated and reported, as described above. Individual panel member responses remained de-identified to minimise the risk of panel members changing their minds to avoid expressing an unpopular opinion or expediting consensus. Where the panel convenor considered statements to be applicable to all people with stroke (generic) rather than of particular importance to those with lateropulsion, the statement was presented again to the panel. It was removed when the panel agreed (≥75%) that the statement was generic.
Ethical considerations
This study was approved by the Edith Cowan University (ECU) Human Research Ethics Committee (2019-00501-NOLAN). The Data Management Plan (2020-DMP-00054) for this study was approved by ECU Research Integrity.
Results
Thirty-nine experts were identified and invited to participate. Twenty-three provided written informed consent to participate. Twenty-two were included as three participants represented the same institution (this institution decided that two participants would complete the responses together, under the name of one-panel member). One participant withdrew before the process began due to a change in their availability. Five experts declined participation and 11 did not respond (of these, one sent an out-of-office autoreply, and one responded after the deadline and after the panel had been finalised). Surveys were distributed to 21 participants in Round One. Of these, 20 surveys were returned. All 20 of these participants completed the four rounds of the process (May to November 2021). Complete results of each round, including levels of agreement, are reported in Supplemental File 1.
Panel demographics
Panel members represented 10 countries: Australia (n = 1), Belgium (n = 2), Brazil (n = 1), Canada (n = 2), France (n = 2), Germany (n = 2), Italy (n = 2), Japan (n = 2), United Kingdom (n = 1), and United States of America (n = 5). The panel consisted of physiotherapists (n = 12, 60%), medical doctors/rehabilitation physicians (n = 4, 20%), movement scientists/kinesiologists (n = 2, 10%), and neuropsychologists (n = 2, 10%). Panel members worked clinically (n = 17, 85%), in research roles (n = 19, 95%), and in educator roles (n = 10, 50%). Of those working clinically, 17/17 (100%) worked in the inpatient setting, 2/17 (12%) also worked in the community/home visiting, and 7/17 (41%) also worked in the outpatient setting. Clinicians worked with people with stroke in the acute (6/17, 35%), sub-acute/rehabilitation (17/17, 100%) and chronic (9/17, 53%) phases of recovery. Panel members and their affiliations are listed in Supplemental File 2.
Delphi panel recommendations
