
Abstract
Objectives
To (1) reflect on challenges to the practice of person-centred rehabilitation; and (2) propose opportunities for the development of person-centred rehabilitation.
Challenges
Person-centred practice has received widespread endorsement across healthcare settings and is understood to be an important, positive approach in rehabilitation. However, the rhetoric of this approach does not always translate meaningfully into practice. Emphasis on patient choice, patient involvement in decision making, and increasing patient capacity for self-management have become a proxy for person-centred rehabilitation in lieu of a more fundamental shift in practice and healthcare structures. System (e.g. biomedical orientation), organisational (e.g. key performance indicators) and professional (e.g. identity as expert) factors compete with person-centred rehabilitation.
Opportunities
Four key recommendations for the development of person-centred rehabilitation are proposed including to: (1) develop a principles-based approach to person-centred rehabilitation; (2) move away from the dichotomy of person-centred (or not) rehabilitation; (3) build person-centred cultures of care in rehabilitation; and (4) learn from diverse perspectives of person-centred rehabilitation.
Conclusion
Fixed assumptions about what constitutes person-centred rehabilitation may limit our ability to respond to the needs of persons and families. Embedding person-centred ways of working is challenging due to the competing drivers and interests of healthcare systems and organisations. A principles-based approach, enabled by person-centred cultures of care, may achieve the aspirations of person-centred rehabilitation.
Introduction
Person-centred rehabilitation has long been advocated for. 1 The rhetoric of person-centred rehabilitation is strong. It is embedded in health policy, professional competencies, and service frameworks.2–4 However, it is not always experienced as such by people and families accessing rehabilitation and research suggests the full scope and potential of person-centred rehabilitation is yet to be realised.5–8 We are two researchers who have undertaken research to contribute to theory and evidence in person-centred rehabilitation from different perspectives. We have each worked with rehabilitation organisations and providers to support the implementation of person-centred rehabilitation in our respective countries. In this paper, we draw from our knowledge and experience to reflect on challenges to the practice of person-centred rehabilitation. We engage with existing evidence to examine the connection between theory and practice and identify opportunities for translating the rhetoric of person-centred rehabilitation into practical action.
We have organised this paper into two sections. In the first section, we focus on the concept and practice and the system and organisational culture of person-centred rehabilitation. We discuss the diversity of perspectives on the concept of person-centred rehabilitation and the consequences for person-centred rehabilitation. We then consider the system and organisational challenges which constrain person-centred rehabilitation. This section is not an exhaustive review of the literature on person-centred rehabilitation. Rather we draw attention to a range of existing theory and practice to illustrate challenges to the practice of person-centred rehabilitation.
