
Abstract
Objective:
To explore whether a structured counselling-based intervention increases vigorous physical activity behaviour of adolescent and young adult cancer survivors.
Design:
Randomized controlled phase II trial.
Setting:
University Cancer Center Hamburg, Germany.
Subjects:
Eighty-nine participants (mean age 24.1 ± 6.3) were randomized to control (n = 44) or intervention group (n = 45).
Interventions:
The intervention group was consulted about physical activity behaviour via interview (week 0), and telephone counselling (weeks 1, 3 and 12). The control group only received general physical activity guidelines for cancer survivors (week 0).
Main measures:
The primary outcome was the rate of participants with ⩾9 metabolic equivalent (MET)-hours per week of vigorous activity post-intervention, measured with the International Physical Activity Questionnaire. Secondary outcomes included assessing physical activity behaviour (e.g. amount and type of physical activity) and quality of life. Assessments were completed in weeks 0 (baseline), 12 (post-intervention) and 52 (follow-up).
Results:
Sixty-nine participants completed the post-intervention- and 47 the follow-up-assessment. The rate of participants performing vigorous physical activity increased from baseline to post-intervention for both without differing significantly (P = 0.541). Both increased their total metabolic equivalent from baseline to post-intervention (intervention group from 55.2 ± 43.7 to 61.7 ± 29.4, control group from 75.3 ± 81.4 to 88.3 ± 80.2). At follow-up the intervention group (73.7 ± 80.2) was more active than baseline when compared to the control group (78.5 ± 50.0).
Conclusions:
A structured counselling-based physical activity intervention did not significantly impact the level of vigorous physical activity behaviour in adolescent and young adult cancer survivors.
Keywords
Introduction
Several reviews have confirmed the importance of developing strategies to promote physical activity and health behaviour changes in young cancer survivors.1,2 The positive impact of vigorous physical activity on the risk for cardiovascular events was documented in reports from the Childhood Cancer Survivor Study.3–5 Hodgkin’s lymphoma survivors who regularly underwent vigorous exercise of ⩾9 metabolic equivalent (MET)-hours per week had a significantly lower risk of treatment-related cardiovascular events than survivors who did not meet the physical activity guidelines. 3 METs are defined as the ratio between the metabolic rate when performing physical activity and the metabolic rate of an individual at rest. Examples of moderate exercise (defined as 3–6 METs) include brisk walking, and weight training with light weights, whereas vigorous exercise (>6 METs) includes circuit training or running at speeds greater than 7 miles per hour. 6
As the curative rates in young cancer patients has increased in recent years, due to the development of improved treatment strategies (including multimodal therapy), so has the focus on how to best support the survivors. The National Cancer Institute defines the age range of adolescent and young adults (AYA) with cancer from 15 to 39 years. When taking into account the aggressive multimodal treatment applied to achieve these increased cure rates, this patient group is particularly vulnerable to short- and long-term health issues. 7 Major cardiovascular events and the development of malignant neoplasms are the most common late toxicities in childhood cancer survivors.8,9
To reduce the risk of a cardiovascular event, adolescents and young adults should adopt a healthy lifestyle with regular physical activity, because historically they are insufficiently active in comparison to controls.10–12
There is a lack of studies aimed at improving physical and psychosocial functioning within this population. 13 Thus, the aim of the Motivate AYA (MAYA) phase II trial was to show the effect of a counselling-based intervention with the focus on improving the vigorous physical activity behaviour of adolescent and young adult cancer survivors.
Methods
A single centre randomized controlled phase II trial with two arms was conducted, with recruitment spanning 2016 and 2017, with the last follow-up taking place in December 2018. The trial was registered at the German Clinical Trial Register (DRKS-ID: DRKS00009453) and did not receive any funding. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (Hamburg Medical Chamber, reference number PV4948) and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. All participants submitted written informed consent before study entry.
Participants were screened for eligibility in the survivorship clinic at the University Cancer Center Hamburg, within the University Medical Center Hamburg-Eppendorf. All patients had completed curative intent cancer treatment and were in follow-up care within the multidisciplinary survivorship clinic.
Inclusion criteria were: adolescent and young adult cancer survivors aged 15 to 39 years, with at least one treatment related (e.g. anthracycline based chemotherapy, chest radiation or cyclophosphamide and chest radiation), or non-treatment related risk factor (nicotine abuse, diabetes mellitus, dyslipoproteinemia or hypertension) for cardiovascular diseases.
Exclusion criteria included: ongoing cancer therapy, pre-existing severe cardiovascular disease or any contraindication for vigorous physical activity.
