
Abstract
Objective
To evaluate the effects of transcutaneous electrical acupoint stimulation (TEAS) on upper limb motor recovery during post-stroke rehabilitation.
Design
Single-blind, randomized controlled trial.
Setting
Four inpatient rehabilitation facilities.
Subjects
A total of 204 stroke patients with unilateral upper limb motor impairment were randomly 1:1 allocated to TEAS or sham TEAS group. Baseline demographic and clinical characteristics were comparable between the two groups.
Interventions
Both groups received conventional physical and occupational therapies. TEAS and sham TEAS therapy were administered to two acupoints (LI10 and TE5) with a pulse duration of 300 µs at 2 Hz on the affected forearm for 30 times over 6 weeks.
Outcome measures
The upper-extremity Fugl-Meyer score (primary outcome), manual muscle testing, modified Ashworth scale, Lindmark hand function score, and Barthel index were evaluated by blinded assessors at baseline, 2, 4, 6, 10, and 18 weeks.
Results
The number of patients who completed the treatment was 99 and 97 in the TEAS and the sham group. No significant between-group difference was found in the Upper-Extremity Fugl-Meyer score, Modified Ashworth Scale, Lindmark hand function score, and Barthel Index after intervention and during follow-up. However, the TEAS group exhibited 0.29 (95% CI 0.02 to 0.55) greater improvements in Manual Muscle Testing of wrist extension than the sham group (p = 0.037) at 18 weeks.
Conclusions
Administration of TEAS therapy to hemiplegic forearm could not improve the upper extremity motor recovery. However, TEAS on the forearm might provide potential benefits for strength improvement of the wrist
Introduction
Globally, stroke is one of the most common causes of death and long-term adult disability, 1 with nearly 2.5 million annual new cases in China. 2 Persistent disability after stroke is associated with serious upper extremity and hand impairment, as more than half of stroke survivors are not able to regain proper arm function even 6 months after stroke. 3
Many studies have aimed at developing treatment methods for upper limb and hand rehabilitation after stroke and some treatments have demonstrated clear effectiveness with ample evidence such as constrained-induced movement therapy and robotic therapy. 4 However, constrained-induced movement therapy is not applicable in patients with moderate to severe impairment. 5 Robotic therapy can be a feasible alternative intervention for patients with severe arm paresis, but robotic devices are usually expensive. 6 The efficacies of other treatment techniques like mirror therapy, mental practice, and virtual reality have not been proven with high-quality evidence.4,7 Therefore, novel rehabilitation approaches should be developed to improve upper limb motor outcomes after stroke.
Transcutaneous electrical acupoint stimulation (TEAS), a combination of transcutaneous electrical nerve stimulation technique and Chinese traditional acupuncture theory, is a potentially efficient, safe, and low-cost therapeutic option for stroke rehabilitation.8–12 Transcutaneous electrical nerve stimulation uses low-voltage electrical currents to provoke nerves or muscles over the skin, generating various therapeutic effects.13,14 In contrast, TEAS therapy is usually with lower frequency (2–4 Hz), higher intensity (to tolerance threshold), and longer pulse width (100–400 ms).15,16 During TEAS treatment, electrical stimulation is administered to selected acupoints, eliciting an “acupuncture point sensation.” 17
Currently, reported clinical evaluations of TEAS therapy in stroke rehabilitation so far have mostly found at least some evidence to suggest therapeutic benefits in walking performance9,10 and overall function. 8 Currently, two studies focused on the effectiveness of TEAS on the affected upper extremity motor performance in stroke patients, and both studies did not find that TEAS was better than the placebo-TEAS when combined with active training.11,12 In addition to promoting motor recovery, TEAS also demonstrated certain effects on relieving muscle spasticity following brain injury. 18 We also found a review article showing the positive effects of TEAS on upper limb functional recovery in stroke patients. 19 However, all included articles were published in Chinese, so the positive finding in this review article suffers from possible language bias. Also, most included RCTs did not accurately describe the stages of stroke, and the duration and treatment protocols of included trials varied significantly. 19
Given these conflicting results about the clinical effects of TEAS in motor recovery in patients with brain damage, the exact therapeutic effects of TEAS on post-stroke upper limb motor recovery remain unclear. Therefore, this single-blind, randomized controlled trial aimed to investigate whether a combination of TEAS therapy and conventional rehabilitation methods could produce additional benefits to stroke patients with arm and hand motor impairments. We hypothesized that TEAS might be effective in improving motor function, spasticity, muscle strength, or activities of daily living during stroke recovery.
