
Abstract
Objective
To examine the trajectory of the Rating of Everyday Arm-use in the Community and Home (REACH) scores over the first-year post-stroke, determine if REACH scores are modified by baseline impairment level and explore the responsiveness of the REACH scale through hypothesis testing.
Design
Consecutive sample longitudinal study.
Setting
Participants were recruited from an acute stroke unit and followed up at three, six, and 12 months post-stroke.
Participants
Seventy-three participants with upper limb weakness (Shoulder Abduction and Finger Extension score ≤ 8).
Main Measures
The REACH scale is a six-level self-report classification scale that captures how the affected upper limb is being used in one's own environment. The Fugl-Meyer Upper Limb Assessment (FMA-UL), Stroke Upper Limb Capacity Scale (SULCS), accelerometer-based activity count ratio and Global Rating of Change Scale (GRCS) were used to capture upper limb impairment, capacity, and use.
Results
The following proportions of participants improved at least one REACH level: 64% from baseline to three months, 37% from three to six months and 13% from six to 12 months post-stroke. The trajectory of REACH scores over time was associated with baseline impairment. Change in REACH had a moderate correlation to change in SULCS and the GRCS but not FMA-UL or the activity count ratio.
Conclusions
Results of hypothesis testing provide preliminary evidence of the responsiveness of the REACH scale. On average, individuals with severe impairment continued to show improvement in use over the first year, while those with mild/moderate impairment plateaued and a small proportion decreased in the early chronic phase.
Introduction
The Rating of Everyday Arm-use in the Community and Home (REACH) scale is a quick-to-administer self-report classification scale that captures how the affected upper limb is being used in real life. In a previous cross-sectional study among individuals with chronic stroke, the REACH scale demonstrated strong inter-rater and test-retest reliability and was strongly correlated with measures of upper limb impairment, capacity, and self-report use. 1 By design, the number, and content of the REACH scale levels were generated to differentiate between meaningful levels of use. This was accomplished by obtaining descriptions of use via focus groups with clinicians and individuals with varying levels of upper limb stroke impairments. 1 Our previous work also showed that the minimal detectable change (MDC95) was 0.75, which provides further support that a change in one level in the REACH scale can be considered a true change in how the arm is being used. 1
To our knowledge, only one study has used the REACH scale to look at longitudinal changes in upper limb use. Assadi et al. 2 measured differences in use between admission to inpatient rehabilitation and six weeks post-stroke and found the median REACH score changed from 2.5 points to 4.0 points respectively. It is unknown however how the REACH score changes over more biologically informed time points that start early and progress into the chronic phase of recovery. 3 Recent longitudinal studies that captured changes in real-world use over the first six months to two years post-stroke have found that the greatest changes occurred in the earlier time points.4–6 In addition, the amount of impairment has been observed to affect levels of sensor-based upper limb use obtained over time5,6 and to modify changes in use over time. 6 It is unknown how baseline impairment levels affect how the arm is being used over the first-year post-stroke or how different levels modify changes in this type of use. Finally, longitudinal studies that capture changes in a construct over a period in which change is expected to occur may provide evidence of that outcome measure's ability to capture changes over time. 7 Thus, the objectives of this study are to examine the responsiveness of the REACH scale by investigating the trajectory of change in REACH scores within the first-year post-stroke and to determine if the level of baseline upper limb impairment affects the trajectory of change.
Methods
Study design
This study pooled data from two prospective observational studies examining upper limb recovery in the first-year post-stroke from the same site. The Characterizing Arm Recovery in People with Severe Stroke study was designed to examine upper limb recovery among individuals with severe stroke only. 8 The REACH longitudinal study was designed to examine the responsiveness of the REACH scale. Ethics approval was obtained for both studies from the university and hospital review boards and all participants provided written informed consent.
Population
All individuals with a suspected diagnosis of stroke admitted to the stroke unit of a tertiary hospital (Vancouver General Hospital) between January 2016 to December 2018 were screened for inclusion. Participants recruited to the Characterizing Arm Recovery in People with Severe Stroke study from January 2019 to March 2020 were also included in this dataset due to the known complexity of recruiting and retaining individuals with severe stroke. 9 Inclusion criteria were: (1) diagnosis of ischemic stroke or intracerebral hemorrhage confirmed by CT or MRI and medically stable; (2) 19 years or older; (3) able to provide informed consent; (4) less than 30 days post-stroke; and (5) have new upper limb weakness as defined by a Shoulder Abduction Finger Extension score of 8 or less. Individuals were excluded if they had any of the following: (1) subarachnoid hemorrhage; (2) another neurological condition (e.g. Parkinson's); (3) upper limb comorbidity (e.g. fracture); (4) unable to participate in follow-up sessions; (5) serious medical condition that would affect the ability to participate (e.g. active cancer), or (6) bilateral weakness. The Shoulder Abduction Finger Extension score was obtained by the unit physical therapists, who were trained in its administration and scoring, for the purpose of screening into both longitudinal studies. Individuals with severe stroke recruited to the Characterizing Arm Recovery in People with Severe Stroke study in 2019–2020 and included in this analysis had the same inclusion as above but were also excluded if they had a Shoulder Abduction Finger Extension score≥4, recurrent stroke or were greater than 90 years old. In addition, attempts were made to recruit patients within 30 days post-stroke. However, if circumstances precluded this (e.g. health reasons or discharge), participants were enrolled when it was safe and possible to do so.
