
Abstract
Introduction
Exercise can decrease fall risk in older adults but less is known about training to reduce injury risk in the event a fall is unavoidable. The purpose of this study was to compare standard fall prevention exercises to novel Fall Arrest Strategy Training (FAST); exercises designed to improve upper body capacity to reduce fall-injury risk in older women.
Method
Forty women (mean age 74.5 years) participated in either Standard (n = 19) or FAST (n = 21) twice per week for 12 weeks. Both interventions included lower body strength, balance, walking practice, agility and education. FAST added exercises designed to enhance forward landing and descent control such as upper body strengthening, speed and practice of landing and descent on outstretched hands.
Results
Both FAST and Standard significantly improved strength, mobility, balance, and fall risk factors from pre to post-intervention. There was a significant time by group interaction effect for upper body response time where FAST improved but Standard did not (p = 0.038).
Discussion
FAST resulted in similar gains in factors that reduce fall risk as a standard fall prevention program; with the additional benefit of improving speed of arm protective responses; a factor that may help enhance landing position and reduce injury risks such as head impact during a forward fall.
Introduction
Determining effective and feasible interventions to prevent the downward spiral of failing health, admission to long-term care and even death following a serious fall-related injury is important to older adults, the health care team, policy makers and the public at large. Exercise programs focused on balance, strength and functional mobility decreases fall risk and improves fall risk factors in community-dwelling older adults1,2; however the impact of training other modifiable aspects of injury protection such as response time and effective landing and descent strategies is unknown.
The risk of injury from falls depends on both the severity of impact and neuromuscular capacity such as bone and muscle strength of the affected body part.3,4 Women are at higher risk of fall-related injuries than men and are much more likely to sustain upper limb fractures from a fall. 5 The majority of reported falls in community-dwelling older women is forward, commonly due to tripping. 6 Forward falls usually occur with hand contact as a protective response to prevent head, hip or torso injury. 4 The effectiveness of these upper body protective strategies, including response time, unfortunately decreases with ageing. 7 Video surveillance studies in long-term care facilities have observed a high number of falls where head impact occurred with hand impact, but in the majority of observed falls, older adults were unsuccessful in utilizing the arms to prevent head impact, suggesting an ineffective protective response to prevent brain injury. 8
There is growing evidence supporting interventions such as perturbation training designed to enhance lower extremity postural reactions in decreasing fall risk and fall rates in older adults and clinical populations, 9 but little is known about the effect of training upper body strength, response time and landing capacity to reduce fall and injury risk. Younger adults can modify forward fall arrest strategies to improve safe landing and reduce hand and wrist impact forces by learning to land with a “soft” slightly flexed elbow, “catching the ground”, and a controlled descent.10,11 Other factors such as pre-impact configuration of the body may also be important to reduce injury risk. 4 The critically important question is whether fall arrest training practice focused on enhancing upper body and upper extremity strength, response time and landing strategies, can enhance older adults’ ability to react and effectively control a forward fall and diminish the risks of serious injury such as head injury.
The purpose of this study was to compare the effects of Fall Arrest Strategy Training or FAST, to Standard fall prevention exercise on fall risk factors including upper body strength, mobility and response time, in older women.
Method
A randomized design compared effects of two interventions on fall and injury risk variables of interest (clinicaltrials.org NCT04844047). Ethics approval was received by the University of Saskatchewan, Saskatoon, Canada Biomedical Ethics Review Board (Bio 16–72) and all participants signed consent prior to testing. Women aged 60 years or older were recruited via announcements and posters in the community in 2016–2017. Exclusion criteria included upper body injury or pain within the last six months, any fracture within the past year, a history of a distal radial fracture in the past two years or any history of more than one distal radial fracture, history of upper extremity neurological conditions or medical conditions contradicting strength testing or training, signs of severe cognitive impairment or unable to safely ambulate independently in the community. A screening questionnaire as well as the Mini-Cog 12 determined presence of any of the exclusion criteria noted above. Eligible participants were randomly assigned 1:1 to FAST or Standard by someone not directly involved in the study using a computer generated random allocation (https://www.randomizer.org). Participants received a sealed envelope with group assignment after pre-testing, prior to commencement of the intervention. Trained testers, blinded to group assignment, conducted testing at a laboratory-testing site. Outcome measures for strength, mobility, response time and fall risk are described below. There were two cohorts resulting in four interventions: Two Standard and Two FAST.
Upper extremity muscle strength
Functional multi-joint upper extremity muscle strength measures reflected the muscle action, positioning and activation similar to the descent control required for a forward fall arrest.13,14 Three trials of concentric pushing and eccentric resisting (Figure 1) were obtained utilizing an isokinetic dynamometer (Humac NORM Isokinetic Dynamometer, CSMi, Stoughton, MA) and a standardized protocol as described in previous publications with excellent test re-test reliability (Intraclass correlation coefficient = 0.98; 0.97). 14 The Push Off Test (Figure 2), originally described by Vincent et al., 15 used a calibrated handgrip dynamometer (Model #5030J1, JAMAR, DMM Canada) with the handle reversed, to measure the ability to push down on a stable surface. Angle of elbow flexion and shoulder extension were standardized (Intraclass correlation coefficient = 0.92–0.94). 14 Composite scores (Left mean of three trials + Right mean of three trials) were used for all strength measures.