Patients who met the inclusion criteria and agreed to participate in the study were randomly assigned to one of two groups: the intervention group or the control group. An uninvolved third-party researcher, who had no stake in the outcome of this study, was responsible for the allocation. Participants were designated to either group based on the random drawing of a slip of paper from a sealed opaque envelope (a one indicating the control group and a two indicating the intervention). The participants were then told into which group they were allocated.
At baseline assessment (week 0), post-intervention (week 12) and follow-up (week 52), all participants completed the questionnaire assessment.
The primary outcome was the rate of participants partaking in vigorous physical activity, defined as ⩾9 MET-hours per week of vigorous activity, as measured with the short version of the International Physical Activity Questionnaire (IPAQ). 14 This questionnaire records the intensity and time spent on each physical activity within the last 7 days. These values are then entered into a scoring protocol, to produce either a category (i.e. low, moderate, vigorous) or a continuous variable (i.e. MET minutes per week). According to the scoring protocol, metabolic equivalent scores were calculated using the following values: walking (3.3 METs), moderate intensity (4.0 METs) and vigorous intensity (8.0 METs). The time variables for walking, moderate and vigorous activity exceeding ‘3 hours’ have been truncated to be equal to ‘3 hours’.
Secondary outcomes were the amount and intensity of the participants’ physical activity behaviour, also measured with the International Physical Activity Questionnaire; as well as quantifying the interest in, and need for, a clinical exercise programme, and overall quality of life.
To find out about the patients interest of participating in a clinical exercise programme we asked about the preferred physical activities: ‘Which exercise activities would you like to practise?’ When a participant indicated that they had no desire to participate in a given activity, they were then prompted to give their reasoning from a list of pre-determined excuses, such as: too large a distance, too large time effort for additional activities, feeling too weak for physical activities, never liking physical activity or other reasons. The rationale behind this line of questioning was included in order to inform future clinical practice decisions, and to best tailor future exercise programs to survivors.
The quality of life was assessed by the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30). 15 Additionally, demographic data (sex, age, body mass index), medical history (age at diagnosis, cancer diagnosis, medical treatment, time between end of therapy and study inclusion) were collected at baseline.
Consenting participants of the intervention group received individual physical activity counselling by a sports scientist, based on an adaption of the Transtheoretical Model, which we described extensively in Table 1.16,17 The Transtheoretical Model was first developed to facilitate behavioural change within the context of cigarette smoking and has since been transferred and modified for further health behaviours and is an appropriate method to increase physical activity.16,18 University-aged students post Transtheoretical Model-intervention targeted on increasing physical activity levels improved their exercise stage of change more so than controls. 19 Thus, the Transtheoretical Model can be deemed a feasible and applicable intervention in adolescent and young adults. It includes five stages of change: precontemplation, contemplation, preparation, action and maintenance (Table 1). 17
