
Abstract
Background
Acceptance and Commitment Therapy interventions are increasing in use in neurological populations. There is a lack of information on the measures available.
Purpose
To identify and classify the measures used in Acceptance and Commitment Therapy research studies with adults with acquired neurological conditions.
Methods
PRISMA-ScR guided scoping review. MEDLINE, PsycInfo and CINAHL databases searched (up to date 29/06/2022) with forward and backward searching. All study types included. Extraction of Acceptance and Commitment Therapy process-of-change and health-related outcome measures. Outcomes coded using the Core Outcome Measures in Effectiveness Trials (COMET) taxonomy.
Results
Three hundred and thirty three papers found on searching. Fifty four studies included and 136 measurement tools extracted. Conditions included multiple sclerosis, traumatic brain injury and stroke. Thirty-eight studies measured processes of change, with 32 measures extracted. The process measure most often used was the Acceptance and Action Questionnaire (n = 21 studies). One hundred and four health-related outcome measures extracted. Measures exploring quality of life, health status, anxiety and depression occurred most frequently, and were used in all included neurological conditions. COMET domains most frequently coded were emotional functioning/well-being (n = 50), physical functioning (n = 32), role functioning (n = 22) and psychiatric (n = 22).
Conclusions
This study provides a resource to support future identification of candidate measures. This could aid development of a Core Outcome Set to support both research and clinical practice. Further research to identify the most appropriate and relevant targets and tools for use in these populations should include expert consensus, patient, carer and public involvement and psychometric examination of measures.
Keywords
Introduction
Mental health needs are commonly unmet in people with neurological conditions,1,3 and developing interventions to support wellbeing is a global research priority.4,8 Acceptance and Commitment Therapy is a trans-diagnostic approach 4 that shows promise.5,7 There is evidence, for example, trials in multiple sclerosis (MS)8,11 and traumatic brain injury (TBI),12,13 of decreased anxiety 11 and psychological distress,12,13 and increased acceptance.9,10 However, it is unclear which measures are available for process of change and outcomes.
The process of change in Acceptance and Commitment Therapy is increased psychological flexibility4,14,15; ‘…to respond to situations in ways that facilitate valued goal pursuit’. 16 Psychological flexibility is conceptualised with six facets that support or undermine its expression; the ‘Acceptance and Commitment Therapy hexaflex’ 17 and ‘in-hexaflex’ 15 , respectively (see Figure 1). A growing number of tools purport to measure this mechanism of change.
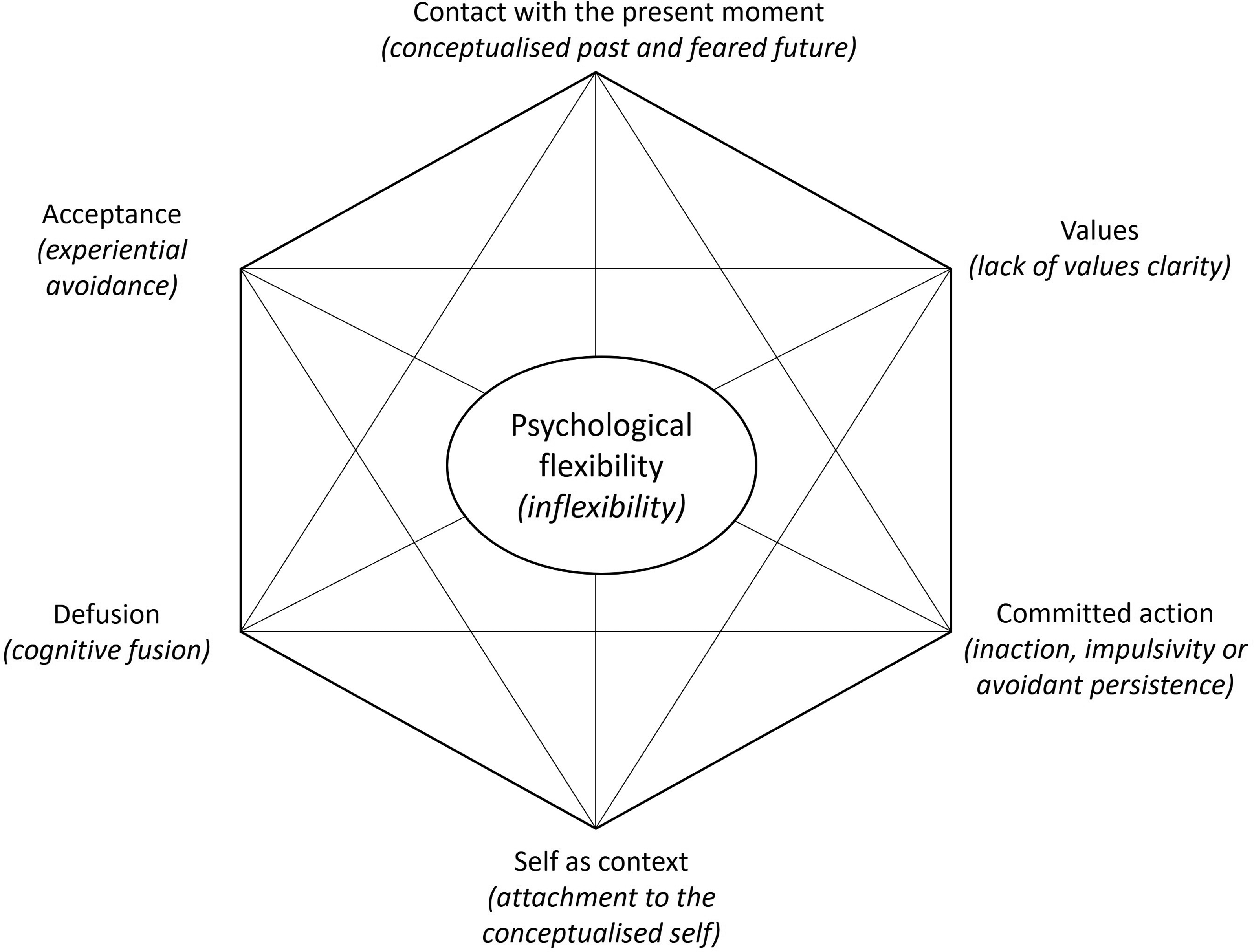
The acceptance and commitment therapy hexaflex (and in-hexaflex) 15 (adapted from copyright Steven C. Hayes. Used by permission).