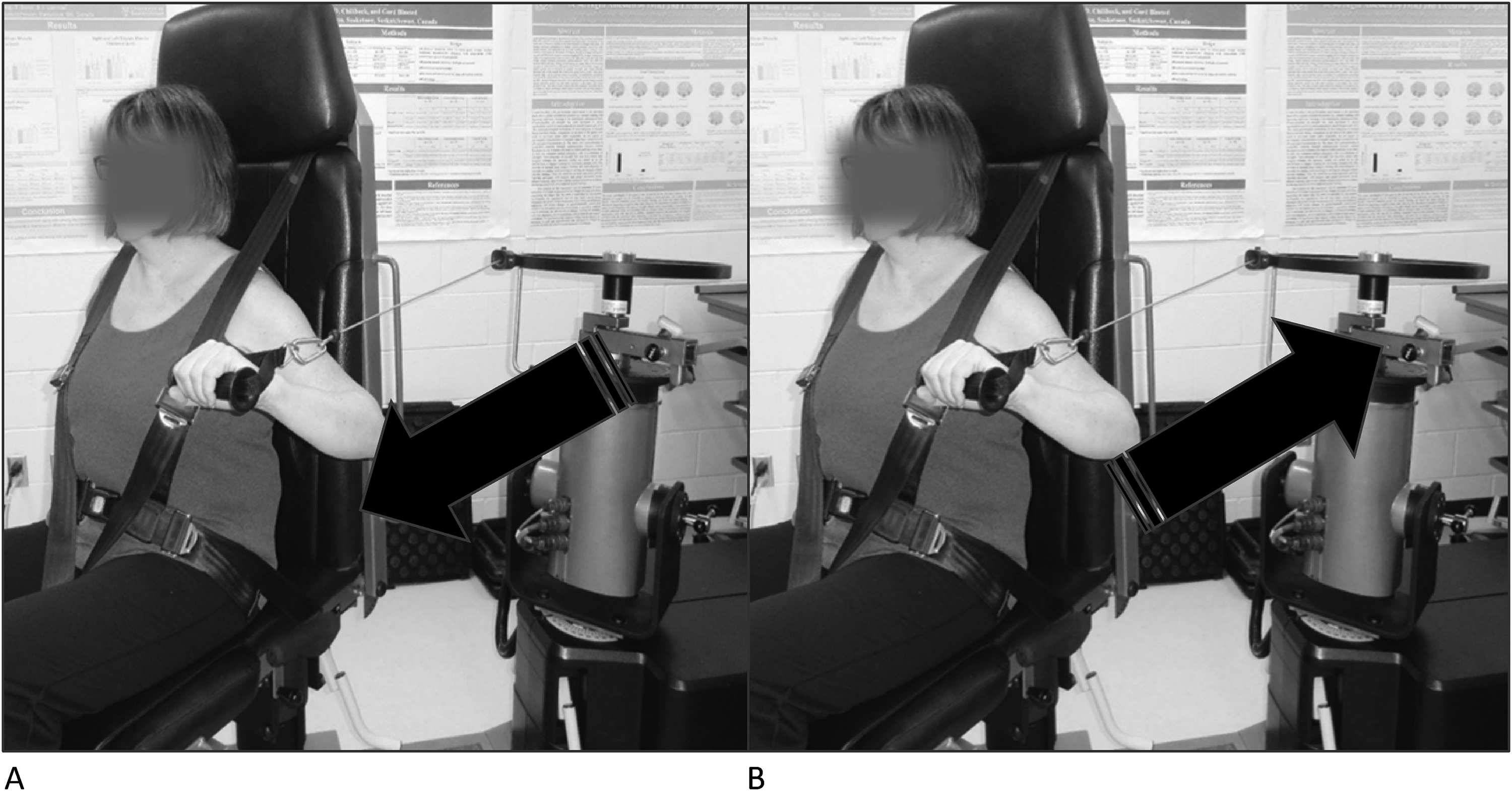
Concentric muscle strength test (A) and eccentric muscle strength test (B).
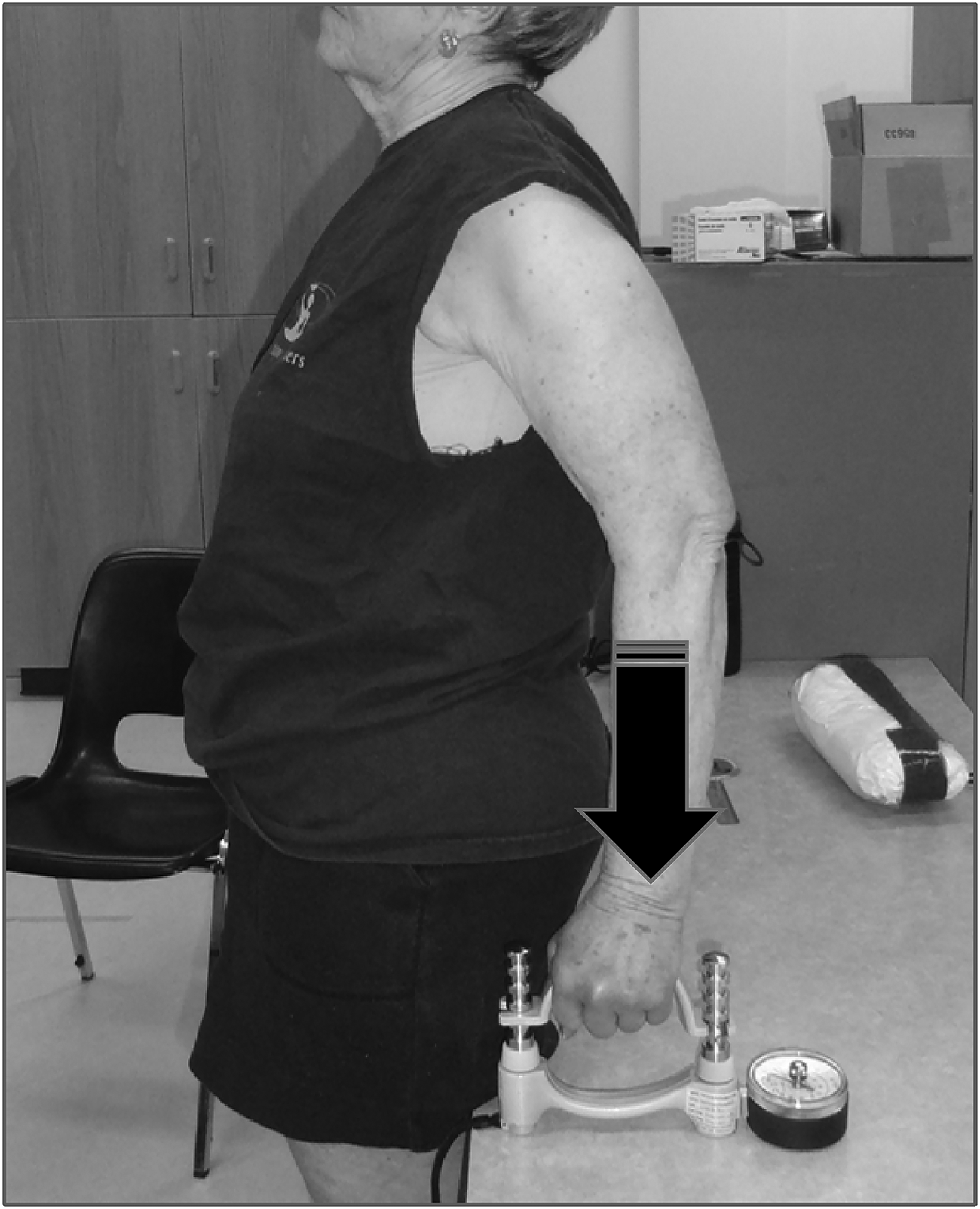
Push off test.
Upper extremity mobility
Wrist extension and shoulder extension range of motion (active motion with passive overpressure) were measured with the participant sitting on a standard chair with no armrests, using a manual goniometer and a standardized protocol. 16 Composite scores (Left mean of two trials + Right mean of two trials) were used for shoulder extension and wrist extension mobility.
Upper extremity response time
From a standing position with arms by their side, participants responded to an audible signal with randomized timing (between one to five seconds; Figure 3) by reaching either left or right or both arms together, as fast as possible, to touch a target on dual force plates (fs = 2000 Hz, OR6-7, AMTI, Watertown, MA, USA). Force and audio signal timing data were synchronously collected on the same system. Target height just below shoulder height was standardized to the participants’ height and arm length. Upper extremity response time was defined as time from the audible signal to force plate contact. An average of five trials for each of left, right and both hands were used with excellent inter-trial reliability. 17

Measurement of upper extremity response time.
Fall risk factors
There were five standard measures used for fall risk. The Fall Risk for Older People in the Community questionnaire, a valid and reliable measure of multi-factorial fall risk status was administered via interview. 18 The Timed Up and Go test is a reliable and valid measure of fall risk and functional ability (Intraclass correlation coefficient = 0.99). 19 Total time was recorded after one practice trial. The 30-s chair stand test 20 assessed the number of full sit to stand repetitions performed in 30 s without the use of arms. Test re-test reliability reported as intraclass correlation coefficient 0.84–0.92. 16 Balance was measured using one leg standing. 21 Participants were given two attempts to reach the maximum of 60 s on both legs and the average of two trials was recorded with a composite score (Left + Right) used for analysis. The Activities-Balance Confidence Scale 22 was used to monitor changes in balance confidence during daily living tasks.
History of falls, including details regarding the reason for the fall, injuries sustained and the direction of the fall were recorded using a standard questionnaire. 23 The Physical Activity Scale for the Elderly 24 monitored activity level outside of the intervention.
Intervention
The Standard intervention consisted of a fall prevention exercise program designed for community-dwelling older adults 25 focusing on balance, leg strength, walking and mobility exercises. FAST intervention included the same exercises as Standard, but also incorporated FAST goals as described below. Both groups received a half-hour fall prevention education session once per week and attended twice per week exercise, 45 min in length, for 12 weeks at two assisted living sites in the community. Women living on site as well as in the community participated. The same two instructors; licensed physical therapists with more than 10 years of experience in fall prevention programing, led both interventions.