Description of the counselling intervention based on the Transtheoretical Model.
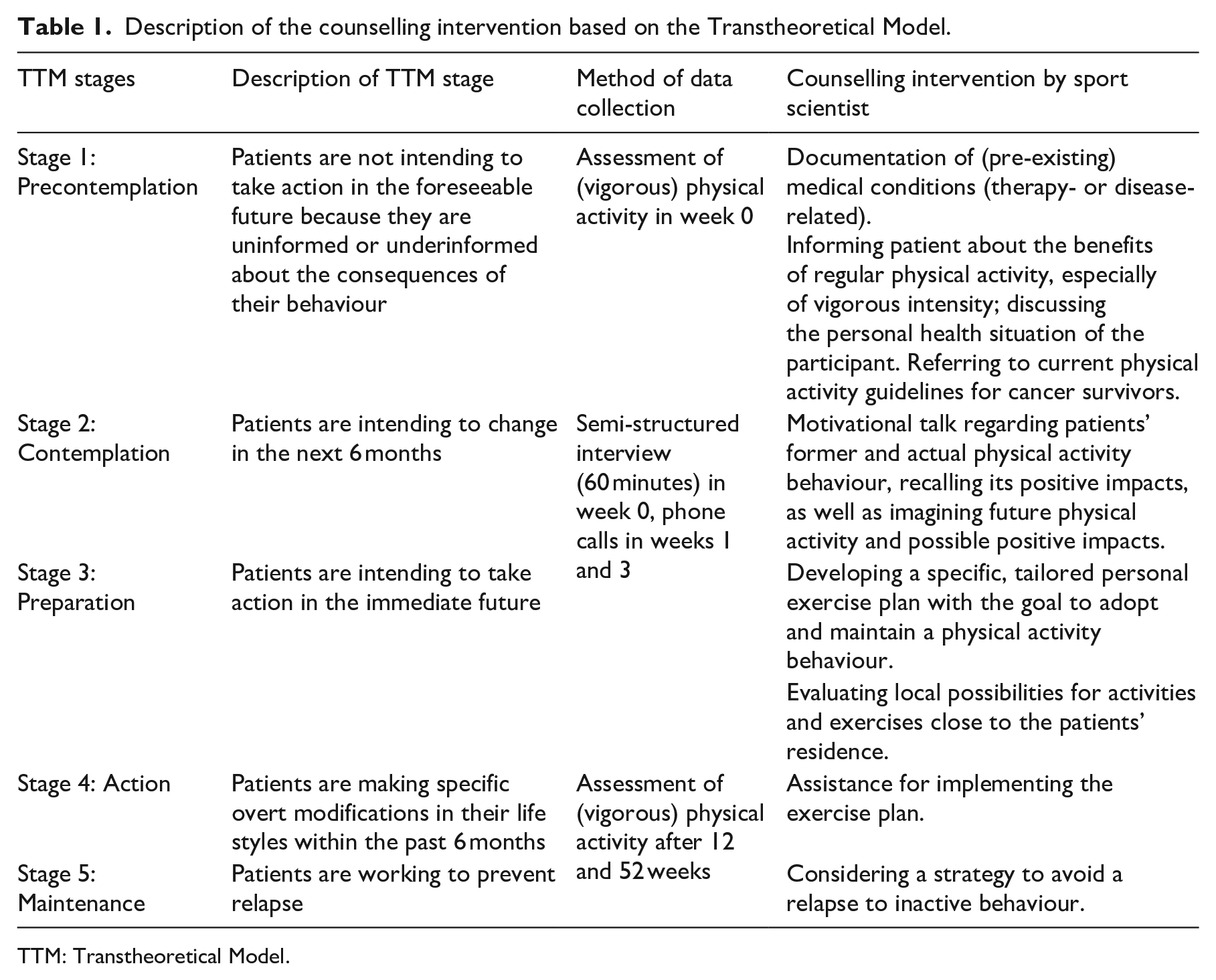
TTM: Transtheoretical Model.
The semi-structured interview had a duration of 60 minutes and included the documentation of physiological limitations for physical activity (therapy- or disease-related, or in general) and physical activity behaviour before and after cancer treatment. Thus, the individual needs of the participant were assessed and a personalized plan with the goals of adopting and maintaining physically active behaviour was developed. In addition, the sports scientist evaluated local possibilities for physical activity and exercises, including oncological training- and exercise therapy to address therapy-induced side effects, and handed out the current guidelines for cancer survivors. After 1 and 3 weeks, the sports scientist consulted the participants again by telephone to clarify questions, ask for the status of implementing the physical activity plan and to offer further assistance. The intervention ended in week 12 with a final consultation, which also was delivered via telephone.
Patients of the usual-care control group received a handout with the physical activity guidelines for cancer survivors 20 at baseline by the physician during the medical survivorship care consultation.
Participants completed the aforementioned assessment questionnaires in weeks 0, 12 and 52, regardless of their allocation (i.e. intervention or control group). Questionnaires were given to all participants in person for the baseline data collection (week 0) and via post for the remainder for the trial.
Statistical analysis
The rate of participants with ⩾9 MET-hours per week 3 months after general physical activity recommendations was expected to be 25%, based on previous experience within survivorship care. In order to be considered to be effective, the intervention should double this rate to 50%. With a one-sided alpha of 10%, 46 participants were need to detect this difference with a targeted power of 85%. To account for an expected dropout of 10%, at least 50 patients were enrolled in each arm. A per-protocol analysis was chosen in order to best test the effect of counselling on physical activity behaviour in optimal conditions, and to eliminate any bias that could have arisen had the dropouts been included in the final analysis.
A logistic regression model was used to analyse the longitudinal primary outcome (Table 3) and a linear regression model was used to analyse the secondary outcomes (Table 4). The model estimated marginal frequencies, and the corresponding 95% confidence intervals were computed and compared pairwise both, for the time point and the two groups, where the group comparison of the rate of participants with ⩾9 MET-hours per week of vigorous activity after 12 weeks comprises the primary outcome.
Results
Among the 115 potentially eligible survivors, 89 agreed to participate and underwent randomization (Figure 1). Table 2 shows the baseline patient characteristic of the total cohort and the evaluable cohort; 69 (36 in the intervention group and 33 in the control) participants completed the post-intervention assessment and 47 (30 intervention and 24 control) the follow-up assessment. The 3-month attrition rate was 22.5%. There were no statistical differences in the baseline demographic variables between the groups.