Increasing psychological flexibility is posited to benefit outcomes such as depression and anxiety.14,15 Clinical trials seek standardised outcome measures to enable data pooling to guide clinical practice. 18 The Core Outcome Measures in Effectiveness Trials (COMET) initiative supports standardisation, providing a taxonomy 19 to classify outcomes used in trials. This may be useful in categorising measurement tools across different study types.
This review identified and summarised process and health-related outcome measures used in Acceptance and Commitment Therapy intervention studies with adult neurological populations, to inform the choice of measures for future studies to meet mental health needs and support well-being. 20
Objectives
Identify acquired neurological populations in which Acceptance and Commitment Therapy has been evaluated
Identify time-points at which the measurement tools were used
Identify and categorise tools used to explore Acceptance and Commitment Therapy process of change
Identify and categorise tools used to investigate health-related outcomes
Code outcome measurement tools according to COMET taxonomy 19
Methods
This review was informed by Arksey & O’Malley's five-stage scoping review methodology 20 and enhanced using strategies recommended by Levac et al. 21 Reporting was guided by the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews. 22 A protocol for this review was written in advance of data collection and retrospectively published as a pre-print at: https://osf.io/cm4kt/.
Adult population (≥18 years old) with an acquired neurological condition. Our working definition of this term was:
Acquired: not inherited, present at birth or neurodevelopmental. Neurological conditions: disorders of the brain, spinal column or peripheral nerves with a range of causes,
23
including progressive conditions, such as MS and dementia, and acquired brain injuries, such as stroke and TBI.
Interventions of interest were those identified by the original authors as: Acceptance and Commitment Therapy, based on Acceptance and Commitment Therapy or where Acceptance and Commitment Therapy is a component (i.e. interventions were included if they used other strategies as well as Acceptance and Commitment Therapy), where intervention was provided due to the presence of the acquired neurological condition. We included studies with or without a comparator.
Included studies had at least one health-related outcome or Acceptance and Commitment Therapy-related process measure. The latter are those relevant to the mechanism of change in Acceptance and Commitment Therapy – psychological flexibility, or its facets (see Figure 1). Health-related outcome measures are those targeting any aspect of health (physical or mental). Measures that exclusively explored satisfaction, adherence, usability and cost were excluded.
We included all study designs that use pre- and post-measurement of outcomes and/or processes of change, for example, clinical reports, service evaluations, case studies, quasi-experimental studies and randomised controlled trials (RCTs) and excluded reviews. We included studies with full texts available in English. Some studies used translated versions of measures published in English. The translations are reported together with the English versions and not classified separately.
