
Abstract
Objective
To explore how stakeholders in rehabilitation conceptualise ‘successful rehabilitation’, to inform the development of a minimum dataset and core outcomes for sub-acute rehabilitation.
Design
Qualitative consensus study using the nominal group technique.
Setting
Online focus groups.
Participants
Consumer representatives (n = 7), clinicians (n = 15), and health service managers (n = 9) from Australia.
Intervention
Participants responded to the question, ‘What does successful rehabilitation look like?’. Following item generation, they prioritised their top five responses, allocating 100 points across items to denote relative importance.
Main measures
Prioritised responses were analysed across stakeholder groups using qualitative content analysis.
Results
Ten themes were identified. ‘Successful rehabilitation’ is: (1) person and family centred; (2) effective; (3) inter-professional; (4) accessible; (5) goal oriented with meaningful outcomes; (6) connected to the continuum of care; (7) evidence-based and supportive of innovation and research; (8) appropriately funded and skilled; (9) satisfying and engaging; and (10) safe.
Conclusions
Stakeholder-defined ‘successful rehabilitation’ aligned with principles of value-based care and evidence-based rehabilitation. Provision and receipt of person and family centred care was the most important indicator of successful rehabilitation. Measures of success should include indicators of structure, process, outcome, and experience, and be conducted at multiple time-points.
Introduction
Globally, as many as 2.41 billion people have a health condition that would benefit from rehabilitation. 1 Population ageing and advances in curative medicine have fuelled the need for long-term management of chronic health conditions, where the outcome of interest is functioning, rather than mortality or morbidity. 2 Rehabilitation is, ‘a set of interventions designed to optimize functioning and reduce disability in individuals with health conditions in interaction with their environment’. 3 , page 1 While as many as one in three people live with a health condition that would benefit from rehabilitation, many countries around the world are not equipped to meet this need. 4 To this end, the World Health Organization (WHO) Rehabilitation 2030 initiative has outlined ten areas for action, one of which centres on the collection of information relevant to rehabilitation to enhance health information systems, including system level data and information on functioning. 5
Meaningful measurement of system outputs and patient outcomes has the potential to drive quality improvement, strengthening and extending rehabilitation services. Knowing what to measure however, requires the operationalisation of a meaningful definition of ‘successful rehabilitation’. Wade 6 extracted data from systematic reviews and trials, identifying features of rehabilitation found to benefit patients. Their resulting evidence-based definition posits ‘effective rehabilitation’ as a problem-solving process within the context of the holistic biopsychosocial model of health, that is delivered in a person-centred manner by an expert, multidisciplinary team who set collaborative team-based goals and monitor intervention outcomes. It includes repeated practice of functional activities, education with an emphasis upon self-management, psycho-social support, and specific interventions that are tailored to the patient's priorities, needs and goals. 6 Central to this definition is a person-centred approach to rehabilitation. As Wade 6 surmise, while rehabilitation as a process is effective, the heterogeneity of clients, interventions and health disciplines, combined with the requirement for patient participation and human interaction, plus the measurement of hard-to-define outcomes, culminates in the need for a highly individualised approach. The authors resolve that rehabilitation in design, delivery and measurement, must be person-centred, individualised and tailored. 6
Value-based healthcare seeks to produce outcomes that are important to consumers relative to the cost of achieving those outcomes. 7 This approach incorporates principles of person-centred care, championing the measurement of outcomes that matter to consumers. 8 The use of replicable, standardised approaches adds further value, enabling data and outcomes to be benchmarked and compared, driving ongoing quality improvement. To date, such initiatives have been condition-specific, 9 however in clinical practice, there is often a need and desire to collect data and outcomes across patient groups. Commonalities have been identified across rehabilitation minimum data sets and core outcome sets supporting the feasibility of such an approach. 9 Therefore, we aimed to explore how ‘successful rehabilitation’ is conceptualised by key stakeholders in rehabilitation, to inform the development of a minimum dataset and core outcomes for sub-acute rehabilitation.