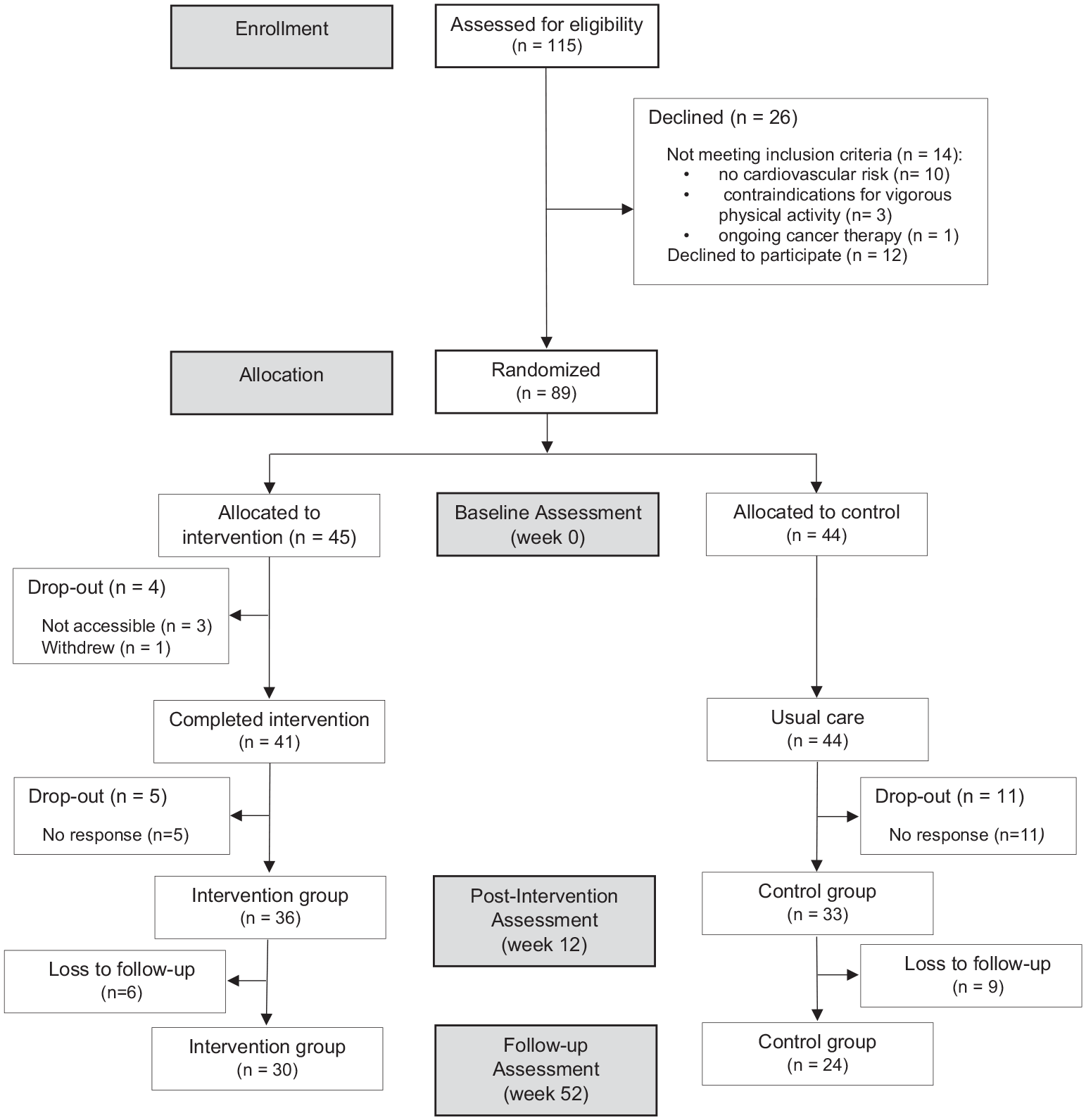
CONSORT flow diagram.
Patient characteristic of the total cohort (n = 89) and evaluable cohort (n = 69).
