
Abstract
Objectives
To evaluate 20 days and 3 months follow-up effectiveness of cardiac rehabilitation (CR) enhanced by resistance/balance training and telephone-support program compared to usual CR care in improving quality of life, clinical course and physical activity behavior.
Design
Single-centre randomized controlled trial.
Setting
Inpatient CR clinic
Subjects
116 (76.1 ± 6.7 years, 50% male) patients 14.5 ± 5.9 days after valve surgery/intervention were randomized to intervention group (IG, n = 60) or control group (CG, n = 56).
Intervention
Additional resistance/balance training (3 days/week) during phase-II CR and telephone-support program during 3-month follow-up. CG patients were provided with usual CR care.
Main measures
Short Form 36 Health Survey scales, European Quality of Life 5 Dimensions 3 Level Version QoL index, visual analog scale, clinical course, and physical activity behavior assessed with standardized questionnaires.
Results
IG reported statistically significant higher mental component score (48.5 ± 6.91 vs. 40.3 ± 11.21 at the baseline, 50.8 ± 9.76 vs. 42.6 ± 9.82 after 20 days, 49.4 ± 8.45 vs. 40.5 ± 8.9 after 12 weeks follow up), general health (48.6 ± 3.17 vs. 45.0 ± 2.95 at the baseline, 53.6 ± 3.02 vs. 43.8 ± 2.55 after 20 days, 53.2 ± 3.11 vs. 44.2 ± 3.07 after 12 weeks) and role limitations due to emotional problems (48.5 ± 15.2 vs. 27.7 ± 11.5 at the baseline, 72.7 ± 12.6 vs. 30.5 ± 11.2 after 20 days, 66.6 ± 14.2 vs. 36.1 ± 11.2 after 12 weeks) in all three assessments (p < 0.05). CG patients had more documented hospital admissions (4 (8%) vs 10 (25%), p = 0.027), atrial fibrillation paroxysms (3 (6.0%) vs. 10 (35.0%), p = 0.011) and blood pressure swings (13 (26%) vs. 20 (50%), p = 0.019). IG patients chose more different physical activities (1.7 ± 0.7 vs. 1.25 ± 0.63, p = 0.002), spent more time being physical active every day (195.6 ± 78.6 vs. 157.29 ± 78.8, p = 0.002)
Conclusions
The addition of resistance/balance exercises and telephone-support program 12 weeks after to the CR could linked to higher physical activity levels and fewer clinical complications but did not lead to a significant improvement in quality of life.
Keywords
Background
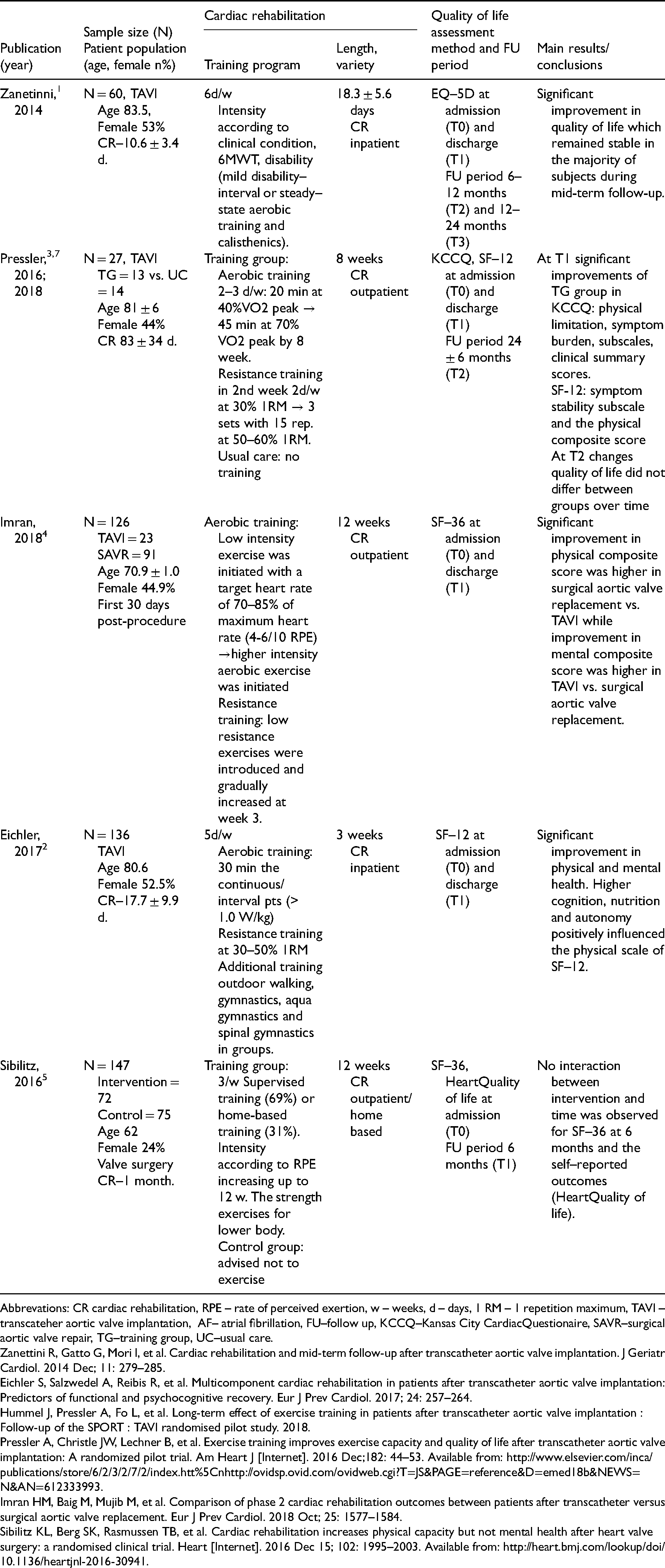
Improving the quality of life of older people with multiple chronic conditions and a high degree of frailty may be as important as a survival benefit. 1 Although cardiac rehabilitation (CR) is widely recommended for patients undergoing valvular surgery and interventions, 2 few studies have evaluated its impact on quality of life1–6 (see Appendix 1) and the results are controversial. A Cochrane meta-analysis confirms the lack of evidence-based data in this area. Only two of the integrated studies evaluated the impact of CR on quality of life. 6
Physical inactivity could be another burden for older patient recovering after open heart surgery. The results of a large cohort study (n = 6587) revealed a significant association between insufficient physical activity after heart valve surgery and higher risk of mortality within 5 years follow-up. 7 A meta-analysis (40 randomized control trials, N = 6480) of the effects of CR on physical activity levels found moderate evidence of an increase in physical activity with participation in rehabilitation compared with controls. 8
In this context, the focus must be placed on the content and setting of exercise-based CR, with the question of how the greatest therapeutic effectiveness can be achieved. Age- and/or disease-related loss of muscle mass and strength can be the main reason for reduced levels of activities of daily living, mobility and participation, and therefore critically affects patients' quality of life. Appropriate resistance/balance training can improve the ability to develop muscular strength in the elderly. 9 Nevertheless, these training methods are not routinely used in the CR of these patient populations, and their impact on the effectiveness of CR measures has been poorly studied. 10 What is more, while telephone support programs are well established in particular fields of CR, there are lack of evidence in others. 11
The aim of our study was (1) to evaluate 20 days and 3 months follow-up effectiveness of CR enhanced by resistance and balance training and telephone support program compared to usual CR care in improving quality of life; (2) to investigate its impact on the patient's clinical course and their physical activity behavior in the first three months after completion of CR.