In the second section, we offer four opportunities for the continued development of person-centred rehabilitation so it can be implemented to its full potential. These recommendations are not meant as quick fixes to cultural and systemic assumptions and practices. Rather, they are meant as a possible way forward to enable person-centred rehabilitation in a healthcare system with competing drivers and interests. Figure 1 provides a summary of the key points addressed in each of these sections.
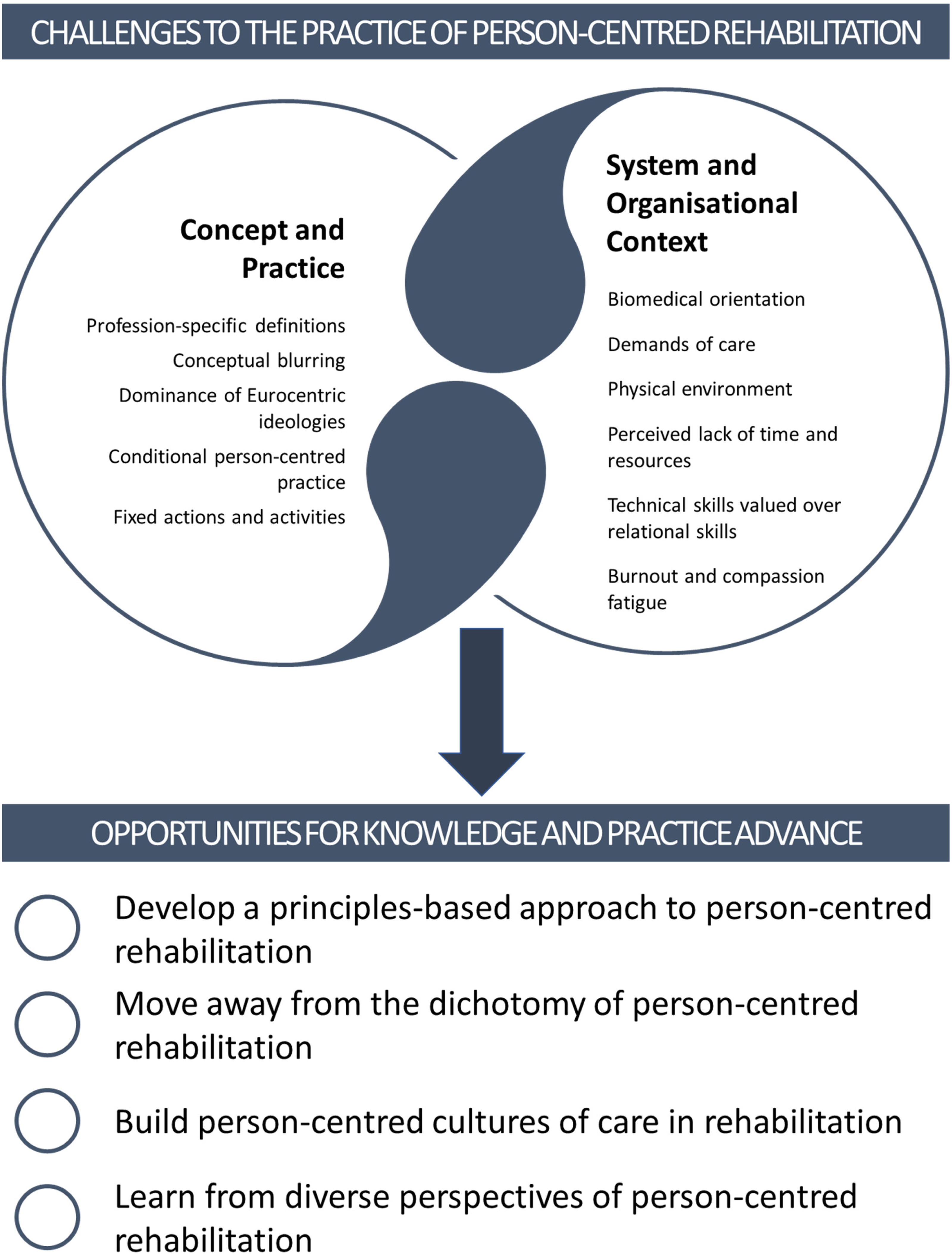
An overview of the key arguments presented in this paper.
Where our perspectives come from?
Our reflections in this paper come from our own research6,7,9–16 and by listening to the experiences of people and families accessing rehabilitation and their practitioners. At a theoretical level, we are inspired by a field called critical rehabilitation studies.12,17–22 In critical rehabilitation studies, researchers make visible and explore taken for granted assumptions inherent in everyday or common clinical practices and disciplines. For instance, Hammell22,23 pointed out the tendency to accept rehabilitation professional assumptions as truth without critical reflection, and highlighted tensions and inconsistencies between the ideology and practice of client-centredness. 22 Similarly, Gibson et al.17,18 showed that rehabilitation professionals’ assumptions about independence may be counter to a person-centred approach, because their views are individualistic rather than treating the person-served within the cultural and relational context in which they live and received their care. Other critics have argued that some people such as those with cognitive or communicative impairment may be inadvertently excluded from person-centred rehabilitation 8 because of the emphasis on promoting autonomy, patient choice, and active involvement of clients in decisions about their care. 24
Challenges to the practice of person-centred rehabilitation
The concept and practice of person-centred rehabilitation
There are a range of competing definitions, concepts, and disciplinary-based frameworks for person-centred rehabilitation. In both rehabilitation research and practice, we have been at risk of working independently, without collaboration and in competition with each other in our endeavour to advance person-centred rehabilitation. This has likely hindered continued development in the practice of person-centred rehabilitation.
There is an extensive body of research aiming to conceptualise, define, operationalise, measure, and evaluate person-centred rehabilitation.25,26 A wide range of models have been established, including models specific to profession, diagnosis or setting.27–31 These efforts support the operationalisation of person-centred rehabilitation in different settings, which can be helpful in some instances. However, profession- or diagnosis-specific models may have limited application in rehabilitation which is argued to be a complex intervention involving a multidisciplinary team, and where multimorbidity is common. 32 Further, the independent development of multiple models reduces the likelihood of negotiating a common understanding of person-centred rehabilitation.