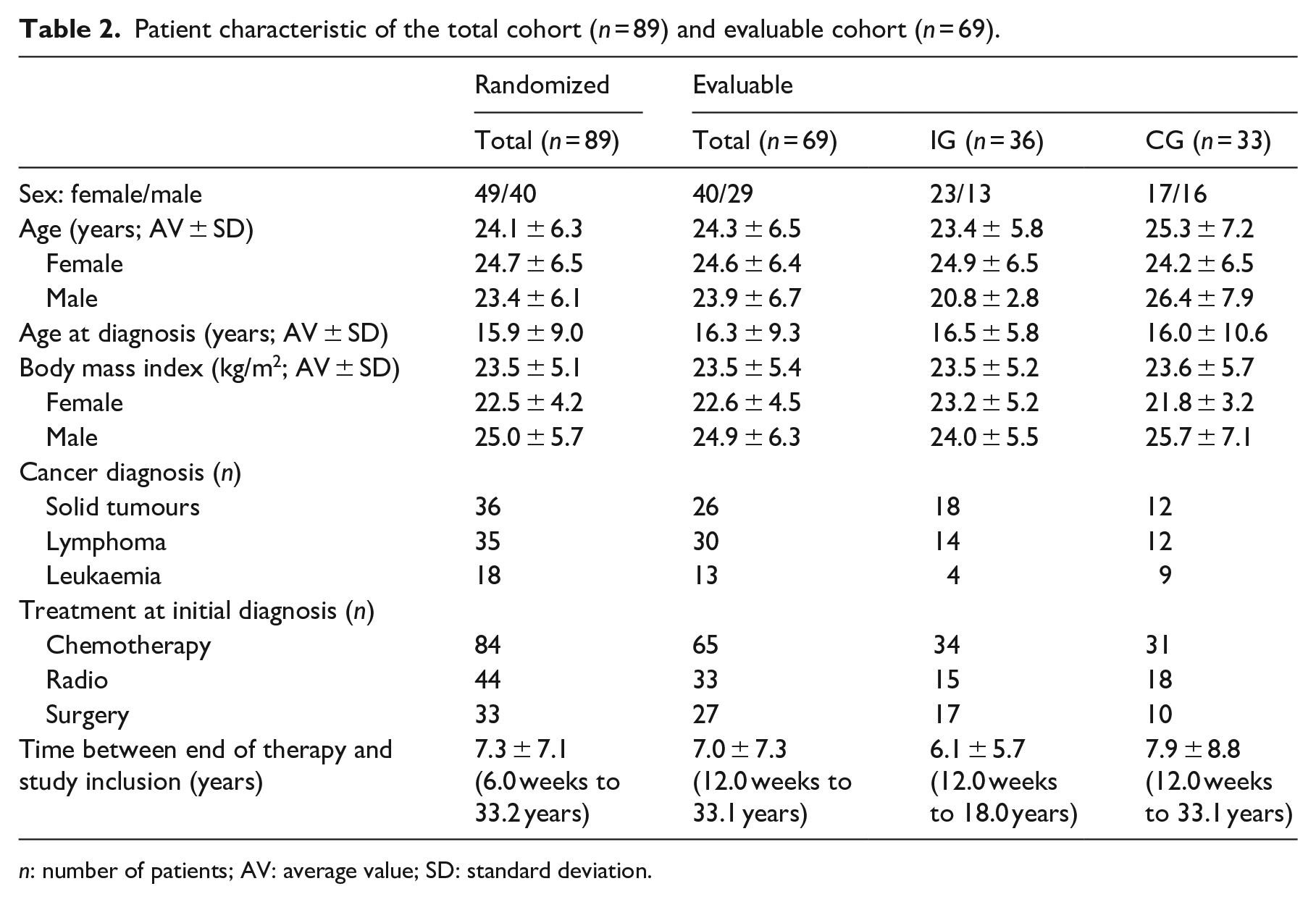
n: number of patients; AV: average value; SD: standard deviation.
Despite the evenly balanced baseline factors, the control group (with a MET score total of 75.3 ± 81.4) was generally more active than the intervention group with a total score of 55.2 ± 43.7 METs, though, the difference was not significant (P = 0.261).
The vigorous physical activity level for the primary outcome could be assessed for 61 participants post-intervention and for 47 at follow-up (Table 3). The rate of participants recording vigorous physical activity behaviour of ⩾9 MET-hours per week did not differ significantly between the groups (P = 0.541). The intervention could not double the rate.
Rate of participants with ⩾9 MET-hours/week of vigorous activity (primary outcome, intergroup comparison).