Consensus was achieved regarding a total of 119 recommendations for education about lateropulsion, rehabilitation approaches and considerations for rehabilitation delivery, positioning, managing fear of falling and fatigue, optimal therapy dose, and discharge planning. Statements for which some agreement was achieved and statements that remain to be clarified are outlined in Supplemental Files 3 and 4, respectively. No statements resulted in clear disagreement.
Education about lateropulsion to people with lateropulsion and caregivers
The panel agreed that customised education about lateropulsion should be provided to caregivers and persons with lateropulsion in accordance with their unique clinical presentation. There was consensus that education should encompass:
Characteristics of lateropulsion Rehabilitation and management strategies; and Impact and prognosis of lateropulsion.
Elements recommended (consensus was achieved) for inclusion in education are outlined in Table 1. Statements for which some agreement was achieved and statements that remain to be clarified are outlined in Supplemental Files 3 and 4, respectively.
Elements recommended for inclusion in the education about lateropulsion to the affected person and their family/caregivers.
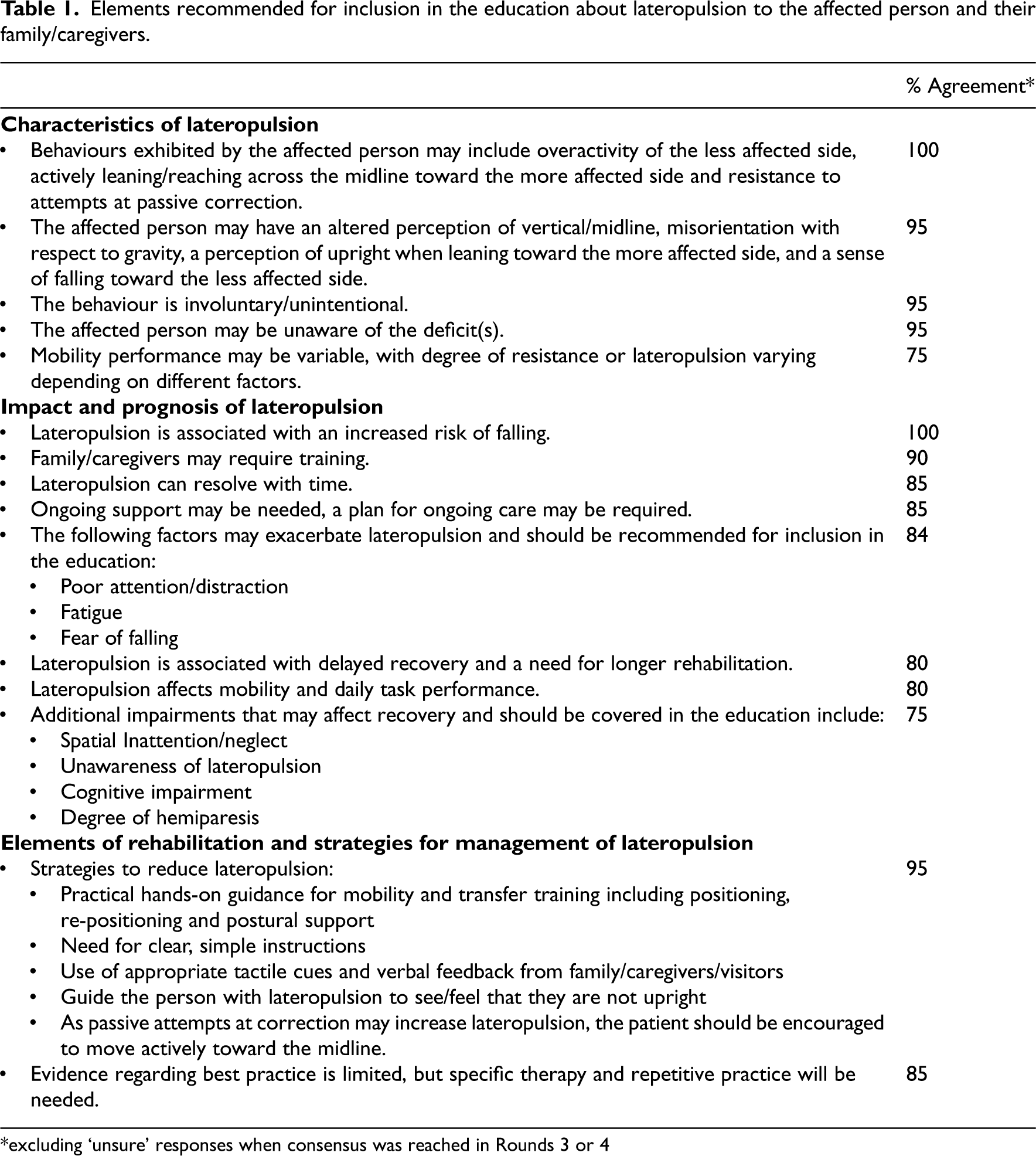
*excluding ‘unsure’ responses when consensus was reached in Rounds 3 or 4
Elements of rehabilitation of lateropulsion
Consensus was achieved regarding the overall approach to rehabilitation and various specific rehabilitation strategies for a person with post-stroke rehabilitation. Recommendations (consensus achieved) regarding elements of rehabilitation of lateropulsion are outlined in Table 2. Statements for which some agreement was achieved and statements that remain to be clarified are outlined in Supplemental Files 3 and 4, respectively.
Recommendations regarding elements of rehabilitation.
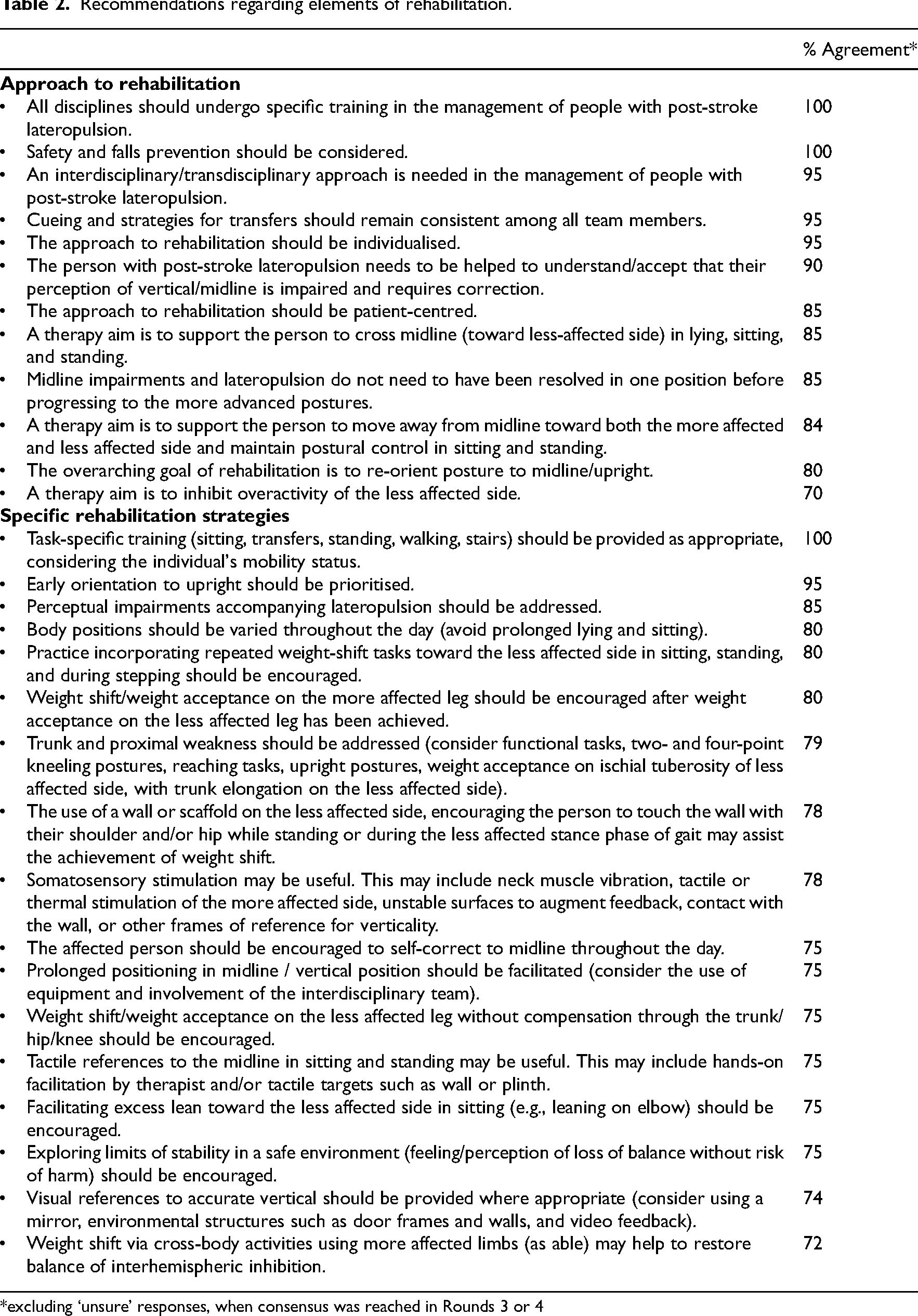
*excluding ‘unsure’ responses, when consensus was reached in Rounds 3 or 4
Various ‘novel’ treatment strategies
11
that may require non-standard equipment were suggested. Treadmill or robot-assisted gait training22–25 which is supported by some evidence, was recommended by 14/20 panel members (70%). Because the evidence for effectiveness in rehabilitation of lateropulsion was not yet considered to be sufficient, the panel did not recommend routine use of the following interventions:
Video games referring to horizontal/vertical. Virtual reality training. Transcranial direct current stimulation. Functional neuromuscular electrical stimulation. Transcutaneous electrical nerve stimulation applied to contralesional side of the neck. Whole-body tilt apparatus. Force platform bio-feedback. Recumbent stepper.