The overall goal of FAST 25 was to increase fall-arrest capacity or the neuromuscular ability to prevent and minimize injury during a fall by: (1) Increasing upper body strength utilizing both concentric and eccentric contractions, (2) Improving trunk and neck postural control, and (3) Optimizing forward descent strategies for effective landing and controlled descent with hands. For example, exercises in FAST not included in Standard: (1) wall push-ups with controlled and quick body descents, (2) floor activities (as able) weight shifting on hands and knees, (3) shoulder and elbow strengthening with elastic bands and light weights, (4) wrist extension and shoulder extension stretches, and (5) quick upper extremity movement practice such as reaching activities, balloon and ball toss. Training progression for upper extremity strength and body control included increasing the distance standing from the wall, progressing to one arm descents, increasing reps and speed and moving to greater gravity and body weight resistance such as hands and knees position on the floor as able. For example, wall push-ups progressed as follows: both hands five repetitions, both hands 10 repetitions, move away from wall (body lean approximately 45 degrees) both hands five repetitions, progress to 10 repetitions. This sequence was repeated with one hand push-ups as able. Push-ups using greater resistance on the floor were started once participants could easily do 10 reps against the wall both hands at body lean of approximately 45 degrees and if able to get up and down from the floor independently. Rapid hand and arm motion started with quick reach and touch to the wall in a static standing position, to reaching quickly with both hands to the wall and descending the body in a controlled fashion. Further progressions included increasing repetitions from five to 10, starting with the body further from the wall, and increasing speed. Other challenges to reaction speed included ball toss and balloon games which were interspersed throughout the 12 weeks. Instructions were provided to participants to progress at their own pace. Instructors monitored and encouraged participants to not progress to increased challenges if there was a loss of correct technique, excessive fatigue or pain. Individual progressions were not recorded but participants were asked to self-monitor and report any concerns to the instructors.
Analysis
Based on previous pilot data, with an estimate of a 10% change in upper extremity strength, a sample size n = 22 per group was determined for an effect size 0.30, power = 0.90, α = 0.05). 25 Independent t-tests compared group pre-test values for age, height, weight, physical activity status, fall history status, and outcome variables. Intention to treat repeated measures MANOVA tests were used to determine time effects and group*time effects for the four primary outcome categories: (1) Upper Extremity Strength (concentric, eccentric, push-off test), (2) Upper Extremity Mobility (shoulder extension, wrist extension), (3) Upper Extremity Response Time (left, right, both) and (4) Fall Risk Factors (Fall Risk for Older People in the Community questionnaire, Timed Up and Go test, 30-s chair stand, one leg stand, and Activities-Balance Confidence Scale). Significance level was set at α = 0.05. Frequency and descriptive data described number of falls, number of injurious falls and fall direction. A one-way repeated measures ANOVA compared pre to post self report in the Physical Activity Scale for the Elderly.
Results
There were 21 women in FAST (age 73 ± 9 years) and 19 women in Standard (mean age 76 ± 7 years; Figure 4) with no significant differences between the groups for age, height, weight, body mass index, program attendance, physical activity status, number of prescription medications, or any pre-intervention outcome measures (Table 1). Ninety-five percent of the sample were right-handed. There were no adverse effects or events reported during the intervention period. At pre-intervention, 18 participants (46%) reported having a fall within the previous 12 months, eight from FAST and 10 from Standard. Fall history as well as the description of the direction and any injuries sustained for all falls reported can be found in Table 2.
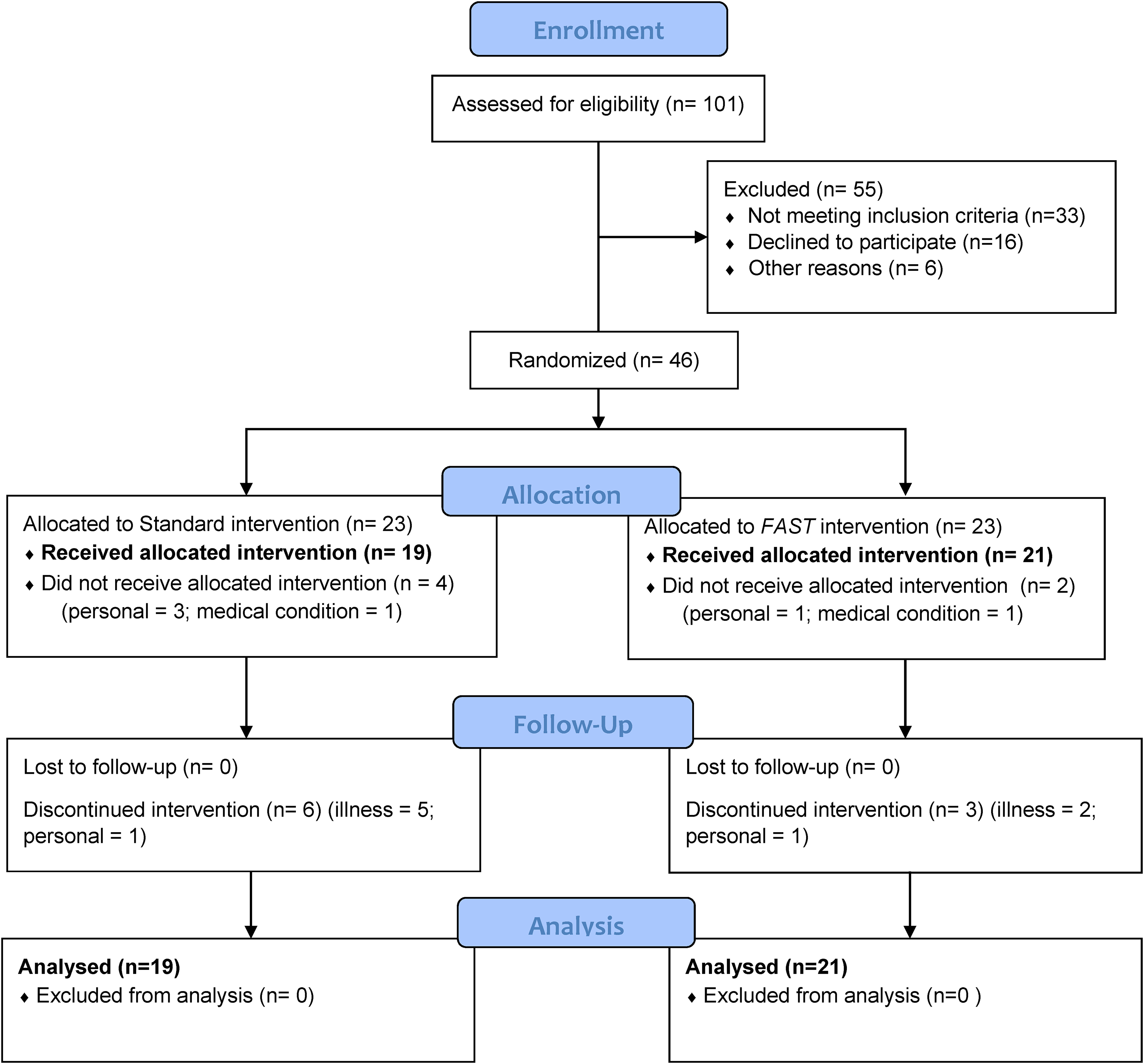
Participant flow diagram.