Forward and backward searching was carried out with all included papers. Study authors were contacted in instances where the full paper was not available online, where additional information was required to make decisions about inclusion, or to answer methodological questions.
The umbrella term ‘acquired neurological conditions’ is not consistently used in the literature. Therefore, conditions were entered individually as keyword search terms and related MeSH terms, using the same terms as a Cochrane review with a similar population. 24 The following search terms were used to capture the intervention [“Acceptance and Commitment Therapy”/] and “Acceptance and Commitment Therapy”.mp. The search strategies were drafted in consultation with a university librarian (See Supplemental materials for MEDLINE search strategy. This was adjusted for PsycInfo and CINAHL, using differing MeSH terms.).
Identified papers were imported into Endnote and duplicates removed. Screening comprised of two stages: title and abstract, full text.
Stage one – Title and abstract phase
Initial learning phase – two members of the research team screened a small batch of papers (n = 5) and then discussed any discrepancies in screening decisions. This learning process was repeated a number of times until consistency was reached. Fifty percent of the papers were independently screened by two researchers. A moderate level of agreement (i.e. the value of kappa is ≥ 0.41 (Altman, 1991 cited in
25
) was required to proceed to the next stage. We erred on the side of inclusion if there was any disagreement between the researchers. The other 50% of total papers were screened by one researcher. As above, however disagreements were resolved by:
Discussion between the researchers aiming for consensus Contacting the study authors to request additional information Consensus discussion with all authors of this review (AB, SC, EP).
Stage two – Full text screening phase:
When measures were relevant to Acceptance and Commitment Therapy mechanisms but were not directly developed in the context of Acceptance and Commitment Therapy, information about each measure was reviewed (e.g. tool development papers), alongside data extracted from the studies. Consensus on whether to include the measure as a process measure was reached through discussion between review authors.
The process measurement tools identified were grouped according to what aspect of the Acceptance and Commitment Therapy hexaflex they measured (see Figure 1). The authors organised measures according to the hexaflex in a best-fit manner, with reference to rationale for the use of the measure provided in the included studies, papers describing the development of the measures, consulting a previous review, 28 and discussion between authors of this review.
In addition, health-related outcome measures used in any of the studies were identified and:
Categorised broadly according to what they were measuring, based on data extracted from the papers, available development papers, assessment manuals and publisher descriptions, followed by consultation between the review authors. Then; Coded according to the COMET taxonomy, which is organised into five core areas: death, physiological/clinical, life impact, resource use and adverse events. Each core area consists of a number of outcome domains. There are 38 outcome domains in total. As per guidance,
19
each measure was coded according to all relevant outcome domains addressed in the measure; achieved through reviewing every item on each measure. If measures were not freely available to review individual items, coding was done based on overall aims and any other information freely available.
In order to ensure robustness of COMET coding, Susanna Dodd (author of the taxonomy) was consulted with questions on the coding process and regarding uncertainties in classification of specific tools. Furthermore, MP independently carried out COMET coding for 10% of the measures found. MP and HF first discussed any discrepancies and then Dodd was consulted regarding any outstanding uncertainties.
Step (2) was only carried out for measures extracted from studies identified in the original 2020 search. For reasons detailed in the discussion, this step was not completed for measures identified during the 2022 updated search.
Results
Searching yielded 333 papers (see Figure 2). After duplicate removal and screening there were 54 included studies (from 65 reports). Reviewers had at least a substantial level of agreement (kappa = 0.67) at first stage screening.