Considerations for management of lateropulsion
There was consensus that the approach to management of post-stroke lateropulsion should be informed by severity of lateropulsion, the person's awareness of their lateropulsion, and individual stroke and person-related factors. Recommendations regarding considerations for the management of lateropulsion are outlined in Table 3. Statements for which some agreement was achieved and statements that remain to be clarified are outlined in Supplemental Files 3 and 4, respectively. As agreed by the panel, strategies not of particular importance to those with lateropulsion, versus those without, have been excluded from this report.
Consensus statements regarding considerations for management of lateropulsion.
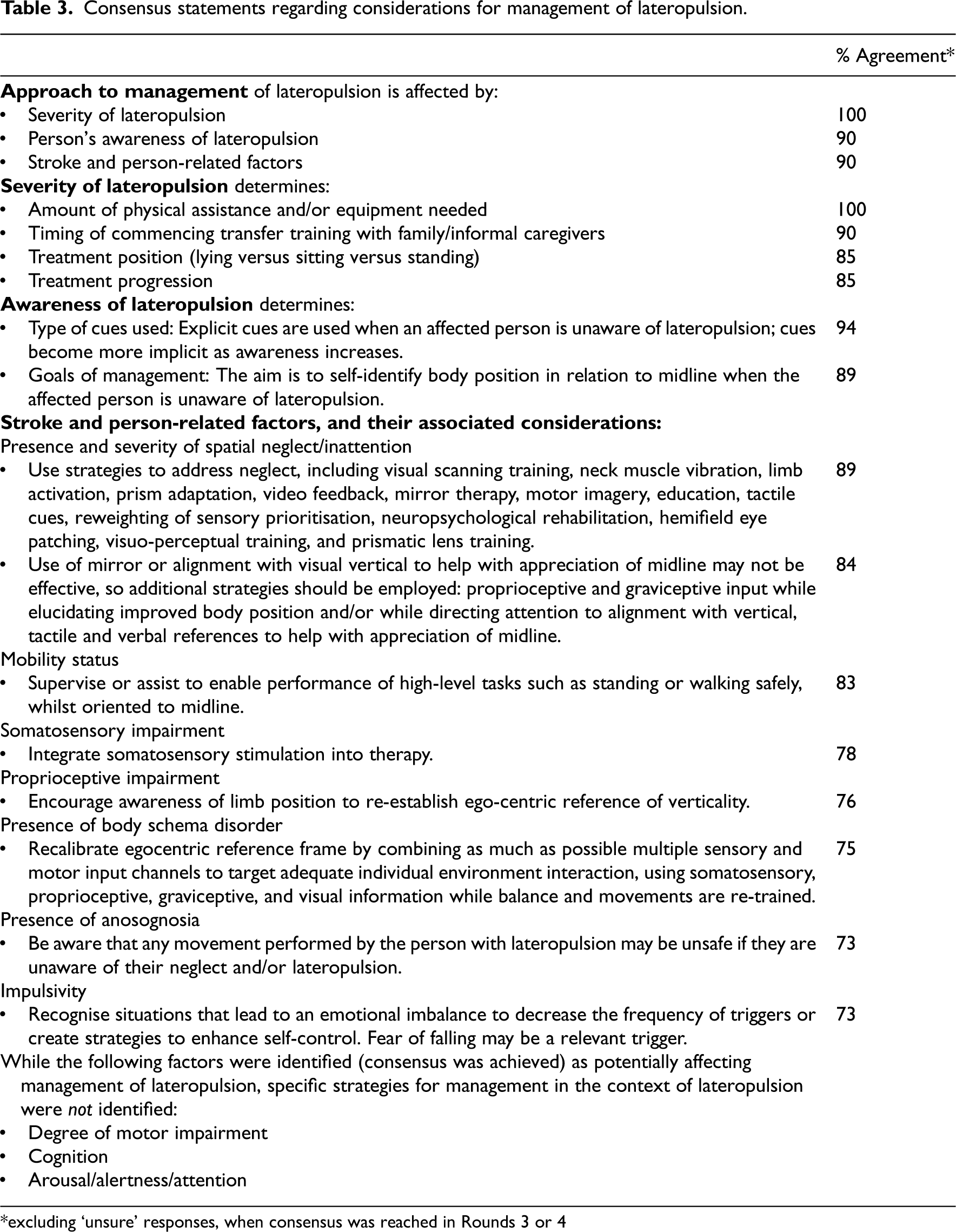
*excluding ‘unsure’ responses, when consensus was reached in Rounds 3 or 4
Optimal therapy dose
Dose of rehabilitation was conceptualised in terms of the dose domains described by Hayward et al. 16 : Duration, days per week, sessions per day, session length, session density, session difficulty, and intensity. Considering only people with post-stroke lateropulsion who are medically stable, there was consensus that optimal rehabilitation dose differs between people with stroke with lateropulsion versus those without lateropulsion, when all other stroke-related factors are the same. There was consensus that in people with post-stroke lateropulsion, the optimal therapeutic dose depends on severity of lateropulsion, stage of recovery 26 after stroke, and person and stroke-related factors (presence of neglect/inattention and overall functional status).4,5,27–33
Attempts in Rounds one and two at ascertaining specific dose recommendations produced widely varying results. Rounds three and four aimed to achieve agreement on dose recommendations in comparison to people with stroke without lateropulsion or requirements relative to those without the relevant stroke-related factor. Complete results of therapy dose recommendations, including levels of agreement reached in Rounds Three and Four, according to the severity of lateropulsion, stage of recovery, and person and stroke-related factors, are outlined in Supplemental File 5.