Demographic, pre-intervention and post-intervention data for FAST (n = 21) and standard (n = 19).
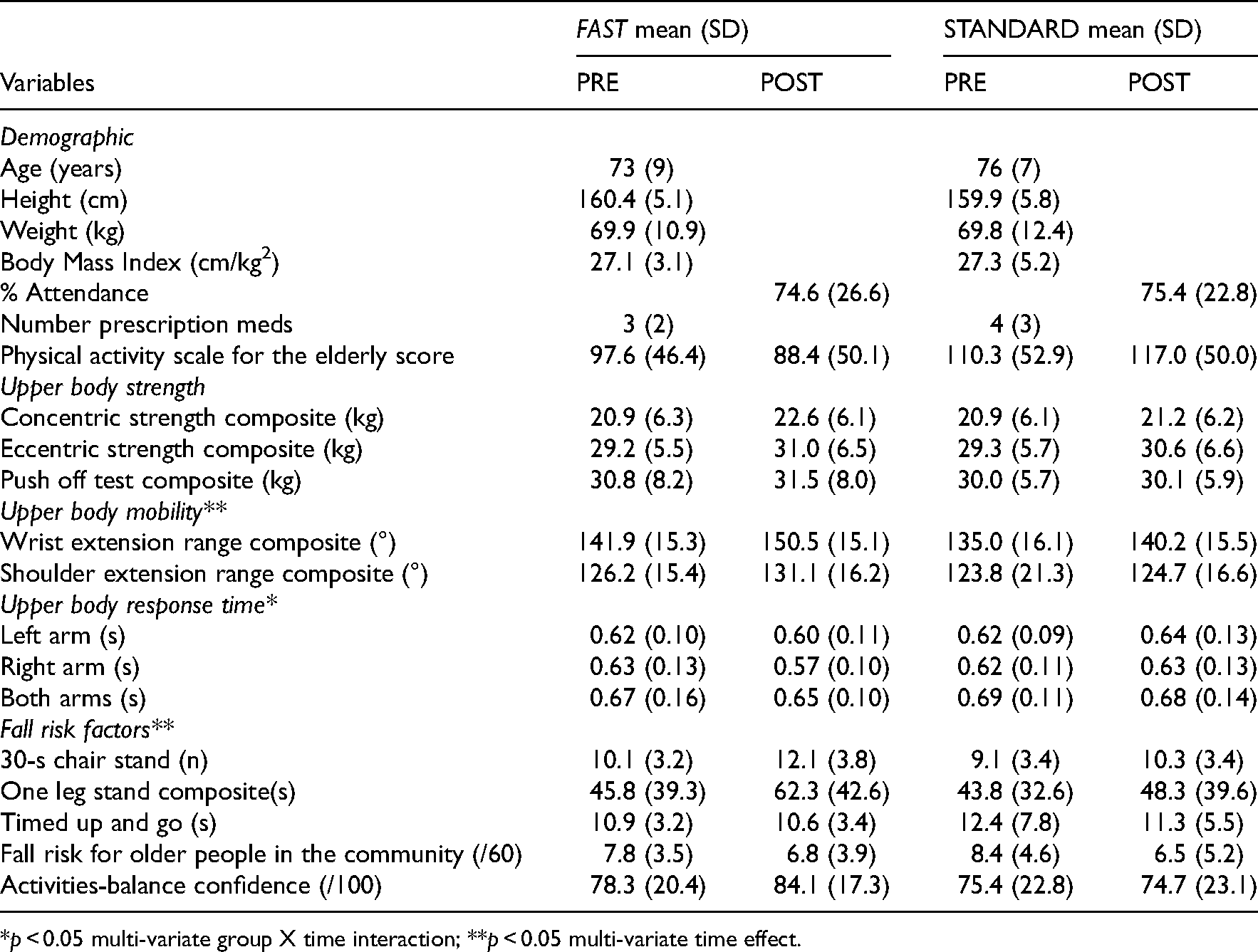
*p < 0.05 multi-variate group X time interaction; **p < 0.05 multi-variate time effect.
Fall history at pre-intervention (in the past 12 months), at post-intervention (in the past three months) and description of falls.