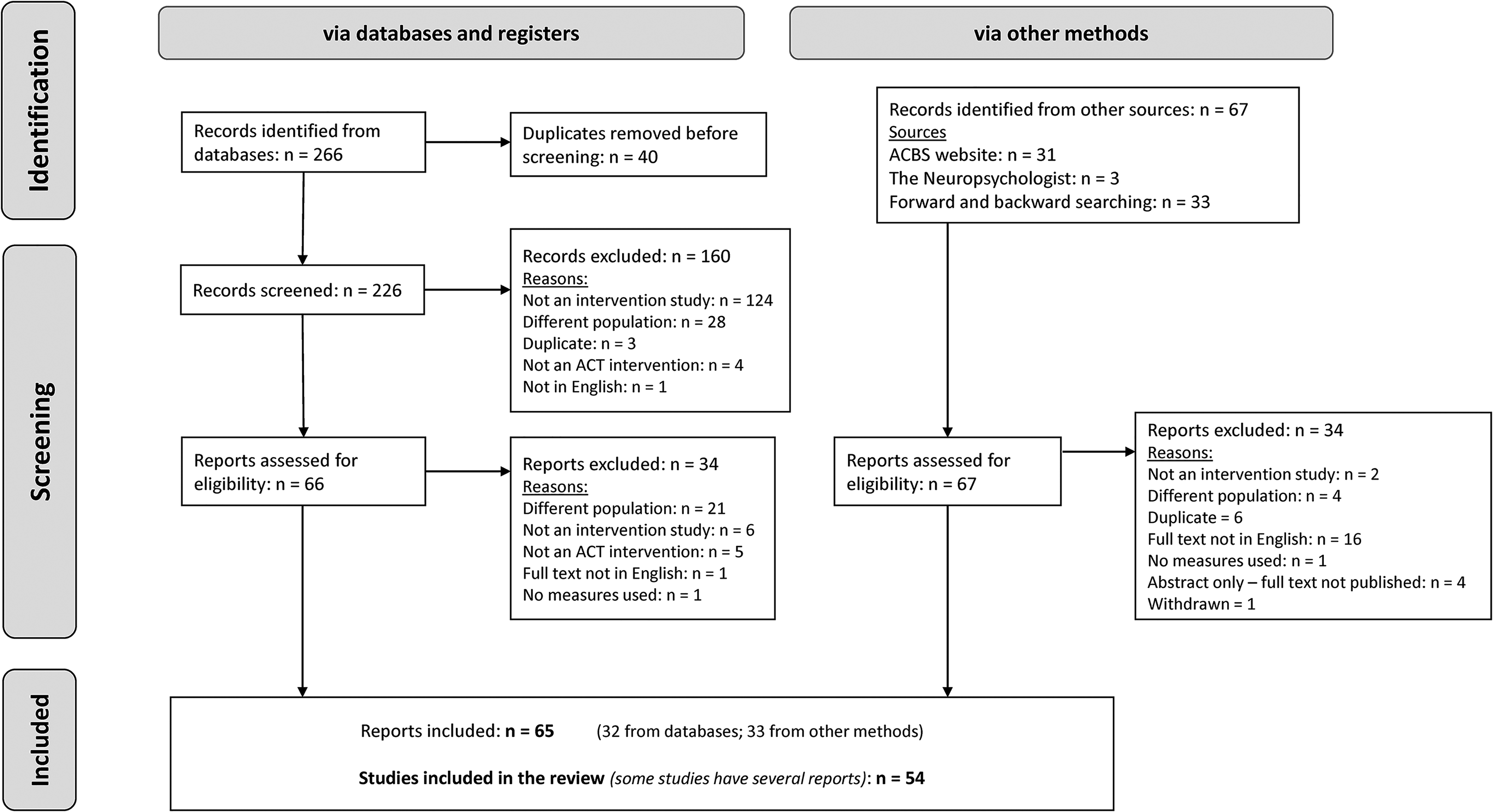
PRISMA flowchart – selection of sources of evidence.
Most of the studies were RCTs (n = 22) or other non-randomised research studies (i.e. those with non-randomised group allocation) (n = 16), with fewer clinical reports (n = 8) and n = 8 unclear for categorisation. The overall mean sample size was 44.1 (range 1–240). Most studies are from the UK (n = 13), Iran (n = 12), US (n = 9) and Australia (n = 7). In total, 136 measurement tools were extracted. Many studies did not specify whether tools used were selected on the basis of measuring processes of change or outcomes.
Objective 1. Neurological populations
The participants had a range of acquired neurological conditions: of the 22 RCTs identified, eight were in MS, six in TBI, three in stroke, two in epilepsy, one in Parkinson's disease, one in spinal cord injury and one for both TBI and stroke. Some studies included participants with a range of different neurological conditions. Throughout the results, these studies are referred to as including ‘multiple conditions’.
The most commonly stated aim of studies was to reduce psychological distress (including anxiety, depression, post-traumatic stress disorder, stress, and emotional and psychological difficulties) (n = 30 studies). This aim was stated across studies in all neurological populations included in this review (apart from studies with multiple conditions). Physical symptoms were targeted in studies in certain conditions, for example, seizures in epilepsy (n = 2) and pain in MS (n = 3). Other studies had nuanced intended aims or outcomes for their interventions, for example, increasing psychological adjustment across multiple conditions, including TBI and MS (n = 5) and increasing resilience in MS (n = 5).
Objective 2. Time points
All studies used pre- and post-intervention measures. Thirty-three of 54 studies (61%) carried out assessments at other follow-up time points, ranging from 1 month post-intervention to 12 months post-intervention.