As agreed by the panel, strategies which may be used to increase therapy dose are relevant to all people with stroke, so they were not included in these recommendations. Statements for which some agreement was achieved and statements that remain to be clarified are outlined in Supplemental Files 3 and 4, respectively.
Addressing fear of falling
There was consensus that fear of falling toward the less affected side is an issue affecting rehabilitation in people with post-stroke lateropulsion, although evidence that lateropulsion is associated with increased risk of falls is still lacking.
Recommendations (consensus achieved) addressing fear of falling are outlined in Table 4. Statements for which some agreement was achieved are outlined in Supplemental File 3. As agreed by the panel, while general falls prevention strategies apply, only strategies considered by the panel to be of particular importance to those with lateropulsion have been included in these recommendations.
Recommendations (consensus was achieved) to address fear of falling in people with post-stroke lateropulsion.
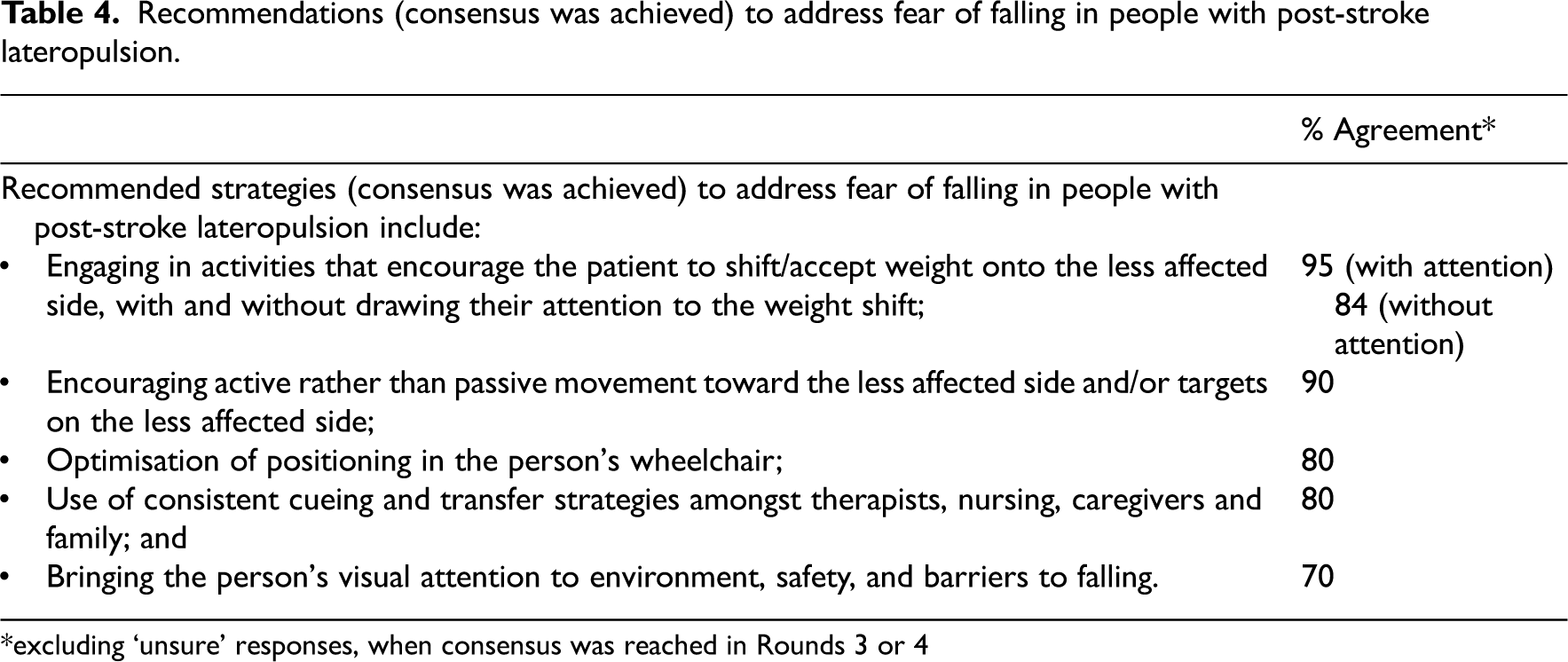
*excluding ‘unsure’ responses, when consensus was reached in Rounds 3 or 4
Positioning
While general aims of positioning after stroke apply, as agreed by the panel, only those considered by the panel to be of particular importance to people with post-stroke lateropulsion were included in these recommendations. Consensus statements regarding optimal positioning for people with post-stroke lateropulsion are outlined in Table 5. Statements for which some agreement was achieved are outlined in Supplemental File 3.
Recommendations (consensus was achieved) regarding positioning for people with post-stroke lateropulsion.