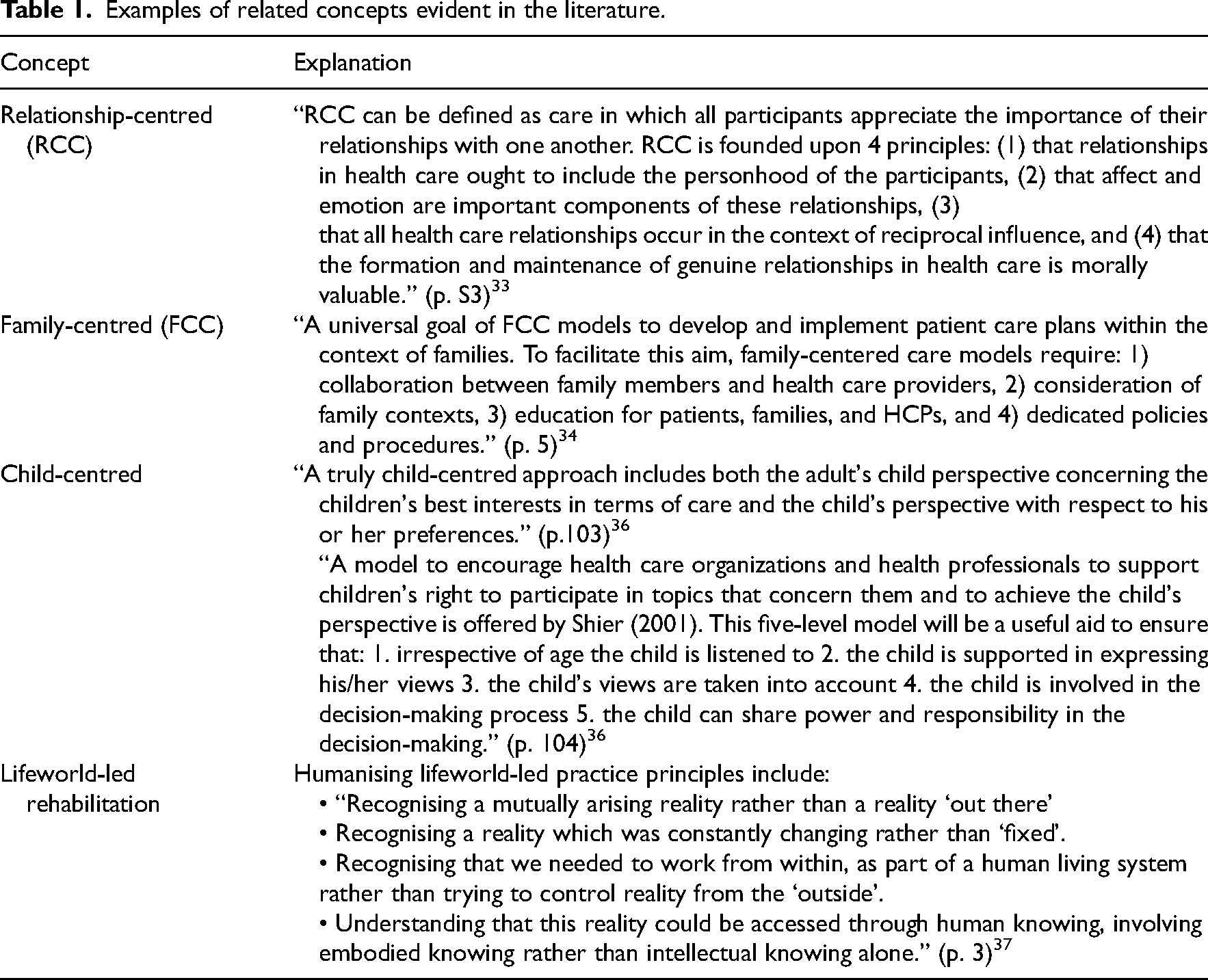
The range of perspectives on person-centred rehabilitation makes it difficult to establish a shared sense of what constitutes person-centred rehabilitation and how to operationalise that for clinical practice. This is compounded by the availability of multiple, overlapping concepts. For example, the literature refers to relationship-centred, 33 family-centred34,35 and child-centred 36 care, all of which overlap with the central tenants of person-centred rehabilitation (see Table 1). There are also new approaches being developed, such as lifeworld-led rehabilitation, 37 in response to the perceived shortcomings of existing models or the implementation of person-centred rehabilitation. These ideas, concepts and approaches have increased conceptual blurring and hampered improvement in defining, refining, and implementing person-centred rehabilitation.
Examples of related concepts evident in the literature.
Consistent with the broader rehabilitation evidence base, 38 most existing research exploring person-centred rehabilitation draws on western perspectives. Of the 170 papers included in our scoping review, there were no included papers engaging with indigenous perspectives of person-centred rehabilitation.25,26,39 This is likely to have an effect on how person-centred rehabilitation is understood and implemented in practice. For example, Eurocentric ideologies of individualism and independence are pervasive in rehabilitation17,18 and may impact how ‘personhood’ may be understood and conceptualised. 40
While the ideal of person-centred rehabilitation has widespread support, in practice rehabilitation professionals find it challenging. Several tools and practices have been developed to support person-centred ways of working in rehabilitation. For example, there is extensive research aiming to optimise person-centred approaches to goal planning,41–45 engagement,46–49 therapeutic relationship,50–60 communication,61–64 education,65,66 interdisciplinary teamwork 15 and self-management67–69 – all aiming to support the practice of person-centred rehabilitation through a focus on transdisciplinary rehabilitation processes.