Methods
The study was a single-centered randomized controlled trial with parallel group design with follow-up at 3 months conducted at Kulautuva rehabilitation center at Lithuania University of Health Sciences Hospital's (Kulautuva, Lithuania). This study was conducted according to the principles of good clinical practice. It was approved by the local ethical board (Kaunas Regional Biomedical Research Ethics Committee No. BE-2-39, BE-2-57), registered at ClinicalTrials.gov (NCT04234087) and drawn up in accordance with the Consolidated Standards of Reporting Trials (CONSORT) statement guideline. The Lithuanian University of Health Sciences was responsible for oversight of study conduct and governance. Inclusion period was January 2018 to November 2019.
Inclusion criteria were: age ≥65 years; the ability to start CR within ≤4 weeks after valve surgery or transcatheter aortic valve implantation; 6-min walk distance ≥100 - ≤350 m to ensure homogeneity of the study population; and patient consent to participation in the study. Exclusion criteria were: heart failure New York Heart Association Class IV; 12 hemoglobin <9 g/dL; wound healing disorders; cognitive and/or mental disorders; linguistic deficits; as well as exercise-limiting comorbidities (primarily orthopedic, neurological conditions) that would exclude the patients from participating in CR according to study protocol.
Patients were screened for eligibility by a physician on the first day of admission to the inpatient CR clinic (14.5 ± 5.9 days after valve surgery or intervention). A sample of 116 patients (76.1 ± 6.7 years, 50% male) who fulfilled the inclusion criteria were randomized (allocation ratio 1:1) to the intervention (n = 60) or a control group (CG) (n = 56) using a computerized list
All study participants attended standardized 20-calendar-day inpatient multidisciplinary phase-II CR, including patient education: diet counseling and risk factor management, psychological support (individual counseling, auto-relaxation education, smoking cessation) as well as individually dosed and adapted exercise training with continuous endurance training, gymnastics and respiratory muscle training (see Appendix 3). Duration and intensity of the exercise session were individually adapted based on clinical and functional status.
Subjects randomized to the intervention group (IG) received additional individually tailored exercise sessions of resistance and balance training delivered by a physical therapist in a small group (3 patients) (see Appendix 4). The resistance training was started at the earliest on the third CR day. The focus was on lower limb muscle training, including 4–6 exercises with free weights, resistance bands, gravity-assisted exercises, and exercise equipment (HUR, Finland). The training was started with low intensity (< 30% 1-repetition maximum, rate of perceived exertion (Borg scale) ≤ 11, 5–10 repetitions) and was gradually increased up to moderate intensity (30–50% and up to 60% 1-repetition maximum, rate of perceived exertion (Borg scale) 12–13, 8–15 repetitions) performing 3 sets with a 3 min rest between sets, if tolerated. The balance training included exercises to improve static and dynamic balance ability. It was performed on 2–3 days/week for 10–15 min. The complexity of the balance exercises was selected and incremented individually by changing the standing position (standing on both legs/standing upright/standing on one leg), the base on which the stands were performed (flat/uneven) and/or using unstable surfaces. Furthermore, if tolerated, the visual information was varied (open/closed eyes) and/or additional tasks performed while balancing. After completion of the CR, the IG participants were encouraged to continue the exercise training at home according to the physiotherapist recommendations. Furthermore, participants received a telephone call every second week during the 12 weeks follow up period (6 calls in total) where they were asked to answer questions regarding their health and physical activity as well as encouraged to continue exercise training and be physically active. CG patients were given general physical activity recommendations and received one call for a follow-up visit arrangement.
There were three assessment times: before randomization (admittance to CR); at after 20 days CR; and at three months after CR completion. All assessments were blinded and performed by certified staff members that were not involved in clinical care (two medical doctors with specialization in cardiology, one physiotherapist and one nurse).
Quality of life was assessed only during live visits using two different quality of life questionnaires: European Quality of Life 5 Dimensions 3 Level Version (EQ-5D-3L) and the Short Form 36 Health Survey (SF-36). The SF-36 is a 36-item, patient-reported survey of patient health and measures eight scales: physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health. The Physical Component Summary and Mental Component Summary were calculated from all scales do in different proportions to the scoring of both physical and mental measures. 13 For both questionnaires validated Lithuanian versions are available. 14
The assessment also included medical history (i.e. cardiac diagnosis, cardiovascular risk factors, concomitant diseases), hospitalizations since the last examination taken from medical records and standardized interview regarding patients’ clinical course, and physical activity habits after completion of the CR (see Appendix 2). Physical performance and physical frailty were assessed using Short Physical Performance Battery - SPPB test (0–7 points – frail, 8–9 pre-frail, 10–12 – robust). 15
Patients who agreed to participate but did not attend the follow-up visit, received additional telephone call and were asked to answer the same standardized questions (see Appendix 2) regarding their clinical course, events, hospitalization since last examination and physical activity habits within the three months after completion the CR and were included in the analysis. Participants who could not be reached by phone after 12 weeks were considered “lost in follow-up,” and their vital status was checked in the Lithuanian national e-health system.
The sample size was calculated as a function of the expected change in the results of the SPPB score. In order to detect a 1 standard deviation difference in SPPB score between the arms, we calculated we would need 91.4 evaluable patients under the assumption of a two-sided type I error of 5% and a power of 80% (t-test). Rounding up and accounting for an expected loss to follow-up of 5% (in terms of missing primary outcome data), implied that we would require a sample size of ∼96 patients. Trial was ended after calculated sample size + 20% was reached.
All analyses were performed in the intention-to-treat population integrating the data of all randomized patients. Continuous and categorical variables are presented by mean, standard deviation, absolute, and relative frequencies. Chi-square tests and t-tests were used to test for baseline differences between groups. Multivariate analysis of variance with repeated measurements was used for statistical analyses of time-, group-, and treatment-related changes and differences, with p < 0.05 considered as significant. Results were analyzed in two stages: first, global means were interpreted and, second, the marginal scores were compared if the respective p-value was significant. All tests were performed two-sided with p-values less than 0.05 indicating significance. Statistics were calculated using Jamovi 1.0.8.
Results
Patient baseline characteristics are summarized in Table 1, study flowchart is demonstrated in Figure 1.