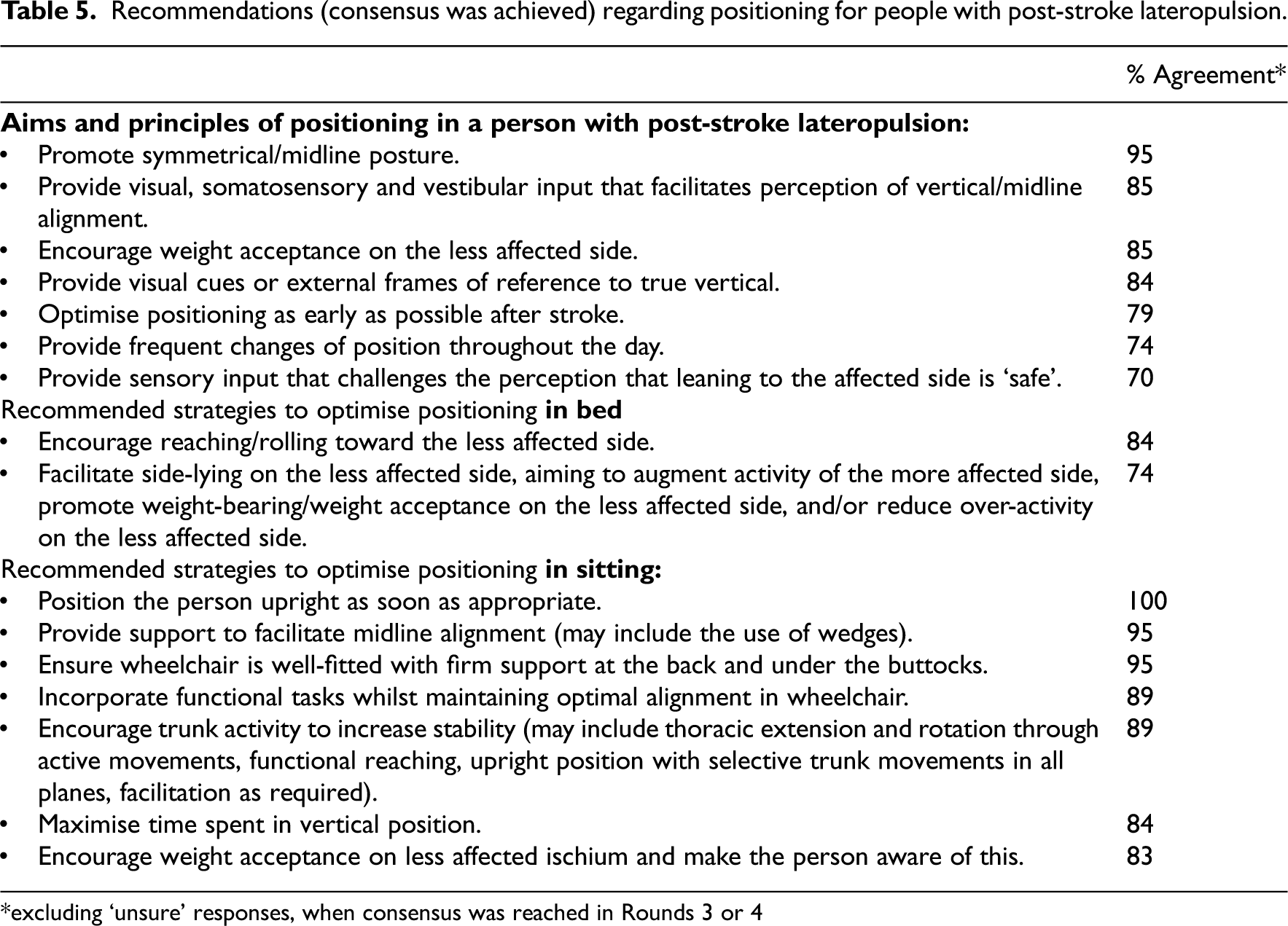
*excluding ‘unsure’ responses, when consensus was reached in Rounds 3 or 4
Management of fatigue
There was consensus that fatigue affects the performance of people with post-stroke lateropulsion and that lateropulsion becomes more apparent or more severe as the person becomes fatigued. Consensus regarding all statements relating to management of fatigue was achieved (Table 6). While general fatigue management strategies apply, only those strategies considered by the panel to be of particular importance to those with lateropulsion were included in these recommendations.
Recommendations (consensus was achieved) regarding management of fatigue for people with post-stroke lateropulsion.
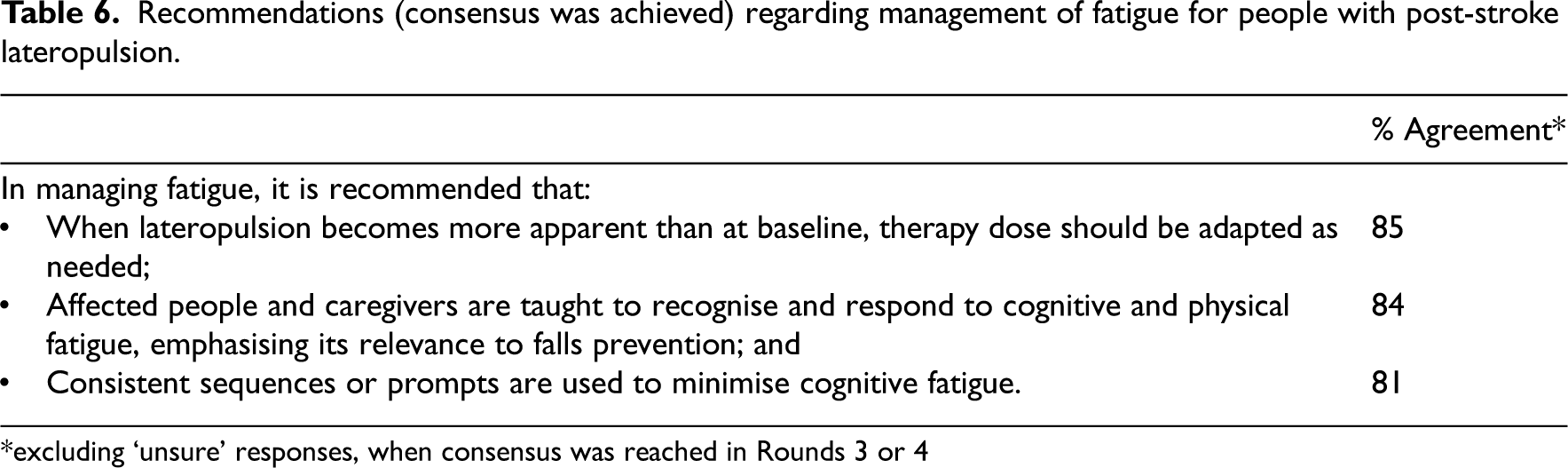
*excluding ‘unsure’ responses, when consensus was reached in Rounds 3 or 4
Discharge planning
Recommendations regarding discharge planning considered planning for discharge to home or to a residential care facility. Consensus regarding all statements relating to discharge planning for people with post-stroke lateropulsion was achieved (Table 7).
