
Abstract
Objective:
This study aims to further validate the Hessisch Oldendorf Risk of Falling Scale (HOSS) for neurological rehabilitation patients.
Design:
The overall scale performance and fall rate was calculated in a retrospective data analysis.
Setting:
The study was performed in a subacute care facility during inpatient neurological rehabilitation.
Subjects:
The study population (n = 512) included neurological and neurosurgical patients with heterogeneous levels of disability.
Main measures:
The HOSS total score and the suspected risk of falling were compared with the number of falls. Characteristics of fallers and non-fallers were compared using non-parametric group comparisons. Overall scale performance was assessed by calculating the area under the receiver operating characteristic curve of the HOSS as well as by calculating the sensitivity and specificity.
Results:
A total of 82 (16%) patients experienced at least one fall. Fallers were characterized by an older age, a longer length of stay, a more severe impairment in the activities of daily living upon admission, a hemiparesis, an orientation disorder, a need of a walking aid device and an urinary incontinence. The number of falls was associated with the HOSS total score. Sixty-four fallers and two hundred seventy-four non-fallers were correctly categorized leading to a sensitivity of 78.0% and a specificity of 63.7%. The area under the receiver operating characteristic curve of the HOSS was 0.778 ± 0.25 (CI = 0.729–0.828, P < 0.001).
Conclusion:
The scale performance of the HOSS showed a good sensitivity and an adequate specificity to identify neurological patients who are at high risk of falling during inpatient rehabilitation.
Keywords
Introduction
Falls are one of the most frequent complications during inpatient hospitalization and are more frequent among patients with neurological disorders during rehabilitation. 1 Summarizing seven studies with neurological patients during inpatient rehabilitation, a median of 16.3% sustained at least one fall.2–8 To prevent falls it is crucial to identify patients at high risk of falling. Although several fall risk assessments or screening tools are available to identify potential fallers in different settings only a few of them have been specially developed for neurological patients during inpatient rehabilitation. Both, the “Marianjoy-Falls-Risk-Assessment-Tool” and the “Casa-Colina-Fall-Risk-Assessment-Scale” were designed for rehabilitation patients (across all indications), but have not been validated for neurological rehabilitation patients, yet. The “Stroke-Assessment-Tool-of-Fall-Risk” was developed in 2014 in particular for stroke patient, but is a time-consuming tool that requires input from an interdisciplinary team of nurses, physicians and therapists, resulting in limited feasibility. The “Berg Balance Scale” and the “Timed Up and Go” test are frequently used to estimate a patient’s fall risk by evaluating the walking ability and balance of a patient. However, among severely impaired neurological patients, the feasibility of those tests is limited due to serious balance and gait disturbances resulting in an overestimation of the risk of falling.
The “Hessisch Oldendorf Risk of Falling Scale” (HOSS, “Hessisch Oldendorfer Sturzrisiko Skala”) has been specially designed for neurological patients undergoing inpatient rehabilitation, 9 based on an evaluation of fall protocols of this patient group. It is an easy-to-use 11-item scale, which can be assessed by nurses on the day of admission. The aim of this study was the evaluation of the predictive validity of the HOSS to predict falls for neurological patients during inpatient rehabilitation.
Methods
The study was conducted as a retrospective cohort study at a large specialized subacute care facility for inpatient rehabilitation of neurological patients in Germany. A retrospective study design was chosen to avoid any influence on the behavior of the clinical staff and on the fall incidence. All patients admitted between 1st June 2018 and 30th November 2018 with a length of stay beyond seven days and a written informed consent agreeing to use clinical routine data for scientific evaluation were included. Patients who were immobilized during the observation period, had a preceding stay in the facility or an outpatient rehabilitation were not included in the study population. The observation period for each patient was defined as the length of stay until the first interruption. For example, if a patient had to be transferred to an acute hospital and was not re-transferred on the same day, the observation period was terminated and later stays were not included into data evaluation.
Falls, defined as an event leading to involuntary contact to the ground, floor or other lower level 10 and the corresponding fall protocols were taken from the medical records and were counted for each patient. Fall protocols were written immediately after the fall and include information about the context of the fall (place, time, description of the fall, cause), patient’s characteristics (age, use of walking aid, medication, continence), injuries and interventions needed for the prevention of subsequent falls.
The HOSS is an 11-item scale (Table 1) with a total score ranging from 1 to 22 points. The total score is classified into four risk groups (low risk (1–5 points), medium risk (6–10 points), high risk (11–15 points), and very high risk (16–22 points)). 9 For verification of the scale performance a dichotomous classification was used, whereby a score of more than 10 points indicates a high risk of falling.
Hessisch oldendorf risk of falling scale.
