
Abstract
Objective:
The aim of the study was to investigate whether liuzijue qigong could improve the ability of respiratory control and comprehensive speech in patients with stroke dysarthria.
Design:
A randomized controlled trial.
Setting:
The research was carried out in the department of rehabilitation.
Participants:
Altogether, a total of 98 stroke patients with dysarthria participated in the study.
Interventions:
Patients were randomly divided into two groups (the experimental group: basic articulation + liuzijue qigong, 48 patients or the control group: basic articulation + traditional breathing training, 50 patients). All therapies were conducted once a day, five times a week for three weeks.
Main measures:
Primary outcome measure: Speech breathing level of the modified Frenchay Dysarthria Assessment. Secondary outcome measures: the modified Frenchay Dysarthria Assessment, maximum phonation time, maximal counting ability, /s/, /z/, s/z ratio, and the loudness level. All outcome measures were assessed twice (at baseline and after three weeks).
Results:
At three weeks, There were significant difference between the two groups in the change of speech breathing level (81% vs 66%, P = 0.011), the modified Frenchay Dysarthria Assessment (5.54 (4.68–6.40) vs 3.66 (2.92–4.40), P = 0.001), maximum phonation time (5.55 (4.92–6.18) vs 3.01(2.31–3.71), P < 0.01), maximal counting ability (3.08(2.45–3.71) vs 2.10 (1.53–2.67), P = 0.018), and /s/ (3.08 (2.39–3.78) vs 1.87 (1.23–2.51), P = 0.004), while no significant differences were found in the change of /z/ (3.08 (2.31–3.86) vs 2.10 (1.5–2.64), P = 0.08), s/z ratio (1.26 (0.96–1.55) vs 1.03 (0.97–1.09), P = 0.714), and the change of loudness level (69% vs 60%, P = 0.562).
Conclusions:
Liuzijue qigong, combined with basic articulation training, could improve the respiratory control ability, as well as the comprehensive speech ability of stroke patients with dysarthria.
Trial registration:
ChiCTR-INR-16010215.
Introduction
Stroke often causes neuromuscular injury that results in dysarthria of varying severity. 1 Changes in respiration, vocalization, resonance, and articulators may also be involved in dysarthria in stroke victims. 2 Respiration is the energy source of speech 3 and Fugl-Meyer and Grimby 4 has suggested that insufficient respiratory capacity is one of the common characteristics of stroke patients. Respiratory impairment during speaking has been characterized by inadequate respiratory support and impaired respiratory / phonatory coordination, which has a great impact on speech production. 3 The clinical manifestations include improper loudness (e.g. too low a loudness level or irregular excessive loudness variability), abnormal breathing patterns (e.g. chest breathing, rapid and shallow breathing during speech, the patient speaks a word and then pauses), and low vocal quality (e.g. unstable phonatory, tremor or a strained-strangled-harsh voice).3,5,6 Inadequate respiratory support is mainly caused by significantly decreased vital capacity, and an inability to generate enough subglottic air pressure.3,7 Inappropriate or inconsistent lung volume levels are the main factors leading to impaired respiratory and vocal coordination. 6
Patients with inadequate respiratory support may benefit from treatments that directly targeting the respiratory subsystem. 8 Therapy aimed at strengthening the breathing muscles, such as blowing balloons, bubbles, and feathers, 9 are most commonly employed, as well as pushing and pulling training, breath resistance through pursed lips and other techniques.3,10 There are many other ways to improve breathing and vocal coordination for speech, such as inhaling quickly and exhaling slowly, inhaling through the nose, and exhaling through the mouth. 11 However, studies have proven that only training the breathing muscles may fail to maintain stable vital capacity, inspiratory pressure, and expiratory pressure during speech, which were less responsive to achieve stability of airflow and made the patient feel fatigued with increased hoarseness. 12 Furthermore, due to natural coupling of the systems of respiration and the vocal cords, combination treatments for both have been shown to be more effective than single breathing exercises. 13 As a high-effort, intensive phonatory-respiratory therapy, Lee Silverman Voice Treatment was aimed at improving respiratory drive, vocal fold adduction, and more generally respiratory and phonatory synergy activities to increase speech intelligibility. 14 In addition, among respiratory training therapies, upper limb movement is considered to be important and has been shown to be effective in increasing respiratory muscle strength and forced expiratory volume. 15 Therefore, if a combination of breathing, phonation and upper limb movement training is established, it may have a better therapeutic effect for patients with stroke-related dysarthria.
Liuzijue qigong, a traditional Chinese fitness exercise compiled by the China Qigong Management Center, 16 is derived from traditional Chinese medicine, and involves breathing exercises along with mantras of six speech sounds (Xu, He, Hu, Si, Chui, and Xi). Specifically, people inhale through their noses and then exhale through six different tongue and mouth shapes, as well as following proper upper limb movements to control breathing from the top down and vice versa. 17 In recent years, liuzijue qigong has been applied to individuals with chronic obstructive pulmonary diseases (COPD),18–20 and it has been confirmed to be effective in improving their pulmonary function, exercise capacity, and quality of life. Considering that liuzijue qigong is a method of guidance combining respiration and phonatory, supplemented by upper limbs movements, these exercises were performed on patients with dysarthria due to stroke.