Methods
This study was a randomized, single-blind, controlled trial conducted in four inpatient rehabilitation facilities (two rehabilitation hospitals and two community hospitals) in Shanghai, China, from January 1st, 2016 to December 31st, 2018. This study was a subproject belonging to a large project named ‘Effects of traditional rehabilitation medicine on stroke survivors with hand dysfunction’ funded by the National Science & Technology Pillar Program during the Twelfth Five-year Plan Period. The ethical approval was obtained from the Review Board of Ethics Committee of Huashan Hospital and registered at the Chinese Clinical Trial Registry (ChiCTR-IOR-15006102). This study fulfilled the principles of the Declaration of Helsinki, and it was conducted and reported according to the recommendations of CONSORT guidelines.
At each research center, potential participants with unilateral upper limb impairment after stroke were consecutively screened by the physicians (XW, KZ) for eligibility. Study participants were all required to sign a written informed consent before enrolment.
Due to recruitment challenges, the original inclusion criteria were modified to include participants with a wider age range (increased from 40–80 to 18–85) and onset range (increased from 14 days–12 months to 10 days–2 months). The recruitment did not begin until the revised inclusion criteria were approved by the Review Board of Ethics Committee of Shanghai Third Rehabilitation Hospital. The final inclusion criteria were: (1) Medically stable; (2) First-ever cerebrovascular accident; (3) MRI or CT confirmed ischemic or hemorrhagic stroke; (4) Stroke onset between 10 days and 12 months; (5) 18 to 85 years of age; (6) Brunnstrom stages I–V in the affected hand; (7) Intact skin on the hemiparetic forearm.
The exclusion criteria were: (1) Patients with significant cognitive impairment (MoCA ≤ 24); (2) Severe shoulder or hand pain; (3) Excessive sensory disturbance, aphasia, unilateral neglect, or apraxia; (4) A history of serious neurological or psychiatric diseases; (5) A history of alcohol or drug dependence; (6) Implanted stimulators (such as cardiac pacemaker); (7) Pregnancy.
All eligible participants who signed written informed consent were randomized 1:1 to receive TEAS or sham TEAS therapy, using a center-stratified randomization procedure by computer-generated random numbers with SPSS software (version 25.0, Chicago, IL, USA). Randomization was performed by a physician (YC) who was not involved in the recruitment, data collection, and treatment of the study. Randomization codes were concealed in sequentially numbered opaque envelopes to ensure allocation concealment. The therapists who delivered the conventional rehabilitation therapy and the included patients were masked to allocation.
Patients in both groups were subjected to conventional rehabilitation which lasted for 60 min per day, 5 days a week for 6 weeks. The conventional rehabilitation included daily physical and occupational therapies that were widely accepted, individual-specific, and routinely practiced by experienced therapists in each center. The intervention, directed at both upper and lower extremities, was aimed at improving skills in basic daily activities. It combined the techniques of muscle stretching, active/passive mobilization, neuromuscular facilitation, and task-specific training. All therapists received standardized training for consistency before intervention and were not involved in the group assignment and outcome measurements.
TEAS therapy was administered to two acupoints (LI10 and TE5) on the affected forearm through a pair of surface electrodes (40 × 26 mm) connected to the electrical stimulator (MyoNet-COW, NCC Medical Co Ltd., Shanghai, China) (Figure 1). The acupoints selected in this study originated from previous reports on TEAS treatment for motor function recovery in individuals with central nervous system injuries.11,20 TEAS treatment had a pulse width of 300 µs and a frequency of 2 Hz in the constant mode at the maximum tolerable intensity. 21 The 2 Hz modality was used because evidence indicated that low-frequency TEAS could highly activate the motor cortex when compared to high frequencies, such as 100 or 120 Hz, in ischemic stroke patients. 22 The sham group was administered with an identical treatment, except that the electrical circuit of the stimulator had been internally disconnected. That is, the lights and screen of the stimulator were on, but there was no real electrical stimulation. Patients in the sham group were informed that they might or might not feel mild tingling sensations during treatment. TEAS or sham TEAS therapy lasted for 30 min per session, 5 days a week for 6 weeks. The stimulation lasted for 30 min per session because a previous study found that 30 or 60 min of neuromuscular electrical stimulation led to similar upper limb motor function improvements in stroke patients. 23 TEAS and sham TEAS therapy were performed by two experienced physical therapists who had received standardized training on the use of TEAS equipment before the study intervention.