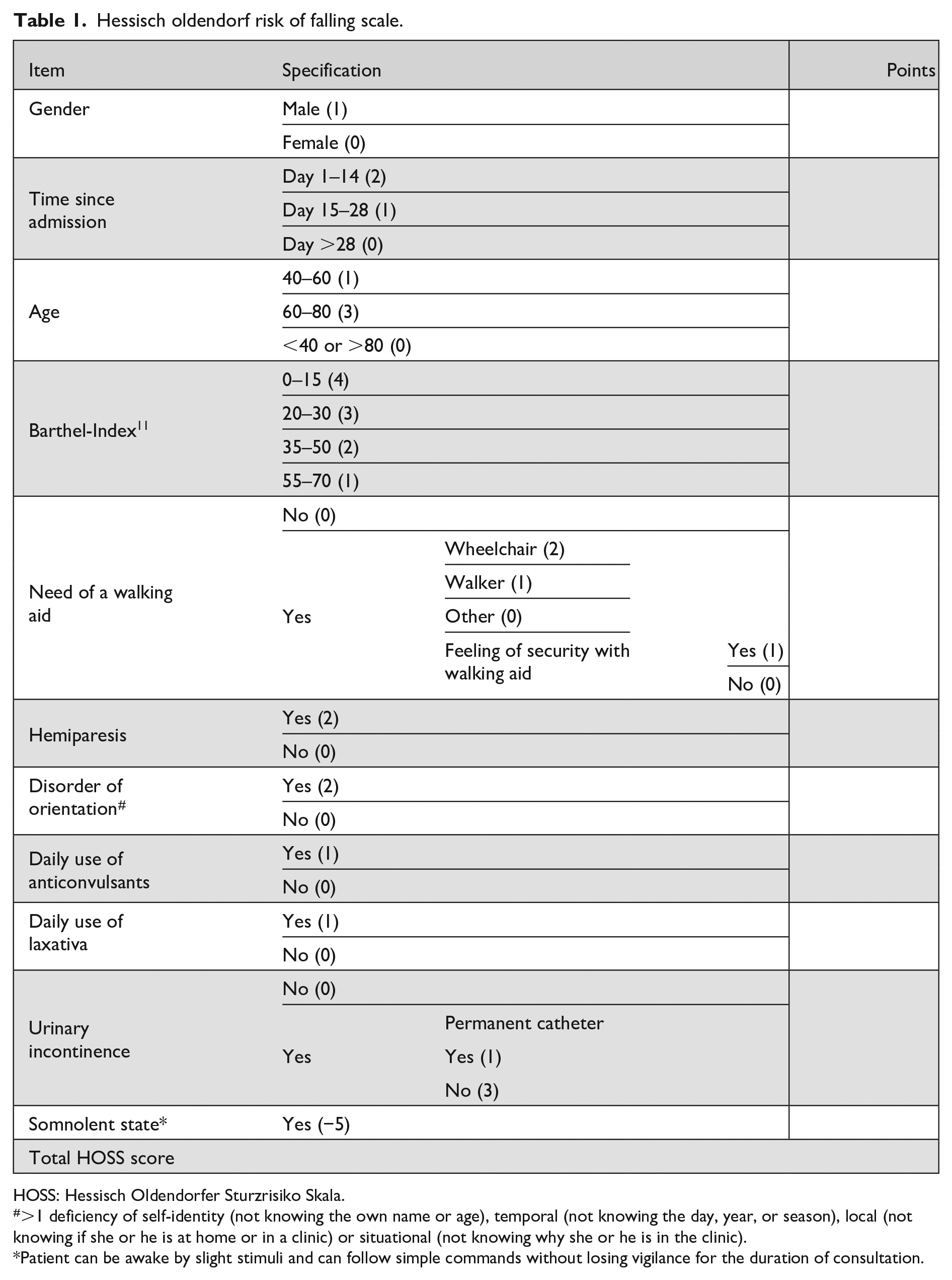
HOSS: Hessisch Oldendorfer Sturzrisiko Skala.
>1 deficiency of self-identity (not knowing the own name or age), temporal (not knowing the day, year, or season), local (not knowing if she or he is at home or in a clinic) or situational (not knowing why she or he is in the clinic).
Patient can be awake by slight stimuli and can follow simple commands without losing vigilance for the duration of consultation.
The risk of falling upon admission was assessed by the HOSS for each patient retrospectively using saved data from the internal clinical information system. All data were routinely collected during the patient stay and analyzed retrospectively.
Statistics
The SPSS software package was used for statistical analyses. Since most of the data was not normally distributed, non-parametric statistical methods were used. A two-tailed P-value <0.05 was considered to be significant.
The fall rate per person/year was calculated by the number of falls divided by the length of stay multiplied by 365 days (one year) for each patient. In addition, the absolute risk to fall depending on the HOSS total score was calculated by the number of falls divided by the number of patients. To determine the relationship between the number of falls and the HOSS total score a correlation analysis by Spearman was performed. Group comparisons between fallers and non-fallers were performed with χ2-test (categorical data) or Mann–Whitney-U Test (numeric data).
A cross-table was generated by entering patients classified at risk (yes/no) according to the HOSS total score with a cutoff of 10 points. To identify the predictive validity of the HOSS, sensitivity, specificity, predictive values, diagnostic odds ratio, and accuracy of the HOSS were calculated. Furthermore, the overall diagnostic accuracy of the HOSS was assessed using the Hosmer–Lemeshow goodness of fit test and the area under the receiver operating characteristic (ROC) curve.
To determine the effect of each HOSS item and to control the prediction model of the HOSS, all HOSS items were entered in a binary logistic regression model (fallers vs non-fallers) using the block-wise inclusion method. For the model, the odds ratios with the associated confidence intervals and the explained total variance (Nagelkerkes R2) are reported.