Outcomes
Each participant underwent four testing sessions at the following time points: (1) baseline; (2) three months post-stroke; (3) six months post-stroke, and (4) 12 months post-stroke. Demographic and stroke information including age, sex, date and type of stroke, stroke severity, and medical interventions received were collected at baseline from the medical chart. All other assessments were administered by a trained physical or occupational therapist or research staff. Upper limb impairment was captured using the upper limb portion of the Fugl-Meyer. This measure consists of 33 items rated on a 3-point scale from 0 (cannot perform) to 2 (performs fully) for a total of 66 points. 10 The Stroke Upper Limb Capacity Scale was used to capture upper limb capacity and consists of 10 items rated on a 2-point scale from 0 (cannot perform) to 1 (can perform). 11 Upper limb use was captured using the REACH scale, Global Rating of Change Scale and accelerometers. Participants were first administered the Global Rating of Change Scale at time point 2. This scale asked participants to rate the level of change in their amount of arm use on a 6-point scale from 0 (no change) to 5 (very much more/less) since they first had their stroke.
Participants were asked to wear accelerometers on both wrists for one day at the baseline assessment and three consecutive days at the follow-up assessments. Actical accelerometers (Phillips Respironics, Pennsylvania, USA) were used for the REACH-Longitudinal participants and Actigraph 3GTx accelerometers (ActiGraph, Florida, USA) were used for the Characterizing Arm Recovery in People with Severe Stroke study participants. Both accelerometer brands are triaxial accelerometers which measure acceleration in all three movement planes. The Actical accelerometers integrate the accelerometer signal from all three axes and provide a single activity count for a 15-second epoch using a proprietary algorithm. The Actigraph accelerometers provide an activity count over a 1-second epoch for each axis using a proprietary algorithm. Actigraph activity counts from all three axes were then combined for each second using the following equation:
Statistical analyses
Linear mixed effects modeling was used to explore the trajectory of REACH scores in the first-year post-stroke using the subject as the random effect. Specifically, we generated three sequential models. Model 1 was the crude model with time input as the only fixed effect to examine the trajectory of REACH scores over time for the full sample. Time was input as a categorical variable to allow for a non-linear change in REACH scores. Baseline (time 1) was used as the referent time point. The second model included the interaction between time and baseline impairment, dichotomized into severe and mild/moderate levels, to examine the effect of baseline impairment on the trajectory of change in REACH scores. The severe impairment group was defined by baseline Fugl-Meyer Upper Limb scores of 10 or less and the mild/moderate impairment group was defined by scores of 11 and greater. 13 Finally, age and sex were added to the interaction model to examine their effect on REACH scores. Linear mixed-effects models were selected due to their ability to handle missing data and provide interpretable trajectories over time within the sample size constraints of this hypothesis-generating study. Bivariable logistic regressions were conducted to explore differences in demographics and clinical characteristics (i.e. age, sex, side of weakness, type of stroke, dominant affected, baseline impairment and use) between the participants who did (n = 55) and did not (n = 18) continue in the study beyond the three-month timepoint.
Recent guidelines developed by the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) initiative recommend that responsiveness be directly examined by generating hypotheses about the expected change scores. 14 When no gold standard measure of the construct exists, the guidelines recommend using a construct approach to hypothesis testing such as generating hypotheses about the expected direction and magnitude of correlations between change scores or about the size of expected differences in change scores between known groups. Evidence for construct validity is stronger as the quantity and specificity of hypotheses increase. 15 Six hypotheses were generated to examine the responsiveness of the REACH score. The first column in Table 1 provides the hypotheses and their rationale. Correlations for hypotheses 1–4 were measured using Spearman's rho and scatterplots. Change scores between baseline and three months post-stroke were examined in hypotheses 1–4 to maximize the number of people who experienced a change in the analysis. Mean differences in change scores for hypotheses 5 and 6 were obtained from the linear mixed effects models. Specifically, values for hypothesis 5 were obtained from model 1 and values for hypothesis 6 were obtained from model 2. All analyses were conducted using R (version 4.1.1).
Responsiveness hypotheses.
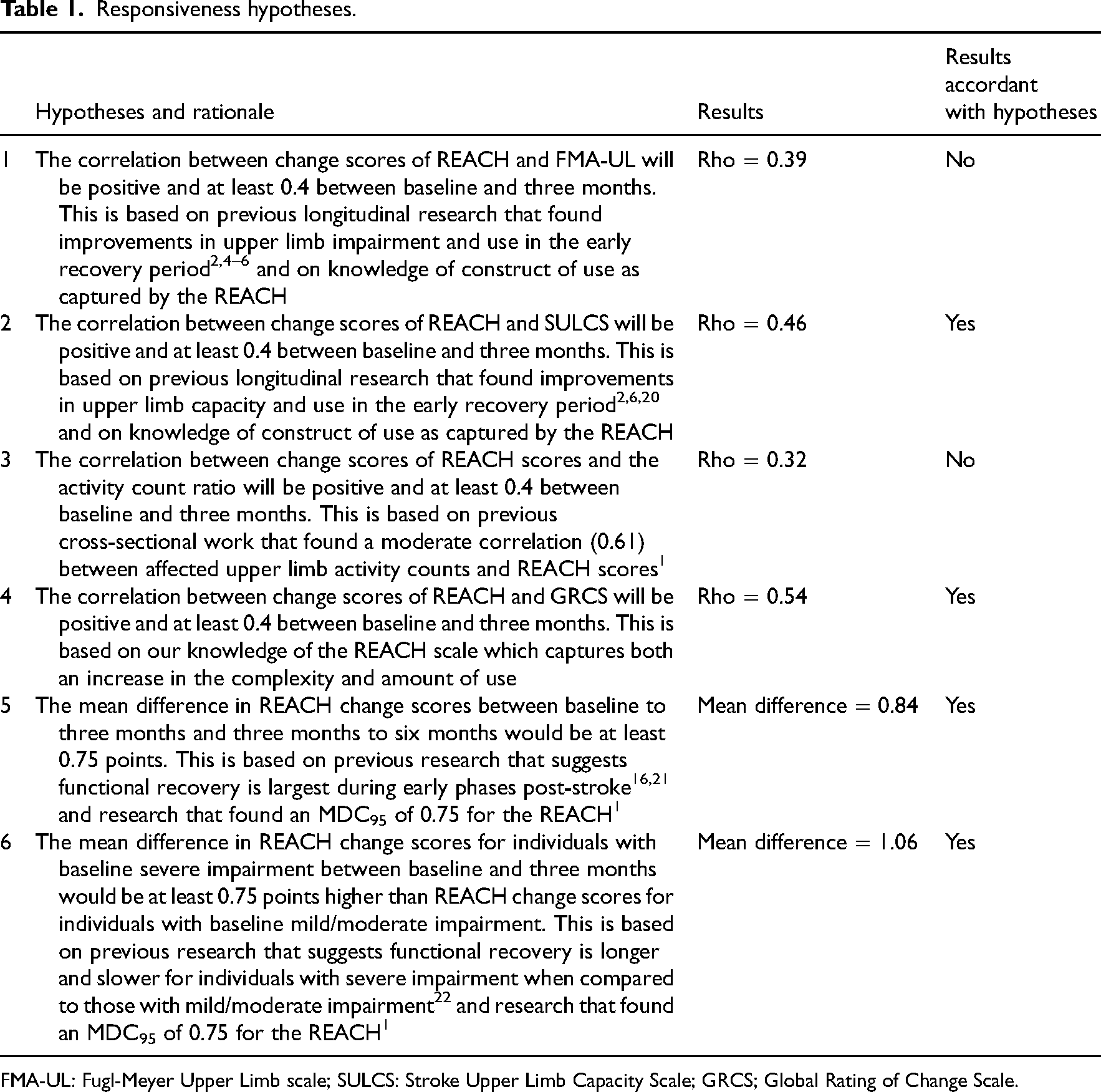
FMA-UL: Fugl-Meyer Upper Limb scale; SULCS: Stroke Upper Limb Capacity Scale; GRCS; Global Rating of Change Scale.