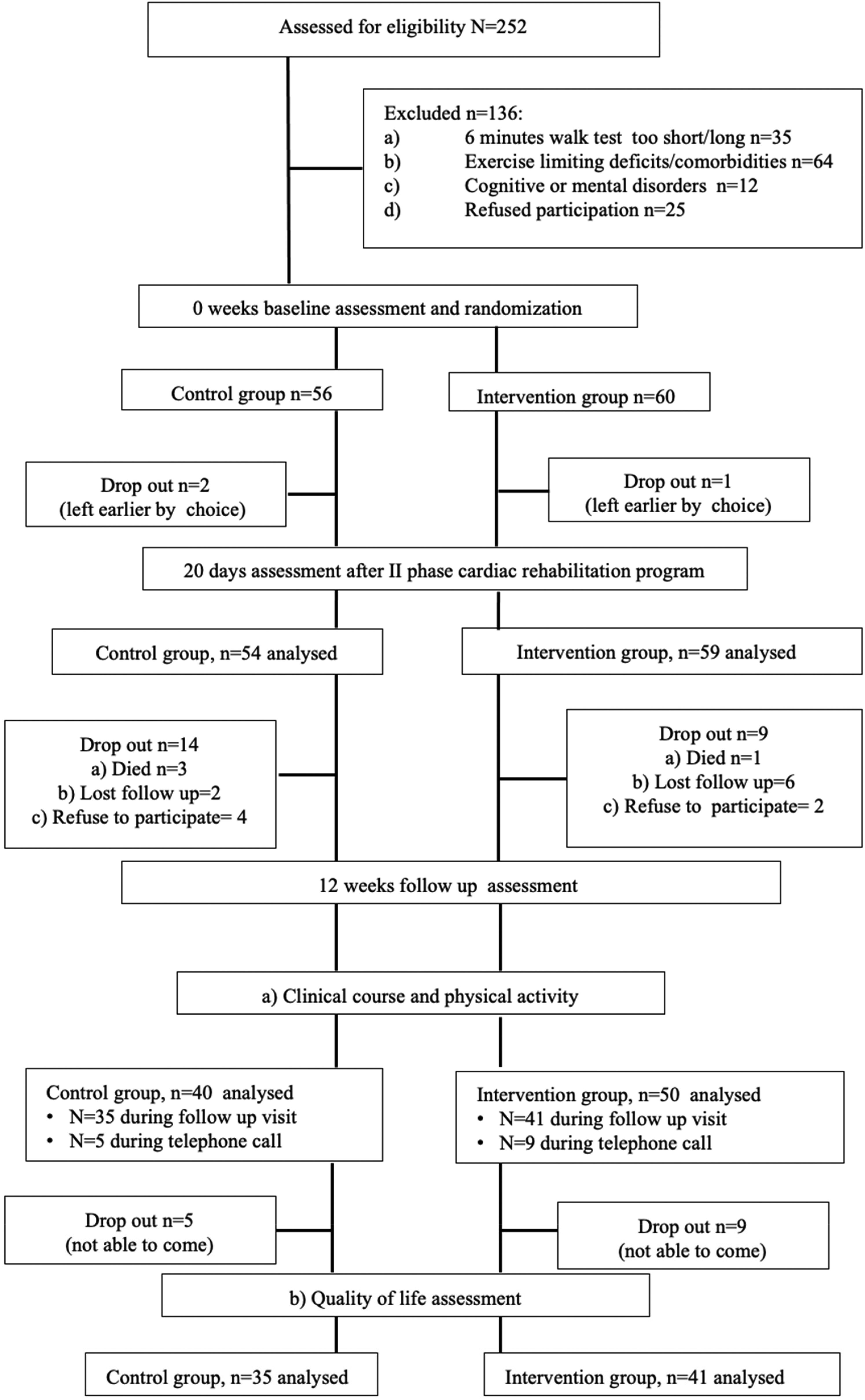
Study flow-chart.
Patient baseline characteristics, differentiated between control and intervention groups.
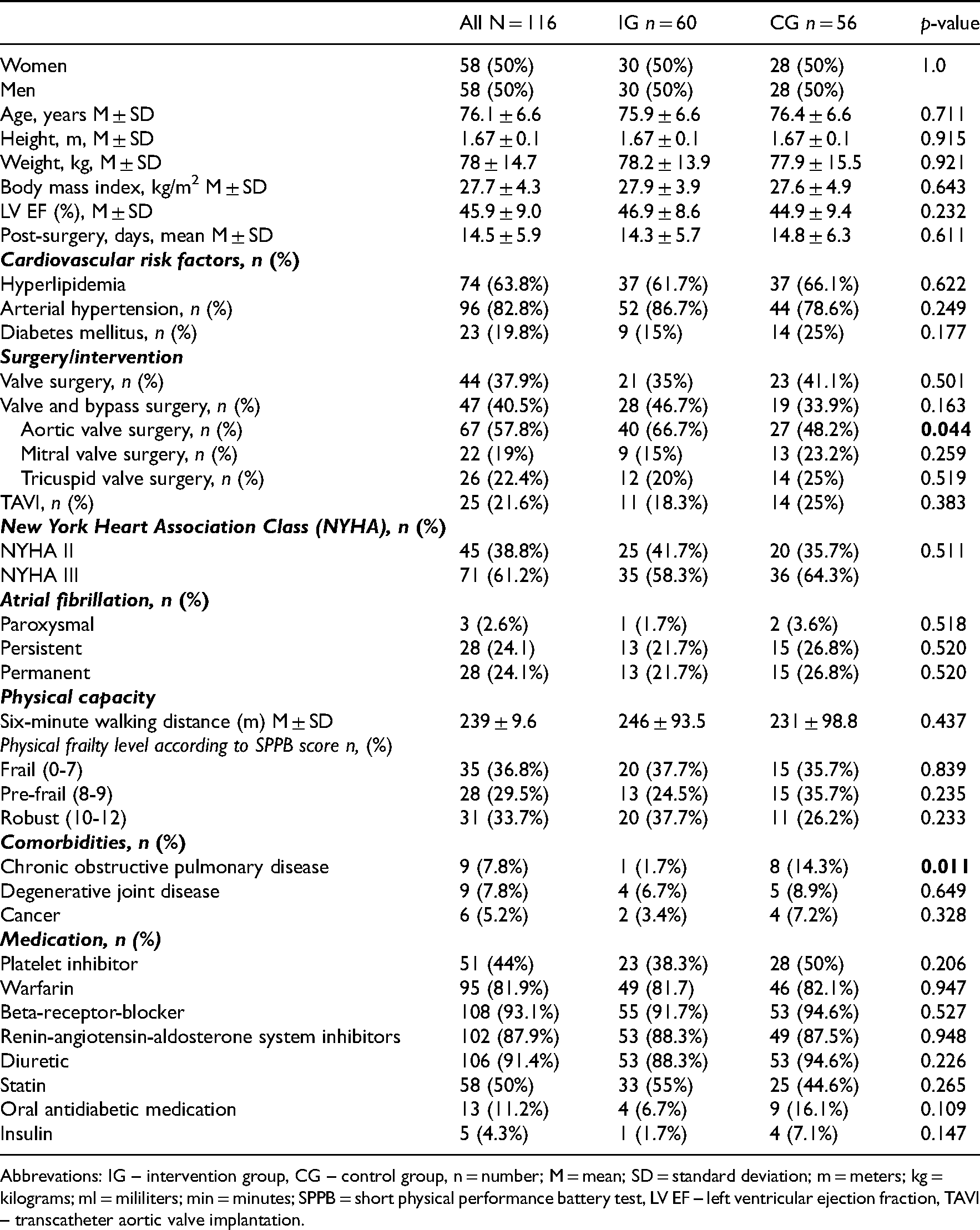
Abbrevations: IG – intervention group, CG – control group, n = number; M = mean; SD = standard deviation; m = meters; kg = kilograms; ml = mililiters; min = minutes; SPPB = short physical performance battery test, LV EF – left ventricular ejection fraction, TAVI – transcatheter aortic valve implantation.
The main outcomes of the 20-day CR on quality of life are summarized in Table 2. The results show neither significant difference between groups nor significant intervention effect (p-value interaction).
Short-term (20 days) results on quality of life measured by SF-36 (eight scales and 2 summary scores) and EQ-5D-3L (index score and visual analog scale) questionnaires. Multivariate analysis of variance with repeated measurements were used to detect changes between intervention and control groups.