Objective 3. Process measurement tools
There were 32 different Acceptance and Commitment Therapy-related process measurement tools identified, across 38 of the 54 included studies (70%) (see Table 1). Eleven of the 24 tools (34%) were used in more than one study. Twenty-seven tools were generic and five were condition-specific. Two pain specific measures were identified and were used with MS populations.
Summary of measures relevant to acceptance and commitment therapy processes.
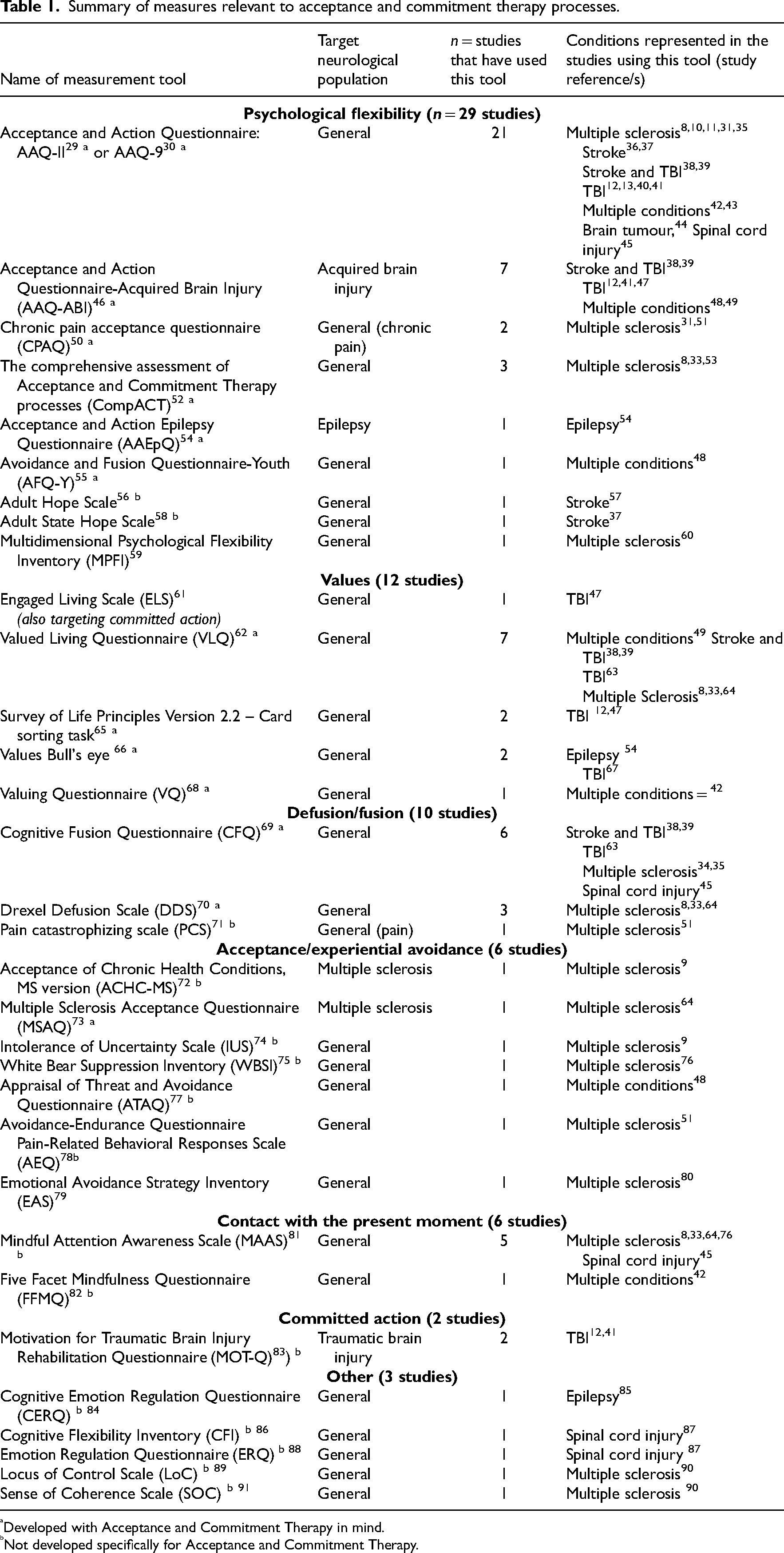
Developed with Acceptance and Commitment Therapy in mind.
Not developed specifically for Acceptance and Commitment Therapy.