Materials and methods
This study used the nominal group technique 10 within a series of focus groups to explore how stakeholders conceptualise ‘successful rehabilitation’. Focus groups were held online using Zoom video conferencing software to comply with physical distancing policies in response to the COVID-19 health pandemic. Ethical approval for this research was granted by the Human Research Ethics Committees for Royal Brisbane Women's Hospital (LNR/2020/QRBW/62466), The University of Queensland (2020001248) and Griffith University (2020/378), in accordance with the National Health and Medical Research Council Statement on Ethical Conduct in Human Research.
Participants were clinicians, health service managers and consumer representatives. Clinicians and health service managers working in rehabilitation settings within the Metro North Health and Hospital Service in Brisbane, Australia were invited to participate. Recruitment materials were disseminated through the health service rehabilitation networks. Following expressions of interest, participants were purposively sampled to generate maximum variation in: rehabilitation speciality (in areas of: stroke, major trauma/burns, amputation, geriatrics, deconditioning post-acute illness, acquired brain injury, progressive neurological conditions, spinal cord injury); setting (inpatient, community-based); discipline (allied health, nursing, medicine); and gender (female, male). Consumer representatives were trained representatives working within relevant consumer advocacy groups or health services and included both people with the lived experience of rehabilitation and caregivers. Consumer representatives were recruited from rehabilitation and disability non-government organisations (NGOs) in Australia. Participants were required to be (a) at least 18 years of age at day of consent; and (b) working within an organisation that supports consumers to access rehabilitation services. Consumer representatives were also purposively sampled to ensure maximum variation across rehabilitation speciality areas; and gender. Participants were provided with a written information sheet and consent form prior to attending the focus groups. At least one week was allowed for each eligible participant to decide whether to participate. A standard process for obtaining informed consent was followed.
One focus group was held with each stakeholder group in July 2020. Participants were offered a Zoom trouble-shooting session with a member of the research team prior to their group session to mitigate any potential issues with the use of the technology. Participant privacy in the online environment was protected using Zoom security features, for example, the ‘waiting room’ function was used to control entry to the focus group and the meeting was ‘locked’ once all attendees were present. Each focus group took approximately 1.5 to 2 h and sessions were recorded to allow for data checking.
The lead author (SW) facilitated all focus groups using the nominal group technique, with assistance from co-authors AB and AY. The nominal group technique is a structured group decision-making process that has been used to determine priorities in healthcare.11–13 It is an effective and efficient data collection research method that supports equal participation with a turn-taking approach between group members. 14 The nominal question, ‘What does successful rehabilitation look like?’, was provided to all participants prior to their group to allow time for reflection and was again presented at the beginning of each focus group. A multi-stage process followed: (1) silent generation of ideas in response to question; (2) round-robin presentation of ideas; (3) clarification and grouping of ideas; and (4) individual prioritisation of top five responses. Clinicians and managers used an anonymous online survey to independently rank their top five responses, allocating a total of 100 points across these items to indicate relevant importance. Consumer representatives ranked and distributed points across their top five items in Zoom breakout rooms. This allowed the research team (SW, AY, AB) to support consumer representatives with communication, cognitive or physical impairments, as required. Support was tailored to individual needs to ensure participants had equitable access to the information, for example, reading items aloud for participants with reading comprehension difficulties due to stroke and aphasia or transcribing responses for participants with physical impairments which made typing difficult.
The raw data (prioritised ideas) from each group were analysed. Points allocated to each idea were summed to produce a ranked list for each group. This was followed by calculation of: the relative importance, ranked priority by percent and voting frequency as per the method of McMillan and associates. 15 To allow comparison across groups, the prioritised ideas from each group were analysed using qualitative content analysis. 16 Content analysis was performed by authors AB and SW with input from all co-authors. Familiarisation with the dataset was achieved through repeated readings and review of audio recordings and notes. Similar ideas were then grouped into categories and further organised into larger themes. As per McMillan et al., 15 a secondary analysis was conducted, involving calculation of the sum of scores, ranked priority, relative importance, ranked priority by percent and voting.