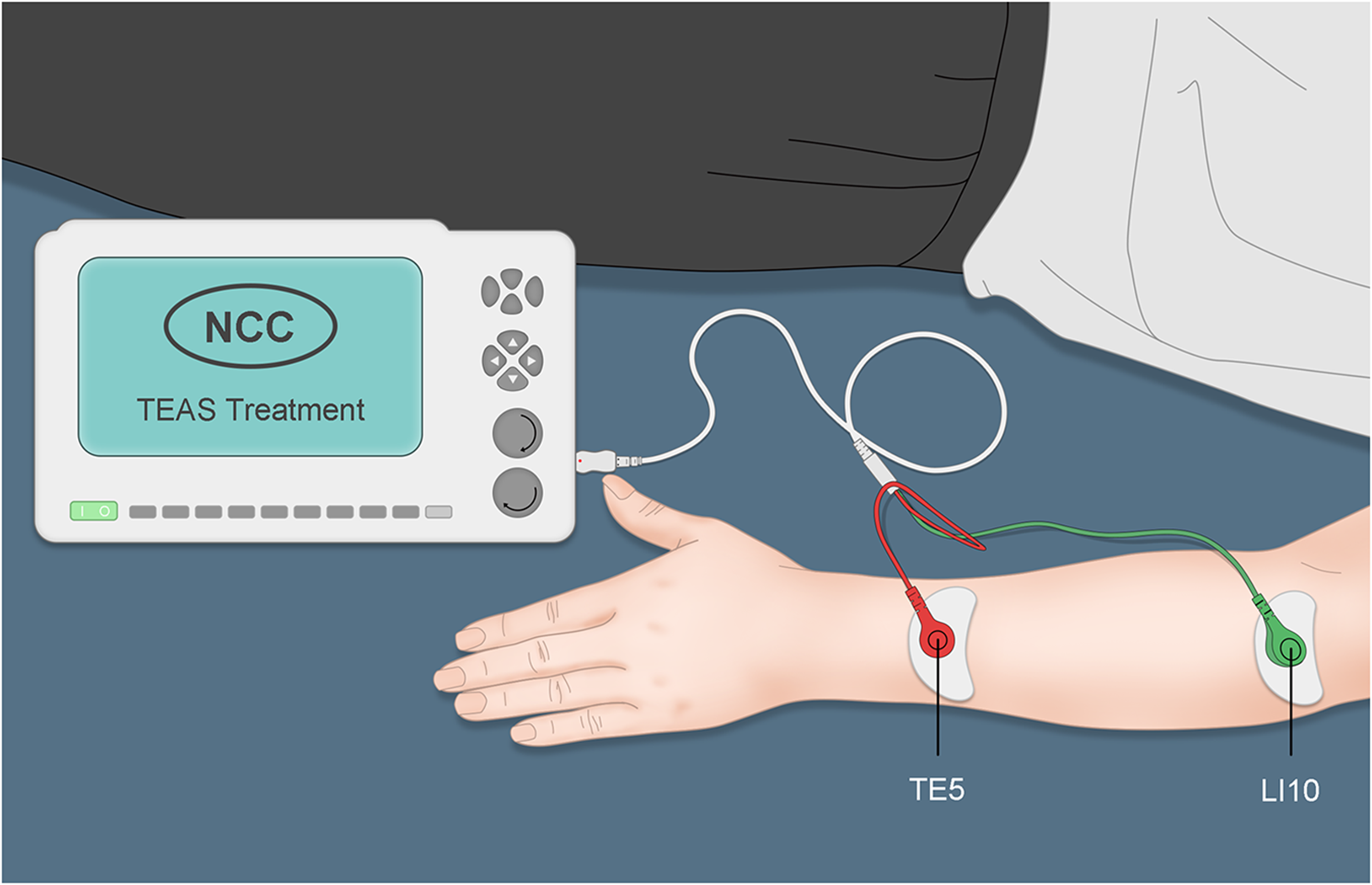
Forearm acupoints used in this study.
The study participants were evaluated by two experienced assessors (HW, YX) that were blinded to the treatment assignment at baseline, after every 2 weeks during the treatment period, and at 4 and 12 weeks after completion of treatment. Before the assessment, a standardized assessment protocol that included the patient's position, verbal instruction, and demonstration to the patient was developed. Assessors were obliged to follow this standardized protocol and they were trained by a senior therapist to ensure that they could perform the assessment in a proper way. The primary outcome measure was the Upper-Extremity Fugl-Meyer score. Secondary outcome measurements included muscle strength assessment, muscle spasticity, hand function, and activities of daily living. The following variables were evaluated:
The primary outcome measure was the change in the Upper-Extremity Fugl-Meyer score from baseline to 6 and 18 weeks. It is a valid and reliable assessment of upper limb impairment both within and between raters in stroke survivors,
24
which consists of 33 items scored on a 3-point (0–2 points) ordinal scale for a maximum possible score of 66.
25
Post hoc outcome measurements of the proximal (0–42 points) and distal (0–24 points) subscales were also performed to examine the adjacent and remote effects of TEAS. Muscle strength of wrist flexion and extension was measured by Manual Muscle Testing on a scale from 0 (no muscle activity) to 5 (normal muscle power). Although few studies have directly investigated the rater reliability of Manual Muscle Testing in stroke survivors, it has shown excellent inter-rater reliability in trained examiners to assess the grade of muscle weakness in a wide range of pathologies.