Recommendations (consensus was achieved) regarding discharge planning for people with post-stroke lateropulsion.
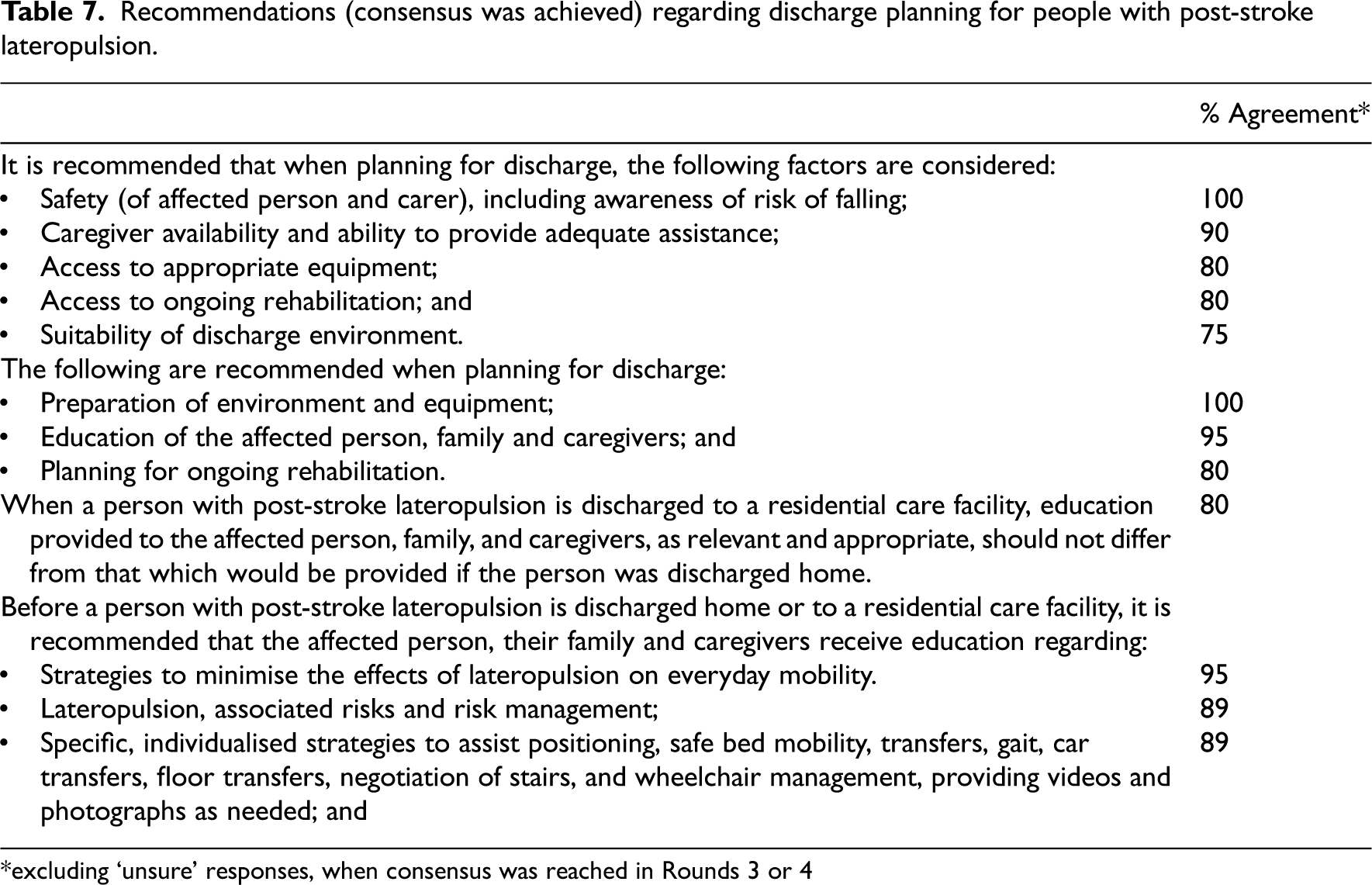
*excluding ‘unsure’ responses, when consensus was reached in Rounds 3 or 4
As agreed by the panel, specific strategies and procedures regarding planning for equipment/environment and ongoing rehabilitation requirements are applicable to all people with stroke, so were not included in these recommendations.
Discussion
This Delphi Panel Process aimed to describe and develop an international expert consensus on best-practice ‘usual care’ rehabilitation of post-stroke lateropulsion, using resources that are readily available in the majority of clinical settings. Clinicians may use these recommendations to anticipate rehabilitation length of stay, and to plan rehabilitation dose and specific rehabilitation strategies for people with post-stroke lateropulsion, considering lateropulsion severity, stage of post-stroke recovery, and influence of additional post-stroke impairments.