Results
A total of 31 participants participated in one of three focus groups. Participants included 15 clinicians (73% female), 9 health service managers (56% female) and 7 consumer representatives (43% female). Participant characteristic data are detailed in Table 1. Maximum variation was achieved for all sampled variables except area of rehabilitation expertise. Clinicians/managers with expertise in burns and consumer representatives with expertise in burns or amputation were unable to be recruited. One of the consumer representatives only participated in the final ranking stage and not the focus group discussion as they were not able to attend the scheduled discussion time.
Participant characteristics (n = 31).
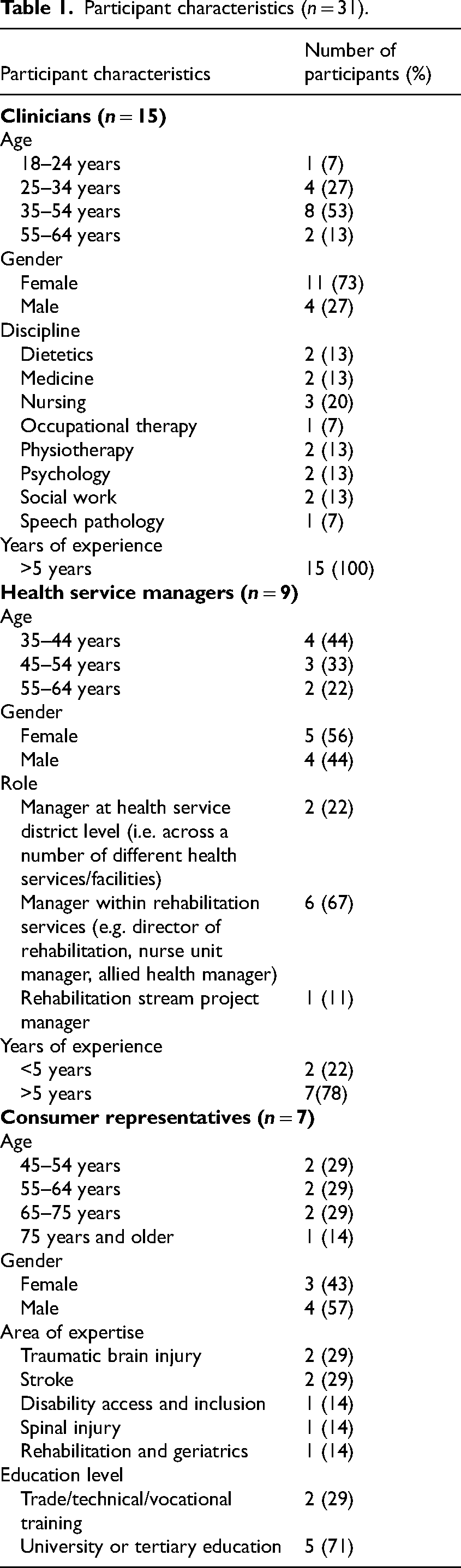
Participant characteristics (n = 31).
Clinicians generated 38 items to describe ‘what successful rehabilitation looks like’, prioritising 24 items in the ranking stage. Health service managers generated 29 items and prioritised 21, and consumer representatives generated 27 items with 18 prioritised. The top five items for each stakeholder group are presented in Table 2.
‘What does successful rehabilitation look like?’: top 5 ideas prioritised by each stakeholder group.