26
Wrist flexors spasticity was assessed by measuring resistance to passive wrist extension with the Modified Ashworth Scale scored using a 6-point (0, 1, 1 + , 2, 3, 4) scale. This scale has very good intra-rater reliability in the assessment of upper limb spasticity in patients with hemiparesis.
27
The grasp function of the hand was assessed by a subscale selected from a reliable and valid tool named the Lindmark Motor Score.
28
Patients were required to hold a tennis ball with their fingers abducted and flexed around the ball. It reported using a 4-point scale: 0 = cannot grasp; 1 = can grasp but unable to hold against slight resistance; 2 = can hold the ball for 5 s but release it upon moderate resistance or the grasp becomes uncoordinated or changed; 3 = can hold the ball against strong resistance for 5 s and release it in a normal way. Barthel Index was used to assess the patient's independence in basic activities of daily living. The original 10-item scale was used for a maximum possible score of 100. Evidence indicates that the Barthel Index has excellent inter-rater reliability to be an appropriate outcome measure for stroke trials and practice.
29
The sample size was calculated prior to the start of the study using a previously reported method,
30
based on the assumption that the mean difference between the two groups would be 5 points in the Upper-Extremity Fugl-Meyer score with a common standard deviation of 12 points in both groups. Furthermore, we assumed that the study would have a dropout of 10%, and the final target sample size was 204 participants with 102 assigned to each group when setting a power of 80% and a significance level of 0.05.