Results
In total, 512 neurological patients (321 men (63%), 191 women (37%)) with a median age of 64 years (IQR = 53–78 years) were included in the study. Strokes (ischemic (n = 211, 41%), hemorrhagic (n = 74, 14%)) and traumatic brain injuries (n = 78, 15%) were the most frequent diagnoses. Eighty-two patients (16%) sustained one (n = 52) or more than one fall (n = 30). The first fall occurred after a median length of stay of 26 days (IQR = 10–40 days). The mean fall rate per patient/year was 2.05.
Fall protocols
In total, 151 fall protocols were analyzed from 82 patients of the study population. Detailed information on the falls is presented in Supplemental Material 1. Most falls occurred in the patient room (n = 102, 68%), between 5 and 7 pm (n = 26, 17%) and when the patient tried to stand up without assistance (n = 93, 62%). All falls occurred on normal wards, no patients on intermediate care or intensive care units fell.
The most frequent causes to explain the falls were urge to go to the toilet (n = 21, 14%), motor agitation and/or disorientation (n = 19, 13%), disturbance of balance (n = 16, 11%), incorrect use of the walking aid (n = 15, 10%), lack of body stability due to hemiparesis and/or missing trunk control (n = 13, 9%), wrong self-confidence (n = 10, 7%), and gait disorders (e.g. weakness of the foot extensors) (n = 8, 5%). Less frequent reasons were strength deficits (n = 5, 3%), environmental factors (n = 4, 3%) such as slippery floor, technical malfunction/employee deviance (n = 3, 2%), and inattention (n = 2, 1%).
The time until the fall was noticed by the staff was mostly shorter than five minutes (n = 82, 54%). Most of the fallers were found in a supine position (n = 92, 61%) and needed assistance to get up (n = 135, 89%). Most fallers were either not oriented in any field (n = 43, 28%) or fully oriented (biographically, temporally, situationally, spatially) (n = 45, 29%). Most frequently, patients were biographically oriented (n = 94, 62%), followed by spatially (n = 73, 48%), situationally (n = 61, 40%) and temporally (n = 55, 36%).
Most fallers showed no visible injuries (n = 87, 57%) and the most frequent immediate intervention after the fall was a check of the vital signs (n = 32, 21%).
Comparison between fallers and non-fallers
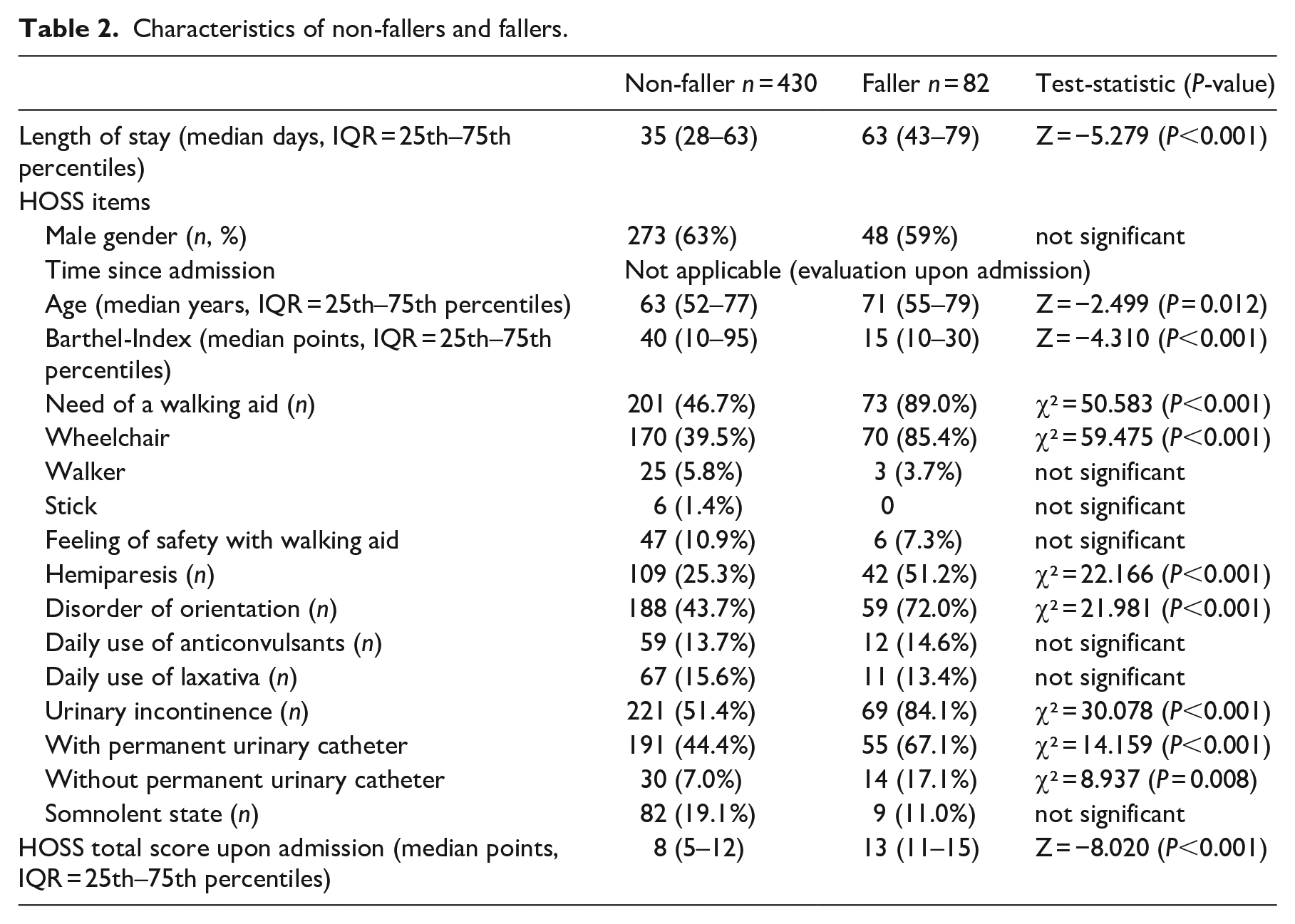
There were no differences between fallers and non-fallers with respect to gender and diagnosis. However, fallers were significantly older than non-fallers, had more often a hemiparesis, an orientation disorder, a need of a walking aid device and an urinary incontinence than non-fallers (Table 2). Furthermore, fallers had a significantly lower Barthel-Index and a higher HOSS total score upon admission as well as a longer length of stay than non-fallers (Table 2). At the end of rehabilitation, fallers were more frequently discharged to long-term care facilities than non-fallers (χ2 = 11.915, P = 0.001).