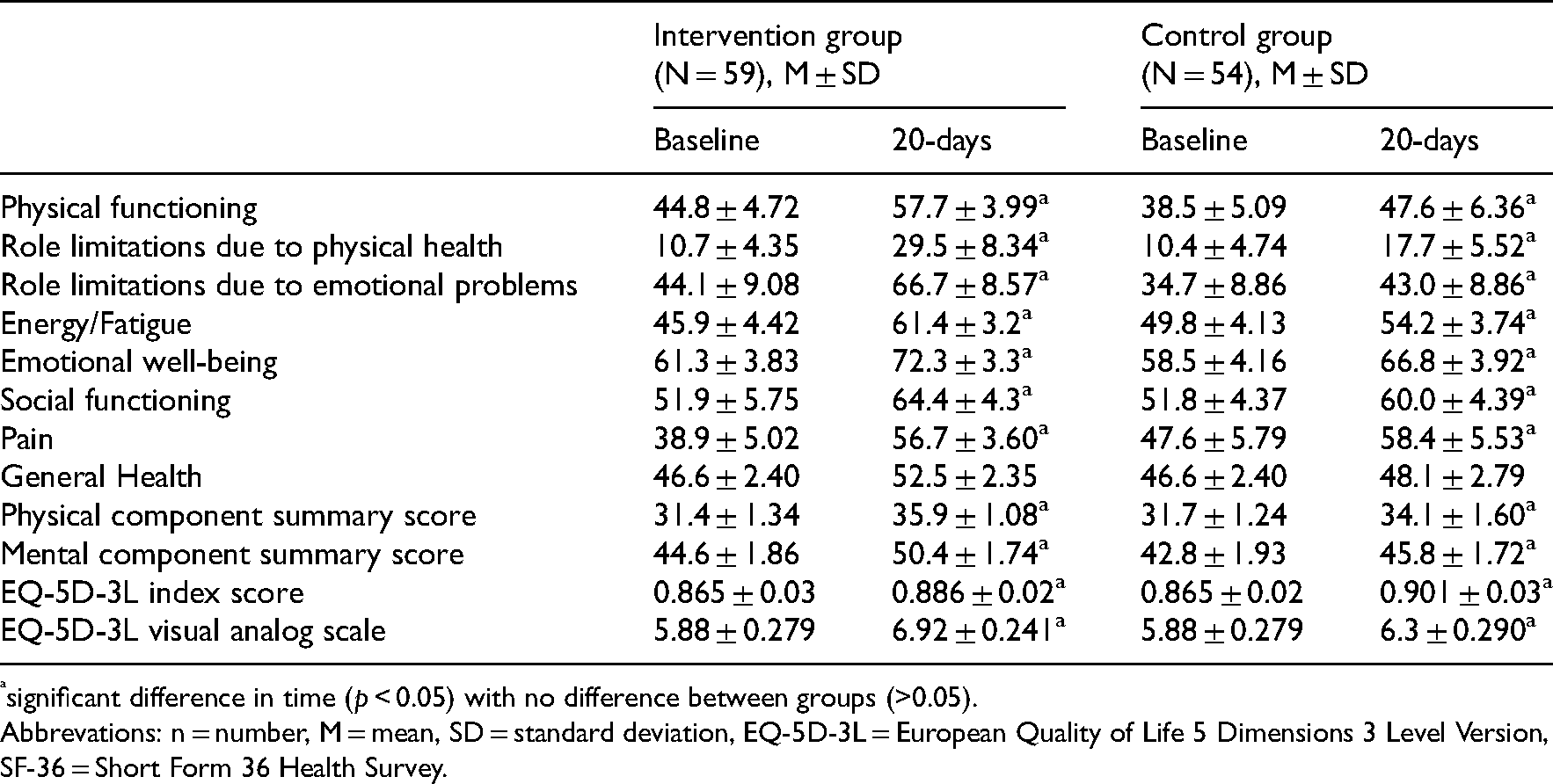
significant difference in time (p < 0.05) with no difference between groups (>0.05).
Abbrevations: n = number, M = mean, SD = standard deviation, EQ-5D-3L = European Quality of Life 5 Dimensions 3 Level Version, SF-36 = Short Form 36 Health Survey.
The main outcomes after 3 months follow-up on quality of life are summarized in Table 3. Only the results of patients who attended all three visits were included in the analysis. Compared to CG the IG reported significantly higher quality of life scores for role limitations due to emotional problems, general health, and total mental health component scores at all three visits, with no significant change over time.
Medium-term results on quality of life measured by SF-36 (eight scales and 2 summary scores) and EQ-5D-3L (index score and visual analog scale) questionnaires. Multivariate analysis of variance with repeated measurements were used to detect changes between intervention and control groups.
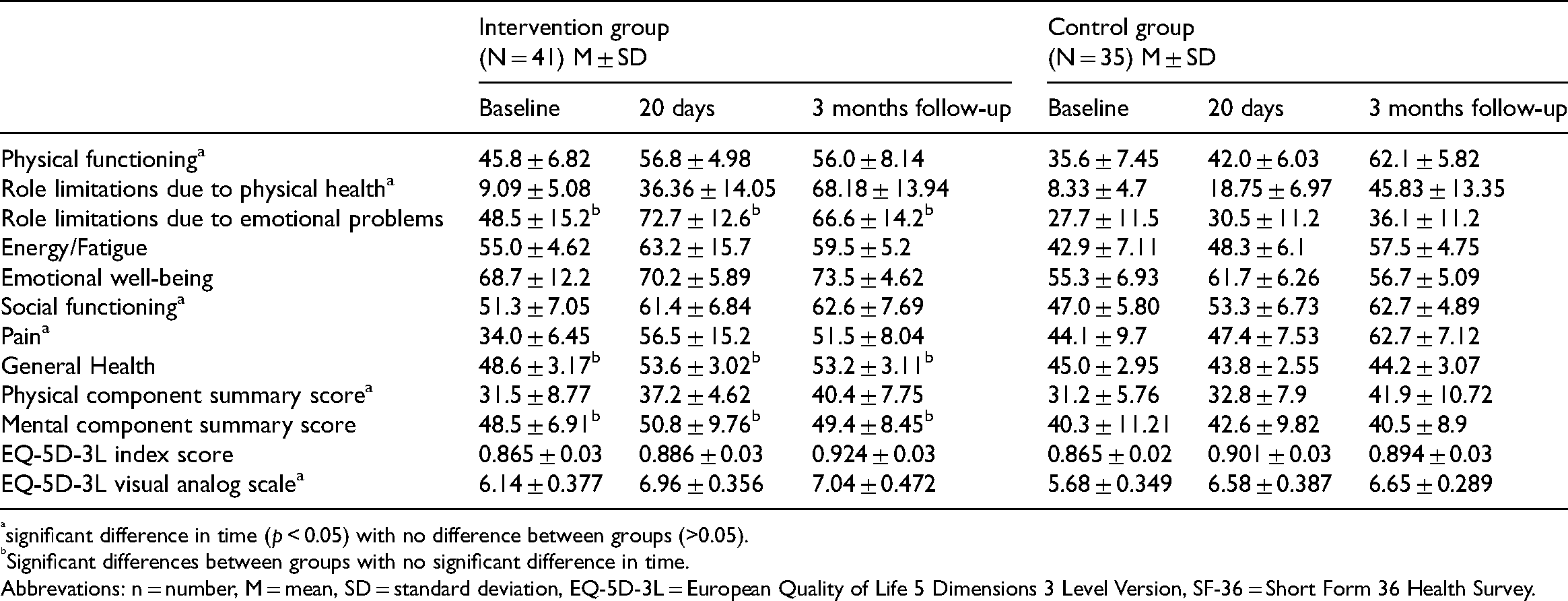
significant difference in time (p < 0.05) with no difference between groups (>0.05).
Significant differences between groups with no significant difference in time.
Abbrevations: n = number, M = mean, SD = standard deviation, EQ-5D-3L = European Quality of Life 5 Dimensions 3 Level Version, SF-36 = Short Form 36 Health Survey.
During 3 months follow-up period four patients died (IG n = 1; CG n = 3) (Table 4). The patients in the CG reported a more complicated clinical course during the 12-week follow-up period. Compared to IG there were significantly more cases of hospitalization documented in the CG. Furthermore, CG patients were significantly more often diagnosed with atrial fibrillation paroxysms and uncontrolled blood pressure episodes during 12-week follow up. What is more, IG patients tend to choose more different physical activities and spent significantly more time being physically active within the first 12 weeks after CR, compared to CG (Table 4).
Patients 3 months follow up results differentiated between control and intervention groups. Chi-square and T-tests were used to detect changes between intervention and control groups.