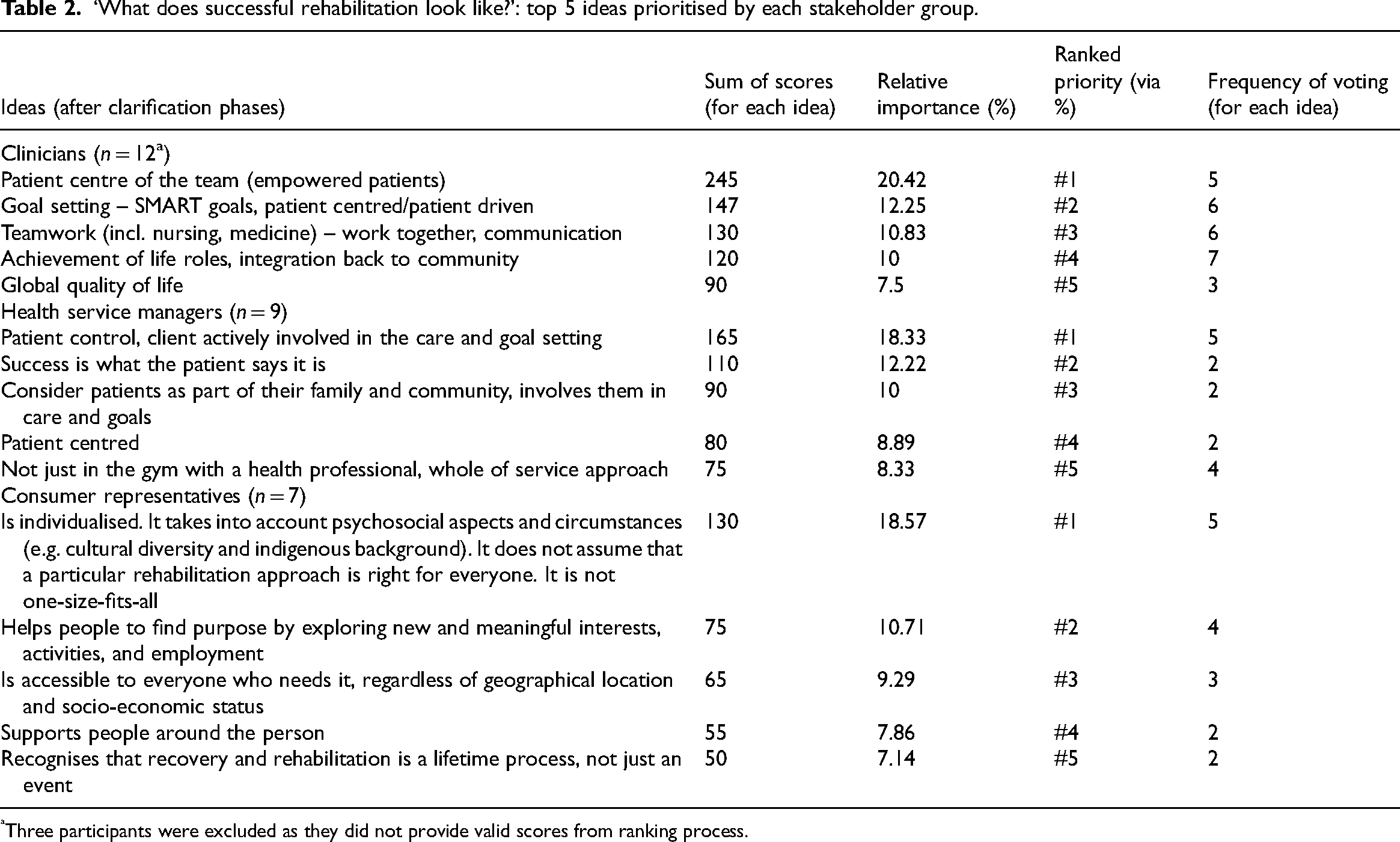
Three participants were excluded as they did not provide valid scores from ranking process.