Characteristics of non-fallers and fallers.
Diagnostic accuracy of the HOSS
The number of falls was associated with the HOSS total score (r = 0.360, P < 0.001; Figure 1). In addition, the absolute risk to fall showed a nearly linear relationship with the HOSS total score from 2 to 17 points, followed by a decrease of risk with very high (>17 points) HOSS total scores (Figure 2).
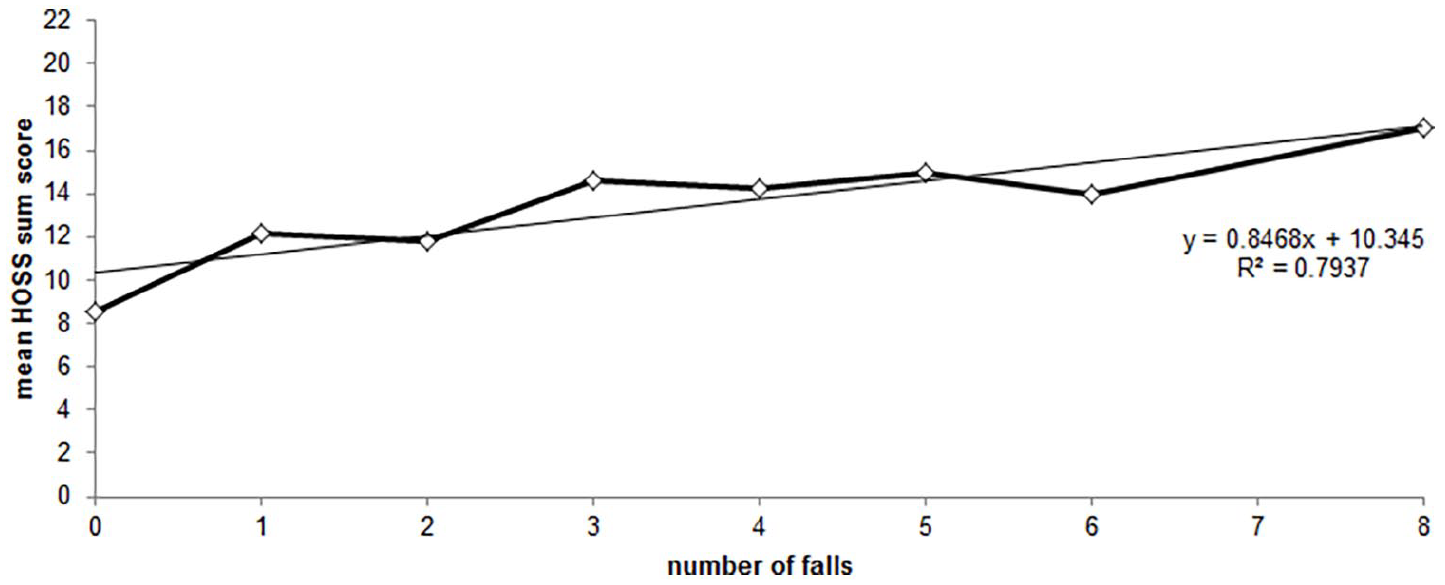
Association between the number of falls and the HOSS total score.