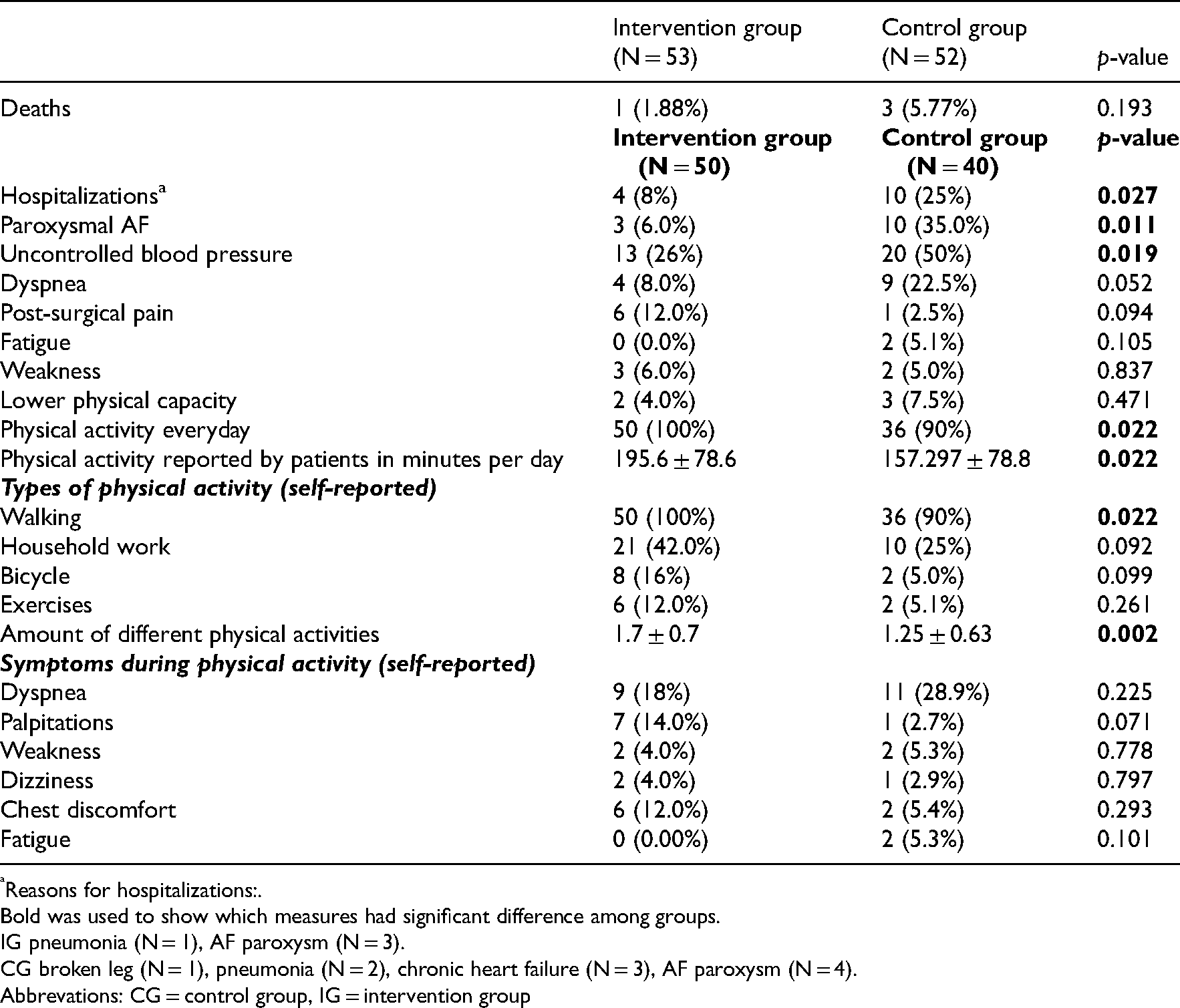
Reasons for hospitalizations:.
Bold was used to show which measures had significant difference among groups.
IG pneumonia (N = 1), AF paroxysm (N = 3).
CG broken leg (N = 1), pneumonia (N = 2), chronic heart failure (N = 3), AF paroxysm (N = 4).
Abbrevations: CG = control group, IG = intervention group
Discussion
In this randomized clinical trial, we compared the outcomes of an usual care CR and CR program enhanced by resistance/balance training and telephones support, in older patients after valve surgery and intervention. The outcomes demonstrate no significant effect on quality of life. Patients of the IG reported significantly higher physical activity levels within the first 12 weeks after CR. Furthermore, the results demonstrate significant difference between groups in clinical course within the first 12 weeks after CR including fewer hospital readmissions in the IG.
Results of our study demonstrated that during 3 months follow-up period CG patients were more often hospitalized, diagnosed with atrial fibrillation and blood pressure swings. While patients that participated in additional resistance and balance training spend more time being physically active and choose more different physical activities compared to CG during follow-up. This is an important finding. Muscular strength and endurance are key components of physical fitness and the basis for every physical activity 16 A minimum level of muscle strength and endurance is necessary to maintain the ability to perform activities of daily living and functional independence in old age and/or in the presence of disease-related limitations. 16 Our study results correspond with Lund et al. that found that valve surgery patients who participated in exercise-based CR were more likely to have a moderate or high physical activity level (27). 17 Current guidelines recommend to include individually adapted exercises to improve coordination (especially sensomotoric training and balance training) into the exercise based CR especially in older and/or frail patients. 18
Its already known that telephone support programs in CR for heart failure patients demonstrate its effectiveness to reduce the risk of all-cause mortality and heart failure-related hospitalizations as well as to improve health-related quality of life. 11 No study results are available on the effectiveness of telephone support programs in elderly patients after heart valve surgery or intervention. The results of our study show that telephone calls every two weeks during 12 weeks follow-up after CR could be linked with higher physical activity in the IG while no significant effect on quality of life was found.
Available studies evaluating the impact of exercise-based CR on quality of life for patients after valve surgery or intervention, demonstrate that significant increase in quality of life can be expected at discharge from CR,2,4 while follow-up results are controversial. The results of a small randomized control trial (N = 27) including patients after transcatheter aortic valve intervention demonstrated significantly higher quality of life values (measured by Kansas City cardiomyopathy questionnaire and SF-12) in CR participants at discharge compared to no-training group. 3 In contrast, no significant differences in quality of life values between groups were observed at 24-month follow-up. 3 In the CopenHeart trial (randomized control trial; N = 147) no significant differences between CR and usual care were demonstrated in SF-36 mental component score and HeartQuality of life results at 6 months follow up after CR. 5 On the other hand Zanettini et al. showed a significant improvement in quality of life (EQ-5D) at discharge from inpatient CR in elderly patients after transcatheter aortic valve intervention which remained stable in the majority of subjects during 6–12 months follow-up. 1
The addition of resistance and balance exercises to the CR program and the controlled continuation of the exercise program in the first 12 weeks after rehabilitation did not lead to a significant improvement in quality of life scores in the IG compared with the control. Nevertheless, it may be assumed that the observed higher physical activity levels and fewer clinical complications during the 12 weeks follow-up period reported in the IG compared to CG are at least partly the result of the additional intervention provided. However, given the high number of missing data at this visit, the benefit of additional resistance and balance training is unclear and future studies are needed to learn more about optimal CR exercise regime in this patient cohort.
Study limitations
The study has several limitations: (1) This was a single-center study and the results may not be generally applicable to all patients after heart valve surgery or intervention; (2) Patient population was heterogenic as the study included patients after open-heart surgery and transcatheter aortic valve intervention; (3) The results may be affected by the imperfect adherence to the intervention and fewer training sessions fulfilled than originally planned - 6.1 ± 1.2 on average (out of 9); (4) A significant number of drop-outs and missing data cases complicated the statistical analysis and limit study results; (5) The study was unblinded for patients and staff, although during evaluation of physical tests, all researchers were blinded to the allocation group; (6) We used standardized questions rather than validated questioners while evaluating participants physical activity levels.
Clinical messages
Additional resistance and balance training in CR did not affects quality of life of patients after valve surgery/intervention.