Data was input by the EpiData software (version 3.1, the EpiData Association, JM Lauritsen) after double-checking by trained researchers (SC, LD). All analyses were performed by an independent statistician (YW) using the SPSS software. A modified intention-to-treat analysis was adopted: we analyzed all assigned subjects for whom outcome data at 6 weeks were available. 30 For missing data, we moved the last data forward or, if no former value was available, the next recorded value was used. The student's t-test and chi-square test were performed to ensure homogeneity at baseline. The normality of data distribution was evaluated using the Kolmogorov–Smirnov statistic. Generalized estimating equations (GEEs) were used to estimate the effects of treatment between the TEAS group and the sham group on all outcomes. Results are presented as mean and 95% confidence intervals (CIs) and the level of statistical significance was defined as α = 0.05 of two-sided probability.
Results
Details of participant recruitment, allocation, and follow-up are displayed in the flow diagram (Figure 2). Out of the 980 stroke survivors who were screened for eligibility, a total of 217 met our study criteria, with 204 of them agreeing to participate in this study. There were no differences in baseline demographic, stroke-related, and upper limb motor characteristics between the two groups. The average time from stroke onset at enrollment was 95.7 days (range, 11 to 349), with 72, 92, and 40 patients at acute (35.3%), subacute (45.1%), and chronic (19.6%) stages. The baseline means upper-extremity Fugl-Meyer score was 15.2 (range, 0 to 62), with 154 (75.5%) patients being severely impaired (0 to 22 points) 31 (Table 1).
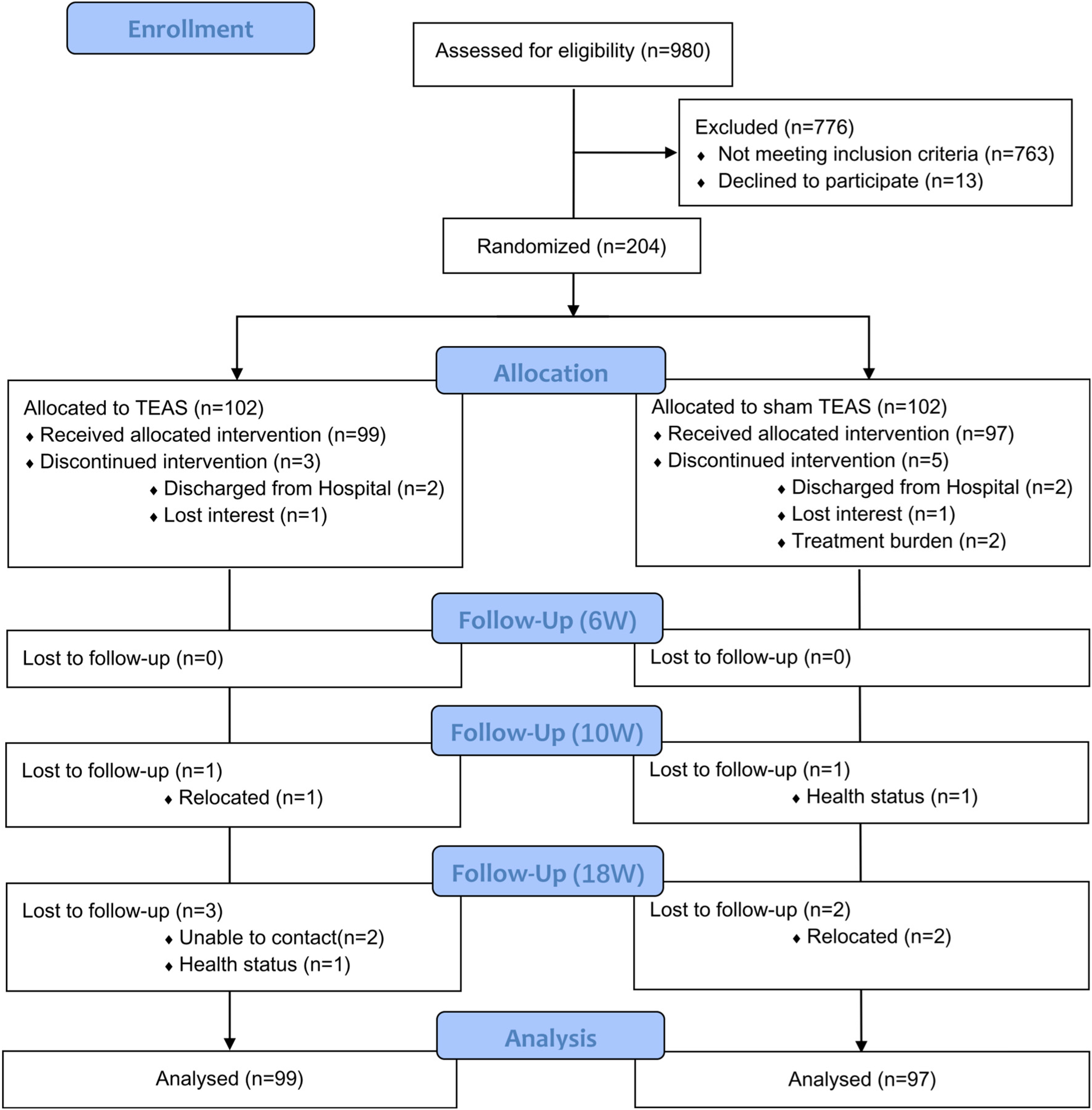
CONSORT flow diagram for enrollment and outcomes.
Baseline characteristics of the patients.
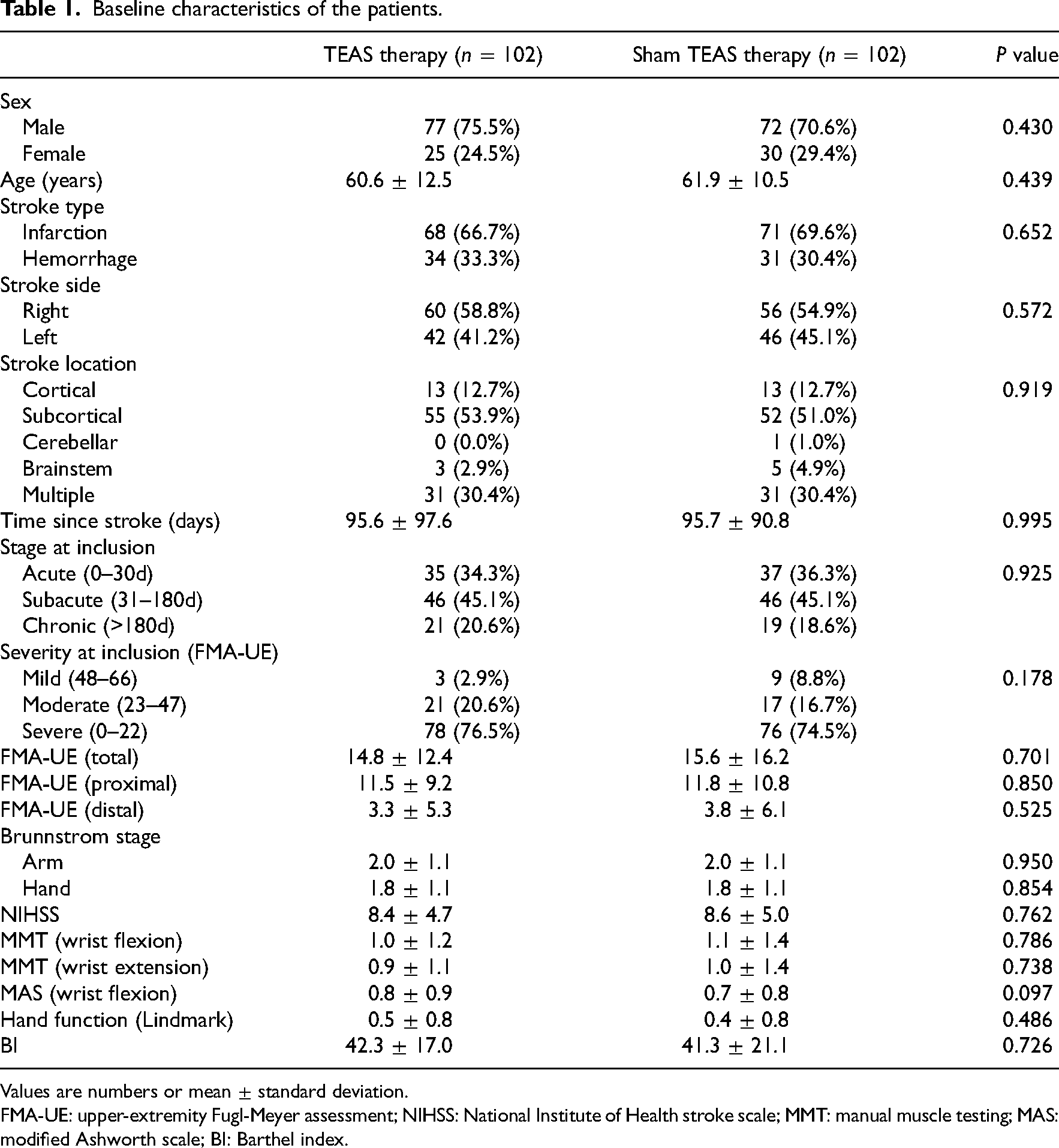
Values are numbers or mean ± standard deviation.
FMA-UE: upper-extremity Fugl-Meyer assessment; NIHSS: National Institute of Health stroke scale; MMT: manual muscle testing; MAS: modified Ashworth scale; BI: Barthel index.
Primary outcome: At the end of treatment, the mean change in the upper-extremity Fugl-Meyer score from baseline was higher in the TEAS group, however, the between-group differences were not significant (difference: 1.62 points, 95% CI: −1.16 to 4.40, p = 0.254). Post hoc analysis also did not reveal any significance in the distal and proximal subscales. At 18 weeks, the between-group differences in the Upper-Extremity Fugl-Meyer score and its subscales were still not significant (Table 2).
Changes in primary and secondary outcomes.
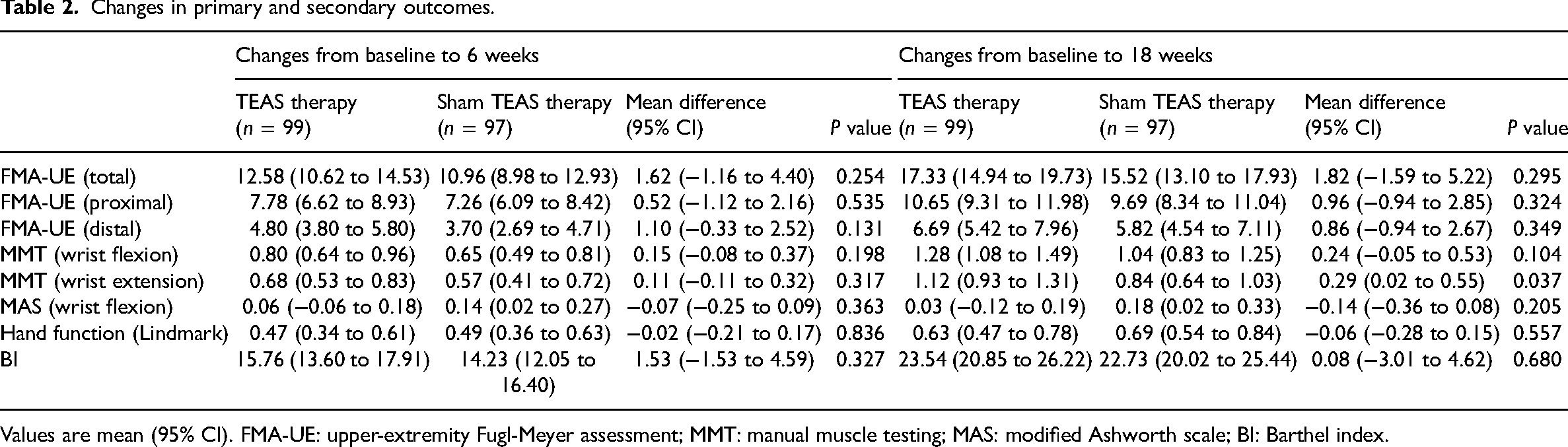
Values are mean (95% CI). FMA-UE: upper-extremity Fugl-Meyer assessment; MMT: manual muscle testing; MAS: modified Ashworth scale; BI: Barthel index.