Results
Study participants
A total of 2888 individuals were screened for study inclusion between January 2016 and March 2020 and a total of 73 individuals enrolled in the two studies (Figure 1). The most common reason for exclusion was too little arm weakness. Table 2 outlines the demographic and clinical characteristics of enrolled participants by baseline impairment category. Approximately 30% of our sample had severe baseline impairment according to a baseline upper limb Fugl-Meyer score of 10 or less.
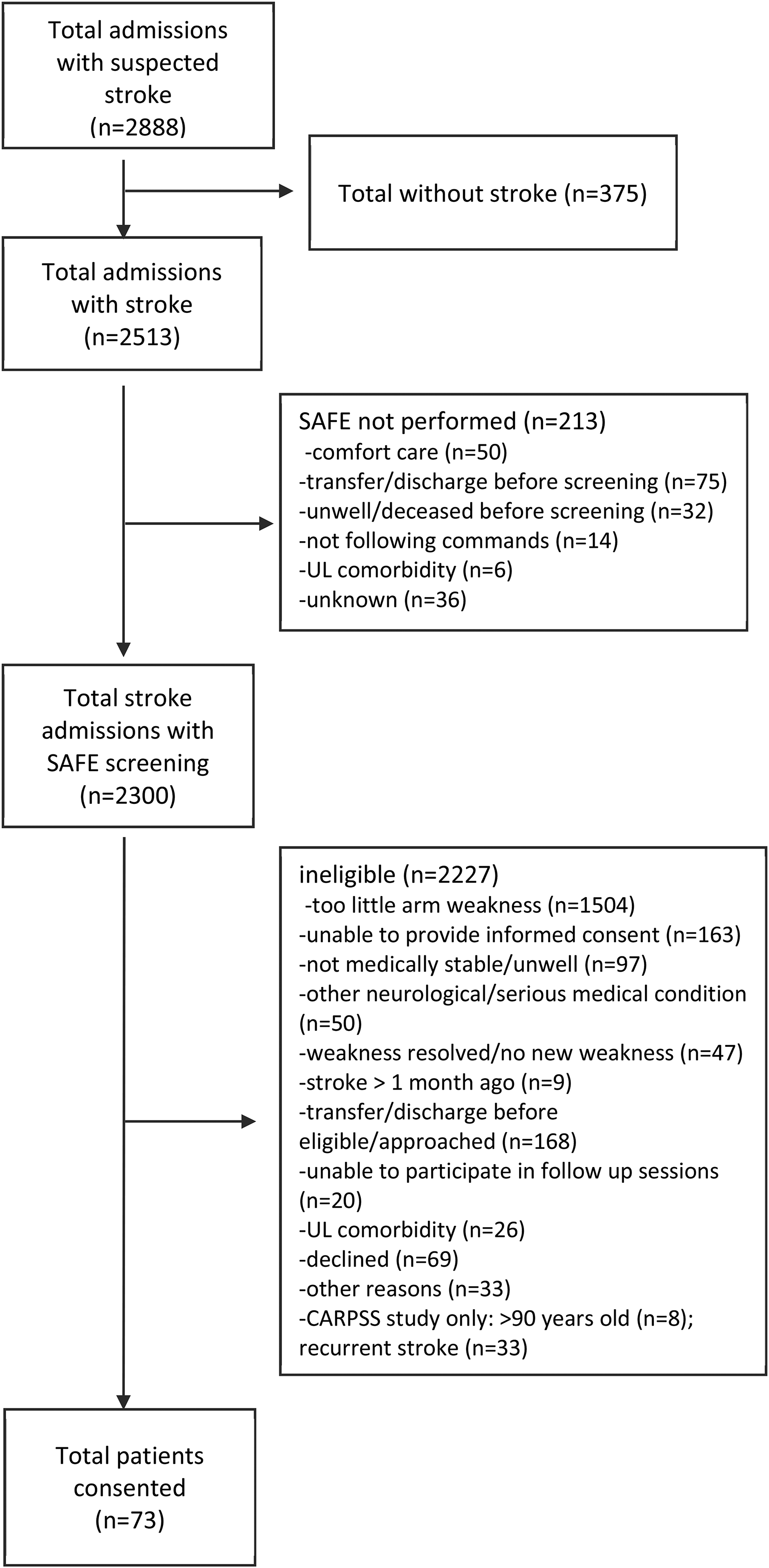
Summary of included participants.