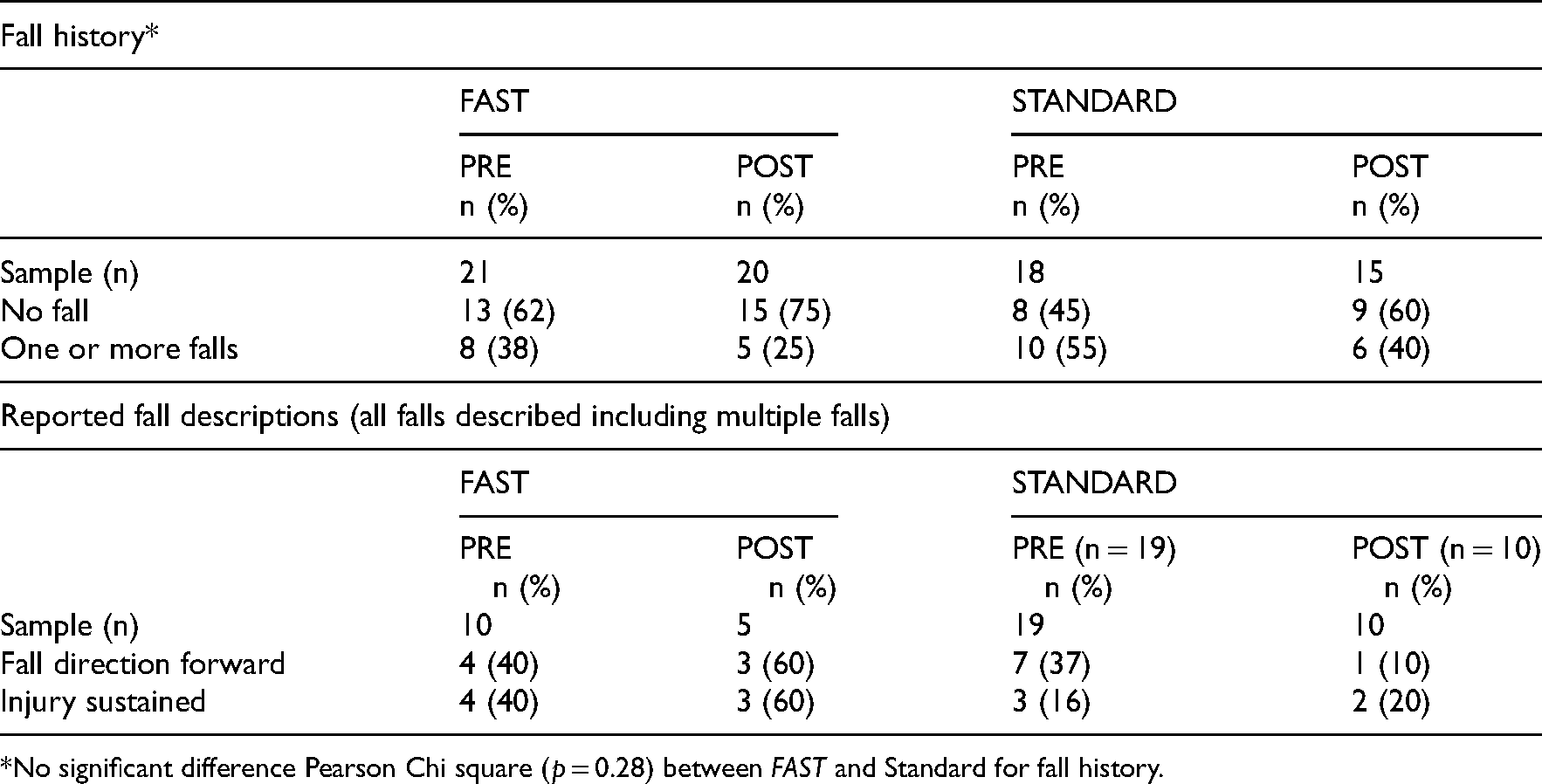
*No significant difference Pearson Chi square (p = 0.28) between FAST and Standard for fall history.
Roy's largest root was used for all multivariate and univariate p-values. For upper extremity strength there was a borderline significant multivariate time effect (F3,36 = 2.87; p = 0.050; partial Eta2 = 0.193) with significant univariate improvement for concentric (F1,38 = 5.41; p = 0.025; partial Eta2 = 0.125) and eccentric (F1,38 = 6.58; p = 0.014; partial Eta2 = 0.148). There was no significant time by group interaction (p = 0.391).
There were significant multivariate time effects for Upper Extremity Mobility (F2,36 = 5.92; p = 0.006; partial Eta2 = 0.248) with significant univariate improvements for wrist extension (F1,37 = 11.56; p = 0.002; partial Eta2 = 0.238). There was no significant multivariate time by group interaction (p = 0.559).
There were no significant multivariate time effects for Upper Extremity Response Time (p = 0.444) but there was a significant time by group interaction (F3,36 = 3.12; p = 0.038; partial Eta2 = 0.206) where only FAST improved upper extremity response time. Univariate time by group interaction analysis revealed a significant right hand response (F1,38 = 5.74; p = 0.022; partial Eta2 = 0.131; refer to Figure 5).