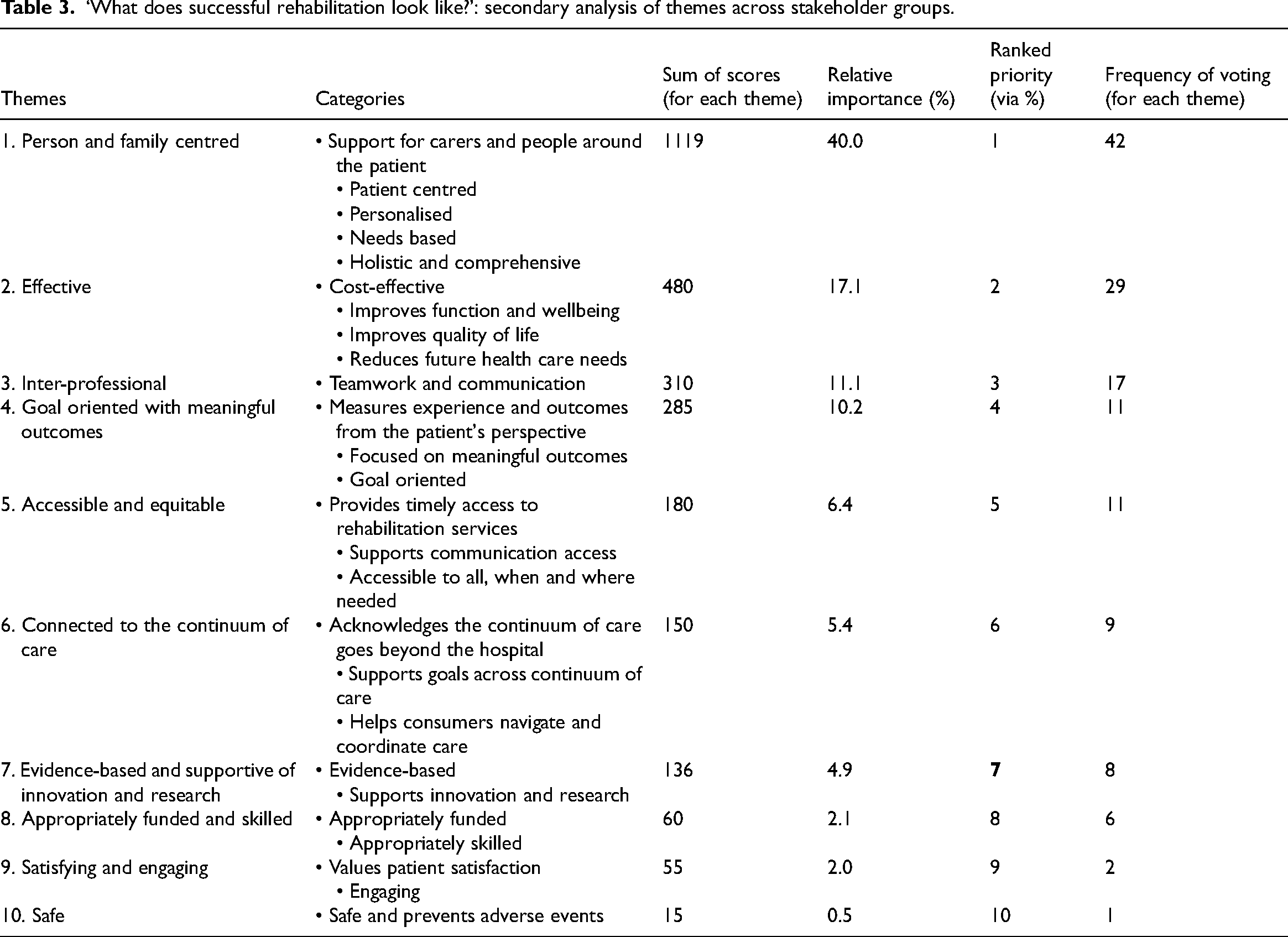
All items prioritised by clinicians, managers and consumer representatives were combined and analysed qualitatively using inductive content analysis. Ten themes and 26 categories were generated (see Table 3).
‘What does successful rehabilitation look like?’: secondary analysis of themes across stakeholder groups.