The main aim of the study was to investigate whether liuzijue qigong could improve respiratory control ability and comprehensive speech ability in individuals with dysarthria after stroke.
Methods
A single-center, evaluator-blind, randomized controlled trial was conducted and approved by the the Ethics Committee of Shanghai Xuhui District Central Hospital (Ethical code. 2016-31). Shanghai Xuhui Central Hospital was responsible for the conduct and integrity of the study. Registration was completed on the Chinese Clinical Trial Registration Platform (identifier: ChiCTR-INR-16010215), following the Consolidated Standards of Reporting Trials (CONSORT) guidelines.
From June 2016 to June 2018, participants aged 40–80 in the Rehabilitation Department, Shanghai Xuhui Central Hospital, were recruited into the study. The recruitment process consisted of the following four steps: (1) Physicians familiar with the inclusion criteria screened potential patients, then contacted the primary researcher. (2) The primary researcher explained the study to the participants, as well as the rights and obligations of the subjects, and then asked them for their opinions. (3) The qualifications of the participants were evaluated. (4) An informed consent form was signed in person by the participants and their relatives.
Inclusion criteria were as follows: (1) diagnosed with cerebral infarction or hemorrhage; (2) met the diagnostic criteria for stroke in Chinese medicine; (3) first stroke followed by dysarthria; (4) a score of <27 on the modified Frenchay Dysarthria Assessment 21 and with speech breathing level of the modified Frenchay Dysarthria Assessment ⩾ b of post-stroke dysarthria; (5) onset two weeks to six months earlier; (6) could tolerate 40 minutes of speech training; (7) normal or Brunnstrom level ⩾ IV motor function in at least one upper limb; (8) sitting balance level ⩾ 3; (9) stable vital signs; volunteer participation.
Exclusion criteria included: (1) with unconsciousness or severe cognitive disability; (2) combined aphasia; (3) inability to complete 40 minutes of speech training; (4) acute diseases of the heart, brain, kidney, or other major organs; (5) serious mental disorder.
Eligible patients were randomly divided to the liuzijue qigong group (liuzijue qigong + basic articulation training) or the traditional breathing group (traditional breathing training + basic articulation training) in a 1:1 ratio. Randomization sequence was generated by Excel and the grouping information (serial number, group, selected treatment, etc.) were packed in opaque sealed envelopes, which were opened by the research staff and assigned to the enrolled patients in order. The envelope was prepared by an individual who was not related to the clinical part of the study. The primary researcher was responsible for managing the table and the assignment of all patients in the study. One group of therapists performed the intervention, while another group of professionals evaluated the results. The exchange of information between these two groups were not permitted during the experiment, nor were they allowed to collect information from the subjects involved.
All subjects received basic articulation training, including articulation organ training and pronunciation training. Articulation organ training was to facilitate the opening of the throat and relaxation of the muscles involved in vocalization. For example, patients were required to vocalize /en/ and /u/ repeatedly and as rapidly as possible, in order to improve the flexibility of the lips, tongues, and jaws. In the pronunciation training stage, patients began the training with basic stimuli like single vowels and progressed to diphthongs, syllables, sentences, and connected speech, as they met the standard requirements at every level. Basic articulation training was followed by liuzijue qigong or traditional breathing training (20 minutes for each), and all therapies were conducted five times a week, for three weeks, in a speech training room, whose background noise was ⩽30 dBA. Patients were trained by experienced therapists, who ensured that the training process complied with the predetermined protocol.
Liuzijue qigong group
Therapists were trained on liuzijue qigong for six months by a senior fitness expert from the WuShu College of Shanghai Sport University. The program was based on the manual of Liuzijue (General Administration of Sports of China) 17 and the book of Health Qigong and Stroke Rehabilitation. 22
Liuzijue qigong involved inhaling through the nose and exhaling through the mouth while producing six different sounds (Xu, He, Hu, Si, Chui, and Xi), supplemented by corresponding movement guidance.
At the beginning of the treatment, therapists taught patients how to pronounce the six words, correcting the mouth shape, and adjusting the position of the lips and tongue if necessary.
The symmetrical range of motion of both upper limbs was maintained after different levels of assistance were provided by the therapist.
Patients were instructed to gradually change from natural abdominal breathing patterns to anti-abdominal breathing patterns.
Patients were guided by a therapist to breathe in a relaxed, slow, and gentle manner, gradually extending the length of the exhalation to be as long as possible.
A suitable posture was adopted by each patient (standing position, sitting position) according to their balance ability.
Assistive devices (e.g. elastic band, Bobath ball, or long wooden stick) were used if necessary to assist the completion of movements.
Control group
Patients assigned to the control group were told to keep their torso straight, shoulders level, and head centered.
The patients were encouraged to use abdominal breathing. The therapists put their hands on both sides of the patients’ costal arches to help them inhale smoothly through their nose and exhale slowly through the mouth.
The patients were asked to stretch both arms and move them up and down slowly, while the therapist assisted in expanding the chest during inhalation and compressing the chest during exhalation.