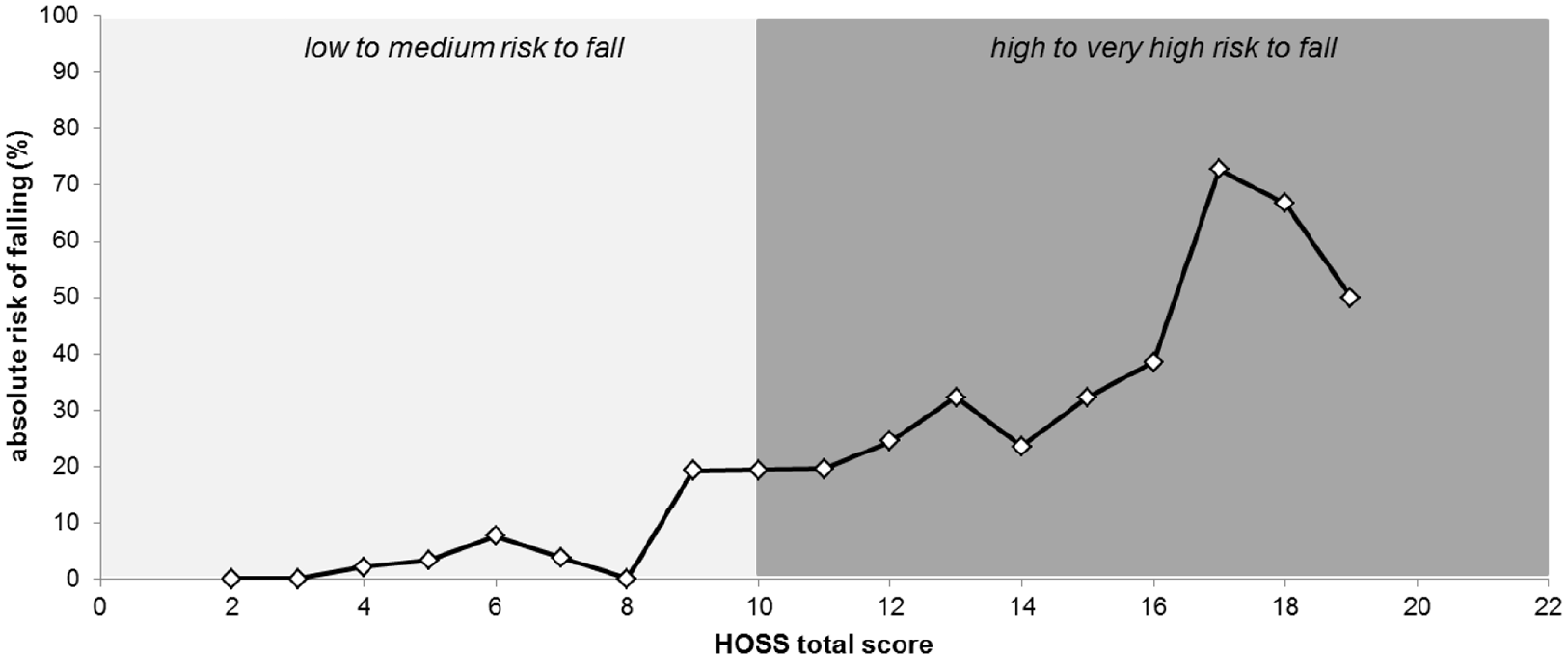
Relationship between the HOSS total score and the absolute risk of falling in neurological patients during inpatient rehabilitation.
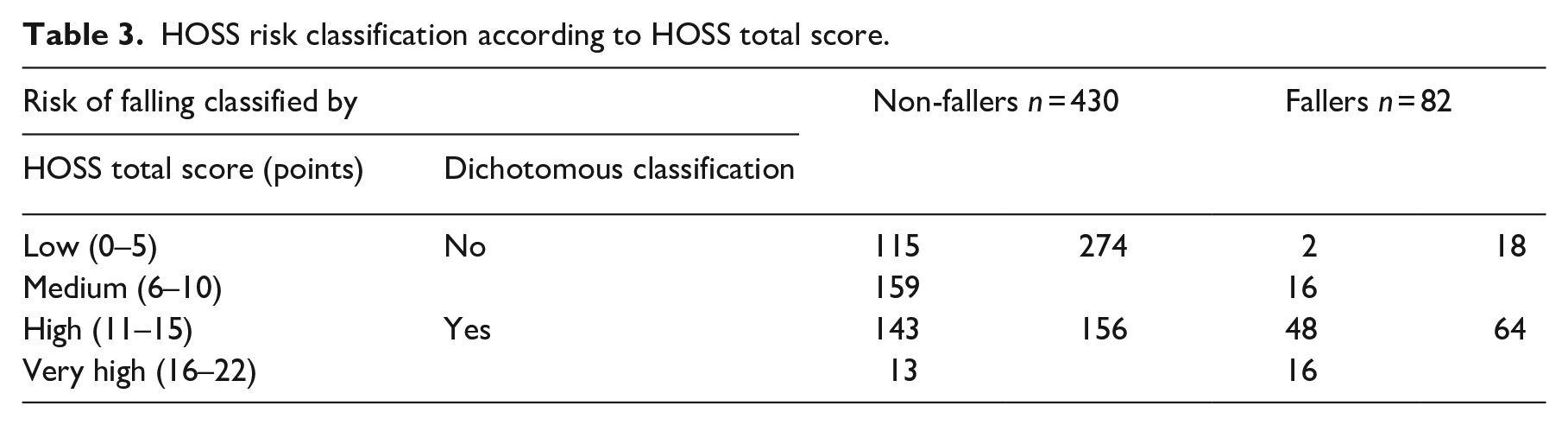
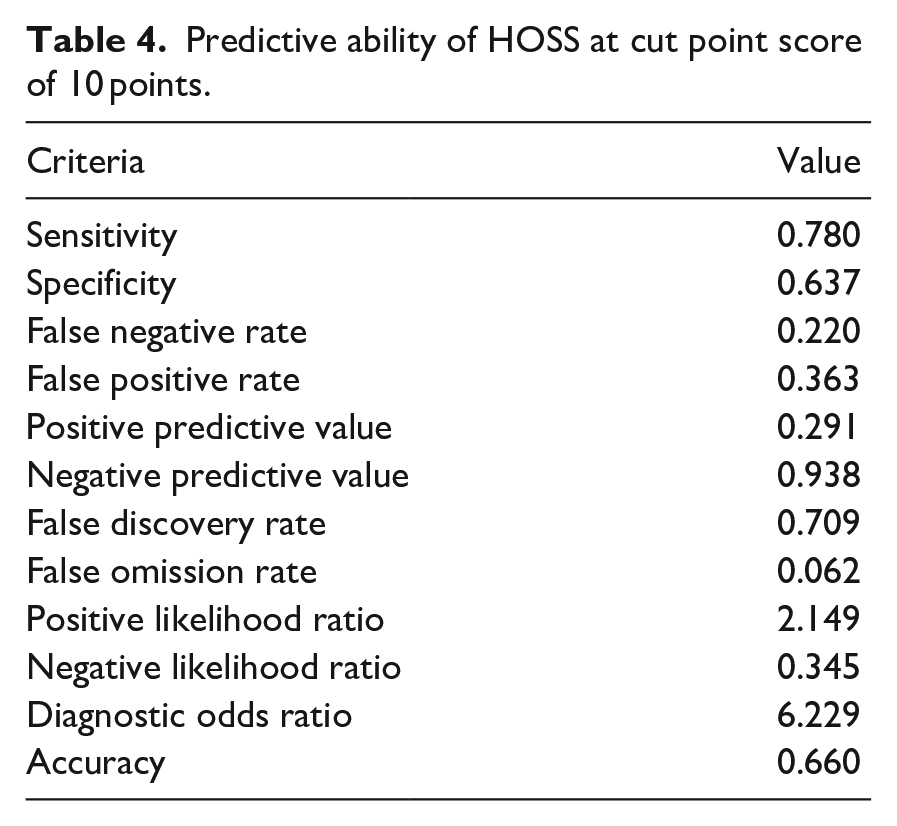
According to the classification of the HOSS, 117 patients (23%) had a low, 175 patients (34%) a medium, 191 patients (37%) a high, and 29 patients (6%) a very high fall risk (Table 3). Based on the dichotomous