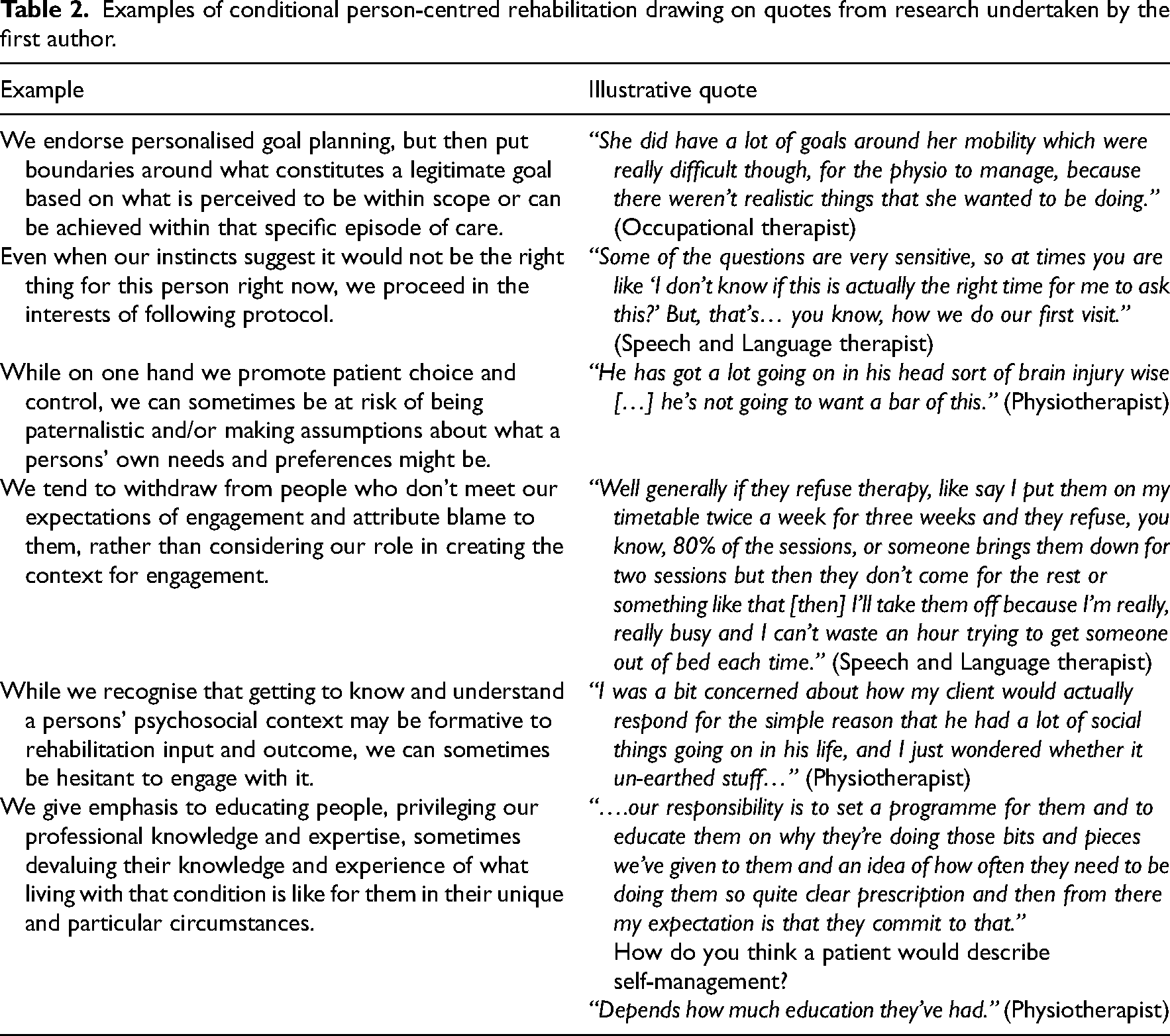
Despite this, health professionals find it difficult to balance perceived professional responsibilities with the needs and preferences of persons and families accessing rehabilitation,5,41,42 struggle to let go of their role as expert,7,67,69 experience tensions in managing professional boundaries, 50 and feel limited in their ability to meet their own aspirations for care due to competing service demands.69,70 Language such as ‘benign dictators’ 69 and ‘benevolent manipulation’ 6 has been used to articulate such tensions, argued to be a result of the biomedical model.7,69 Our reading of this literature is that, at best, we currently implement a form of conditional person-centred rehabilitation. Table 2 provides some illustrative examples of how conditional person-centred rehabilitation can materialise in practice.
Examples of conditional person-centred rehabilitation drawing on quotes from research undertaken by the first author.
This evidence suggests we may have been at risk of underestimating the complexity of putting person-centred rehabilitation into practice. We have fallen into a pattern of reducing person-centred rehabilitation down to a set of key actions and activities centred on activating people to be involved in their rehabilitation. As such, fixed actions and activities, such as involving patients in decision making about their care and increasing patient capacity for self-management, have become a proxy for person-centred rehabilitation in lieu of a more fundamental shift in practice and healthcare structures.
Led by Jesus, 9 we recently carried out a thematic synthesis of the literature. In our findings, we conceptualised person-centred rehabilitation as a way of thinking about, organising, and delivering rehabilitation which can be enabled and enacted across multiple layers (person-professional dyad, micro-system and macro-system), each with its own set of attributes. These findings highlight the importance of moving beyond what happens in the therapeutic encounter, to include the role of structures and processes that may constrain or make possible person-centred rehabilitation.
The system and organisational context of person-centred rehabilitation
Embedding person-centred rehabilitation into healthcare delivery systems of care is challenging. Nonetheless, emerging evidence demonstrates the potential beneficial impacts of person-centred rehabilitation for patients, professionals, and teams. These benefits highlight the broader impact and value of person-centred cultures of care.
Healthcare systems are generally organised hierarchically and prioritise cost efficiency for the organisation. 71 They often draw from the biomedical model of care 72 wherein clinicians are given more authority and power compared to patients 7 and patients often accept medical paternalism. 73 Although clinicians are treated as experts, they are not necessarily supported to provide high quality, person-centred services. 74 In other words, most healthcare organisations’ structures and processes – such as policies, professional obligations and responsibilities, practice conventions, clinical documentation, service drivers – do not value the perspectives and experiences of clinicians or their patients. 6 If we want to provide services that are more person-centred, we need to challenge the usefulness of the biomedical model and reimagine structures and processes 75 which support, enable and make person-centred rehabilitation possible.