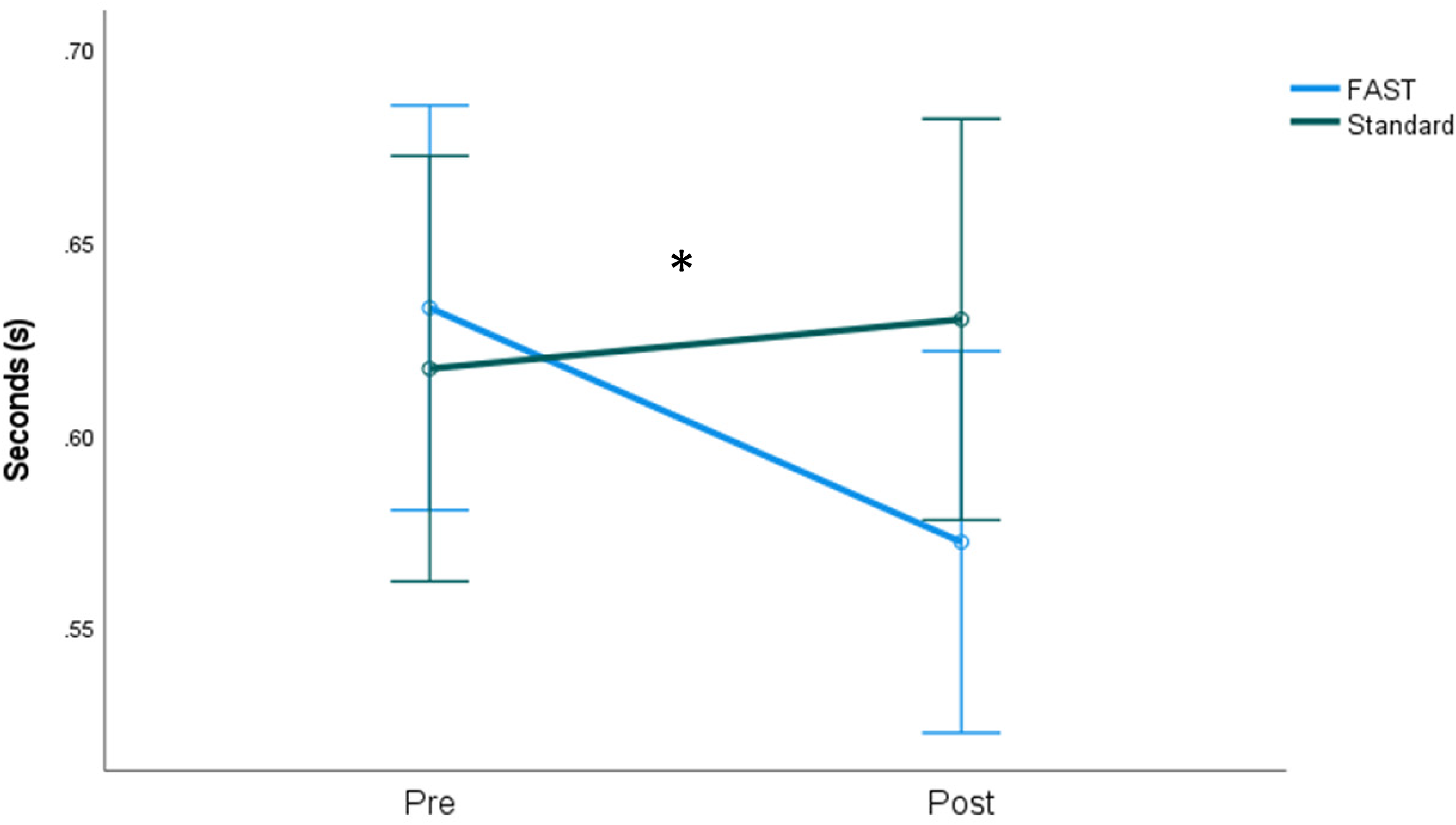
Right upper extremity response time with 95% confidence intervals. * p = 0.022.
There were significant multivariate time effects for fall risk factors (F5,34 = 6.96; p < 0.001; partial Eta2 = 0.506) where significant univariate improvements for the Fall Risk for Older People in the Community questionnaire (F1,38 = 10.52; p = 0.002; partial Eta2 = 0.217), 30-s chair stand (F1,38 = 27.29; p < 0.001; partial Eta2 = 0.418) and one leg stand (F1,38 = 5.73; p = 0.022; partial Eta2 = 0.131). There was no significant time by group multivariate interaction (p = 0.318).
Discussion
The purpose of this study was to determine the effect of 12 weeks of FAST compared to a Standard fall prevention program on upper body strength, mobility and response time, and fall risk factors in older women. The addition of FAST within the same allotted time of 45 min twice per week as Standard resulted in similar significant changes in functional performance known to decrease fall risk factors in older adults. Of importance, the addition of FAST improved upper extremity response time, a finding not observed following the Standard program.