Baseline demographic and clinical characteristics by impairment category.
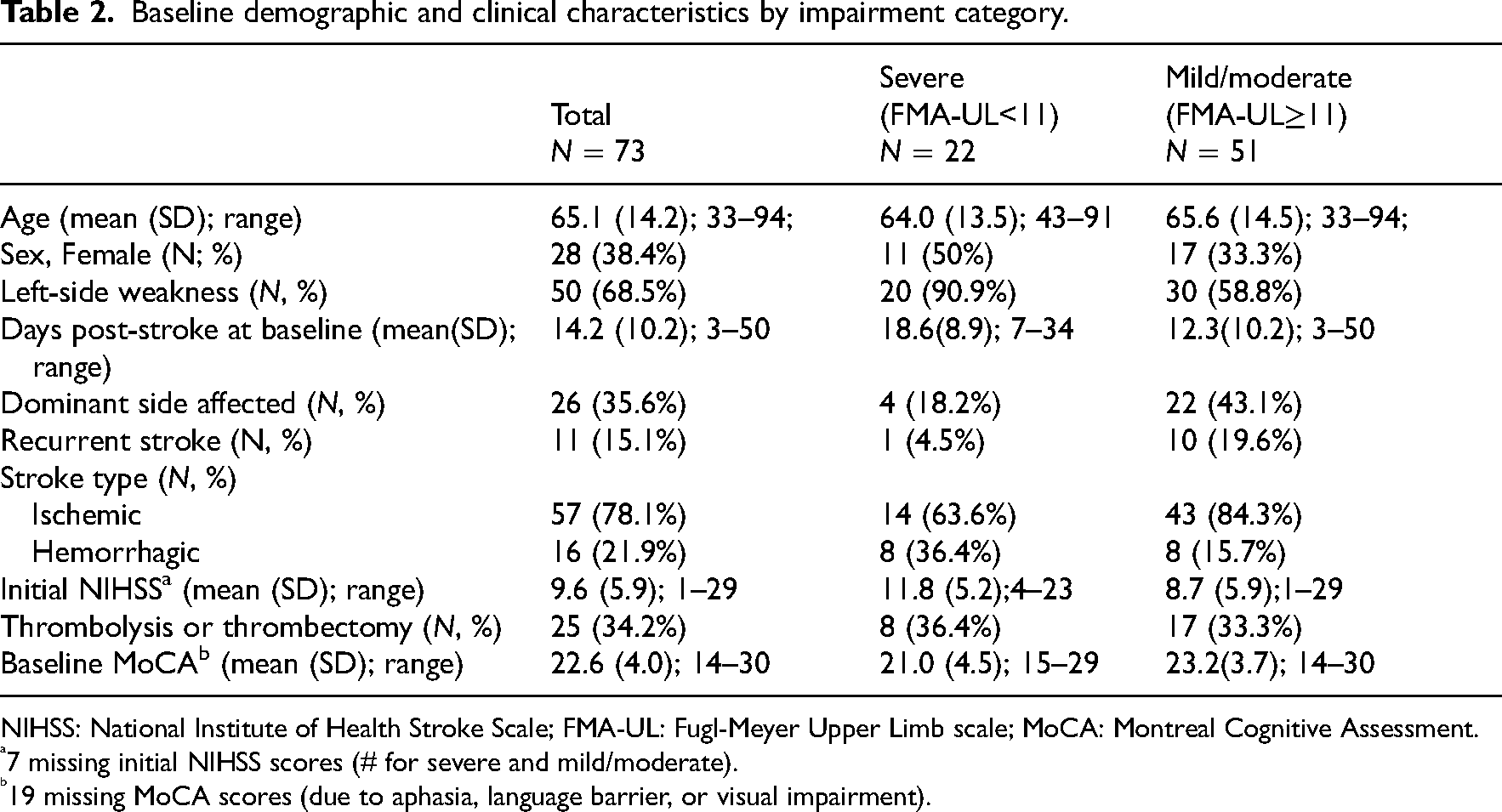
NIHSS: National Institute of Health Stroke Scale; FMA-UL: Fugl-Meyer Upper Limb scale; MoCA: Montreal Cognitive Assessment.
7 missing initial NIHSS scores (# for severe and mild/moderate).
19 missing MoCA scores (due to aphasia, language barrier, or visual impairment).
Trajectory of REACH scores over time
On average, the assessments were collected at 14.2 (SD = 10.2), 98.1 (SD = 14.4), 194.9 (SD = 34.7) and 376.1 (SD = 19.4) days post-stroke which approximate the two weeks, three months, six months, and 12 months timepoints respectively. Over the four time points, we obtained 234 of the 292 REACH values (80.1%). We observed 83.6% retention at three months, 72.6% at six months and 64.4% at 12 months. A greater proportion of individuals with left-sided weakness had missing data beyond the three-month time point however age, sex, type of stroke, dominant side affected, baseline impairment and REACH scores were not associated with the odds of missing data beyond the second time point (Supplementary Table S1).