Often the demands of care compete with the practice of person-centred rehabilitation. For example, in inpatient stroke rehabilitation there is increasing pressure on services to reduce length of stay. Focusing on length of stay as a metric of service performance (structure) leads to a focus on reducing impairment and optimising function (process) for the primary purpose of getting someone safe to discharge (outcome). In this context, rehabilitation is time-limited, focused on what is achievable from the professionals’ perspectives and in the timeframes they have. 41 It contributes to professionals privileging ‘realistic’, 76 service-centric, discipline-specific goals 41 over what may matter to the person (similar to the first example provided in Table 2). This can have the effect of limiting people's hope and sense of possibility for the future despite this being a critical resource for recovery.76–78
The physical environment can also play a role in enabling or hindering person-centred rehabilitation.79,80 Recent research drawing on experience-based co-design with patients and professionals in stroke units introduced changes in the environment in collaboration with staff and patients. 80 For example, changes included reclaiming shared spaces (which had become storage facilities or staff meeting spaces) so that patients could socialise with each other and their visitors, reorganising the ward and reducing clutter, painting corridors and introducing artwork, and creating space for personal belongings and pictures at the bedside. Staff and patients reported that these changes made the ward feel more inclusive, led to increased activity opportunities for patients, and changed the nature of bedside conversations prompted by the items from home.
Healthcare professionals often highlight that time (or lack of) is a barrier to person-centred rehabilitation.73,81 However, person-centred rehabilitation does not necessarily need to take more time. 70 Rather, the values of person-centred rehabilitation can be integrated into all that we do and embedded in how we work. Instead of focusing on how much time we have (or don't have), it may be important to examine how we prioritise and use our time (and what demands that we prioritise our time in that way). The inpatient stroke rehabilitation example above highlights that our structures contribute to some ways of working being prioritised (e.g. service-centric, discipline-specific processes and outcomes) over others (e.g. person-centred processes and outcomes) in the time we have.
Ideas about what constitutes the core of rehabilitation practice are embedded in health curricula and organisations – where ‘hard’ technical skills are routinely prioritised over ‘soft’ relational skills – rather than promoting a more integrated way of working that weaves them together. Indeed, there is an inferred hierarchy in the language of ‘hard’ versus ‘soft’. Relational skills are critical to the implementation of person-centred rehabilitation. However, they are often positioned as innate, or an ingrained personality trait, rather than something that can be taught, developed, and nourished. This inevitably results in limited investment in the ongoing growth and development of relational ways of working in education and practice.79,81 This may in turn influence how person-centred rehabilitation is positioned in everyday rehabilitation practice, particularly in the context of other competing demands and limited time and resources.
Rehabilitation professionals report experiencing work-related stress and burnout.82–86 Compassion fatigue, characterised as a stress response in health professionals ‘culminating in a decrease in compassionate feelings towards others because of an individual's occupation’ (p. 10) 87 highlights the potential for a direct relationship between work-related stress and one's capacity to offer person-centred rehabilitation services. This relationship may be influenced by intra-team and organisational factors. For example, support and cooperation, shared understanding and goals, mutual respect and flexibility and sharing tasks are relationship characteristics that enhance person-centredness within interdisciplinary teams. 15 Similarly, patients have observed that when professionals treat each other in person-centred ways, their interactions appear less hierarchical and there is a greater sense of interprofessional congruity. 81 Implementing person-centred ways of working may be beneficial for professionals and rehabilitation teams, potentially countering work-related stress.
In summary, person-centred practice has received widespread endorsement across health settings and contexts, and is understood to be an important, and positive approach in rehabilitation. However, the rhetoric of person-centred rehabilitation does not always translate into clinical practice. Research highlights a tension between organisational, system and professional factors and attending to the needs and preferences of persons.
In the following section, we highlight four opportunities for the ongoing development of person-centred rehabilitation.
Opportunities for the continued development of person-centred rehabilitation
In this section, our recommendations draw from several literatures and in a certain sense are not novel. Indeed, Restall et al. touched on many of the points we make in their framework of strategies for client-centred practice published 20 years ago. 88 Our suggestions are intended as focused reminders and practical steps that we can take to address challenges to the implementation of person-centred rehabilitation. Our intention is for these suggestions to support rehabilitation professionals and organisations reimagine how they may enable person-centred rehabilitation in diverse settings and communities. In this sense, our work follows current calls for unpacking how social and political determinants of health impact our lives, decolonising clinical practice, resisting neo-liberal policies that ration care, and reimagining healthcare that embraces disability justice.89,90
Develop a principles-based approach to person-centred rehabilitation
Attempts to reduce person-centred rehabilitation to a fixed set of behaviours have resulted in a transactional approach to person-centred rehabilitation. 91 Greater recognition of the multidimensional nature of person-centred rehabilitation – which is both person- and context-bound – would help us move beyond person-centred rehabilitation as a particular set of actions or behaviours. Instead, we suggest focusing less on ‘what’ constitutes person-centred rehabilitation and more on ‘how’ we work and ‘who’ we are, and how what we do is experienced by people.