Secondary outcomes: At 6 weeks, both groups exhibited significant improvements in Manual Muscle Testing scores (wrist flexion/extension), Lindmark hand function scores, and Barthel Index scores when compared to the baseline. However, there were no significant between-group differences for all these outcomes. At 18 weeks, patients in the TEAS group exhibited higher MMT scores in wrist extension when compared to the sham group (difference: 0.29 points, 95% CI: 0.02 to 0.55, p = 0.037). There were no significant between-group differences in other outcomes. Regarding wrist flexor spasticity, no significant changes from baseline were found in both groups at 6 and 18 weeks (Table 2).
Findings from the longitudinal GEEs analyses of the primary outcome within each group showed that both groups demonstrated significant improvements along the 18 weeks in total (both p < 0.001), proximal (both p < 0.001), and distal (both p < 0.001) score of the upper-extremity Fugl-Meyer assessment. This result means that 6 weeks of conventional rehabilitation combined with TEAS/sham TAES therapy can significantly improve the upper limb motor function in stroke patients. The changes in primary and secondary outcomes during the 18-week study period compared to the baseline are presented in the Supplementary Material. Overall, the longitudinal GEEs analyses did not show any significant between-group difference.
The TEAS interventions in this study were not associated with any serious adverse events or side effects. The treatment compliance was excellent, with a total of 196 (96.1%) participants completing their assigned treatment interventions, while 189 (92.6%) participants received all assessments during follow-up. Reasons for withdrawal are provided in the flow diagram (Figure 2).
Discussion
The major finding of this multicenter, randomized, single-blind, controlled study was that 6 weeks of TEAS on the forearm acupoints did not demonstrate better effects than sham TEAS on upper limb motor recovery when combined with conventional rehabilitation. We also found that TEAS might contribute to the increase of wrist extension strength at 12 weeks after treatment, although the absolute between-group difference was small and of weak significance.
Acupuncture therapy is an important supplement to conventional stroke rehabilitation in China. 32 However, acupuncture therapy is associated with limitations, such as possible risks of broken needles and infection, heavy dependence on the therapist's skill, as well as lack of standardization and reproducibility. 32 Transcutaneous electrical nerve stimulation has been proved to improve hand-related function in patients with spinal cord injury 33 and stroke.34,35 Prolonged periods of peripheral sensory stimulation contributes to increasing the excitability of the cortico-motor excitability. 36 As a combination of transcutaneous electrical nerve stimulation and acupuncture, the TEAS is non-invasive and safe,9,20 and it is equipped with built-in therapeutic parameters that make it standardized in clinical practice. 37 To the best of our knowledge, our study represents the largest clinical trial of TEAS on upper limb recovery in stroke patients.
Primary outcome measurements revealed that 6 weeks of TEAS intervention brought a mean improvement of more than 10 points in the upper-extremity Fugl-Meyer scores in both groups. However, the longitudinal analyses showed that the between-group differences were not statistically significant. Subgroup analysis of proximal and distal scores of the upper-extremity Fugl-Meyer assessment also did not reveal any significant between-group difference. This negative finding was consistent with two previous TEAS studies with similar design. 12 Alwhaibi et al. 12 compared the therapeutic effects of TEAS (applied to LI11 and LI4) and sham TEAS on upper limb motor recovery in chronic stroke patients. The results indicated that adding TEAS to task-specific training did not further improve the upper-extremity Fugl-Meyer score and Box and Block Test Interestingly, the activity of the motor area (C3) in the TEAS group increased significantly compared with the sham group, suggesting that the degree of cortical remodeling was not enough to cause significant changes in motor recovery. In another study conducted by Christina et al., 73 stroke patients were randomized to TEAS (applied to LI4, LI10, LI11, and LI15), placebo-TEAS, and control group. 11 The results showed that all between-group differences in Action Research Arm Test and hand strength were not significant except that the TEAS group demonstrated greater improvements in hand grip and pinch strength than the control group. In sum, based on our findings and previous evidence, we suggest that adding TEAS to conventional rehabilitation may not bring additional improvements to the upper extremity and hand function. It is also possible that the functional enhancements derived from the TEAS treatment protocol were too small to show any significant effect. However, our result should not be generalized to all stroke populations since most participants (75%) had severe dysfunction. In future studies, stroke patients with mild and moderate upper limb motor impairments should be recruited and studied respectively.