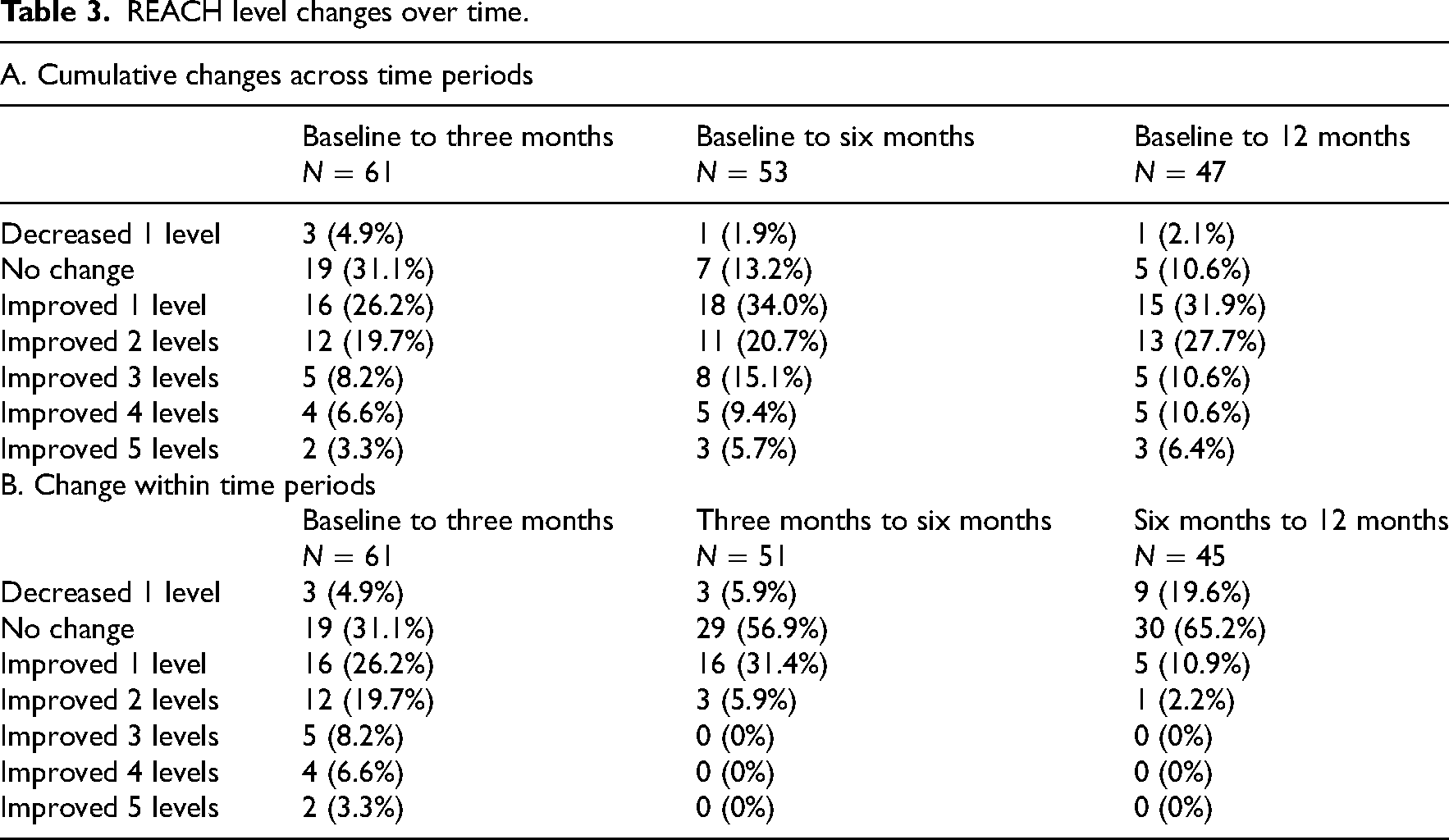
Approximately 87% of the participants experienced an improvement in their REACH score by 12 months post-stroke (Table 3A). Improvement was operationalized as an increase of at least one level. Relative to baseline, one participant decreased their score and five participants experienced no changes in their REACH score by 12 months. Table 3B displays changes in REACH levels within each of the three assessment intervals. The greatest number of participants improved their REACH score from baseline to three-months post-stroke (64%). This is in contrast to 37.3% and 13.1% who improved at least one level between three to six months and six to 12 months post-stroke. Within each time interval, a gain in one level was the most common shift experienced by participants who improved. Shifts beyond one level were mainly restricted to the baseline to three months interval. For instance, a total of 38% of individuals improved more than one level between baseline and three months compared to 6% between three and six months and 2% between six and 12 months post-stroke. Individuals who improved more than one REACH level between the first two time points were largely those with baseline mild/moderate level impairment (91%). Finally, the greatest percentage of participants decreased a level during the six-to-12-month period (19.6%) compared to the baseline to three month and three-to-six-month periods (4.9% and 5.9% respectively). All those individuals who declined one level between six and 12 months interval had baseline mild/moderate impairment and thus the majority (8/9) involved decreasing from higher REACH levels (i.e. decreasing from level three and higher).
REACH level changes over time.