A focus on principles which can underpin ways of working, rather than specific behaviours, may enable a more responsive and reflexive way of working. A reflexive way of practicing may be best described as asking oneself the question ‘what am I doing when I am doing what I am doing?’ 92 Further, a principles-based approach doesn't rely on the cognitive or communication capacities of individuals to meet the demands of person-centred rehabilitation and so ensures the aspirations of person-centred rehabilitation can be universally available to all. We might call this a person-centred approach to person-centred rehabilitation.
There are already examples evident in the literature which are consistent with a move towards a principles-based approach. For example, findings from a secondary analysis of qualitative data examining examples of care that were experienced by persons served as person-centred 11 drew attention to an orientation to care including: recognising and responding to the context of care for persons and families; prioritising and investing in the development of relationships; building a currency of trust; and developing a belief in self and one's capabilities. In our thematic synthesis of literature exploring person-centred rehabilitation 9 we identified five attributes of person-centred rehabilitation including: (1) respectful of and tailored to the person, (2) reflexive and adaptive to the situation at hand, (3) nurtures a supportive relationship, (4) focused on meanings, hope, and strengths, and (5) collaborative, empowering, and enabling. Both examples describe an approach to person-centred rehabilitation which is reflexive and responsive, rather than a pre-defined set of professional behaviours and actions.
Move away from the dichotomy of person-centred rehabilitation
Embracing the multidimensional nature of person-centred rehabilitation would also help us to move away from thinking about person-centred rehabilitation as a dichotomy – that you are either person-centred or not. Most rehabilitation providers inherently believe in the value of a person-centred approach. 91 However, conceptualising person-centred rehabilitation as a dichotomy fails to acknowledge the complexity of person-centred rehabilitation as a human endeavour, which is subject to our fallibilities and vulnerabilities and which takes place within complex and competing organisational structures and demands. We should acknowledge the potential for ‘simultaneous moments of person-centred and non-person-centred care’ (p. 2) 79 and that we may be person-centred with some people, in some contexts, on some days and not on others.
Moving away from the dichotomy of person-centred rehabilitation will allow for a more open, honest, and respectful conversation about person-centred rehabilitation. A conversation that acknowledges these complexities, and where humility is not just welcome, but necessary for continued practice advance. We could consider a continuum of person-centred rehabilitation, similar to the continuum of engagement. 93 Or, we could reconsider person-centred rehabilitation as part of a complex adaptive system 94 which enables a learning culture characterised by an ‘ability to tolerate productive tensions, learn from mistakes, support and enable innovation, maximise individual potential, and understand the interrelationship between team/system processes and the effectiveness of outcomes achieved’ (p. 2). 79
Fundamentally, this more reflexive engagement with person-centred rehabilitation may mean we are more likely to examine and address some of the tensions experienced by clinicians in the implementation of person-centred rehabilitation. It may help us to reimagine some of the central tenets of our professional identities that constrain person-centred rehabilitation. For example, critically reflecting on the what, why and how of professional boundaries, or indeed challenging the basic premise of boundary. 95 Or, extending how we think about what constitutes expertise in rehabilitation and how to retain credibility while also showing vulnerability. 96 We suggest moving beyond the dichotomy of person-centred rehabilitation is a necessary step in this reimagining.
Build person-centred cultures of care in rehabilitation
We need to make ‘person-centred moments’ an ‘everyday cultural pattern or norm’ (p. 2). 79 For this, we need to build person-centred cultures of care which enable person-centred rehabilitation (see Figure 2). This includes having a system-wide commitment to person-centred rehabilitation. Person-centred practice needs to be top-down. 81 That is, it needs to be valued and embedded within health curricula, by healthcare service organisations, and in healthcare policy. For person-centred rehabilitation to be embedded in the social fabric of what we do and how we practice, we need to develop an understanding of person-centred rehabilitation across multiple stakeholders, including funders, insurers, and policy makers.