Participation in additional resistance and balance training together with telephone support program could led to higher physical activity levels and fewer clinical complications in 3 months follow-up.
Declarations
We declare that our study adheres to CONSORT guidelines. The CONSORT checklist is attached as an supplementary file.
Footnotes
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request
Author contributions
Eglė Tamulevičiūtė-Prascienė Conceptualization, Methodology, Investigation, Writing - Original Draft, Aurelija Beigienė: Investigation, Kamilė Gerulytė, Urtė Lukauskaitė: Investigation, Writing - Original Draft, Raimondas Kubilius Conceptualization, Writing - Review & Editing; Birna Bjarnason-Wehrens: Conceptualization, Methodology, Writing - Original Draft.
All authors have read and approved the final manuscript
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethics approval
Our study protocol was approved by the Lithuanian University of Health Sciences Kaunas Regional Biomedical Research Ethics Committee (Nr. BE-2-39, BE-2-57). All patients gave their written consent to participation in the study. The study was conducted according to the principles of good clinical practice.
Trial registration
NCT NCT04234087, Registered 21 January 2020, https://clinicaltrials.gov/ct2/show/NCT04234087?term=Tamuleviciute-Prasciene&draw=2&rank=1
Appendix 1. Characteristics of authors personally reviewed studies on valve surgery/intervention,cardiac rehabilitation and quality of life
| Publication |
Sample size (N) |
Cardiac rehabilitation | Quality of life assessment method and FU period | Main results/conclusions | |
|---|---|---|---|---|---|
| Training program | Length, variety | ||||
| Zanetinni, 1 2014 | N = 60, TAVI Age 83.5, Female 53% CR–10.6 ± 3.4 d. |
6d/w Intensity according to clinical condition, 6MWT, disability (mild disability–interval or steady–state aerobic training and calisthenics). |
18.3 ± 5.6 days CR inpatient |
EQ–5D at admission (T0) and discharge (T1) FU period 6–12 months (T2) and 12–24 months (T3) |
Significant improvement in quality of life which remained stable in the majority of subjects during mid-term follow-up. |
| Pressler, 3 ,7 2016; 2018 | N = 27, TAVI TG = 13 vs. UC = 14 Age 81 ± 6 Female 44% CR 83 ± 34 d. |
Training group: Aerobic training 2–3 d/w: 20 min at 40%VO2 peak → 45 min at 70% VO2 peak by 8 week. Resistance training in 2nd week 2d/w at 30% 1RM → 3 sets with 15 rep. at 50–60% 1RM. Usual care: no training |
8 weeks CR outpatient |
KCCQ, SF–12 at admission (T0) and discharge (T1) FU period 24 ± 6 months (T2) |
At T1 significant improvements of TG group in KCCQ: physical limitation, symptom burden, subscales, clinical summary scores. SF-12: symptom stability subscale and the physical composite score At T2 changes quality of life did not differ between groups over time |
| Imran, 2018 4 | N = 126 TAVI = 23 SAVR = 91 Age 70.9 ± 1.0 Female 44.9% First 30 days post-procedure |
Aerobic training: Low intensity exercise was initiated with a target heart rate of 70–85% of maximum heart rate (4-6/10 RPE) →higher intensity aerobic exercise was initiated Resistance training: low resistance exercises were introduced and gradually increased at week 3. |
12 weeks CR outpatient |
SF–36 at admission (T0) and discharge (T1) | Significant improvement in physical composite score was higher in surgical aortic valve replacement vs. TAVI while improvement in mental composite score was higher in TAVI vs. surgical aortic valve replacement. |
| Eichler, 2017 2 | N = 136 TAVI Age 80.6 Female 52.5% CR–17.7 ± 9.9 d. |
5d/w Aerobic training: 30 min the continuous/interval pts (> 1.0 W/kg) Resistance training at 30–50% 1RM Additional training outdoor walking, gymnastics, aqua gymnastics and spinal gymnastics in groups. |
3 weeks CR inpatient |
SF–12 at admission (T0) and discharge (T1) | Significant improvement in physical and mental health. Higher cognition, nutrition and autonomy positively influenced the physical scale of SF–12. |
| Sibilitz, 2016 5 | N = 147 Intervention = 72 Control = 75 Age 62 Female 24% Valve surgery CR–1 month. |
Training group: 3/w Supervised training (69%) or home-based training (31%). Intensity according to RPE increasing up to 12 w. The strength exercises for lower body. Control group: advised not to exercise |
12 weeks CR outpatient/home based |
SF–36, HeartQuality of life at admission (T0) FU period 6 months (T1) |
No interaction between intervention and time was observed for SF–36 at 6 months and the self–reported outcomes (HeartQuality of life). |
Abbrevations: CR cardiac rehabilitation, RPE – rate of perceived exertion, w – weeks, d – days, 1 RM – 1 repetition maximum, TAVI – transcateher aortic valve implantation, AF– atrial fibrillation, FU–follow up, KCCQ–Kansas City CardiacQuestionaire, SAVR–surgical aortic valve repair, TG–training group, UC–usual care.
Zanettini R, Gatto G, Mori I, et al. Cardiac rehabilitation and mid-term follow-up after transcatheter aortic valve implantation. J Geriatr Cardiol. 2014 Dec; 11: 279–285.
Eichler S, Salzwedel A, Reibis R, et al. Multicomponent cardiac rehabilitation in patients after transcatheter aortic valve implantation: Predictors of functional and psychocognitive recovery. Eur J Prev Cardiol. 2017; 24: 257–264.
Hummel J, Pressler A, Fo L, et al. Long-term effect of exercise training in patients after transcatheter aortic valve implantation : Follow-up of the SPORT : TAVI randomised pilot study. 2018.
Pressler A, Christle JW, Lechner B, et al. Exercise training improves exercise capacity and quality of life after transcatheter aortic valve implantation: A randomized pilot trial. Am Heart J [Internet]. 2016 Dec;182: 44–53. Available from: http://www.elsevier.com/inca/publications/store/6/2/3/2/7/2/index.htt%5Cnhttp://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed18b&NEWS=N&AN=612333993.
Imran HM, Baig M, Mujib M, et al. Comparison of phase 2 cardiac rehabilitation outcomes between patients after transcatheter versus surgical aortic valve replacement. Eur J Prev Cardiol. 2018 Oct; 25: 1577–1584.
Sibilitz KL, Berg SK, Rasmussen TB, et al. Cardiac rehabilitation increases physical capacity but not mental health after heart valve surgery: a randomised clinical trial. Heart [Internet]. 2016 Dec 15; 102: 1995–2003. Available from: http://heart.bmj.com/lookup/doi/10.1136/heartjnl-2016-30941.
Appendix 2. Standardized questions used for examination 3 months after completion of rehabilitation (T2) to assess clinical course and physical activity level.
