
Abstract
Objective:
In this paper, we aim to provide a comprehensive description of the multicomponent self-management intervention for adults with epilepsy, ZMILE.
Rationale or theory:
Acquiring self-management skills has been shown to play a vital role in enabling patients with epilepsy overcoming (health-related) struggles in daily life and coping with limitations their condition poses on them. ZMILE is a course consisting of education (to increase concordance to treatment), goal-setting (proactive coping), and self-monitoring.
Resources needed:
The course is guided by two nurse practitioners and each patient is allowed to bring one family member or friend. Self-monitoring plays an important role and can be done through e-Health tools or written diaries.
Processes involved:
During and after the course, patients are required to work toward a personally defined goal using a five-step approach by means of pro-active coping. Moreover, patients are expected to use self-monitoring tools to reflect on their own behavior and identify ways to optimize medication intake when required.
Quantification:
ZMILE is provided in an outpatient setting over five weekly group sessions and one booster session. From the start, patients are encouraged to set individual goals. Each group session will have a different theme but part of every session is reflecting on personal goals and to learn from eachother.
Conclusions:
The ZMILE-intervention has been evaluated and may be a promising intervention in terms of effectiveness and feasibility for adults with epilepsy, relatives, and professionals. We present the adapted version which can be implemented in clinical practice.
Introduction
The extent to which people with epilepsy are able to manage their condition plays a vital role in coping with the condition and overall quality of life. For example, antiepileptic drugs are prescribed as standard treatment for people with epilepsy but are only moderately effective in achieving and maintaining positive seizure control.1 –3 One of the reasons for poorly controlled epilepsy is shown to be poor concordance, which refers to the consensual agreement about taking antiepileptic drugs that has been established between patient and practitioner. 4 In addition, many people with epilepsy “seem to be unaware of missed drug intake.” 5
People living with chronic disorders such as epilepsy share challenges that include obtaining appropriate care, adhering to complex medication regimens, and making lifestyle adjustments while coping with symptoms, disabilities, and emotional impact. 6 Self-management programs are developed to support patients in coping with their chronic condition. 7 In fact, studies have shown that self-management programs are useful for individuals with chronic conditions such as asthma, heart disease, and diabetes.7–17 However, as poor epilepsy management cannot directly be linked to poor seizure control, these results cannot be generalized to people with epilepsy. Hence, there is a scarcity of evidence to prove the effectiveness of self-management programs for people with epilepsy. 6 Moreover, previously existing programs designed for epilepsy focused mainly on psycho-education (i.e. educating patients about their condition).