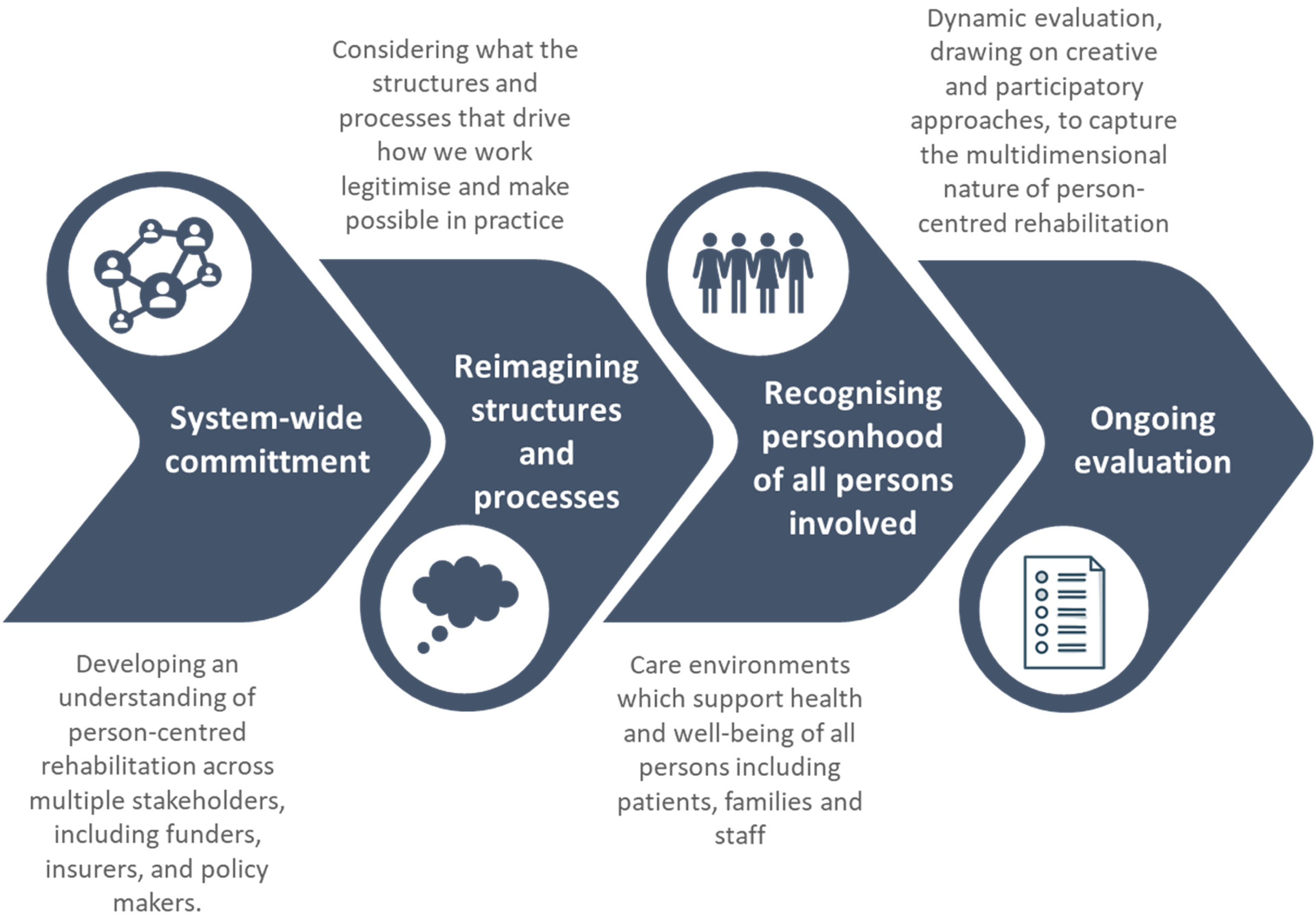
Building person-centred cultures of care.
Structures and processes that drive how we work – such as key performance indicators, documentation practices, assessment processes, discharge planning – need to be reimagined to make person-centred rehabilitation possible. Earlier we referred to the example of inpatient stroke rehabilitation and length of stay as a metric of service performance. What if the only key performance indicator was the person with stroke living the life they want to live, and the key outcome of interest their long-term health and well-being. How would this change what is prioritised in stroke rehabilitation? It is these kinds of thought experiments that help us to envisage what could be or how it could be different.
A person-centred culture of care includes recognising all persons involved in person-centred rehabilitation including patients, family, care partners, and professionals. The Senses Framework proposes that in the best care environments all parties should experience six senses, including a sense of security, belonging, continuity, purpose, achievement, and significance, 97 resonating with theories of well-being. 98 Nolan et al. provides an excellent example of how these six senses might be experienced by patients, families/care partners and professionals in dementia care.
For example, they suggest a sense of security in this context may include ‘attention to essential physiological and psychological needs and to feel safe and free from threat, harm, pain and discomfort’ (for patients), ‘to feel free from physical threat, rebuke, or censure, to have secure conditions of employment, to have the emotional demand of work recognised and to work within a supportive culture’ (for staff), and ‘to feel confident in knowledge and ability to provide good care without detriment to personal well-being, to have adequate support networks and timely help when required and to be able to relinquish care when required’ (for family/care partners). Person-centred cultures of care which value health professionals and provide resources for them to meet the demands of person-centred rehabilitation is likely to have a ripple effect for patients and family care. 74
A person-centred culture of care involves ongoing evaluation of person-centred rehabilitation.79,81 If we acknowledge the multidimensional nature of person-centred rehabilitation, we need to carefully consider how one evaluates person-centred rehabilitation, and what constitutes a good outcome. This may include the development of dynamic assessments which focus not only on whether person-centred rehabilitation was delivered, but also how it happens, what allows it to happen, what skills are needed and so on. 99 It may be that evaluations need to move beyond measures as we conventionally understand them, and move towards integrating more qualitative, creative and participatory approaches to evaluating person-centred rehabilitation. 100
Learn from diverse perspectives of person-centred rehabilitation: An example from Māori culture
Learning from diverse worldviews has the potential to enhance and augment our current understanding of person-centred rehabilitation. Angus Macfarlane, a Māori scholar, argues that when professionals develop understanding and awareness of the knowledge, beliefs, values and traditions that may be produced and perpetuated through ‘mainstream’ culture, they may be more likely to be respectful of and responsive to other cultures and perspectives. 101
In New Zealand, Māori practitioners show how Māori perspectives and tikanga (cultural protocols) can be embedded within healthcare. For example, Hinemoa Elder conceptualised paediatric traumatic brain injury as not just an injury to the brain, but an injury to wairua, which she defined as a profound sense of connectivity between Māori and all aspects of the universe. 102 She developed a framework, Te Waka Oranga, to serve as a practical tool which privileges Māori knowledge and enables families to work in partnership with clinical knowledge. 103 Similarly, Cameron Lacey, Suzanne Pitama and colleagues have developed the Meihana Model – a framework to guide clinical assessments which incorporates explicit acknowledgement of factors that may affect that journey (such a colonisation, racism, etc.) 104 – and Hui process – a framework to guide clinical interactions which mirrors cultural rituals of encounters. 105
In more recent work, Bobbie-Jo Wilson explored what matters most in the therapeutic relationship for Māori and found a sense of wairua (spirit) and hononga (connection) are fundamental for meaningful interactions for Māori, and that hononga is enabled and enhanced through whakapapa (genealogy), whānaungatanga (relationships), tikanga (cultural protocols), and in an environment which invites whānau (extended family) to engage as Māori. 59