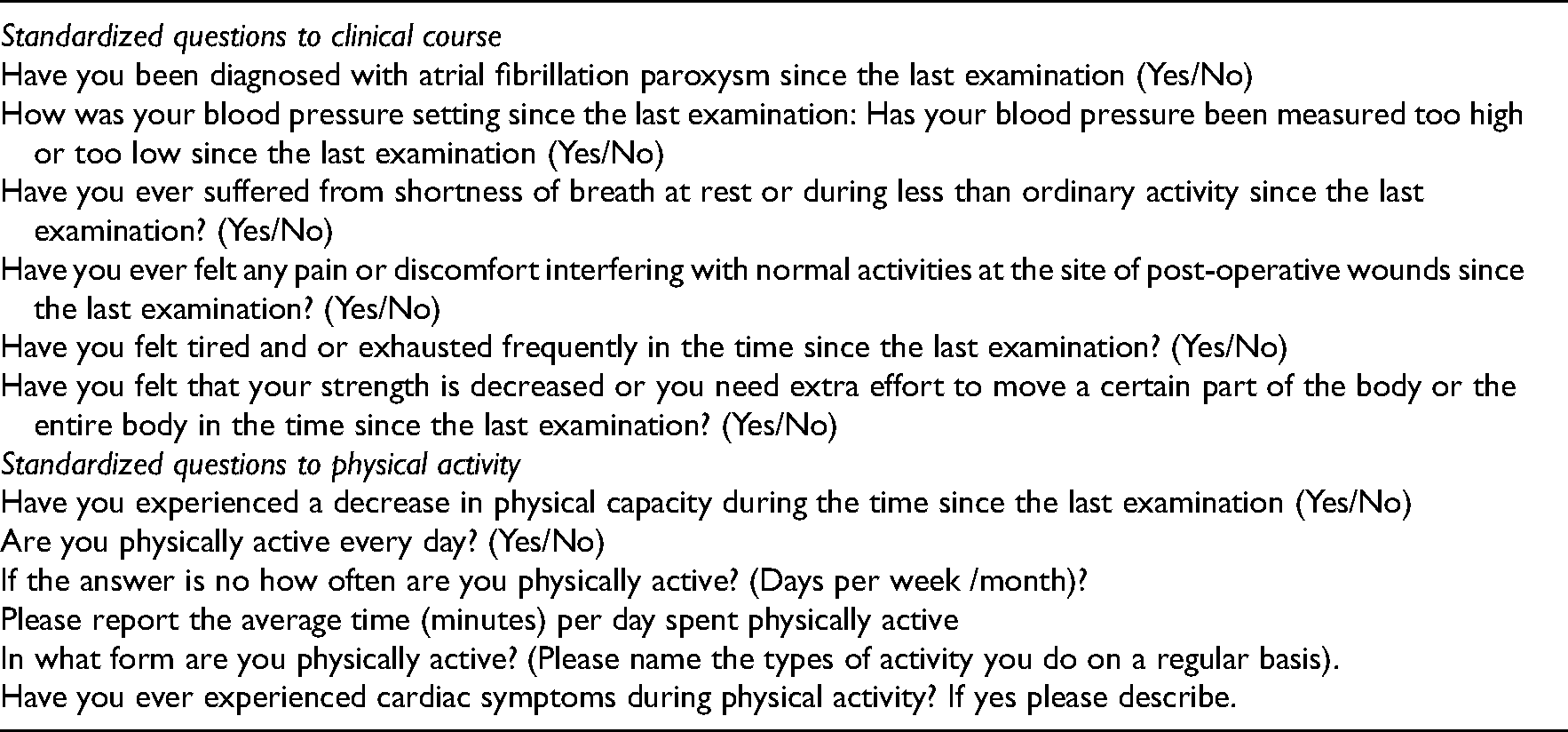
| Standardized questions to clinical course |
| Have you been diagnosed with atrial fibrillation paroxysm since the last examination (Yes/No) |
| How was your blood pressure setting since the last examination: Has your blood pressure been measured too high or too low since the last examination (Yes/No) |
| Have you ever suffered from shortness of breath at rest or during less than ordinary activity since the last examination? (Yes/No) |
| Have you ever felt any pain or discomfort interfering with normal activities at the site of post-operative wounds since the last examination? (Yes/No) |
| Have you felt tired and or exhausted frequently in the time since the last examination? (Yes/No) |
| Have you felt that your strength is decreased or you need extra effort to move a certain part of the body or the entire body in the time since the last examination? (Yes/No) |
| Standardized questions to physical activity |
| Have you experienced a decrease in physical capacity during the time since the last examination (Yes/No) |
| Are you physically active every day? (Yes/No) |
| If the answer is no how often are you physically active? (Days per week /month)? |
| Please report the average time (minutes) per day spent physically active |
| In what form are you physically active? (Please name the types of activity you do on a regular basis). |
| Have you ever experienced cardiac symptoms during physical activity? If yes please describe. |
Appendix 3. Exercise training program for both usual care (control group) and intervention group.
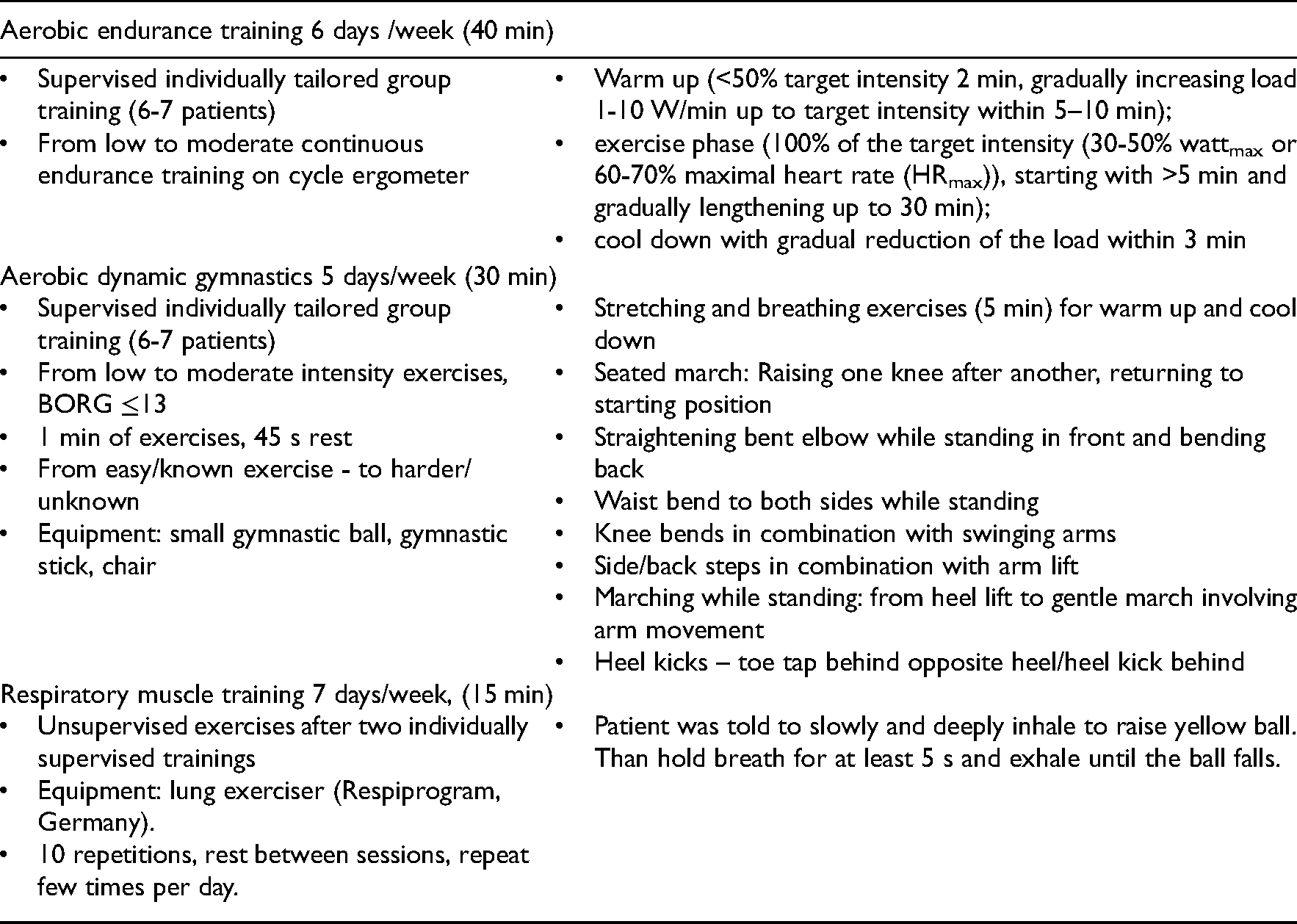
| Aerobic endurance training 6 days /week (40 min) | |
|---|---|
|
Supervised individually tailored group training (6-7 patients) From low to moderate continuous endurance training on cycle ergometer |
Warm up (<50% target intensity 2 min, gradually increasing load 1-10 W/min up to target intensity within 5–10 min); exercise phase (100% of the target intensity (30-50% wattmax or 60-70% maximal heart rate (HRmax)), starting with >5 min and gradually lengthening up to 30 min); cool down with gradual reduction of the load within 3 min |
| Aerobic dynamic gymnastics 5 days/week (30 min) | |
|
Supervised individually tailored group training (6-7 patients) From low to moderate intensity exercises, BORG ≤13 1 min of exercises, 45 s rest From easy/known exercise - to harder/unknown Equipment: small gymnastic ball, gymnastic stick, chair |
Stretching and breathing exercises (5 min) for warm up and cool down Seated march: Raising one knee after another, returning to starting position Straightening bent elbow while standing in front and bending back Waist bend to both sides while standing Knee bends in combination with swinging arms Side/back steps in combination with arm lift Marching while standing: from heel lift to gentle march involving arm movement Heel kicks – toe tap behind opposite heel/heel kick behind |
| Respiratory muscle training 7 days/week, (15 min) | |
|
Unsupervised exercises after two individually supervised trainings Equipment: lung exerciser (Respiprogram, Germany). 10 repetitions, rest between sessions, repeat few times per day. |
Patient was told to slowly and deeply inhale to raise yellow ball. Than hold breath for at least 5 s and exhale until the ball falls. |
Appendix 4. Additional resistance and balance training sessions 3 times/week. Supervised individually tailored small group training (3 patients).