Acceptance and Commitment Therapy-related processes were measured in studies of MS, acquired brain injury (including stroke and TBI), spinal cord injury, epilepsy, brain tumour and multiple conditions.
Composite measures of psychological flexibility were most commonly used, that is, in 29/38 (76%) of the studies that included a process measure. The Acceptance and Action Questionnaire29,30 was the tool most often used (21 studies, 55% of the studies including a process measure). A number of condition-specific variations of this measure were also identified in this review (Acceptance and Action Questionnaire-Acquired Brain Injury, 46 Acceptance and Action Epilepsy Questionnaire, 54 Chronic Pain Acceptance Questionnaire 50 bringing the total number of studies using the Acceptance and Action Questionnaire and/or variants to 26.
Other tools measured a specific facet of the hexaflex (Figure 1). Values were measured most commonly (and most often using the Valued Living Questionnaire, 62 n = 7 studies), followed by defusion (or conversely, cognitive fusion), acceptance (or conversely experiential avoidance), contact with the present moment and committed action. No tools specifically targeted self-as-context. In contrast, five other process measures were identified that were not specifically linked to any of the hexaflex facets.
Objective 4. Outcome measurement tools
There were 104 distinct outcome measurement tools extracted from the 54 included studies. Seventy-three (70%) of these tools were used once. Table 2 lists all the extracted tools organised by category, with COMET coding presented for tools extracted from studies identified in the 2020 search (see objective 5 for a summary of this COMET coding).
Outcome measurement tools.

Tools which are not related to a neurological condition.
Tools designed for use in neurological conditions of various causes.
The first category is
The most commonly used measurement tools were the 12-Item Short Form Survey 92 (n = 6 studies) and the EQ-5D 94 (n = 6 studies), followed by the Multiple Sclerosis Quality of Life Instrument, 95 Satisfaction with Life Scale 96 and the World Health Organization Quality Of Life measure 99 (each used in n = 4 studies).
The second category is
Further outcome categories identified were participation (i.e. involvement in life situations) (n = 13 studies), stress (n = 6 studies), resilience (n = 5 studies), pain (n = 4 studies), fatigue (n = 3 studies), seizures (n = 3 studies), self-efficacy (n = 3), sleep (n = 3 studies) and memory (n = 2 studies). Each tool in these categories was used in a maximum of four studies. Pain, fatigue and resilience were only measured in MS and seizures were specific to studies in epilepsy.
Objective 5. COMET taxonomy
Fifty-three of 76 tools (those identified in the 2020 search) were freely available and reviewed item-by-item. COMET coding of all extracted measures showed that three of the five COMET core areas (physiological/clinical, life impact and adverse events) and 13 of the 38 outcome domains were represented in the data set (see Table 3). As discussed in methods, COMET outcome domains are not mutually exclusive (see Table 2).
COMET core areas and outcome domains represented in the data set.
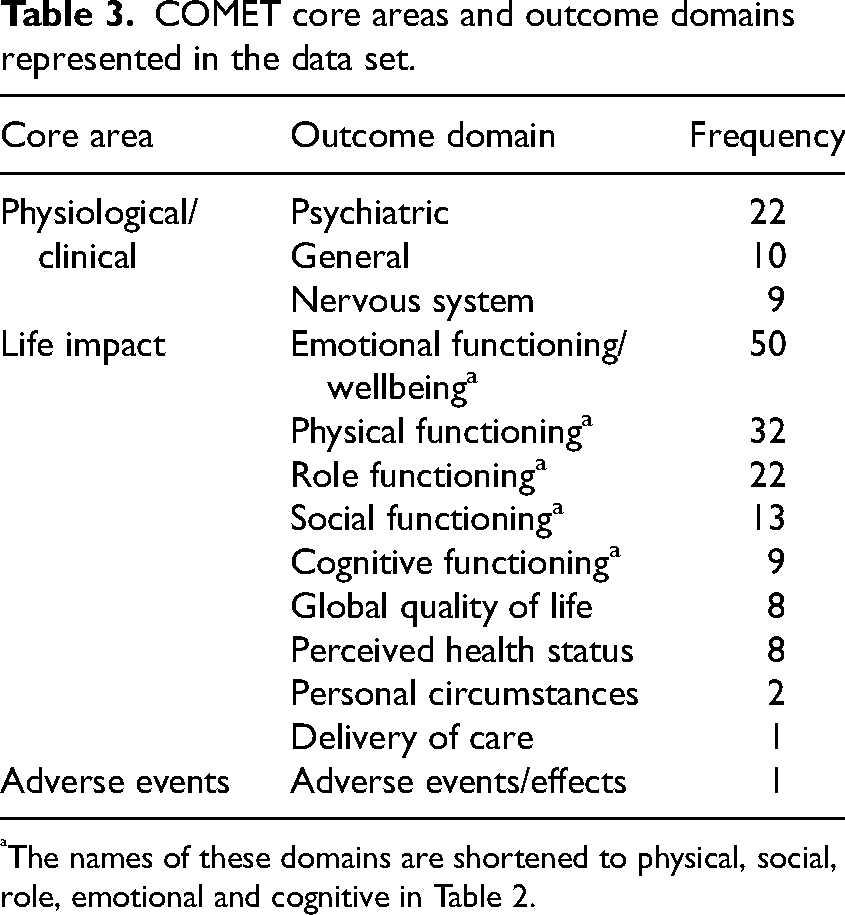
The names of these domains are shortened to physical, social, role, emotional and cognitive in Table 2.