Patients had to do several sets of movements to increase lung capacity, such as blowing feathers, candles, and so on.
Patients were told to pronounce the vowel “a” in one long breath, while increasing the loudness from low to high and then decreasing the loudness.
At the same time, patients were instructed to feel the movement and pressure of the diaphragm, in order to control the expiratory air flow better.
Primary outcome measure
The speech breathing level of the modified Frenchay Dysarthria Assessment was selected as the main indicator, which had five different levels of speech breathing dysfunction, namely:
(a) No abnormal situation.
(b) Due to poor breathing control, fluency was occasionally interrupted. The patient might realize that sometimes it was necessary to stop and take a deep breath, which required additional breathing to complete the task.
(c) The patient must speak quickly due to poor respiratory control and the voice may disappear. The patient might need four breaths to complete the task.
(d) The patient spoke when he/she inhaled or exhaled, or a breath was to shallow to process a few sentences. Poor coordination and obvious variability. The patient might need to breathe seven times to complete a task.
(e) The speech was severely distorted due to the inability to control breathing and only one word could be managed per breath.
Secondary outcomes
The comprehensive evaluation of dysarthria using the modified Frenchay Dysarthria Assessment, 21 which was composed of eight assessment items (reflex, respiration, lips, tongue, jaw, palate, larynx, and speech) and 28 sub-items (as shown in the Supplemental Appendix). Each item and sub-item were divided into five scales (from “a” to “e”) and the dysarthria was quantified by the number of “a” ratings.
Maximum phonation time 23 was measured by recording the duration of the continuous vowel “a” at a comfortable amplitude and pitch level after the maximum inspiration. Subjects were required to repeat the procedure three times according to the appropriate instructions, and the maximum duration was recorded.
Maximal counting ability 24 referred to the longest time that the subject could pronounce the /i/ sound in one breath after inhaling deeply, with continuous fluctuation in pitch and loudness. Three measurements were made, and the maximum value was recorded.