We therefore developed and evaluated the multicomponent self-management intervention for adults with epilepsy, ZMILE. In the randomized controlled trial, we compared ZMILE to the standard treatment for the evaluation of its clinical- and cost-effectiveness.18,19 After completion of the randomized controlled trial, a process evaluation was performed and minor changes were made to the intervention. 20
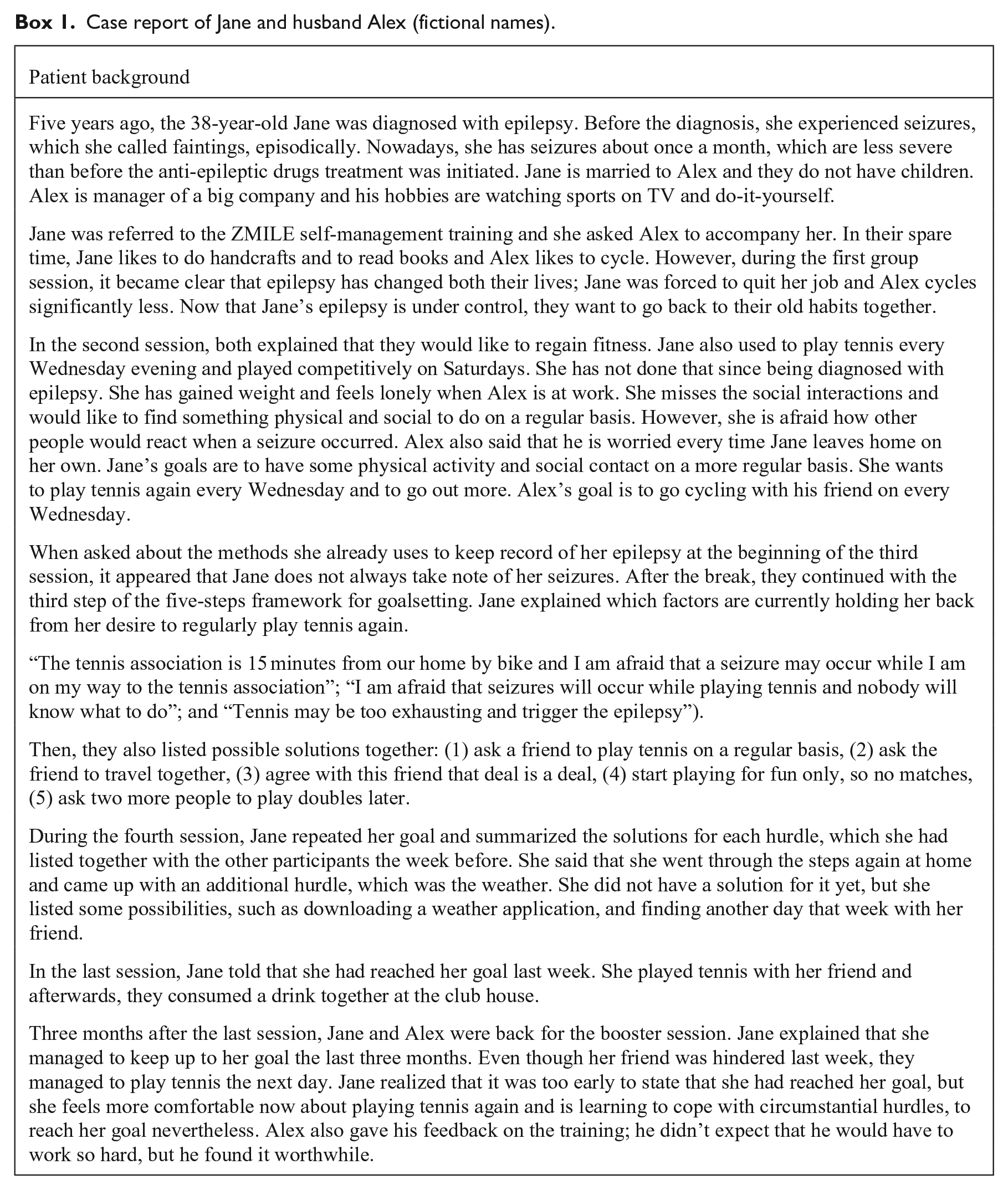
One of the main changes concerns the use of e-health tools which was an important element of our multicomponent intervention. The specifically selected tools are, however, no longer available. Here we present a description, rationale, and justification of the final version which is currently being implemented in Dutch health care using the template for intervention description and replication (TIDieR) checklist and guide (Hoffmann et al. 21 see Supplementary Appendix 1). To illustrate ZMILE, an example case will be used throughout the paper (see Box 1).
Case report of Jane and husband Alex (fictional names).
ZMILE: Multicomponent self-management training with e-health intervention
Rationale
It has long been thought that only people with uncontrolled seizures experience physical, cognitive, and psychosocial burden. 22 Although this indeed plays a role, experience has shown that also people with lower seizure frequency are in need for more control over their life with epilepsy. For example, even with adequate seizure control, patients are expected to adhere to complex medication regimens and cope with symptoms, disabilities, and the emotional impact (e.g. not knowing if and whether a seizure will occur).
Acquiring self-management skills has been shown to play a vital role in enabling patients with epilepsy to overcome (health-related) struggles in daily life and coping with the limitations their condition poses on them. Not surprisingly, self-management is an essential component of the Chronic Care Model (CCM) which is a well-founded leading model describing how improved functional and clinical outcomes for disease management are the result of productive interactions between informed, activated patients, and the prepared, proactive practice team of clinicians and healthcare professionals.23,24
ZMILE aims to provide patients with information, skills, and tools to improve self-management and limit daily struggles. The ZMILE-intervention is designed to essentially provide education to both patients with epilepsy and people close to them.