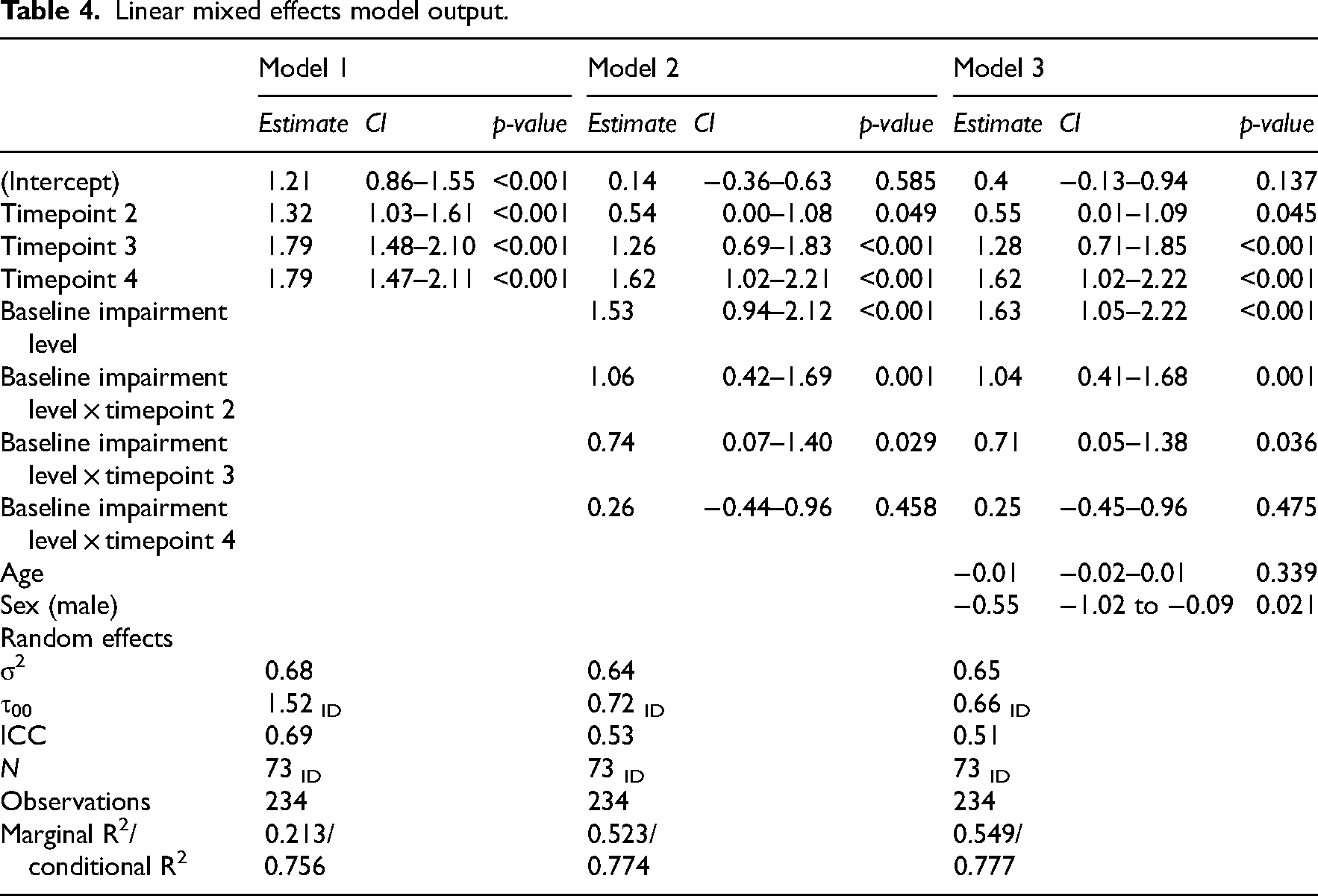
The final linear longitudinal model shows the trajectory of REACH scores over the first-year post-stroke for the severe and mild/moderate impairment groups while controlling for age and sex (Table 4/Figure 2). Table 4 also displays the crude longitudinal model. The average REACH score in the mild/moderate group was statistically significantly higher than the severe impairment group at all time points (Figure 2). In addition, the amount of change in the average REACH score from baseline to approximately three and six months are different for the two impairment groups as evidenced by the significant time by severity interaction term at these time points (three months: 1.04; 0.41–1.68; p = 0.001; six months: 0.71; 0.05–1.38; p = 0.036). The time by-group interaction term was not significant at the 12-month time point indicating the amount of change from baseline to approximately 12 months was not different (0.25; −0.45–0.96; p = 0.475) for the two groups. Finally, being male was associated with lower mean REACH scores when time point, impairment group and age were held constant (mean difference −0.55; −1.02 to −0.09; p = 0.021). Please refer to Supplementary Table S2 for frequencies of REACH scores over time for the full sample and by baseline severity group.
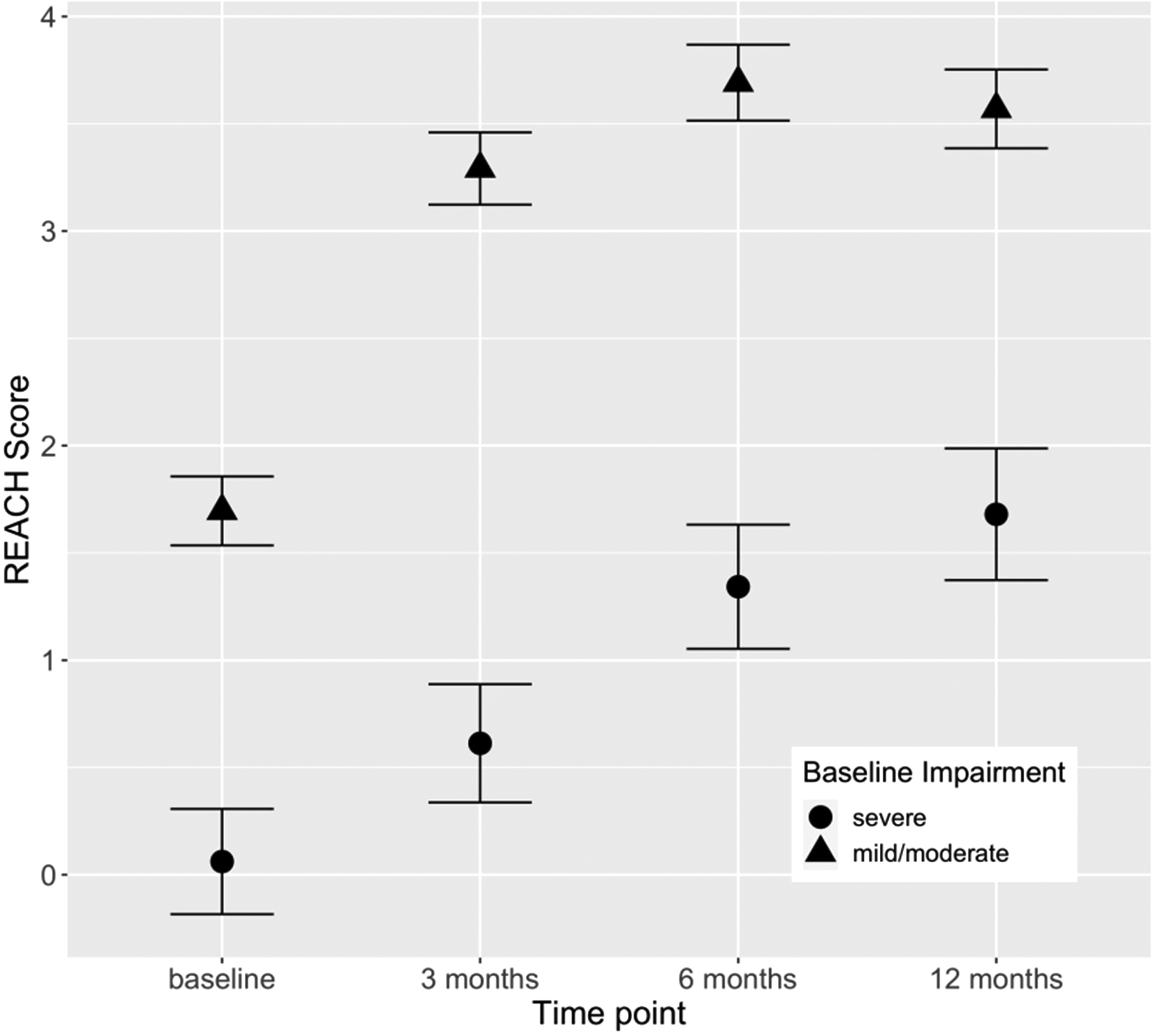
Predicted REACH scores over the first-year post-stroke. REACH Scale Levels: 0-no use/exercise only; 1-assist or easy reach; 2-some reach and grasp with hand manipulation; 4-everyday use unless potential negative consequences; 5-full use. Points (circles and triangles) represent predicted mean REACH scores at the four timepoints for the respective impairment groups obtained from the final linear mixed effects model (i.e. model 3 in Table 4). Intervals indicate + /− one standard error.