Across stakeholder groups, participant responses most frequently related to the notion that successful rehabilitation is person and family centred. Participants emphasised that rehabilitation should be individualised, and that the individual should be considered within the context of their family and community. Managers spoke about the importance of patients being actively involved in goal setting and rehabilitation, emphasising the importance of education and health literacy for successful self-management.
So really the client is actively involved in their care. So not just linked, but actually making the goals…the client needs to know about their condition…to really help with their self-management of it. (Health service manager).
Throughout our journey, it's become very apparent to me how important it is to have an advocate for you, particularly in the early days …. You're not thinking straight. You need somebody there to actually digest the information, make sure things happen. (Consumer representative)
Successful rehabilitation is effective
All three stakeholder groups described successful rehabilitation as being cost-effective and effective in improving function, well-being and quality of life. Managers described that rehabilitation had been successful, ‘when the individual has reached a level of function or ability, to live the life they want to live’. Clinicians discussed effectiveness in terms of ‘high value care’ describing successful rehabilitation as balancing improvements in psycho-social outcomes including emotional well-being, social connectedness and adaption to a new normal, with cost. Consumer representatives emphasized that while recovery encompassed physical improvements, it also extended beyond this to include improvements in well-being and quality of life and adaptation to a new way of being.
Physical aspects, and it is not just physically improving, but adapting to what you currently have. So to achieve the best possible quality of life by adapting to your limitations. (Consumer representative)
Successful rehabilitation is inter-professional
All three stakeholder groups defined successful rehabilitation as being inter-professional. Clinicians emphasised the importance of collaboration across disciplines, with the patient being central to the team.
An interdisciplinary team. We’re not working in discipline silos, there's a lot of cross over and working on goals together. And obviously the patient or the client being a key member of the team. (Clinician)
Successful rehabilitation is accessible
Stakeholders emphasised that equitable access to timely specialist rehabilitation was often inhibited by factors including geographical location and communication disability. For all stakeholder groups, accessible care, received at a time and place that suited the individual was important. Consumer representatives highlighted the importance of achieving equitable patient outcomes where, ‘everyone is able to reach their potential irrespective of location and age’. Clinicians discussed how access influences rehabilitation success:
Access… And that could be access into rehabilitation, whether that be specialists or from a rural point of view for example. But also for those people with, say, communication impairments … making it possible for them to access information in a way that is meaningful to them to make rehab successful. (Clinician)
Successful rehabilitation is goal oriented with meaningful outcomes
All three stakeholder groups emphasised that successful rehabilitation should be goal-oriented and produce meaningful outcomes. Consumer representatives stated that goals should be ‘personally relevant’ and ‘defined in partnership with the patient’. Managers stated that successful rehabilitation should be ‘outcome driven’ and should include measurement of experience. Clinicians highlighted the importance of an iterative goal setting, therapy, outcome measurement process and feedback and review: The opportunity for the client to provide feedback, so not only be involved at the beginning to determine what they would like to work on, but for it to be really successful rehab, it's that ongoing review. (Clinician)
Successful rehabilitation is connected to the continuum of care
Participants recognised that the continuum of care goes beyond the hospital setting. Managers stated that successful rehabilitation, ‘occurs seamlessly across the continuum from acute through sub-acute and community’. Consumer representatives perceived that successful rehabilitation is when consumers receive assistance to navigate and coordinate their care within the community. Clinicians highlighted the importance of transitions between services and locations in the continuum of care noting that, ‘Successful rehab is having a successful transition’.
Successful rehabilitation is evidence-based and supportive of innovation and research
Stakeholders emphasised that successful rehabilitation was based in evidence, and supportive of quality improvement, innovation and research.
Ongoing quality improvement and comparison with peer groups— benchmarking and also fostering research. (Health service manager)
The sessions need to be evidence-based. Sufficient to achieve an outcome. (Consumer representative).