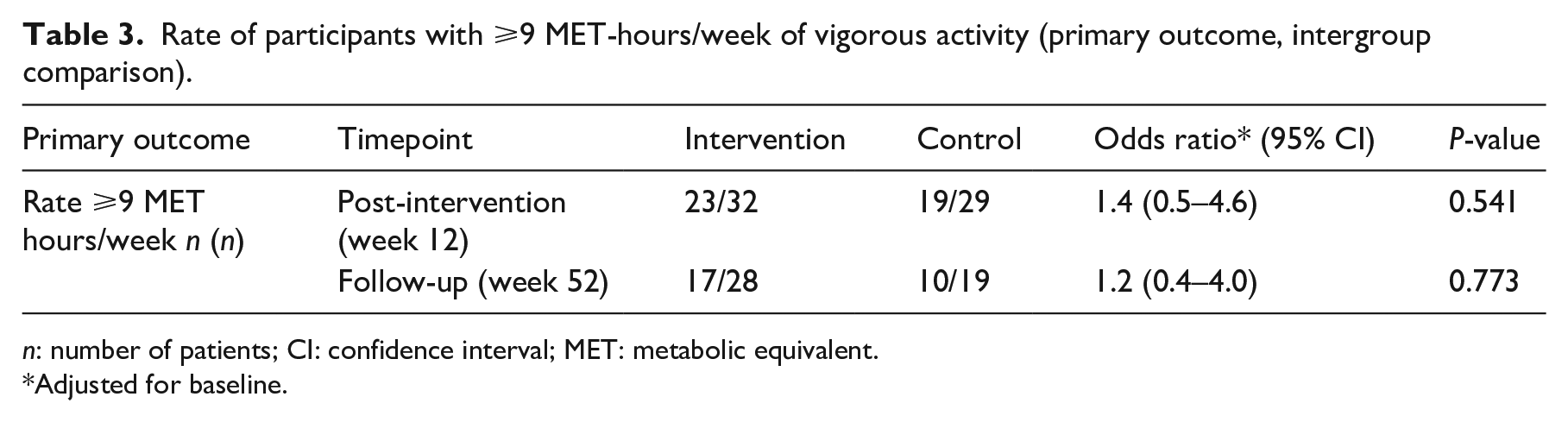
n: number of patients; CI: confidence interval; MET: metabolic equivalent.
Adjusted for baseline.
However, following changes regarding the physical activity behaviour could be seen within the analysis of the secondary outcomes (Table 4):
Course of physical activity behaviour assessed by the IPAQ (intergroup comparison).
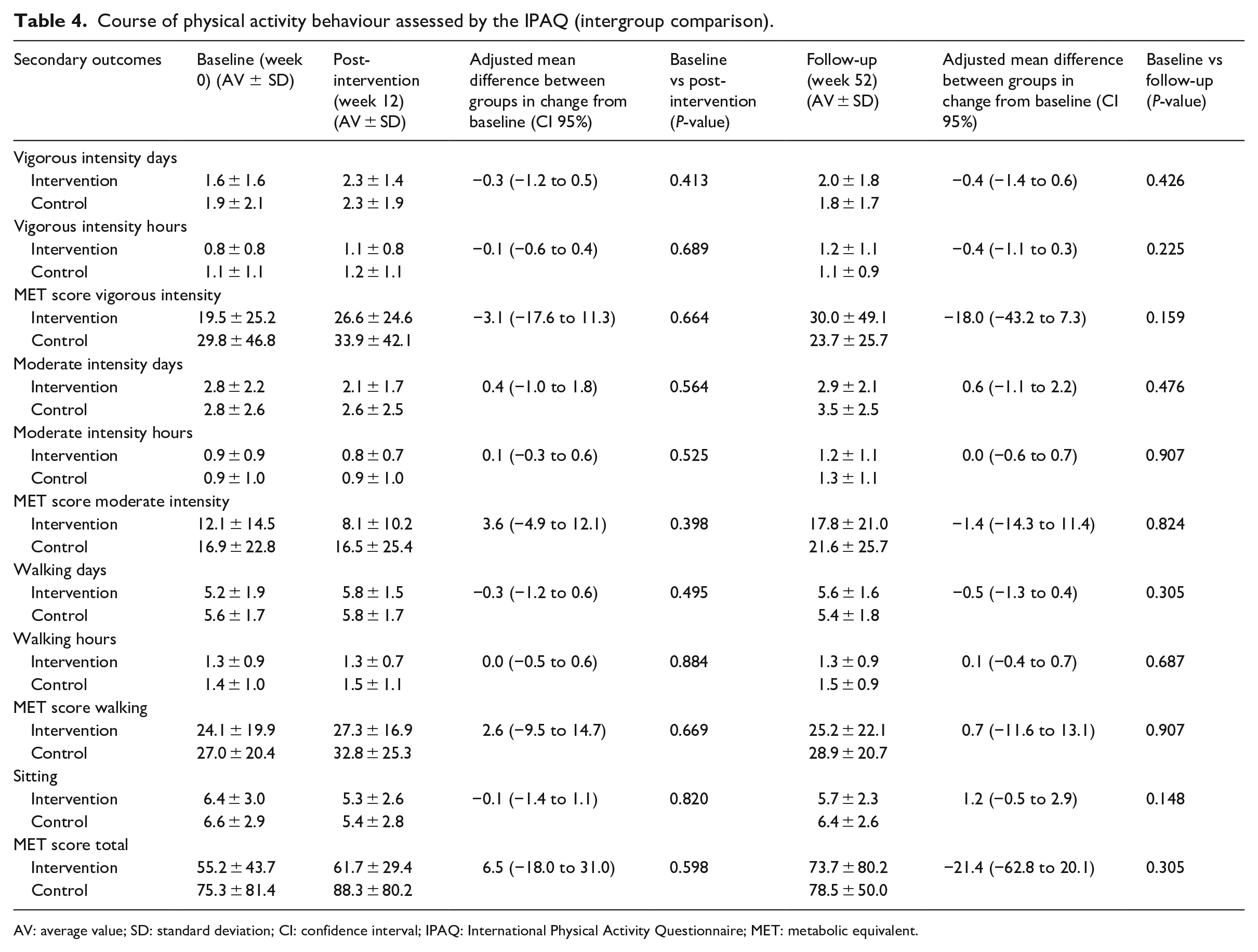
AV: average value; SD: standard deviation; CI: confidence interval; IPAQ: International Physical Activity Questionnaire; MET: metabolic equivalent.
- From baseline to post-intervention both groups increased all parameters of vigorous physical activity (days, hours, MET score). While these parameters at follow-up declined in the control group, a further increase only was noted in the intervention group (days P = 0.426, hours P = 0.225, MET score P = 0.159).
- The intervention group and the control group decreased their moderate intensity activity behaviour from baseline to post-intervention and increased it at follow-up over the baseline value, though the increase was not significant.
- Both groups reduced the time spent sitting from baseline to post-intervention. Whereas the time spent sitting in the control group returned to baseline values at follow-up, the intervention group continued to spend less time sitting (P = 0.148).
Regarding the quality of life questionnaire, improvements were observed for social functioning in both groups, but these were not significant within the intergroup comparison.
Preferred activities of the 69 participants were resistance training (n = 37), swimming (n = 36), yoga (n = 34), cycling (n = 31), running (n = 23), ball games (n = 22), gymnastics (n = 15), walking (n = 11) and other (n = 7).
Reasons for no interest in participating in a physical activity program at the University Medical Center Hamburg-Eppendorf were the distance (n = 29), a lack of time (n = 10), never liking physical activity (n = 5), feeling too weak (n = 3) and other (n = 10).
Discussion
The aim of the MAYA trial was to assess whether physical activity counselling increases the vigorous activity behaviour of adolescent and young adult cancer survivors. The present study is the first randomized intervention trial concentrating on the threshold of ⩾ 9 MET-hours per week of vigorous activity. There was no significant difference within the intergroup comparison from baseline to post-intervention. Also, the intervention could not double the rate of participants with ⩾9 MET-hours per week.