/s/ and /z/ referred to the longest time of pronunciation of /s/ and /z/ after taking a deep breath, respectively. The s/z ratio is the ratio of /s/ versus /z/. 25
Loudness 26 was divided into five levels (whisper, soft, conversation, loud, and shouting, corresponding to level 1, 2, 3, 4, and 5), and it was measured during conversation with the therapist.
All data were collected by experienced physicians at baseline and three weeks after the intervention.
Statistical analysis
The study used IBM SPSS Statistics, version 20 (IBM) for all statistical analyses. General statistical descriptions were used for demographic and clinical characteristics, such as number of cases (%), mean (SD), or mean (95% confidence interval (CI)) (Table 1). Speech breathing level and loudness level were classified as discontinuous variables, and were described according to the number of cases (%). The modified Frenchay Dysarthria Assessment, /s/, /z/, s/z ratio, maximum phonation time, and maximal counting ability, which did not follow normal distribution, were expressed as the mean (95% confidence interval (CI)). Mean (SD) was used for describing continuous variables with normal distribution.
Participant characteristics at baseline.
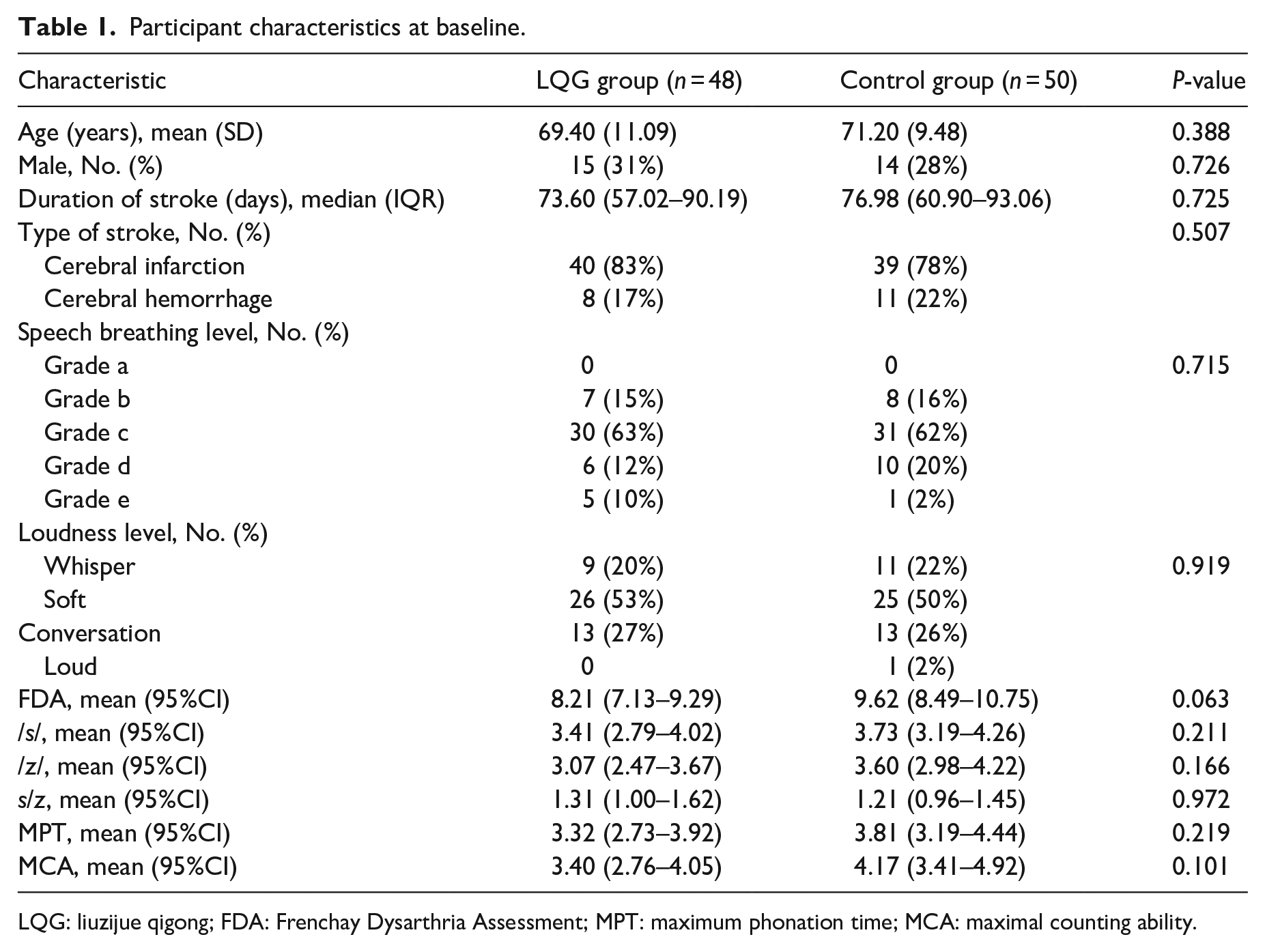
LQG: liuzijue qigong; FDA: Frenchay Dysarthria Assessment; MPT: maximum phonation time; MCA: maximal counting ability.
The Wilcoxon rank sum test was used when comparing two groups of discontinuous variables, such as the speech breathing level. Continuous variables, such as the modified Frenchay Dysarthria Assessment, /s/, /z/, s/z ratio, maximum phonation time, and maximal counting ability did not conform to a normal distribution, so the Wilcoxon signed-rank test was used within a group, and the Wilcoxon rank sum test was used between groups. Statistical significance was set at a P < 0.05.
Results
As Figure 1 showed, 100 patients were screened, and all of them met the inclusion criteria. Two subjects dropped out of the experiment due to change of condition (both in the liuzijue qigong group). A total of 98 cases were statistically analyzed (Figure 1). Baseline characteristics of patients allocated to the clinical study were presented in Table 1. There was no significant difference in baseline characteristics between the two groups (Tables 2 and 3). No serious adverse events were observed.
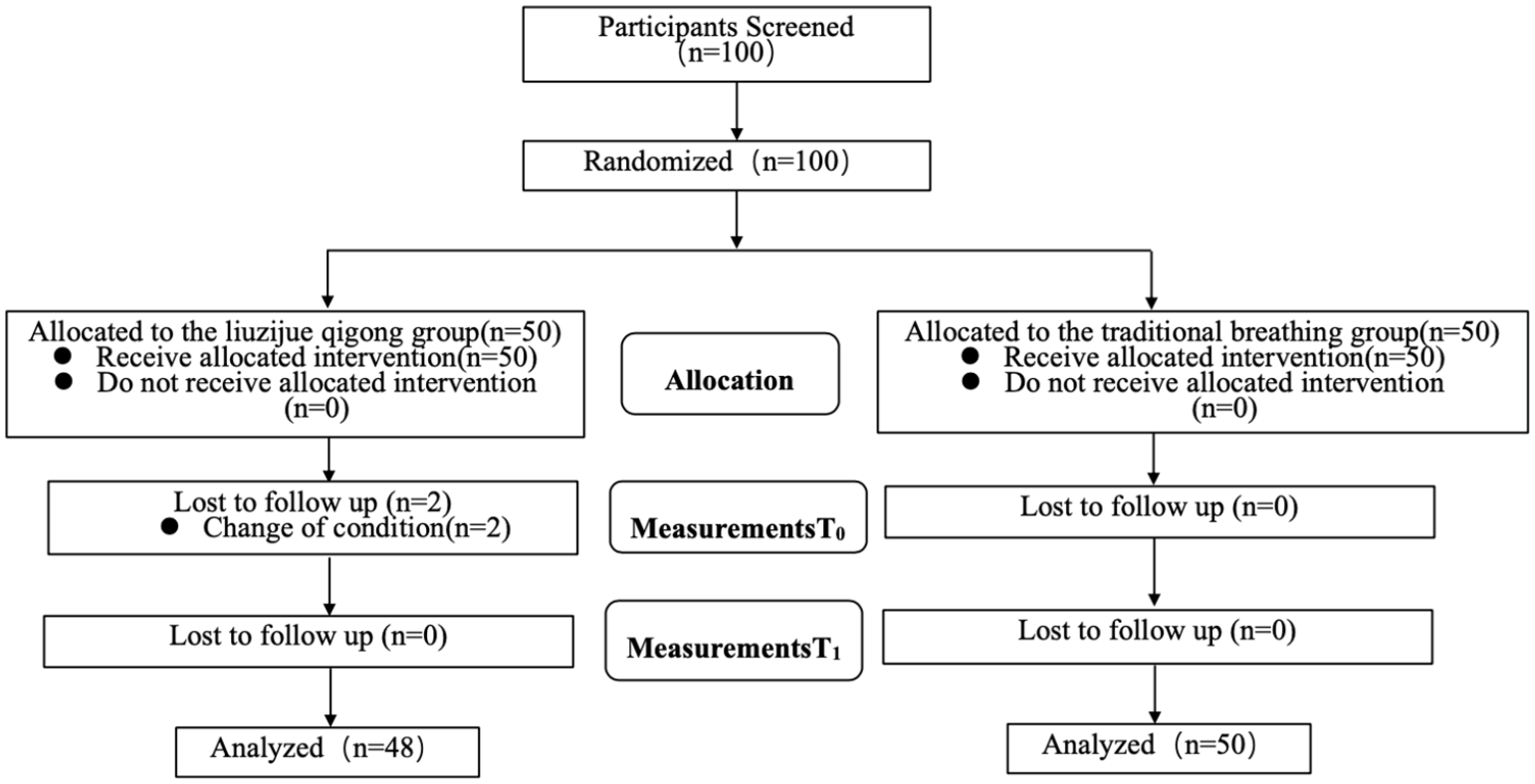
Flowchart.