The first goal of this intervention is to assist patients in acquiring self-management skills which enable them to overcome health-related struggles in daily life (e.g. goal setting and proactive coping). 25 Hence self-management education is aimed to teach problem-solving skills for both the patients as well as her/his relative. 26 This may help to create or enhance supportive environments together with people close to the patient as social supports has been demonstrated to have a positive impact on overall health and quality of life. 23
The second goal of the ZMILE-intervention is to enhance self-efficacy, which is the confidence in one’s own capacity to execute tasks. 7 Many studies have emphasized the importance of increasing self-efficacy as one of the key component to increase patient’s quality of life in self-management programs.7,14,26–29 One systematic review also stated that effective ways of helping people to follow medical treatment could have larger effect than any treatment itself. 30
The last goal of the ZMILE-intervention is to improve patient’s self-monitoring skills by providing knowledge on selecting appropriate e-Health tools as reminder for medication intake. Study has shown that many patients with epilepsy appear to be unaware of missed doses, resulting in non-adherence and therefore potential need for e-Health tools to remind patients of medication intake. 5 Overall, ZMILE aims to engage patients and people close to them in their own care by connecting them in meaningful ways to their own health and care pathway in an effort to improve health outcomes.
Participants and mode of delivery
ZMILE is provided in five consecutive weekly group sessions of two hours each, with a booster session at three months after the fifth session. It is designed for people aged 18 years or over who have been diagnosed with epilepsy and are being treated with anti-epileptic drugs. The group capacity is 6–12 participants, with a maximum of six people with epilepsy as each one of them is allowed to bring one family member or friend.
The training takes place in the evening hours as most people work during daytime, therefore, evening sessions may increase the possibility for family members and friends to participate. In addition, travelling is often a hurdle for people with epilepsy, so if the family member or friend is available, it would be less of a limiting factor for patients to participate. Finally, the availability of group rooms and nurse practitioners is also better during the evening. The use of e-health tools to improve self-monitoring and thereby concordance were an important element of the original treatment protocol, but are no longer available (see paragraph on modification).
Providers and location
ZMILE is designed for the outpatient setting and every session is guided by two nurse practitioners, who have successfully completed two trainings for motivational interviewing techniques and for the ZMILE-intervention. Additional qualities of the nurse practitioners are experience with epilepsy care and in leading group meetings, competence to act as a coach, able to relate experiences among participants, capable of problem-oriented and resolving-oriented framework thinking.
Materials
A detailed protocol and Powerpoint presentation are provided to the nurse practitioners as supporting material. At the beginning of the first session, each participant will receive a comprehensive workbook with all information, instruction, steps, and core messages of the entire training. All course materials, promotional materials, and ZMILE-related publications are available for download from the ZMILE-web page in Dutch (https://vhc.mumc.maastrichtuniversity.nl/zmile). Moreover, it is advised to provide assistance in selecting self-management tools for each patient. This may be done using e-Health smartphone applications (see below), but can also be done using written diaries.