A Māori colleague of the first author, Robert Hogg, recently explained how he draws on Mātauranga (Māori knowledge) as gifted to him by his whānau (family) and te reo Māori (Māori language) in his everyday interactions with people. 106 He used the example of ‘mokopuna’. The literal translation for ‘mokopuna’ is grandchild. ‘Moko’ is typically translated as tattoo, but the deeper meaning is related to imprint. ‘Puna’ is short for mātāpuna (source, the creator) and tupuna (ancestors). He explained therefore that ‘mokopuna’ can be translated as ‘one who wears the marks of an ancestor’. Drawing from this, whenever he interacts with others, he tries to treat them as if they are an ‘ancestor in the waiting’ to honour their whakapapa (genealogy).
These examples highlight the potentially intergenerational nature of care experiences and the importance of recognising the cumulative impact of those experiences, whether positive or negative. Putting this into practice would involve looking beyond the person as individual, to the person as part of a collective. It also highlights the importance of inviting Māori to engage as Māori (rather than requiring them to conform to western ways of being and doing) and acknowledging the tikanga (cultural protocols) of people and places and using that to guide our actions and decisions.
Indigenous perspectives have the potential to challenge and enrich how we think about and practice person-centred rehabilitation. Engaging with and being informed by these perspectives and critically engaging with the cultural and moral assumptions inherent in Eurocentric perspectives may be critical to continued advance in person-centred rehabilitation.
Conclusion
We have provided reflections on the practice of person-centred rehabilitation. This paper is not intended as an exhaustive review of person-centred rehabilitation theory and evidence and so is inherently partial. We have primarily drawn on research that has been undertaken in rehabilitation settings, rather than on person-centred care more generally. Notwithstanding this, we have provided an overview of the conceptual, practical, and organisational challenges that may hamper meaningful implementation of person-centred practice. We have proposed four key opportunities for the development of person-centred rehabilitation. We hope this will generate debate and contribute to further developments in research and practice to achieve the aspirations of person-centred rehabilitation in contemporary rehabilitation practice.
Clinical messages
Fixed assumptions about what constitutes person-centred rehabilitation may limit our ability to respond to the needs of persons and families.
Person-centred rehabilitation may be enabled through person-centred cultures of care at a system level.
Diverse cultural perspectives can enrich how we think about and practice person-centred rehabilitation.
Footnotes
Acknowledgements
The authors would like to thank their colleagues and collaborators who have contributed to their thinking over the years. Both authors recently collaborated with colleagues on a scoping review and thematic synthesis of evidence on person-centred rehabilitation.9,26 Our connection through this scoping review led to the development of a joint symposium presentation at the 2020 American Congress of Rehabilitation Medicine focusing on person-centred rehabilitation. In preparation, we had the privilege of engaging in a series of in-depth and challenging discussions about person-centred rehabilitation while we debated, synthesised, and reconciled our thinking on the topic for the purpose of presentation. We both benefited deeply from this rich, collegial debate and discussion. This formed the starting point for this paper. We would like to thank the reviewers and Professor Derick Wade for his detailed feedback on our drafts and for challenging us to further refine and improve the accessibility of the ideas presented in this paper. NK would also like to acknowledge past, present and associate members of the Centre for Person Centred Research (![]() ) for ongoing debate and discussion on the topic of person-centred rehabilitation; and her colleague Robert Hogg, Associate Dean for Māori Advancement in the Faculty of Health and Environmental Sciences at Auckland University of Technology, for sharing insights from mātauranga and Te Ao Māori.
) for ongoing debate and discussion on the topic of person-centred rehabilitation; and her colleague Robert Hogg, Associate Dean for Māori Advancement in the Faculty of Health and Environmental Sciences at Auckland University of Technology, for sharing insights from mātauranga and Te Ao Māori.
Author contributions
The conceptual ideas presented in this paper were jointly developed by both authors. NK wrote the first draft of the paper, with CP contributing in a substantive way to further developing the writing. Both authors worked together to revise and refine the draft in response to feedback.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.