Results of speech breathing level and loudness level.
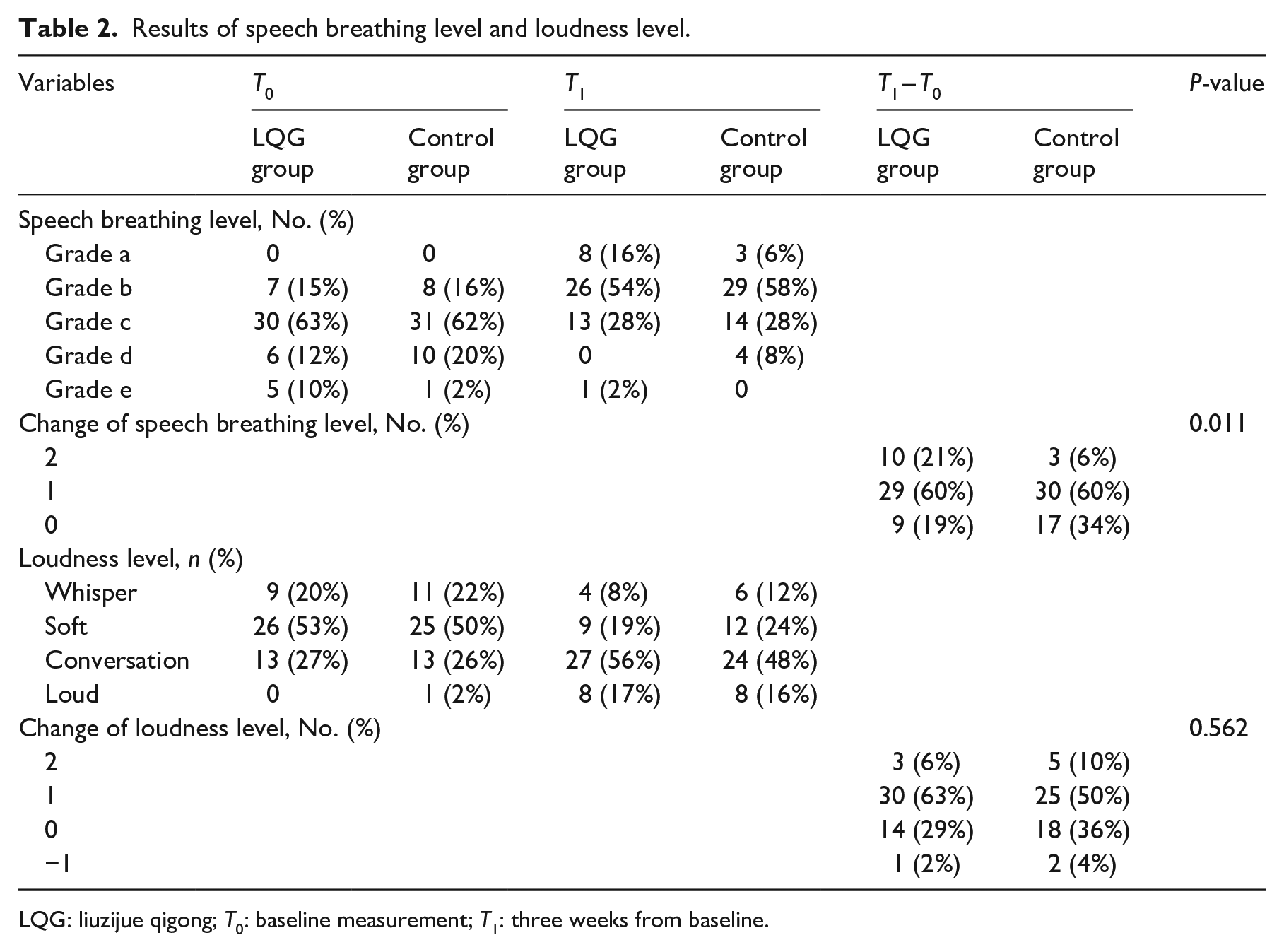
LQG: liuzijue qigong; T0: baseline measurement; T1: three weeks from baseline.