Procedures
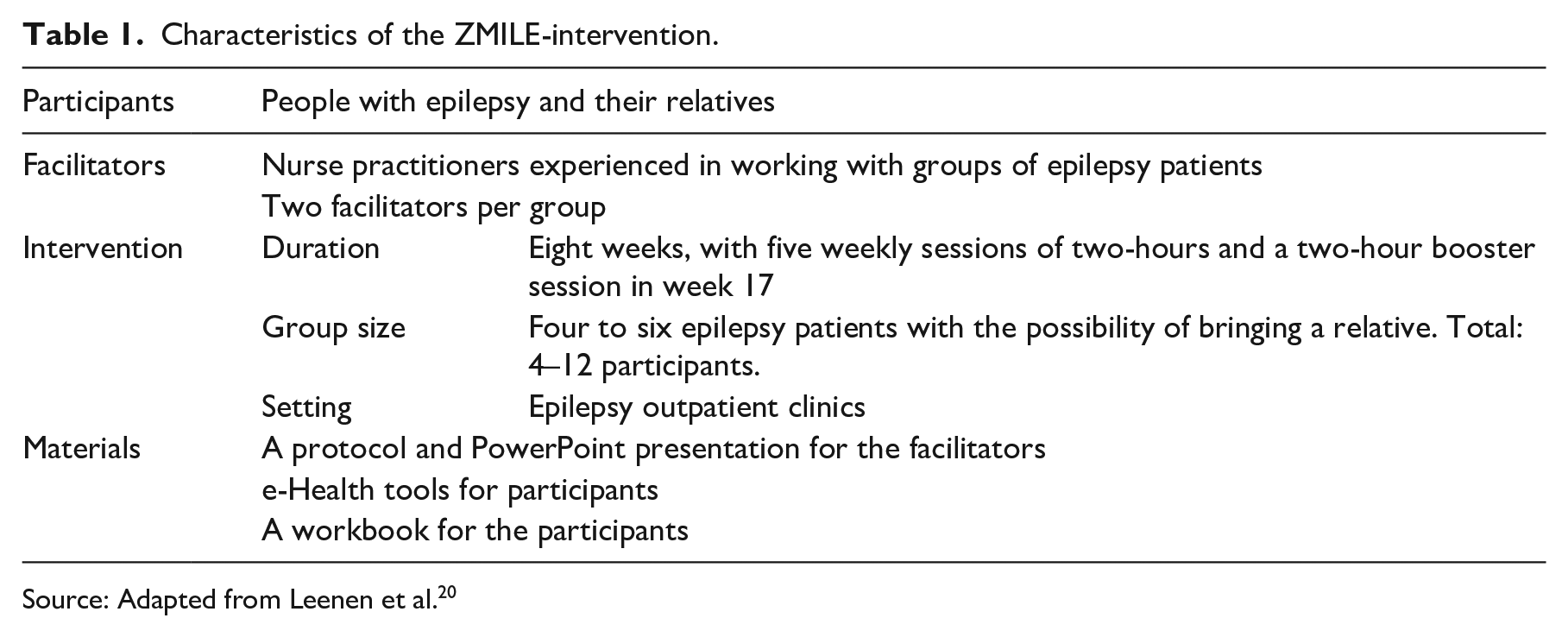
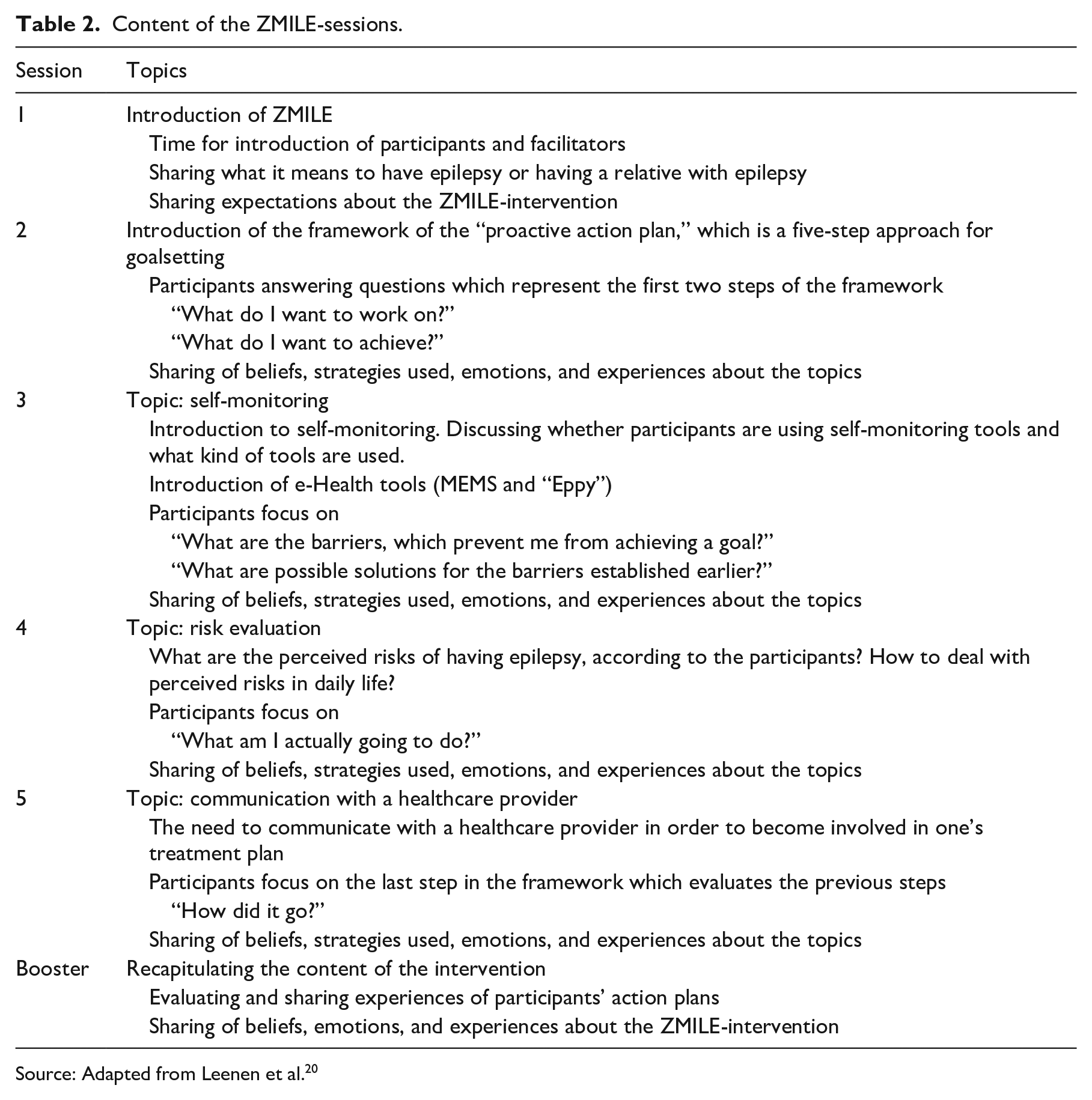
Each group session focuses on one specific theme (see Tables 1 and 2 for a concise summary of the content). The first session is about getting to know each other. Participants are asked to share the impact of epilepsy on their lives, and what they expect from the ZMILE-training. At the end of the first group session, participants are also asked to think about which skills they are good at and skills less as preparation for the next group session.
Characteristics of the ZMILE-intervention.
Source: Adapted from Leenen et al. 20
Content of the ZMILE-sessions.
Source: Adapted from Leenen et al. 20
During the second group session, the five-steps framework of goalsetting is introduced with focus on the first two steps only. This framework is aimed to provide insight of what is needed for goalsetting and to raise awareness that goalsetting differs from only having the intentions to do something. In order to reach a goal, it is important to set goals, to be aware of the hurdles, and to be able to remove those hurdles. The rationale behind the five-steps framework is that it forces the user to think about matters that are often overlooked.
The five steps are essentially (1) define the stressor (e.g. “What would you like to change?”), (2) define the goal (e.g. “What would you like to achieve; more happiness or more confidence?”), (3) define the difference (e.g. “Why haven’t you reach the goal before?”), (4) define an actionplan (e.g. “What is your exact actionplan?”, (5) evaluate the process (e.g. “Have you achieved your goal?”).
The focus of the third group session is on self-monitoring and step three of the five-steps framework. Self-monitoring refers to the observation of symptoms in order to gain insight into one’s own disease progression and therefore be able to anticipate with possible complications. The goals of self-monitoring are for example, (1) having essential disease-related information to share with healthcare professional, (2) to aid making lifestyle changes, (3) to check if one’s goal has been achieved.