Panel recommendations build on approaches to rehabilitation described by Broetz and Karnath, 7 including awareness of altered perception of vertical, attainment of vertical, and weight acceptance on the less affected side, via a combination of visual, verbal, and somatosensory feedback. As more recent evidence has demonstrated the existence of an association between impaired visual vertical perception and lateropulsion, 9 recommendations from this panel emphasised tactile rather than reliance on visual cues achieve vertical alignment. Although a recent study 9 reported spatial neglect, measured via a robust battery of six assessments, to be present in 100% of participants with lateropulsion, earlier studies5,27,29,32 showed the presence of neglect, using a less robust assessment process, in a high proportion, but not all, of participants with lateropulsion. Further research is needed to confirm whether neglect always co-exists with post-stroke lateropulsion. This panel provided recommendations for rehabilitation taking into account the impact of moderate and severe neglect and other cognitive and perceptual impairments, which have not been addressed in previous literature, and which can guide clinical decision-making. Inconsistent measurement and reporting of neglect among studies in people with lateropulsion highlights the need for future recommendations regarding minimum data collection standards.
Previous literature has not provided recommendations regarding education about lateropulsion to the patients and caregivers, the need for interdisciplinary team input, strategies to address fear of falling in affected people, positioning in lying, considerations relating to management of fatigue, and specific considerations for discharge planning. Although based on expert opinion only, the agreed recommendations from this Delphi panel addressing these gaps may guide more effective management of this prevalent condition and provide a foundation for future intervention studies.
Reported treatment duration and intensity of rehabilitation vary in previously published studies. Evidence that people with lateropulsion need longer-duration therapy exists,4,5 but the remaining domains of optimal therapy dose16,34 are not described in the existing literature. Recently published interventional studies compared novel therapies for lateropulsion with ‘usual care’.22–25,35,36 Future studies investigating novel therapies, such as robotic assistance and NIBS, will require dose-finding and dose-ranging16,34 methodologies followed by studies using comparison groups, with well-described ‘usual care’. An agreed best-practice ‘usual care’ approach to the rehabilitation of lateropulsion is not available from the current literature. Recommendations resulting from this process may provide a standard ‘usual care’, against which future interventional studies may be compared.
Prior studies have shown that a longer rehabilitation duration is needed for people with post-stroke lateropulsion, and a further increased duration may be needed for those with older age, severe lateropulsion, moderate or severe neglect, greater number of additional impairments, poorer overall functional status, and right-sided lesions.4,5,27–33 The panel also recommended that rehabilitation is continued as long as a person with post-stroke lateropulsion has ongoing rehabilitation goals. The remaining domains of optimal dose of rehabilitation for those with lateropulsion (therapy days per week, sessions per day, session length, session density, session difficulty, and intensity 16 ) have not been addressed in previous studies. This expert panel was unable to agree on specific dose recommendations and demonstrated wide variation in opinion, but agreed on many factors that may influence optimal dose of rehabilitation (Supplemental File 5). Further clarification of this area of rehabilitation for post-stroke lateropulsion is needed. In addition to the optimal therapeutic dose, recommendations regarding some rehabilitation strategies, considerations for rehabilitation, elements for inclusion in the explanation of lateropulsion, addressing fear of falling, and positioning failed to reach consensus (Supplemental Files 3 and 4), and further research is needed to guide clinical practice.
A major strength of this Delphi process was the expertise of panel members in lateropulsion rehabilitation, all of whom had demonstrated clinical and scientific backgrounds in the area. After the process began, there was no attrition of panel members, with all 20 participants completing all four rounds. Representatives with lived experience of post-stroke lateropulsion provided input into the areas addressed in the initial survey round.
The process was limited to those who were able to participate in English and only identified potential members through publications in English. This language limitation means that potential expert panel members who were not English-speaking were not included. However, the panel had wide global representation, with the representation of varied health systems, although 19/20 (95%) of panel members represented ‘high income’ countries.
Where evidence existed relating to a survey question, the relevant publications were embedded in the surveys for reference, however, the process did not include a critical literature review. While provision of relevant publications was intended to ensure consistency of knowledge base among panel members, it may have introduced a source of potential bias in participant responses.
Addressing mechanisms that underpin lateropulsion, such as impaired perception of vertical, 9 although relevant, was outside the scope of the study. While stroke location and stroke type may also influence the optimal approach to rehabilitation of lateropulsion, these factors were not addressed in this study. The recommendations focused on rehabilitation of the manifestations of lateropulsion, regardless of the underlying mechanisms or stroke type.
Despite its presence in approximately half of the people with stroke, 1 lateropulsion is not currently addressed in the Australian, American, Canadian, or United Kingdom Stroke Guidelines17–20 due to the limited available research. Recommendations were limited to the opinions and experience of the panel experts but built on existing research or clinical recommendations in prior literature. While it is clear that cognitive and perceptual rehabilitation is needed in managing lateropulsion, the majority of specific recommendations resulting from this process focused on physical aspects of rehabilitation. These recommendations may provide a guide to clinical decision-making, until strategy-specific intervention studies become available.
In conclusion, these recommendations for clinical practice are offered to guide national and international clinicians and educators in selecting the physical rehabilitation approaches that will most likely facilitate people with post-stroke lateropulsion to meet their rehabilitation potential, resulting in improved functional outcomes and a lower level of long-term disability. The present Delphi study represents the best available expert opinion for the management of lateropulsion. Future research is needed to confirm recommendations regarding rehabilitation strategies, with and without the use of ‘novel’ therapeutic interventions, to consider the impact of additional cognitive and perceptual impairments, including neglect, on lateropulsion rehabilitation, and to describe optimal positioning options and therapy dose for people with post-stroke lateropulsion.