The physiological/clinical core areas present in the data are in line with the eligibility criteria for this review. Within the life impact and adverse event core areas, all outcome domains were present in the data. The core areas not represented are death and resource use, ineligible for this review. The most frequently occurring core areas and domains are summarised below.
The most commonly occurring physiological domain was ‘psychiatric’. There were also ‘general’ outcomes, including pain, fatigue and life expectancy. According to the COMET guidance, the physiological/clinical domains should be classified according to underlying cause/body system. Therefore, certain measures relating to neurological conditions specifically were coded under the ‘nervous system’ domain (e.g. Parkinson's Disease Questionnaire-39 106 and Functional Assessment of Cancer Therapy scale – Brain. 103 ).
The most commonly classified domain was the life impact domain ‘emotional functioning/well-being’. Measures of mental health signs and symptoms (e.g. anxiety and depression) were classified in this domain, as well as under ‘psychiatric’ (above).
The health status, quality of life and well-being measures identified were coded against all the COMET core areas and outcome domains above (see Table 2 for measure specific results). As per taxonomy guidance, only composite items on quality of life or health status were classified under the ‘global quality of life’ and ‘perceived health status’ domains. For example, the World Health Organization Quality Of Life measure 99 was classified as such, as it contains the composite questions ‘How would you rate your quality of life?’ and ‘How satisfied are you with your health?’. Most health status, quality of life and/or well-being measures included items targeting multiple individual domains. These frequently included the functioning domains (physical, social, role, emotional/well-being and cognitive) as well as often including an item/s about physiological signs and symptoms.
Discussion
This review found that a large number of studies utilised Acceptance and Commitment Therapy for people with a range of acquired neurological conditions (with MS being the most common), using many different measurement tools. Measures targeting psychological flexibility as a composite were commonly used and, in accordance with previous research, 209 , this was most often measured by the Acceptance and Action Questionnaire-II. 29 The majority of studies aimed to reduce psychological distress and thus selected a wide variety of non-condition specific health-related outcome measures exploring distress, anxiety and/or depression.
This proliferation of measures warns us of challenges pooling and comparing data unless we reach consensus on process and outcome measures for future studies. We found that the most commonly measured COMET taxonomy domains were in the life impact core area. This is encouraging as the theoretical model of Acceptance and Commitment Therapy aims to improve functioning and well-being, rather than just focusing on the reduction of psychological distress.7,18 The majority of studies reported measurement time points relative to the end of the intervention in contrast to recommendations to report relative to baseline. 210 In categorising the measures it became clear that there is inconsistency in the definitions and use of terms such as health status, quality of life and well-being, as previously reported. 211
A strength of this review is the meticulous process of categorising and coding all measures with reference to literature, including the novel application of the COMET taxonomy to Acceptance and Commitment Therapy research. 19 Coding consensus was achieved through substantial consultation both internally (paper authors) and externally (with Susanna Dodd, author of the COMET taxonomy). Item-by-item coding of each health-related outcome measure (when freely available) enabled comprehensive mapping according to all outcome domains measured. However, a risk of item-by-item classification is that it does not take into account how the measurement tools have been constructed, and therefore may overestimate the domains that have been measured. Furthermore, as the domains in the COMET taxonomy are not mutually exclusive, the coding process did not aid the categorisation of the many tools into distinct groups. Due to these limitations, COMET categorisation was not completed for additional measures extracted when the review was updated in 2022.