classification, 64 fallers and 274 non-fallers were correctly categorized by the HOSS, leading to a sensitivity of 78.0% and a specificity of 63.7% (Table 4). The ROC curve is displayed in Figure 3. The area under the curve was 0.778 ± 0.25 (CI = 0.729–0.828, P < 0.001), indicating a good predictive power of the scale.
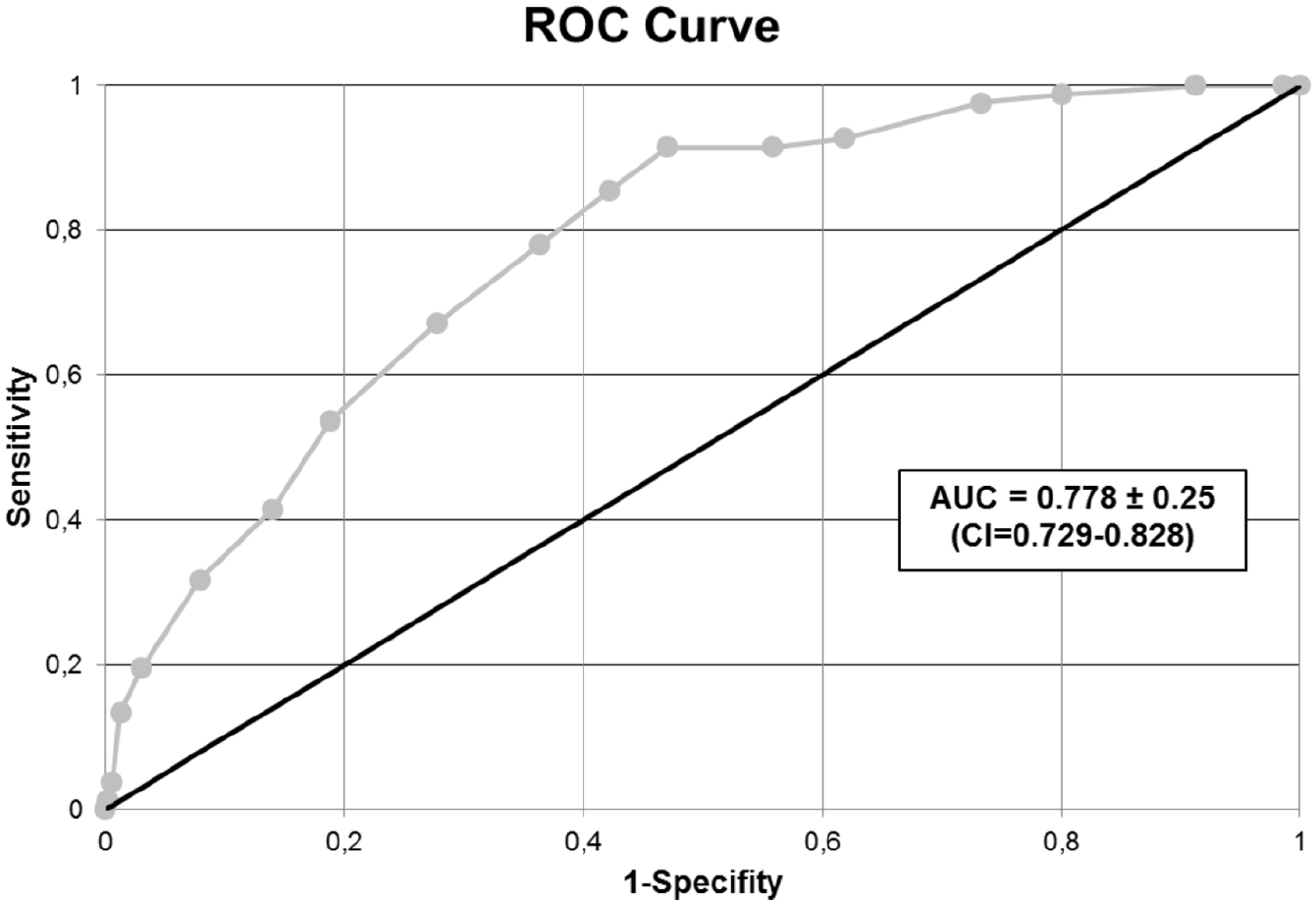
ROC curve of the HOSS total score predicting falls during inpatient neurological rehabilitation.