Results of Frenchay Dysarthria Assessment, /s/, /z/, s/z, maximum phonation time, maximal counting ability.
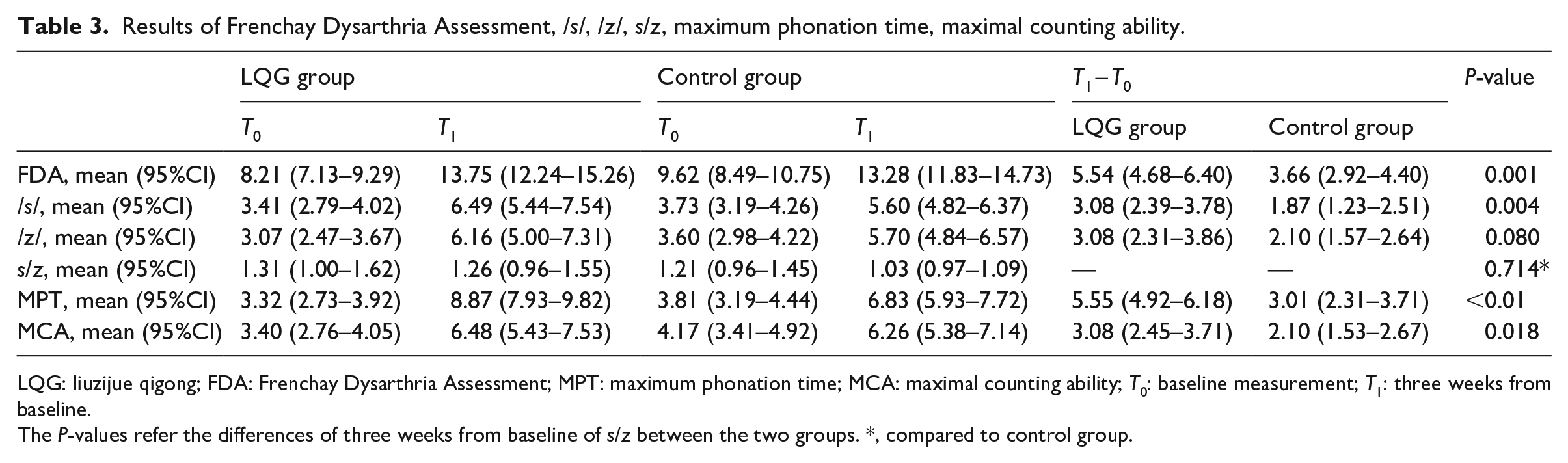
LQG: liuzijue qigong; FDA: Frenchay Dysarthria Assessment; MPT: maximum phonation time; MCA: maximal counting ability; T0: baseline measurement; T1: three weeks from baseline.
The P-values refer the differences of three weeks from baseline of s/z between the two groups. *, compared to control group.
After three weeks of intervention, the change of speech breathing level in the liuzijue qigong group was significantly better than that in the control group (P = 0.011). The level of 19% of patients in the liuzijue qigong group remained unchanged. It had been reduced by one level in 60% of patients, and it had been reduced by two levels in 21%. In contrast, the level of 34% of patients in the control group remained unchanged; it had been reduced by one level in 60%, and it had been reduced by two levels in 6% (Table 2).
There were statistically significant differences between the two groups in the modified Frenchay Dysarthria Assessment (5.54 (4.68–6.40) vs 3.66 (2.92–4.40), P = 0.001), maximum phonation time (5.55 (4.92–6.18) vs 3.01 (2.31–3.71), P < 0.01), maximal counting ability (3.08 (2.45–3.71) vs 2.10 (1.53–2.67), P = 0.018), and /s/ (3.08 (2.39–3.78) vs 1.87 (1.23–2.51), P = 0.004). However, no statistically significant differences were found in the change of /z/ (3.08 (2.31–3.86) vs 2.10 (1.5–2.64), P = 0.08), s/z ratio (1.26 (0.96–1.55) vs 1.03 (0.97–1.09), P = 0.714), or changes in loudness level (69% vs 60%, P = 0.562) between the two groups (Tables 2 and 3).
Discussion
In this study, it was found that liuzijue qigong could improve respiratory control and the comprehensive speech ability of patients with stroke-related dysarthria, in a superior way to traditional breathing training.