A ‘broader’ level categorisation of the measures (as described in methods) was also provided to make overall sense of the tools. This broad categorisation of the outcome measures, and the categorisation of process measures according to the Acceptance and Commitment Therapy hexaflex, were done in a best-fit manner by the authors. Data extracted from the studies themselves were used to inform these decisions, but inconsistencies in this information, and lack of reporting, meant that author consultation was often used, which remains subjective and open to further debate.
This review is limited in only including studies reported in English. However, the inclusion of multiple study types, and of studies that included Acceptance and Commitment Therapy plus other interventions, enabled comprehensive identification of measures used in Acceptance and Commitment Therapy in acquired, neurological populations.
A strength of this review is the enhancement of the scoping review methodology 21 through use of double reviewing during study selection, data extraction and data synthesis.
This review contributes recommendations and future research directions. Our findings highlight reporting inconsistencies in the field that could be improved. The use of suitable reporting guidance (https://www.equator-network.org/) would facilitate data synthesis from Acceptance and Commitment Therapy research trials in systematic reviews. Authors should clarify whether measures were selected to explore processes of change or health outcomes. Authors should explicitly state the process and outcome domains that they are aiming to measure, as well as the measurement tools themselves. There is on-going development of core outcome sets relevant to a number of the populations included in this review. Where available, it is recommended that clinical trials of Acceptance and Commitment Therapy use relevant core outcome sets to inform their choice of measures.
The findings of this review of what has been measured are a useful resource to support identification of candidate measurement tools. However, this cannot be extrapolated to inform what should be measured, or which tools should be used.
In order for specific recommendations to be made for use of Acceptance and Commitment Therapy in acquired, neurological populations, future research is required and should include consensus by experts, use of patient, carer and public involvement,212,213 and examination of the psychometric properties of the measures.
Conclusion
This review summarises a detailed categorisation of the process and outcome measures previously used in Acceptance and Commitment Therapy studies in acquired neurological populations. Acceptance and Commitment Therapy has primarily been used to target psychological distress, but other outcomes including physical health outcomes have also been targeted. We highlight that a wide range of both process and outcome measurements are in use, with little guidance available on selection. This review provides a resource for other researchers and could support development of core outcome sets.
Mental health needs of adults with neurological conditions are poorly addressed and there is an imperative to deliver evidence-based interventions to promote well-being. Clinical guidance on whether Acceptance and Commitment Therapy is useful for this clinical population is being hampered by the lack of agreement on which of the many measures available should be used to evaluate the process of change and outcomes following intervention. Key stakeholders should be involved in consensus-based decision-making, which draws on resources such as this review of candidate measures.Clinical messages
Supplemental Material
sj-docx-1-cre-10.1177_02692155221144554 - Supplemental material for A scoping review to identify process and outcome measures used in acceptance and commitment therapy research, with adults with acquired neurological conditions
Supplemental material, sj-docx-1-cre-10.1177_02692155221144554 for A scoping review to identify process and outcome measures used in acceptance and commitment therapy research, with adults with acquired neurological conditions by Hannah Foote, Audrey Bowen, Sarah Cotterill, Geoff Hill, Matilde Pieri and Emma Patchwood in Clinical Rehabilitation
Supplemental Material
sj-pdf-2-cre-10.1177_02692155221144554 - Supplemental material for A scoping review to identify process and outcome measures used in acceptance and commitment therapy research, with adults with acquired neurological conditions
Supplemental material, sj-pdf-2-cre-10.1177_02692155221144554 for A scoping review to identify process and outcome measures used in acceptance and commitment therapy research, with adults with acquired neurological conditions by Hannah Foote, Audrey Bowen, Sarah Cotterill, Geoff Hill, Matilde Pieri and Emma Patchwood in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors thank Sabrina El Kouaissi for her invaluable support in updating the searches in 2022 and extracting the necessary data, and to Bria Bullard for data checking. They also thank Dr Susanna Dodd for her guidance in coding the outcome measurement tools, and Anna Theis, University of Manchester librarian, for her support and expertise in developing the search strategy used.
Author contributions
HF, AB, SC and EP designed the study. HF and MP charted and collated the data. All authors contributed to discussions about the methodology and analysis of data. HF took the lead on summarising the results and drafted the article. All authors critically reviewed and revised the article and approved the final version for submission.
Author's note
Authors Hannah Foote, Audrey Bowen and Emma Patchwood are also affiliated at Division of Psychology and Mental Health, University of Manchester, Manchester, UK.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This scoping review was funded by Hannah Foote's Research Impact Scholarship, which was awarded by the Division of Development and Alumni Relations, University of Manchester. Emma Patchwood is funded by a Stroke Association Post-doctoral Fellowship.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.