However, by analysing the course of the physical activity behaviour, the study could show a slight sustained impact favouring the intervention group; at follow-up the intervention group had higher values of vigorous activity, a decrease of the time spent sitting, and finally, an increase of the total MET score, despite these between-group differences not achieving statistical significance. The intervention group also exhibited a decrease in moderate levels of physical activity at the 12-week post-intervention assessment. Perhaps this decrease is directly related to the increase in vigorous level physical activity, meaning that they occur concomitantly.
Currently, few randomized trials with small sample sizes and varying methods have examined the physical activity of adolescent and young adult cancer survivors. These trials reported improved cardiac function, 21 increased moderate to vigorous physical activity and maximum oxygen uptake 22 or a significant decrease in fatigue and increase in daily physical activity. 23 Online interventions have been determined to have high feasibility and acceptability among adolescent and young adult cancer survivors, despite there being no significant change in physical activity levels.24,25 A Facebook-based physical activity intervention increased moderate to vigorous activity and led to significant weight loss. 26 Supervised interventions containing a physical activity educational and/or exercise intervention in a group setting led to improved physical activity, quality of life and also cardiovascular, physical and metabolic outcomes of cardiovascular diseases.27,28 To conclude, interventions focusing on physical activity of young cancer survivors are practical, feasible and generally well accepted. The MAYA trial confirms these experiences, while also independently showing that physical activity counselling within survivorship care is feasible. This is due to the lack of adverse events, in combination with the relatively low number of dropouts (3-month attrition rate of 22.5%) leads to the conclusion that the organization and methods of the MAYA trial are feasible. Between the eligibility assessment and the allocation of participants, 26 individuals were excluded from participating in the trial. Slightly more than half of these individuals did not meet inclusion criteria, with slightly less than half declining to participate. Those who declined to participate were not inquired as to the reasoning behind their decision.