Both the inspiratory and expiratory muscles of stroke patients are affected, 27 resulting in reduced forced vital capacity and a reduced forced expiratory volume in one second of pulmonary ventilation function, 28 accompanied by a decrease of maximum expiratory and inspiratory pressures, in particular the maximum expiratory pressure. 29 Consequently, the impaired respiratory system cannot provide stable air flow and constant subglottal pressure, preventing the vocal cords from producing normal phonation. 30 Therefore, one of the goals of breathing training for speech is to improve respiratory functions. More precisely, sustained and stable air flow is the key to achieving the above goals. 3
Liuzijue qigong emphasizes gentle, extended, unconscious, and prolonged breathing, 16 which is a special type of breathing training that focuses on controlled exhalation. Our previous study found that liuzijue qigong improved the maximum inspiratory and expiratory pressures in stroke patients, indicating that it could provide and maintain continuous and stable respiratory airflow and appropriate lung capacity compared with traditional breathing exercises. 31 The reason may also be that liuzijue qigong, as low-load and slow-speed breathing training, more easily activated the main respiratory muscle groups composed of slow-twitch fibers, which were less likely to cause fatigue compared with only breathing muscle strengthening training. 32 Our study has confirmed that liuzijue qigong had a better effect on breathing support during speech, which was indicated by changes in the maximum phonation time and /s/.
Maximum phonation time was used as a direct estimate of respiratory support ability when speaking and an indicator of the efficiency of vocal respiratory mechanisms, as well as indirectly reflecting lung functions. 23 We found that the maximum phonation time ranged between 2.8 and 4.4 seconds in most patients before treatment, which was far lower than that of normal people, and was correlated to the poor respiratory support due to stroke. 3 Our results confirmed a significant improvement in maximum phonation time after liuzijue qigong compared to traditional breathing training. In addition, Tang et al. 33 demonstrated that maximum phonation time in unilateral vocal fold paralysis could be improved by two weeks practice of liuzijue qigong, which was consistent with our results.
The s/z ratio was an indicator of glottal efficiency, 34 combining information from maximum phonation tasks with voiceless /s/ emission and voiced /z/ emission. 35 Among them, /s/ and /z/ also, respectively, reflected respiratory support in the open and adducted states of the vocal cords. 36 In this study, we found that the /s/ and /z/ sounds of patients with motor dysarthria post-stroke were lower than those of healthy people before the intervention. 37 The results of the production of /s/ showed a significant improvement after liuzijue qigong training, which may be associated with increased lung vital capacity and improved respiratory support. However, the production of the /z/ sound was not significantly better than traditional breathing training, likely due to its requirement for higher respiratory support than pronunciation of the /s/. 38 Since the results of the s/z ratio were affected by the values of /s/ and /z/, we did not find a significant difference in the s/z ratio between groups.
The coordination of respiratory and phonatory was also an important target for the treatment of dysarthria. Existing studies have shown that breathing exercises alone were often inappropriate treatment for patients who could speak, and should be modified to synchronize training of breathing and phonation to promote better speech. 3 Maximal counting ability reflected the coordination of respiration and phonation for speech, 24 and accomplishing this task required not only considerable lung capacity, but also consistent and rhythmic contraction of the expiratory muscles, as well as regular, coordinated movements of the vocal cords. During liuzijue qigong exercise, the patients were asked to inhale quickly followed by prolonged exhalation, simultaneously. They needed to master the amount of air inhaled before speaking and learn how to control it during speaking. Repeated inhalation and exhalation training could facilitate switching between inspiration and expiration, in order to obtain considerable coordination and precision of movements. The amount of airflow, length and stability of breathing were adjusted appropriately through auditory feedback of the sounds of the six words. The results revealed that liuzijue qigong was more effective than traditional breathing training in improving patient’s maximal counting ability. In addition, a relevant study has reported that improvements in maximum phonation time were beneficial to the progress of maximal counting ability, suggesting that the establishment of stable respiratory airflow was also one of the important elements for the coordination of respiration and phonation. 24
The modified Frenchay Dysarthria Assessment was used to evaluate the severity of motor impairment of articulation organs, including various aspects of articulation functions (reflexes, breathing, and speech) and structure (lips, jaw, soft palate, larynx, and tongue). It was based on English, and the rehabilitation center of Hebei Provincial People’s Hospital made modifications to make it suitable for Chinese expression, which was termed the modified Frenchay Dysarthria Assessment. 39 The speech breathing level of the modified Frenchay Dysarthria Assessment was the primary indicator of this study 21 and was a comprehensive indicator that reflected respiration support and respiration/phonation coordination ability. The results showed that speech breathing level had been greatly improved in the liuzijue qigong group compared to the control group and this finding was probably because liuzijue qigong provided steady breathing support and worked on respiration/phonatory coordination during speech, producing more syllables in one breath. Once the foundation for breathing and phonation was well established, the patient could more easily use basic stimuli for progressive training, such as vowels, and then on to diphthongs, syllables, sentences, and conjunctions.
The limitations of diaphragmatic movement after a stroke are very common, but upper limb exercise has been proven to be conducive to increasing the diameter of the lower chest cavity and movements of the diaphragm. 40 Liuzijue qigong was also coordinated with corresponding upper limbs movement guidance, which should be carried out in a relaxed, slow, and gentle manner. Each word corresponds to the abduction of the upper limbs and expansion of the chest, especially Si, Chui, and Xi. 16 The duration of the accompanying upper limb movements was synchronized with breathing and vocalization for as long as possible. Zheng’s study also reported an improvement in diaphragmatic activity after liuzijue qigong. 31 Therefore, the gentle upper limb movement of this technique was conducive to guiding prolonged breathing, increasing lung capacity and diaphragmatic activity, improving the coordination of respiratory muscles, and ultimately benefiting improvement of respiratory control during speech.