Balance recovery strategies such as taking a step, reaching to grasp an object or reaching the hands to land and protect the head from impacting the ground are all protective postural control reactions developed in the first year of life that persist into adulthood. 26 There is growing evidence supporting perturbation training designed to enhance lower extremity postural reactions in improving fall risk factors and decreasing fall rates in older adults and clinical populations. 9 Little is known about the effect of training upper body reactions that may help to control and diminish the impact of a forward fall and prevent injury risk such as head or other fall-related injuries. There are several age-related differences in upper extremity reactions to a perturbation in older verses younger adults. 27 These include delayed onset of muscle activation and movement time, variation in strategies used (tendency to reach in the direction of the perturbation verses a counterbalancing motion), and greater forces sustained at impact.7,27 Older women, compared to younger women, also tend to land with stiffer arms, utilize less elbow flexion and absorb less energy during simulated forward fall landings and descents.13,14,28 These age-related factors may partially account for differences seen in fall-related injuries. Younger adults are more likely to experience less serious hand and wrist injuries as compared to older adults who are more likely to sustain serious injuries to the head. 29 In fact, video surveillance studies in long-term care facilities have observed a high number of falls where head impact occurred with hand impact, but the majority of observed falls were unsuccessful in utilizing the arms to prevent head impact. 8
The results from both lab and video surveillance data helps to shed light on potential targeted training for older adults. The ability to quickly respond by reaching the hands forward following a perturbation such as a trip may result in being able to place the upper extremity in a position where it is easier to utilize upper body strength to control the descent. 4 One could argue that rolling the body out of the fall might be another successful strategy to reduce upper body injury. However, based on findings where 97% of the time during forward falls older adults in long-term care respond with an UE protective response, 8 it appears that this reaction may be inherent and challenging to suppress, at least for older adults living in long term care. Training that might help to improve the capacity of the upper extremity to react, place hands in a more effective position, with a stronger upper body to control the descent may add benefit to reducing injury risk. It remains unclear what the impact of this type of training has on preventing or reducing risk of serious injury such as head injury or other upper body injuries common to a fall such as a wrist fracture. There is evidence that both the positioning and the timing of the contraction of muscles on impact in the upper limb during a forward fall are important in reducing the risk of wrist fracture. 30
Few studies have evaluated the effect of training on upper extremity reaction or response time. There is some limited evidence that training voluntary stepping with reach and grasping a handrail can result in improved arm movement times; however there are also observations of grasping errors which can delay contact or potentially impact other risks.9,27 A dynamic stretching program improved upper extremity reaction time in younger adults. 31 Visual-motor training improved upper extremity reaction time performance in athletes. 32 Research for older adults has focused primarily on interventions designed to train lower body reaction time through functional activities such as a balance obstacle course. 9
FAST provided practice of responding quickly in targeted volitional practice as well as through functional and fun activities requiring quick responses. Each session incorporated practice of UE reaching and loading activities, typically against a wall or other firm surface. Unexpected audio cues were used for quick reaching activities with one hand or both hands. Progression of wall descent practice included reaching quickly with both hands to the wall and performing a controlled body lowering (reverse push-up). Other activities such as balloon “keep it in the air”, ball toss, and obstacle courses including quick reaching and passing activities incorporated other training tasks designed to increase speed and accuracy of upper body motion. These activities were only in FAST, and therefore could explain the improvements seen in UE response time, as opposed to other aspects of improvement similar in both groups related to balance, upper limb mobility and strength. An interesting finding in this study, is the significant improvement for the right arm response time but not the left. We are uncertain of the reason for this, but ninety-five percent of the participants were right hand dominant. It is possible when training, participants tended to focus on their dominant hand or it was a tendency to use their dominant hand more during activities such as the balloon or ball toss. Future interventions should encourage equal practice using both hands.
Somewhat surprisingly, FAST did not result in significantly greater improvements in upper body strength and mobility compared to Standard. This finding may be explained by several factors. First, even functional practice of tasks to increase lower body strength, balance and general body agility inherently include some component of strength and mobility in the arms. For example, sit to stand practice was a common, similar activity for both groups. If participants could not control the movement with lower leg strength only, use of hands to push off was encouraged. Arm motion during balance practice also incorporates some upper extremity strengthening and stretching components. Second, it was challenging to include the extent of time needed to progress upper body strength training in FAST within the allotted 45 min. Instructor feedback post-program recommended further modification in order to progress the strengthening component. Finally, it was difficult to control for other activities the participants were involved in outside of the program particularly in assisted living sites where recreational activities are encouraged and readily available.
The improvement in fall risk factors for both interventions after 12 weeks was encouraging. Systematic reviews have concluded that at least 6 months of exercise are required to obtain gains to decrease fall risk.1,2 This finding helps to support similar programing, still recognizing the importance of sustaining interventions for longer in order to realize sufficient clinically meaningful changes to improve fall risk factors. The women in this study represented a broad range of abilities and ages, suggesting fall prevention programing can meet the goals to challenge all levels of ability and retain safety for those at greater risk. The sample size was not adequate to explore difference in fall rates; however, it is interesting to observe that falling forward was the most commonly reported fall direction in this study, similar to another study involving community-dwelling older women. 3
One of the limitations of this study was the potential communication that may have occurred between groups as some participants resided in the same assisted living site. Although a randomized site design may have alleviated this cross contamination risk, it presents other difficulties when sites are not equivalent in resources, functional ability of participants or environmental factors. There were also real life challenges with a influenza outbreak, and an environmental factor at one of the sites that resulted in more difficulty in recruitment and retention than our usual experience with this population. 25 A larger sample size may have resulted in significant findings in upper extremity strength. Post-hoc power analysis revealed 44% power for concentric upper extremity strength, with an estimated required sample n = 46 per group for 80% power with beta 0.20, α = 0.05 (https://clincalc.com/Stats/Power.aspx).
In conclusion, practical and feasible exercises designed to improve upper body fall arrest capacity improved fall risk factors, strength and mobility, and upper extremity response time in older women. Further research needs to determine how upper extremity response time alters the way older adults fall and land as well as determining if interventions such as FAST are beneficial in reducing risk of fall-related injuries such as head or other upper body injuries.
Exercises with balance, strength and functional mobility help to improve fall risk factors in older women after 12 weeks Training focused on upper body capacity to improve the protective responses inherent in forward fall landing and descent can increase movement speed which may help reduce forward fall-related injury riskClinical messages
Footnotes
The authors acknowledge the support of the Saskatoon Health Region and the Staying on Your Feet program.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Saskatchewan Health Research Foundation (grant number Collaborative Innovative Development Grant).