First, patients are asked about their methods of keeping record of their epilepsy, seizure frequency and severity, and medication intake. Secondly, patients learn about different e-Health tools that can be used for self-monitoring. After a break of ten minutes, the focus is on the third step of the goalsetting framework (e.g. “What are the most important differences between the current situation and the desired situation?”, and “What do you need to achieve the desired situation?”).
In the fourth group session, risk-evaluation and the fourth step of the five-steps framework are discussed. Participants learn about the perceived risks of having epilepsy or living with someone with epilepsy. Epilepsy changes lives, which are the risks of epilepsy. Those risks can be categorized into (1) physical changes (i.e. medication management), (2) lifestyle changes (e.g. changes in social contacts, work, and hobbies), (3) changes in thinking and feelings (i.e. emotional management). The group will also discuss about the possible seizure triggers (e.g. missed dose of anti-epileptic drugs and sleep deprivation), and what changes the participants can make in order to lower the risk of those triggers. As such, participants are triggered to extensively think about both causes and consequences of epilepsy-related risks.
After the ten-minutes break, the group continues with the five-steps framework of goalsetting. Whereas step three mainly focuses on turning intentions into goals, step four activates participants to make the goals specific and measurable (e.g. “On Wednesday and Friday evening, I will go out for a 30-minutes walk after dinner”).
Communication with healthcare providers is the theme of the fifth and last group session. Information exchange plays an important role in shared decision making, which is a two-way process that requires input from both healthcare professional and patient. Healthcare professionals provide disease-specific information to their patients (e.g. diagnosis, prognosis, treatment- and care-options, and the associated advantages and disadvantages) on the one hand, whereas the patient is expected to expresses his/her preferences regarding the options and the desired extent of involvement in the shared decision making.
During the second part of this group session, participants are asked to focus on the last step in the five-steps approach of “How did it go?”, which is to share their experience of goalsetting using this approach (e.g. beliefs, strategies used, and emotions)
Three months after the last group session, there is a booster session during which experiences of the ZMILE-training are being recapitulated and evaluated (see case report for an example).
Tailoring
In order to enhance individual proactive coping skills using the five-steps framework of goalsetting and to be able to have patients and people close to them tackling individual problems, each participant was required to set personal goals to work on in between sessions. Each session, feedback moments were scheduled in order for all participants to share their experience and progression, and to receive feedback from the nurse practitioners and the rest of the group (i.e. peer support).
Fidelity and modifications after process evaluation
As part of an implementation study to examine how ZMILE could be embedded in the Netherlands and be made available for patients across the country, the intervention protocol was adjusted based on recommendations made by patients and clinicians during the previously published process evaluation. In this study, characteristics, performance according to protocol, attendance and adherence, and opinion about the intervention were evaluated. 20 These changes were then presented to a group of experts, including clinicians, patients, healthcare insurers, and policy makers.
The ZMILE-intervention was shown to have been performed largely according to protocol. The overall attendance and adherence rates were high and both participants and facilitators had a favorable opinion about the intervention.
Unfortunately neither e-Health tool, the Medication Event Monitoring System nor the Eppy, are now available, and therefore can no longer be used as monitoring and self-reporting tools for the ZMILE-intervention. The Medication Event Monitoring System was specifically designed for scientific purposes (e.g. clinical trials) and “Eppy” has been discontinued and removed from online stores for all major smartphone platforms.
One of the most important suggestions from participants was to plan the booster session at a later time (at three months instead of three weeks). In addition, it was mentioned that the active role of the relative should be emphasized more explicitly. Last, as changing health behavior requires time and continuous effort, a follow-up or maintenance plan was suggested. However, this has not yet been developed.
In comparison with the original ZMILE-intervention (as evaluated in the clinical trial), the current intervention differs in:
The booster session is now scheduled at three months instead of three weeks after the fifth session.
“Eppy” does not exist anymore, so recommendations are provided for more recently developed applications designed for people with epilepsy or more generic self-monitoring applications.
Due to the lack of suitable alternatives, the Medication Event Monitoring System has been excluded from the intervention, but a focus on concordance remains with special emphasis on the use of e-Health aids to record the use of medication.