Nevertheless, in our findings the intergroup results were not significant, potentially due to a variety of reasons: first of all, the rate of participants recording vigorous physical activity behaviour at baseline was far higher than anticipated and the control group was more active than the intervention group. Because of that, and a lack of further funds the trial was terminated early after including 89 participants, which may have impacted the findings and the interpretation of the results. In order to show relevant differences, the sample size of the evaluable cohort would need to be larger. In addition to that, the future use of the Transtheoretical Model needs to be reconsidered to be more effective. The Transtheoretical Model has come under scrutiny because its stages are not mutually exclusive and there is little evidence of sequential movement through discrete stages in studies. 29 While it presents an easy to understand framework, its practical value has been questioned due to the inability to assess the stages due this lack of sequential movement. 29 Despite these criticisms, the Transtheoretical Model-based counselling proved to be a feasible method in this case. However, a longer duration of the trial and including all stages of change, may would have allowed for stronger causal inferences.
Also, the use of the International Physical Activity Questionnaire presents some challenges, as it has a tendency to overreport physical activity levels. Studies with young cancer survivors examining physical activity levels with the International Physical Activity Questionnaire are lacking. Though, a study with cancer survivors aged 18–79 found that this questionnaire significantly overestimated physical activity levels across all intensities and underestimated physical inactivity level when compared with an accelerometer, 30 which is why applying a physical activity questionnaire without objective physical activity measurements (e.g. accelerometers) should be discouraged. The initially planned goal of the MAYA intervention to double the rate of participants with ⩾9 MET-hours per week to 50% in order to be considered effective was proven to be too optimistic. The rate at baseline already was 50% (not 25% as expected). Perhaps this was due to the aforementioned tendency of the International Physical Activity Questionnaire to overreport physical activity levels.
However, there are some limitations present in this study. The monocentric conduction of the trial affects the transferability of the data. Thus, a very physical active control group and small sample size limit the results and lead to a limited statement in this study. The inherent inability that is usually present among exercise-focused studies to blind the participants to their group allocation impacts the generalisability of (and thus limits) the results. This could be due to the potential impact of social desirability bias, that is that the behaviour of the intervention group could have been biased simply by the knowledge of their allocation.
Based on our findings we can recommend the following for future studies within this population:
- Counselling interventions should focus on the barriers and motivational factors affecting physical activity in adolescent and young cancer survivors.
- Initial screening for physical activity levels and preferences could make the physical activity counselling within the follow-up care more need-adapted and efficient.
- Considering the young age of the target group, social media and online interventions should be considered, in conjunction with home-based programs and motivational activity tracker to promote physical activity engagement.31,32
- Further interventions should have larger cohorts.
Considering the data, it is recommended to integrate structured physical activity counselling as a permanent component within the context of acute cancer centres and cancer rehabilitation centres and the survivorship care of cancer survivors.
Based on these findings in the MAYA trial and experiences within the survivorship clinic, a new program for adolescent and young adult cancer survivors, the CARE for CAYA-Program, was developed. 33 This multicentre trial includes a need-stratification within modular interventions including physical activity, nutrition and psycho-oncology, with the focus on improving the lifestyle and psychosocial situation of the participants.
Clinical messages
Individualised physical activity counselling could be a valid tool to improve physical activity behaviour of adolescent and young adult cancer survivors.
The need to integrate counselling into basic survivorship care in rehabilitation centres exists.
Footnotes
Acknowledgements
We want to thank all patients who participated in this study, all participating clinicians who included patients, and all the staff engaged in this study. Especially, we thank Carrie-Ann Minto for improving the use of English in the manuscript.
Author contributions
All authors contributed to the study conception and design. J.S., B.K., J.M. and W.J. performed data collection. J.S., B.K., J.M., S.D., E.V., F.B., A.S. and W.J. performed the analysis and interpretation of data. J.S. wrote the first draft of the manuscript. J.S., B.K., J.M., J.G., S.E., S.D., G.E., E.V., R.R., M.S., F.B., C.B., A.S. and W.J. critically revised the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.