8, 9, & 10. Successful rehabilitation is appropriately funded and skilled; satisfying and engaging; & safe
Stakeholders emphasised the need for appropriately funded services, skilled clinicians, and services that are satisfying, engaging and safe. Managers spoke about appropriate resourcing and staff skill mix, ‘… resources, definitely, but also having the appropriately skilled interdisciplinary team to provide that care for the client’. Consumer representatives spoke of the importance of the therapeutic relationship, stating that successful rehabilitation needed to be, ‘Engaging. You like the person that you are dealing with’.
Discussion
This study aimed to explore how ‘successful rehabilitation’ is conceptualised by consumer representatives, clinicians and health service mangers in rehabilitation to inform the development of a minimum dataset and core outcomes for sub-acute rehabilitation. Viewed through a measurement lens, participants conceptualised ‘successful rehabilitation’ in terms of process, structure and outcome, aligning with a Donabedian approach to measuring health service quality. 17 This model posits that there is a need to measure and understand each of these three domains, and how they interact, to improve the quality of health care. 7
Overwhelmingly, successful rehabilitation was linked to the presence of patient and family centred care. There is no universally accepted definition for this concept and variations of patient/client/person/consumer/family-centred care are found throughout the literature. While each term possesses subtle differences in meaning, the core component is the same; that is, the person/s’ values and preferences are elicited and used to guide their care. 18 Patient-centred care in rehabilitation has been shown to have a significant impact on rehabilitation satisfaction, 19 treatment adherence, 20 and length of stay and cost. 21 Participants in the current study extended the notion of patient centred care to be inclusive of families. This reflects findings from Wade, 6 whose synthesis of evidence to establish an empirical definition of rehabilitation identified person and family centredness as a key component of successful rehabilitation. A number of person-centred measurement instruments have been developed for acute, long-term care, and home settings 22 and the identification or development of a measure of person-centred care for rehabilitation and its routine use, may help to ensure the implementation of patient and family centred practices within rehabilitation services.
Interprofessional practice (professionals of different disciplines providing services collaboratively 23 ) was also key to conceptualising successful rehabilitation. Reeves et al. 24 state that interprofessional practice occurs in multiple forms – as collaboration, as coordination and as networks – distinguished by the degree of shared team identity, clarity of roles, interdependence, integration and shared responsibility. Consequently, a concerted effort may be required to remove traditional hierarchies and siloed governance structures and promote interprofessional communication and teamwork to achieve this aspect of ‘successful rehabilitation’. Measuring this construct may also necessitate a move beyond the discipline specific measures of process and outcome evident in existing datasets. 9
Rehabilitation is recognised as a life-long journey, on the basis that improvement can continue in various forms beyond what was formerly believed to be a time-limited ‘window’ for recovery. 25 Continuity of care is logistically challenging to measure across different providers, and much rehabilitation data collection focusses on the immediate outcomes of episodes of care rather than longer-term outcomes. 9 Like interprofessional practice, continuity of care cannot be singularly defined or measured; it encompasses the transfer of information between care providers, relational consistency between patient and clinician and management consistency across the continuum of care. 26 Given that better continuity of care, measured by patient report, has also been associated with better interprofessional teamwork, these constructs may be appraised through complementary measures. 27
Our findings support the well accepted notion that evidence-based practice is required for successful rehabilitation. Adherence to evidence-based recommendations in clinical practice is a guiding principle across nursing, allied health and medical disciplines. However, there are many known barriers to the implementation of evidence in practice, including resource, time and training limitations.28,29 Tailored intervention strategies, including education, decision tools and audit with feedback, show promise in improving adherence to clinical practice guidelines. 30 Given these challenges, there may be a need to prioritise recommendations for implementation. In the field of stroke, this has been done using processes that are inclusive of both consumers and health professionals. 31
In the current study, participants highlighted the importance of a health system that is accessible and appropriately funded and skilled. Timely, equitable access to high quality health care and assistive devices has been identified as a priority area by the WHO Rehabilitation 2030 initiative. 4 Access to rehabilitation is known to vary significantly based on a range of socioeconomic factors including income (personal, country) and geographical location, as well as variation in entry criteria related to severity and anticipated discharge destination. 32 Accessibility to rehabilitation is currently not commonly measured in rehabilitation datasets, however, some national clinical registries measure the date the person is ready for rehabilitation (e.g. Australasian Rehabilitation Outcomes Centre clinical datasets; UK Rehabilitation Outcomes Collaborative national database; Canadian Institute for Health Information health indicators) allowing the wait time for rehabilitation to be calculated (e.g. Riksstroke: The Swedish Stroke Register). Routine data collection may assist understanding of the models of care which best support timely access to rehabilitation (e.g. home or community-based rehabilitation, telerehabilitation, mHealth).