Clinical messages
Post-stroke lateropulsion is prevalent and is associated with poorer rehabilitation outcomes and reduced likelihood of discharge home.
In the absence of evidence-based clinical guidelines, these recommendations represent the best available expert opinion for management of post-stroke lateropulsion, using resources that are readily available in the majority of clinical settings.
Supplemental Material
sj-docx-1-cre-10.1177_02692155231172012 - Supplemental material for Clinical practice recommendations for management of lateropulsion after stroke determined by a Delphi expert panel
Supplemental material, sj-docx-1-cre-10.1177_02692155231172012 for Clinical practice recommendations for management of lateropulsion after stroke determined by a Delphi expert panel by Jessica Nolan, Angela Jacques, Erin Godecke, Hiroaki Abe, Suzanne Babyar, Jeannine Bergmann, Melissa Birnbaum, Shenhao Dai, Cynthia Danells, Taiza GS Edwards, Marialuisa Gandolfi, Klaus Jahn, Ryan Koter, Avril Mansfield, Junji Nakamura, Vicky Pardo, Dominic Perennou, Celine Piscicelli, David Punt, Devra Romick-Sheldon, Wim Saeys, Nicola Smania, Nathalie Vaes, Abigail L Whitt and Barbara Singer in Clinical Rehabilitation
Supplemental Material
sj-docx-2-cre-10.1177_02692155231172012 - Supplemental material for Clinical practice recommendations for management of lateropulsion after stroke determined by a Delphi expert panel
Supplemental material, sj-docx-2-cre-10.1177_02692155231172012 for Clinical practice recommendations for management of lateropulsion after stroke determined by a Delphi expert panel by Jessica Nolan, Angela Jacques, Erin Godecke, Hiroaki Abe, Suzanne Babyar, Jeannine Bergmann, Melissa Birnbaum, Shenhao Dai, Cynthia Danells, Taiza GS Edwards, Marialuisa Gandolfi, Klaus Jahn, Ryan Koter, Avril Mansfield, Junji Nakamura, Vicky Pardo, Dominic Perennou, Celine Piscicelli, David Punt, Devra Romick-Sheldon, Wim Saeys, Nicola Smania, Nathalie Vaes, Abigail L Whitt and Barbara Singer in Clinical Rehabilitation
Supplemental Material
sj-docx-3-cre-10.1177_02692155231172012 - Supplemental material for Clinical practice recommendations for management of lateropulsion after stroke determined by a Delphi expert panel
Supplemental material, sj-docx-3-cre-10.1177_02692155231172012 for Clinical practice recommendations for management of lateropulsion after stroke determined by a Delphi expert panel by Jessica Nolan, Angela Jacques, Erin Godecke, Hiroaki Abe, Suzanne Babyar, Jeannine Bergmann, Melissa Birnbaum, Shenhao Dai, Cynthia Danells, Taiza GS Edwards, Marialuisa Gandolfi, Klaus Jahn, Ryan Koter, Avril Mansfield, Junji Nakamura, Vicky Pardo, Dominic Perennou, Celine Piscicelli, David Punt, Devra Romick-Sheldon, Wim Saeys, Nicola Smania, Nathalie Vaes, Abigail L Whitt and Barbara Singer in Clinical Rehabilitation
Supplemental Material
sj-docx-4-cre-10.1177_02692155231172012 - Supplemental material for Clinical practice recommendations for management of lateropulsion after stroke determined by a Delphi expert panel
Supplemental material, sj-docx-4-cre-10.1177_02692155231172012 for Clinical practice recommendations for management of lateropulsion after stroke determined by a Delphi expert panel by Jessica Nolan, Angela Jacques, Erin Godecke, Hiroaki Abe, Suzanne Babyar, Jeannine Bergmann, Melissa Birnbaum, Shenhao Dai, Cynthia Danells, Taiza GS Edwards, Marialuisa Gandolfi, Klaus Jahn, Ryan Koter, Avril Mansfield, Junji Nakamura, Vicky Pardo, Dominic Perennou, Celine Piscicelli, David Punt, Devra Romick-Sheldon, Wim Saeys, Nicola Smania, Nathalie Vaes, Abigail L Whitt and Barbara Singer in Clinical Rehabilitation
Supplemental Material
sj-docx-5-cre-10.1177_02692155231172012 - Supplemental material for Clinical practice recommendations for management of lateropulsion after stroke determined by a Delphi expert panel
Supplemental material, sj-docx-5-cre-10.1177_02692155231172012 for Clinical practice recommendations for management of lateropulsion after stroke determined by a Delphi expert panel by Jessica Nolan, Angela Jacques, Erin Godecke, Hiroaki Abe, Suzanne Babyar, Jeannine Bergmann, Melissa Birnbaum, Shenhao Dai, Cynthia Danells, Taiza GS Edwards, Marialuisa Gandolfi, Klaus Jahn, Ryan Koter, Avril Mansfield, Junji Nakamura, Vicky Pardo, Dominic Perennou, Celine Piscicelli, David Punt, Devra Romick-Sheldon, Wim Saeys, Nicola Smania, Nathalie Vaes, Abigail L Whitt and Barbara Singer in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors would like to thank the consumer representatives, Mrs. Marie Speering and family (who contributed to this process in memory of Mr Ted Speering), and Mr Kevin Handforth, for their valuable input into the development of this process.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article: This study was supported by a Raine Medical Research Foundation/Western Australian Department of Health Clinician Research Fellowship (CRF04-R9), the Charlies Foundation for Research (RAC 2020-21-021) and an Australian Government Research Training Programme Scholarship
Ethical approval
This study was approved by the Edith Cowan University (ECU) Human Research Ethics Committee (2019-00501-NOLAN). The Data Management Plan (2020-DMP-00054) for this study was approved by ECU Research Integrity.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.