Discussion
The ZMILE-intervention is designed to be used in an outpatient clinic for a wide range of adult people with epilepsy (i.e. not specifically tailored to specific types or severities of epilepsy), and the goal is to improve self-efficacy, quality of life, adherence, emotional well-being, seizure severity, and proactive coping.
The ZMILE-intervention has been evaluated in terms of clinical effectiveness, cost-effectiveness, and feasibility, and changes to the protocol were made accordingly. Neither effectiveness nor cost-effectiveness showed statistical significance in the primary outcome measure, which was disease-specific self-efficacy. However, improvement has been shown in some domains of the quality of life in the scale of epilepsy, and there was a decrease in anti-epileptic drug side-effects in the ZMILE-intervention group, in comparison with the control group. 18 Moreover, cost-effectiveness estimates for the ZMILE-intervention appeared to be promising. 19 Therefore, the ZMILE-intervention could prove to be a promising and cost-effective addition to the current standard care for adults with epilepsy.
Currently, the project group is examining ways to optimally implement ZMILE in Dutch clinical practice: for example, by finetuning the course materials according to the process evaluation, by developing a maintenance plan, by looking into ways to make the intervention financially accessible to people with epilepsy (e.g. by way of reimbursement), to determine the most suitable and convenient ways to offer the intervention to people with epilepsy (e.g. in terms of location and personnel availability), and to guarantee the quality of the intervention (e.g. training for nurse practitioners).
According to the process evaluation, ZMILE was performed conforming to protocol. The attendance rate among participants, both participants and facilitators, indicated that they would recommend the ZMILE-intervention to other people with epilepsy and their relatives. Moreover, the overall adherence of participants was high. Therefore, the ZMILE-intervention is considered feasible by patients, relatives, and facilitators.
During the randomized controlled trial, two e-Health tools were used. One was a smartphone application for self-reporting which presented problems that led to discontinuation of use, and was later removed from all smartphone application stores. The other one was a system used to monitor medication intake (e.g. Medication Electronic Monitoring System), which was also discontinued from use during the trial as it was mainly used to monitor patients’ adherence in an objective way. However, more recently developed applications designed for people with epilepsy or more generic self-monitoring applications are now recommended in the course manual. This needs to be carefully monitored as the development of such instruments is highly dynamic and ever continuing. Given, the necessity of e-Health tools shown in the process evaluation, additional criteria are provided in the manual to aid the choice of e-Health application at any time.
The main barrier mentioned by all facilitators was the lack of follow-up on the goal-settings tasks and for the support of further self-management. The booster session was meant to follow up the goal-setting tasks. A remark on the booster session was also that it was planned too soon after the last session.
Therefore, in the final ZMILE-intervention, the booster session is scheduled three months after the last session. However, the maintenance of self-management remains a problem, since maintenance requires the process of changing health behavior.
One problem is that the intended behavioral change is likely to decay over time.31,32 For this, a maintenance plan would be desirable after the booster session. However, due to practical constraints (e.g. imbedding in clinical consultation or the requirements of a long-term follow-up) this is not part of the ZMILE-intervention. Future studies should examine the impact of such a maintenance plan, as it has been shown in other studies that maintenance plans implemented in, for example, self-management programs for Chronic Obstructive Pulmonary Diseases, have significant beneficial effects. 11
In summary, some limitations of the ZMILE-intervention and our evaluation study concern the use of e-Health tools and maintenance plans. Both have been found essential elements of the ZMILE-intervention, but were not part of the original study and need to be investigated in further research.
Clinical message
The ZMILE-intervention is a promising multicomponent self-management program that aims to increase people’s understanding of a medical regimen; it improves communication between patient, relative, and healthcare professionals, enhances skills and provides tools to strengthen self-management behavior.
The ZMILE-intervention is feasible from the perspective of patients, relatives, and professionals.
Footnotes
Acknowledgements
All project materials, including the coursebook, can be found at: vhc.mumc.maastrichtuniversity.nl/zmile-interventie-self-management-epilepsy
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Dutch Organization for Health Research and Development (ZonMW), grant application number 836011018.