HOSS risk classification according to HOSS total score.
Predictive ability of HOSS at cut point score of 10 points.
The HOSS items were entered in a binary logistic regression model (χ2 (16) = 109.060, P < 0.001, n = 512). The Nagelkerkes R2 was 0.328 resulting in Cohen’s f2 of 0.488, which corresponds to a strong effect. 12 Goodness-of-fit was assessed using the Hosmer–Lemeshow-Test, indicating a good model fit (χ2 (8) = 9.554, P = 0.298, n = 512). Results of the regression analysis showed, that a non-somnolent state (OR = 4.025, CI = 1.748–9.270, P = 0.001), the need of a walking aid (OR = 5.647, CI = 2.405–13.260, P < 0.001), a hemiparesis (OR = 2.160, CI = 1.238–3.767, P = 0.07), an intake of laxatives (OR = 0.459, CI = 0.213–0.990, P = 0.047) and an orientation disorder (OR = 2.963, CI = 1.493–5.879, P = 0.002) are significant factors increasing the risk of falling in neurological patients during inpatient rehabilitation.
Discussion
A non-somnolent state, a need of a walking aid, a hemiparesis and/or an orientation disorder were significant factors that increased the risk of falling in neurological patients during inpatient rehabilitation. In addition, fallers were older, had more often an urinary incontinence and showed a lower Barthel-Index (higher dependence in the activities of daily living) upon admission, a longer length of stay and were more frequently transferred to long-term care facilities than non-fallers.
To the best of our knowledge, the impact of a somnolent state on the risk of falling was not investigated so far. However, an association of a non-somnolent state with a higher risk of falling is obvious, because a somnolent state is a condition characterized by a slight to moderate reduced vigilance and consciousness. Somnolent patients are often sleepy and show reduced motor activity, which might reduce the risk of falling.
A disorder of orientation was significantly associated with a higher risk of falling in this study. In agreement to this, a multicenter study revealed that a confusional state (defined as agitation, unrest, or disorientation) increased the risk of falling of stroke patients during acute hospitalization. 13 In another multicenter study with patients during geriatric rehabilitation, disoriented patients (assessed by nurses on the day of admission) had a higher risk of falling than oriented patients. 14 However, a “confusional state” detected in the first study lost significance in the multivariate model, 13 which resulted in conflicting result with our own observations. This might be caused by different settings, populations and procedures of orientation assessment.
Reduced motor function, sensory loss or impaired gait and balance are common after stroke or other neurological diseases and increase the risk of falling. Therefore, it was not surprising that a motor disability (characterized by hemiparesis and/or need of a walking aid) was identified as a risk factor in this study. This result is in agreement with Czernuszenko and Członkowska 2 who found that a left side hemiparesis resulted in an increased risk of falling in patients during inpatient neurological rehabilitation. However, Schmid et al. 8 found no effect of a hemiparesis on the risk of falling and another study investigated hemiplegia 4 instead of hemiparesis.
This study revealed that fallers were older than non-fallers, which is in disagreement with one study with stroke patients during inpatient rehabilitation. 6 However, another study reported that an age >65 years increase the risk for multiple falls. 2 Furthermore, a higher age in combination with a low Functional Independence Measure score increases the risk of falling, too. 1
Fallers showed more frequently an urinary incontinence than non-fallers in this study, which was also reported by another study with stroke patients during inpatient rehabilitation. 4 The differentiation between urinary incontinence with and without permanent catheters for the impact on fall incidence was not investigated elsewhere up to now. Previous investigations revealed that an urinary incontinence was associated with multiple falls. 9 In addition, a reduced number of multiple fallers were observed within the group of urinary incontinent patients were provided with permanent catheter compared to patients without permanent catheter. 9 Further studies should address urinary incontinency and catheterization in more detail to clarify this relationship.