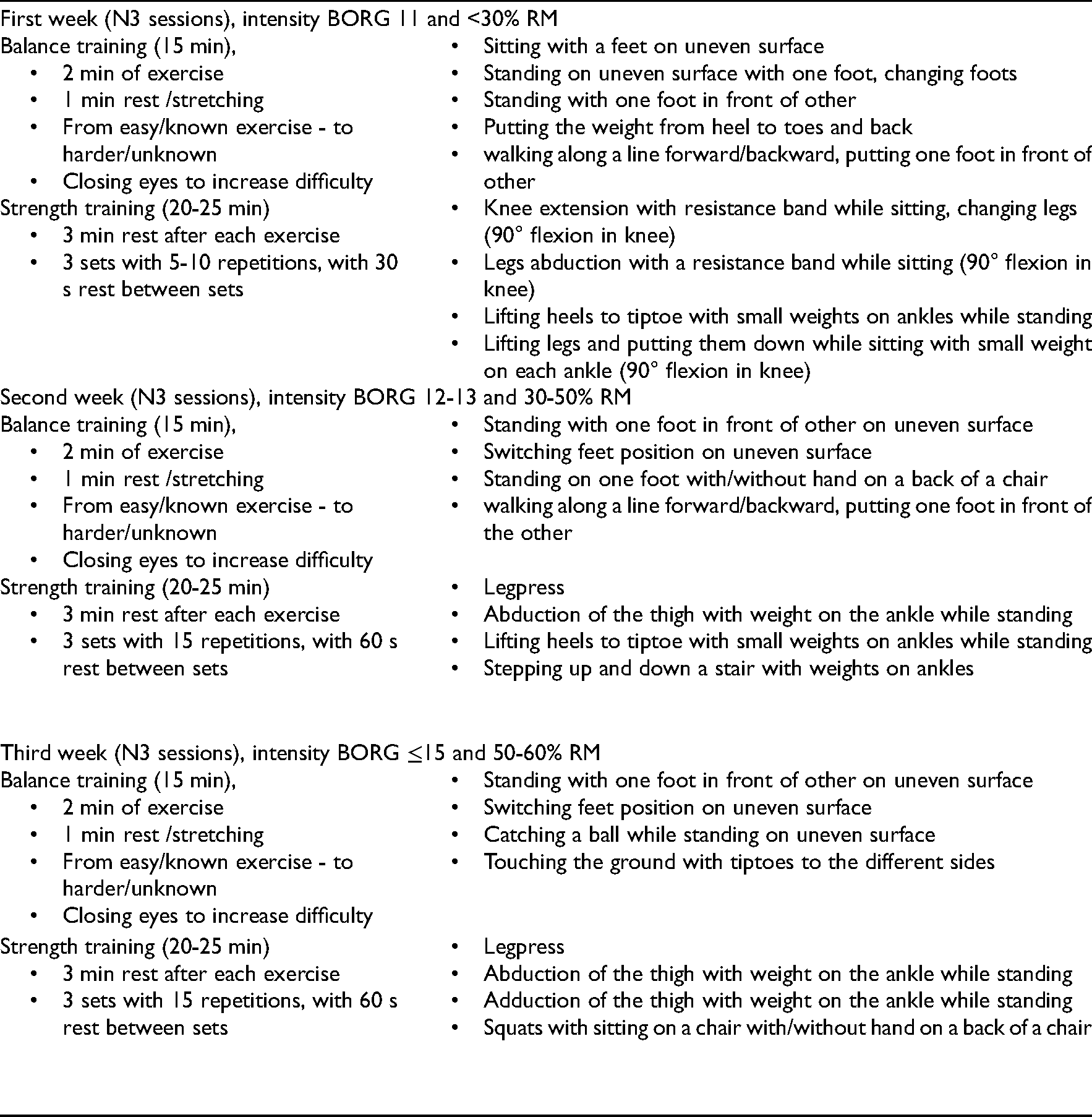
| First week (N3 sessions), intensity BORG 11 and <30% RM | |
| Balance training (15 min),
2 min of exercise 1 min rest /stretching From easy/known exercise - to harder/unknown Closing eyes to increase difficulty |
Sitting with a feet on uneven surface Standing on uneven surface with one foot, changing foots Standing with one foot in front of other Putting the weight from heel to toes and back walking along a line forward/backward, putting one foot in front of other |
| Strength training (20-25 min)
3 min rest after each exercise 3 sets with 5-10 repetitions, with 30 s rest between sets |
Knee extension with resistance band while sitting, changing legs (90° flexion in knee) Legs abduction with a resistance band while sitting (90° flexion in knee) Lifting heels to tiptoe with small weights on ankles while standing Lifting legs and putting them down while sitting with small weight on each ankle (90° flexion in knee) |
| Second week (N3 sessions), intensity BORG 12-13 and 30-50% RM | |
| Balance training (15 min),
2 min of exercise 1 min rest /stretching From easy/known exercise - to harder/unknown Closing eyes to increase difficulty |
Standing with one foot in front of other on uneven surface Switching feet position on uneven surface Standing on one foot with/without hand on a back of a chair walking along a line forward/backward, putting one foot in front of the other |
| Strength training (20-25 min)
3 min rest after each exercise 3 sets with 15 repetitions, with 60 s rest between sets |
Legpress Abduction of the thigh with weight on the ankle while standing Lifting heels to tiptoe with small weights on ankles while standing Stepping up and down a stair with weights on ankles |
| Third week (N3 sessions), intensity BORG ≤15 and 50-60% RM | |
| Balance training (15 min),
2 min of exercise 1 min rest /stretching From easy/known exercise - to harder/unknown Closing eyes to increase difficulty |
Standing with one foot in front of other on uneven surface Switching feet position on uneven surface Catching a ball while standing on uneven surface Touching the ground with tiptoes to the different sides |
| Strength training (20-25 min)
3 min rest after each exercise 3 sets with 15 repetitions, with 60 s rest between sets |
Legpress Abduction of the thigh with weight on the ankle while standing Adduction of the thigh with weight on the ankle while standing Squats with sitting on a chair with/without hand on a back of a chair |