Liuzijue qigong should not only play a positive role in speech breathing abnormalities but also in disorders of the vocal cords and articulation organs. Studies have shown that disturbances of vocal cord adduction in stroke patients include hypoadduction and hyperadduction. 41 When the slow and gentle airflow produced by liuzijue qigong stimulated the surrounding laryngeal muscles, better laryngeal muscle tension was likely to be maintained. At the same time, the vocal cords of the 6 words were all in the state of partial adduction, which might be not only beneficial to promote adductor strength but also relieve spasm of the vocal cords. Moreover, the resistance to airflow imposed by the corresponding articulators made the airflow slower and more even, avoiding the appearance of plosives and aggravation of vocal cord hyperadduction. Hence liuzijue qigong should be applicable to individuals suffering with spastic dysarthria and mixed dysarthria. In addition, the 6 sounds were produced by different organs and involved different mouth shapes and tongue movements. 16 Considering that the airflow produced by respiratory systems was then modified and molded by the articulatory and velopharyngeal, 42 such pronunciation exercises could significantly improve the strength, range and coordination of the articulation organs, and create the necessary conditions for producing clear and meaningful speech. 43 Thus, the results of modified Frenchay Dysarthria Assessment, reflect comprehensive speech ability, 21 and was better than traditional breathing training after liuzijue qigong training.
In conclusion, liuzijue qigong training can improve respiration, vocalization, and the articulatory systems associated with speech production.
However, we found no significant difference in the loudness level between the groups. Characteristics of loudness abnormities due to stroke include a too low or too high volume, uncontrollable changes in volume and an inability to speak quietly. Loudness may be used as an indicator of impaired respiratory support/coordination, but it was difficult for the evaluators to make an objective assessment, which may lead to poor reliability of the results. 26 In future studies, the decibel value will be used to quantify the loudness level, which may be a more objective evaluation method.
Limitations
First, considering that this was a preliminary study to explore the effects of liuzijue qigong on dysarthria after stroke, the treatment period lasted for only three weeks, in order to ensure more controllable training quality and to be less affected by other factors. Long-term clinical trials are unlikely to be carried out in inpatient units and convalescent patients are only allowed to stay for two to three weeks because of limited medical resources. In the future, we will conduct longer-term studies in community hospitals and rehabilitation institutions to obtain more reliable data. Second, aerodynamic analysis including water glass manometer and spirometer measurements have often served as indicators to measure subglottal pressure and average airflow in clinical practice. In future studies, differences in air flow and pressure when producing the six sounds will be evaluated to determine their possible impact.
Conclusions
Our results showed that compared with traditional breathing training applied in the control group, liuzijue qigong, combined with basic articulation training, could improve the respiratory control ability, as well as the comprehensive speech ability, with post-stroke dysarthria patients. These findings indicated that the clinical effect was more better toward liuzijue qigong, and its clinical application may have broad prospects.
Clinical messages
Liuzijue qigong led to more changes than the traditional breathing training in improving respiratory control and comprehensive speech ability for stroke patients with dysarthria.
Supplemental Material
sj-pdf-1-cre-10.1177_0269215521992473 – Supplemental material for Liuzijue qigong versus traditional breathing training for patients with post-stroke dysarthria complicated by abnormal respiratory control: Results of a single-center randomized controlled trial
Supplemental material, sj-pdf-1-cre-10.1177_0269215521992473 for Liuzijue qigong versus traditional breathing training for patients with post-stroke dysarthria complicated by abnormal respiratory control: Results of a single-center randomized controlled trial by Jie Wang, Gaiyan Li, Shanshan Ding, Long Yu, Yan Wang, Lei Qiao, Qilin Wu, Weidong Ni, Hang Fan, Qianyun Zheng, Ying Zhang and Hongli Li in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors thank all individuals who participated in the study. Ying Zhang and Hongli Li were responsible for the conception and design.
Author contributions
Jie Wang, Ying Zhang, Hongli Li, Gaiyan Li, Shanshan Ding and Long Yu wrote the manuscript, including data interpretation, the first draft and revision. Gaiyan Li, Long Yu and Yan Wang were responsible for patient recruitment and enrollment, data acquisition, and statistical analyses were conducted by Jie Wang. Weidong Ni and Lei Qiao were responsible for liuzijue qigong training. Hang Fan and Qianyun Zheng performed traditional breathing training. Shanshan Ding and Qilin Wu participated in the evaluation of indicators for clinical trials. Ying Zhang and Hongli Li revised and reviewed the first draft and agreed on the final version of the submitted manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funded by the Shanghai Municipal Health Commission (Shanghai Traditional Chinese medicine development office), Shanghai Disabled Persons’ Federation;
Ethical approval
The implementation of this study was based on the the Declaration of Helsinki, and the Consolidated Standards of Reporting Trials. This study was approved by the Ethics Committee of Shanghai Xuhui Central Hospital (reference no. 2016-31).
Trial registration
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.