Fallers showed a lower Barthel-Index, which means that patients have a higher dependence in the activities of daily living upon admission. This was also reported by other studies with neurological patients during inpatient rehabilitation.2,4 In addition, one study showed that a Barthel-Index between 6 and 14 points (moderate to severe impairment) was associated with a higher risk of falling than a Barthel-Index ⩽5 points (severe impairment). 4 A patient with a Barthel-Index ⩽5 points is bedridden, which results in a decreased risk of falling. The impact of a moderate level of disability on the risk of falling was observed in another study with neurological and orthopedic patients during inpatient rehabilitation, too. A moderate level of disability (Functional Independence Measure score between 38 and 72 points) was identified as an independent risk factor. 1
The observed higher length of stay of fallers compared to non-fallers in this study was also reported by other studies.2–4,6,7 In addition, Hanger et al. reported that fallers were less frequently discharged home than non-fallers. 6 This agrees indirectly with the observed higher number of fallers discharged to long-term care facilities than non-fallers in this study.
The risk of falling increased linearly with the HOSS total score in this study. However, Barker et al.15,16 detected a non-linear association between mobility impairments (measured by Physical Mobility Scale) and the risk of falling. A non-linear increase in the risk of falling is not surprising since falls are multifactorial and risk factors interact with each other resulting in in- or decreasing effects. The linear relationship between the risk of falling with the HOSS total score in this study is caused by the different weighting of each HOSS item (i.e. scoring from −5 for the item “somnolence” to +4 for the item “Barthel-Index of 0–15 points”). The different weighting of each HOSS item based on the effect of each item on the risk of multiple falls during rehabilitation. 9
Strengths and limitations
The study has some limitations which should be addressed. The study data was collected in a single center, thus the results could be different in other centers and settings. The HOSS itself has a methodological weakness due to the item “Barthel-Index” which translates the sum of the Barthel-Index of a patient into “risk points” of the HOSS. The Barthel-Index is a combination of 10 different items describing the independence of a patient in the activities of daily living (eating, transfers, personal hygiene, toilet use, bathing, standing up and walking, stairs, dressing, bowel control, bladder control). One Barthel-Index item (bladder control) is also scored with one HOSS item (urinary incontinency) resulting in double counting of this patient characteristic. In addition, the Barthel-Index item “standing up and walking” could be associated with one HOSS item “need of walking aid,” because a patient who is completely independent with its wheelchair is counted with 5 points although the patient cannot stand up and walk. It might be that an unknown number of falls without injuries have not been reported, if the patient who sustained the fall, was able to recover alone and did not report this to the clinical staff.
The HOSS was designed to perform subsequent assessments during rehabilitation even if the patient’s abilities change during rehabilitation resulting in changed patient characteristics and reduced/increased risk of falling. One example might be that a motor function of a patient improves during rehabilitation and the need of a walking aid transitioned from wheelchair to walker. For this study, only the admission assessment was used to determine the accuracy of the HOSS to predict falls. Performing re-assessments might result in better specificities and sensitivities of the HOSS.
To the best of our knowledge, the HOSS is the only assessment tool for neurological patients during inpatient rehabilitation, because the HOSS was designed for neurological patients with varying diagnoses (i.e. stroke, hemorrhages, hypoxic or traumatic brain injuries, neurodegenerative diseases). Although it could be used for all neurological patients in all inpatient settings, the diagnostic accuracy might be different if the HOSS is used for a diagnosis subgroup, which was also shown in a previous study of our working group. 17 However, this potential weakness is also a strength, because neurological rehabilitation patients with a varying degree of disability from severely impaired patients with mechanical ventilation and/or tracheal cannula on the intensive care unit or intermediate care unit, moderately impaired patients with still dependence in the activities of daily living as well as patients who are nearly independent in the activities of daily living and have just slight impairments could be assessed with the HOSS. In addition, it is an easy-to-use tool which can be assessed by nurses on the day of admission, which is a necessary feature for the applicability of an assessment tool.
Conclusion
Four key factors have been found to be particularly important for assessing the risk of falling in this study. These key factors are an orientation disorder, a motor disability (hemiparesis and/or need of a walking aid), an urinary incontinence and a non-somnolent state and should therefore be considered upon admission to estimate the risk of falling. In addition, the HOSS has a good predictive power among neurological rehabilitation patients and both, sensitivity and specificity are comparable to the results from a previous study. 17
The next steps for further studies might be (1) the investigation of the external validity of the HOSS in other centers with neurological patients during inpatient rehabilitation; (2) the verification of the scale performance when re-assessments are performed during the rehabilitation course; and (3) testing if the application of the HOSS results in reduced fall rates during rehabilitation.
Clinical messages
The HOSS shows a good overall scale performance for neurological rehabilitation patients.
An orientation disorder, a motor disability and an urinary incontinence of a neurological patient who is not in a somnolent state should be taken into account upon admission for estimating the risk of falling.
Supplemental Material
sj-pdf-1-cre-10.1177_02692155211034149 – Supplemental material for Evaluation of the predictive validity of the Hessisch Oldendorf Risk of Falling Scale (HOSS)
Supplemental material, sj-pdf-1-cre-10.1177_02692155211034149 for Evaluation of the predictive validity of the Hessisch Oldendorf Risk of Falling Scale (HOSS) by Simone B Schmidt, Melanie Boltzmann and Jens D Rollnik in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors thank Melanie Meyer, Sieke Wrede, Miriam Keilhaue and Zora Gornik for their help on collecting the study data.
Authors’ contributions
SBS collected the data, performed data analysis and interpretation, and wrote the paper. MB and JDR were involved in manuscript writing. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.