In this study, the only significant between-group difference was noted in Manual Muscle Testing of wrist extension at 18 weeks. This result suggested that TEAS might be beneficial to muscle weakness, with the effects being confined to muscles adjacent to the acupoints that are stimulated. This finding is consistent with the results reported by other TEAS studies.9–11 Yan et al. 9 found that 3 weeks of daily TEAS treatment at the acute phase to 4 acupoints (St36, Lv3, GB34, and Bl60) of the hemiplegic lower leg significantly increased dorsiflexor strength. A case study of a chronic stroke patient also showed that a 4-week home program consisting of TEAS therapy and task-related training could effectively improve dorsiflexor strength, gait velocity, and walking edurance. 10 There are several possible mechanisms. First, the LI10 and TE5 acupoints are adjacent to extensor carpi radialis and finger extensors, respectively. Six weeks of low-frequency electrical stimulation might partially reverse or slow down the atrophy process of these two muscles.38–40 Second, previous studies reported that prolonged peripheral electrical stimulation leads to reinforced sensory inputs to the sensory cortical representation, which may facilitate motor outputs of the muscles innervated by these sensory-motor areas.22,41 However, whether acupoint stimulation of the LI10 and TE5 during TEAS therapy can improve muscle strength in stroke survivors through a mechanism different from transcutaneous electrical nerve stimulation remains to be further studied.
In this study, there were no statistical between-group differences in other outcomes. Although previous TEAS studies reported some positive results in relieving spasticity in patients with brain damage,9,10,18 they all applied 100 Hz rather than 2 Hz electrical stimulation. Direct evidence is from a randomized controlled trial in brain injury patients which showed that 4 weeks of TEAS at 100 Hz to four acupoints (L14, LU10, ST36, and BL57) could significantly relieve wrist spasticity while 2 Hz and sham TEAS therapy did not. 18 In addition, the TEAS group did not show any superiority in the Lindmark hand function test and Barthel Index. It is probably attributed to the floor effects of these two scales since 75% of participants were with severe impairments. Moreover, the relatively wide standard deviations might be another reason for these negative results.
The strengths of this study included the high compliance rates, extended follow-up period, and the absence of adverse events. However, this study is also associated with several limitations. Although the sample size was based on statistical calculation, the relatively loose inclusion criteria caused large standard deviations in all outcomes. In addition, this study demonstrated the ceiling effect for some outcomes. Furthermore, the treatment dose, defined as the combination of different parameters including treatment frequency, intensity, and duration, should also be investigated. 23 Lastly, according to the theory of acupoint compatibility, when two or more acupoints are selected, the synergy between the acupoints is strengthened. 42 After we compared all the positive and negative studies of TEAS on stroke rehabilitation, we found that the compatibility of four acupoints demonstrated greater effects than two acupoints.8–12 Thus, future studies should evaluate the optimum compatibility of acupoints. 32
In conclusion, adding 6 weeks of TEAS therapy (applied to LI10 and TE5) to conventional rehabilitation could not improve the upper extremity motor recovery in stroke patients. However, our study found positive effects of TEAS on the strength of wrist extension at 12 weeks after treatment completion. Future studies should investigate the effects of different treatment doses and acupoints compatibilities in patients with mild and moderate impairments, respectively. More sensitive assessments such as Wolf Motor Function Test or Action Research Arm Test should also be included in the future.
Clinical messages
Adding 6 weeks of TEAS therapy to two acupoints (LI10 and TE5) on the affected forearm did not bring additional benefits to upper extremity motor recovery as measured by the upper-extremity Fugl-Meyer score in stroke patients.
TEAS therapy might contribute to the improvement of arm muscle strength with the effects being confined to muscles adjacent to the acupoints that are stimulated.
Future studies should investigate the influence of the treatment dose and acupoints compatibility on TEAS therapy in stroke patients with mild and moderate impairments, respectively.
Supplemental Material
sj-pdf-1-cre-10.1177_02692155221138916 - Supplemental material for Effects of transcutaneous electrical acupoint stimulation on upper-limb impairment after stroke: A randomized, controlled, single-blind trial
Supplemental material, sj-pdf-1-cre-10.1177_02692155221138916 for Effects of transcutaneous electrical acupoint stimulation on upper-limb impairment after stroke: A randomized, controlled, single-blind trial by Hewei Wang, Yuzhi Xiang, Chuankai Wang, Yingying Wang, Shugeng Chen, Li Ding, Qiang Liu, Xiaowen Wang, Kun Zhao, Jie Jia and Yao Chen in Clinical Rehabilitation
Footnotes
Acknowledgments
The authors thank all patients and therapists who participated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This trial was financially supported in part by the General Research Project of Shanghai Municipal Health and Family Planning Commission (Grant Nos. 202040034 and 201540197); in part by the Medical research project of Shanghai Jing'an District Health Commission and District Science and Technology Commission (Grant No. 2020MS17); in part by the Key Subjects Construction Program of the Health System in Jing'an District (No. 2021PY04); in part by the National Key R&D Program of China (Grant No. 2018YFC2002301); in part by the China National Nature Science Young Foundation (Grant No. 82102665); and in part by Shanghai Sailing Program (No. 21YF1404600). The authors have no financial conflicts of interest.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.