Linear mixed effects model output.
Responsiveness hypothesis testing
Table 1 displays the results of the hypotheses testing and Figure 3 displays the scatterplots of score changes between the REACH scale and other measures of impairment, capacity and use. Four out of six hypotheses were accordant with the results. For instance, the correlations between REACH change scores and change scores of the Stroke Upper Limb Capacity Scale (i.e. capacity) and the Global Rating of Change Scale (i.e. self-report change in amount of use) were moderate. In addition, mean differences in change scores surpassed the MDC95 of 0.75 between the severe and mild/moderate impairment groups and between the earliest and later time intervals (i.e. baseline to three months vs three to six months post-stroke). The correlation between the change in REACH and (1) change in upper limb Fugl-Meyer (0.39) and (2) activity count ratios (0.32) were weaker than 0.4. Unexpectedly, there were relatively large improvements in the upper limb Fugl-Meyer and Stroke Upper Limb Capacity Scale among the three participants that reduced their REACH level from baseline to three months. (Figure 3A).
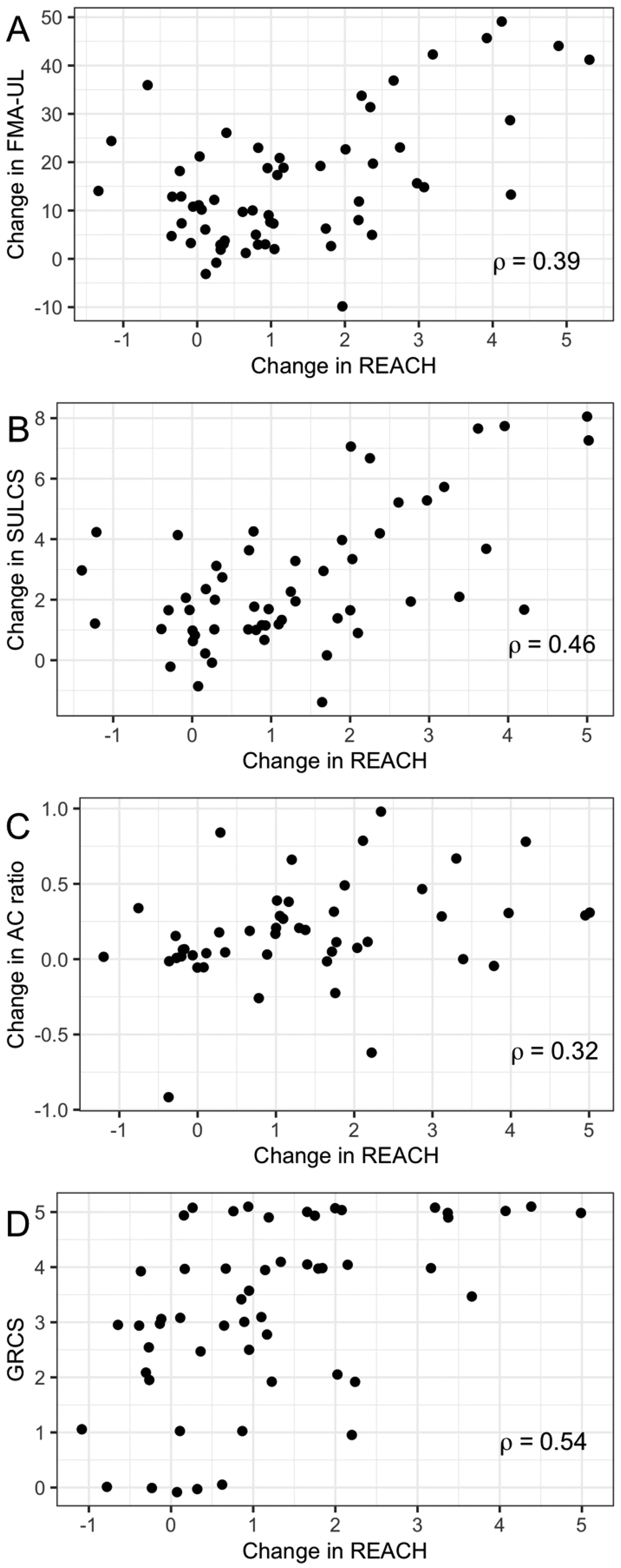
Scatterplots of change scores in REACH and measures of upper limb impairment, capacity, and use between baseline and three months post-stroke. Note: REACH: Rating of Everyday Arm-use in the Community and Home Scale; FMA-UL: Fugl-Meyer Upper Limb Assessment; SULCS: Stroke Upper Limb Capacity Scale; AC: activity counts; GRCS: Global Rating of Change Scale; A: n = 61; B: n = 56; C: n = 25; D: n = 54.