Beyond structure and process-related parameters, participants equated effective rehabilitation with cost-effectiveness, improvements across biopsychosocial domains of health, and safety. The notion of safety encompassed the provision of high-quality professional services and the prevention of physical and psychological adverse events, but also extended to concepts such as culturally safety (i.e. respectful of differences in ethnicity, spirituality, sexuality and other forms of identity). As such, valid measures of safety may require a combination of quantitative, semi-quantitative and qualitative tools, such as critical incident audits and consumer focus groups. 33
A strength of the current study is the inclusion of multiple stakeholder groups, with separate focus group sessions held to reduce power imbalance and desirability bias. Stakeholder groups varied in size, with consumer representatives fewest in number, however this was a reflection of the number of variables sampled for each group. Maximum variation was achieved for all variables except area of rehabilitation expertise and again this is a limitation of the current research. Also noteworthy is that the consumer representatives who participated in this research are likely among a proactive group who are inclined towards agency in their own healthcare. As such, their views may not be entirely representative of, or generalisable to, individuals who prefer to be more passive recipients of healthcare. Clinician and health service managers were recruited from metropolitan settings. Therefore, although our findings highlight issues of geographical access and continuity of care, the experiences of those living in regional and remote areas may not be fully represented. The use of videoconferencing for our focus groups allowed this research to continue during COVID-19 physical distancing restrictions. While efforts were made to support the participation of all interested participants (e.g. with provision of technology trouble-shooting sessions and individual support for consumer representatives), we acknowledge that the lack of an in-person option may have deterred the participation of some.
This study has explored how stakeholders in rehabilitation conceptualise ‘successful rehabilitation’. Our findings indicate that provision and receipt of person and family centred care was by far the most important indicator of successful rehabilitation; however, rehabilitation measurement should also include indicators of structure, process, outcome and experience, and be conducted at multiple time-points. Further research is needed to define the outcomes that should be routinely measured to determine whether high value care is being provided in rehabilitation settings, and whether subsequent quality improvement processes are required.
Clinical Messages
Patient and family centred care is a very important indicator of rehabilitation success. Services should measure patient/family centredness as a quality indicator.
Effectiveness of rehabilitation should be measured in terms of both cost-effectiveness and improvements across biopsychosocial domains of health.
Interdisciplinary practice, collaborative goal setting and attainment and family/carer experience are other important indicators of successful rehabilitation which can be measured by rehabilitation services.
Structure, process, outcome and experience measures should be collected at multiple timepoints to capture rehabilitation success across the continuum of care.
Footnotes
Acknowledgements
The authors acknowledge the time and expertise that consumer, clinicians and health service manager participants contributed to this research, and assistance from Sonia Sam with the recruitment of clinician participants.
Author contributions
KC conceived the study; SW, AY, AB recruited participants and collected and analysed data. SW led the preparation of the manuscript with assistance from AY, JL and BC who drafted sections of the manuscript and provided critical review. All authors approved the final version for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sarah Wallace is supported by a National Health and Medical Research Council (NHMRC) Emerging Leadership Investigator Grant (1175821). This research has been conducted with funding support from a Menzies Health Institute Queensland (Griffith University) 2019 Collaborative Interdisciplinary Grant and a Metro North Hospital and Health Service and University of Queensland Collaborative Research Grant (CRG-183).