Discussion
Our findings were in accordance with four of our six hypotheses which provide preliminary evidence to support the responsiveness of the REACH scale. Specifically, the REACH scale was able to detect differences in arm use changes in the early versus later phases post-stroke. This is consistent with previous longitudinal studies, which found that the largest changes in upper limb use and impairment occurred in the early phases post-stroke.5,6,16,17 In addition, the REACH scale was able to detect differences in arm use early post-stroke for individuals with severe versus mild/moderate baseline impairment. Differences in upper limb use between severity groups were previously observed in the study by Lang et al., 6 whereby greater levels of upper limb capacity, which is highly correlated to upper limb impairment, were associated with greater levels of upper limb use and faster rates of change. Detection of these two important differences suggests that clinicians can be more confident that the REACH scale will pick up changes during standard rehabilitation when they occur. Moreover, progression through the REACH scale involves performance of more complex upper limb movements and thus it is expected that greater functional recovery would be associated with greater increases in complexity of use. The moderate correlations between change scores in the REACH and change scores in capacity and self-reported amount of use can increase clinicians’ confidence that the REACH scale is picking up changes in complexity of use as expected.
The magnitude of correlations between change scores in the REACH and change scores in upper limb impairment and activity counts were lower than expected. One possible explanation is that participants were overestimating their use at baseline. Although the risk for under or over-reporting is present for any self-report measure at any time, the risk may be highest early post-stroke when cognitive and perceptual issues may be more pronounced. Although the therapists were trained to probe deeper when an individual's impairment/functional abilities did not match their reported use, some participants’ perception of their use still may have been higher than reality. We recommend therapists and researchers use all information during an assessment (including spontaneous use of the affected upper limb) to assist in generating probing questions and/or potentially supplement with information from caregivers. The three individuals who declined a REACH level between baseline and three months post-stroke may have overestimated their use at baseline. When these three individuals were removed, the correlation between change scores in the REACH and change scores in the Fugl Meyer Upper Limb scale and activity count ratio increased to 0.52 and 0.36 respectively.
Finally, through examining the trajectory of REACH scores across the first-year post-stroke, we found that upper limb use started and ended at different levels for individuals with severe versus mild/moderate impairment throughout the study period. For those with baseline severe impairment (i.e. Fugl Meyer Upper Limb scale <11), use of the upper limb at six to 12 months post-stroke may more commonly involve using that limb as a stabilizer or simple assist to the other limb during daily activities (i.e. REACH level 1 or 2). In contrast, by six or 12 months post-stroke, upper limb use for individuals with mild/moderate impairment levels may more commonly involve more complex reaching and grasping activities or using that limb for the majority of activities unless there is potential for negative consequences such as causing injury or mistakes (i.e. REACH level 3 or 4). Moreover, on average, the REACH scores for those with baseline severe impairment increased over the first year versus a more curvilinear pattern observed in individuals with baseline mild/moderate impairment. Importantly, it appears that in the early chronic phase post-stroke, some individuals with baseline mild/moderate impairment may decrease a REACH level. This phase post-stroke corresponds to a time of observed plateau in upper limb impairment and capacity6,18 and a time when formal upper rehabilitation has usually ceased. We do not know whether biological processes and/or a lack of rehabilitation is driving these decreases in use for these individuals. However, understanding how the arm is being used in the home and community through measurements such as the REACH scale can help the therapist ensure the arm is being used to its capacity and thus help to prevent loss of any functional gains.
The following limitations must be acknowledged. We did not use a specific score on a cognitive screening measure as inclusion criteria for this study due to their heavy reliance on language skills. 19 This might have skewed some of the relationships between changes in the REACH to changes in other measures. Conversely, despite not restricting participants to high cognitive scores, we were still able to observe changes in the REACH that are consistent with many of our hypotheses and with known trajectories of upper limb impairment and capacity. Finally, we used two different accelerometers in this study to capture changes in upper limb use. There may be differences in the algorithms used to generate activity counts that may have affected the correlations between change scores in the REACH and activity count ratios.
Clinical messages
Preliminary evidence supports the responsiveness of the REACH scale over the first-year post-stroke.
Complexity of upper limb use increases over the first-year post-stroke.
On average, individuals with severe impairment continued to show improvement in use over the first year, while those with mild/moderate impairment plateaued and a small proportion decreased in the early chronic phase.
Supplemental Material
sj-docx-1-cre-10.1177_02692155221134413 - Supplemental material for Responsiveness and trajectory of changes in the rating of everyday arm-use in the community and home (REACH) scale over the first-year post-stroke
Supplemental material, sj-docx-1-cre-10.1177_02692155221134413 for Responsiveness and trajectory of changes in the rating of everyday arm-use in the community and home (REACH) scale over the first-year post-stroke by Lisa A Simpson, Kathryn S Hayward, Lara A Boyd, Beverley C Larssen, W Ben Mortenson, Amy Schneeberg, Noah D Silverberg and Janice J Eng in Clinical Rehabilitation
Footnotes
Acknowledgments
The authors would like to acknowledge Moira McPeake, Sue Peters, and the Vancouver General Hospital acute stroke program for their assistance with screening the patients and for their overall support of the study.
Author contributions
All authors read, edited, and approved the final version of the article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the Canadian Institutes of Health Research Foundation Grant, Canadian Institutes of Health Research Project Grant (grant numbers FDN 143340 and PJT-153330).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.