
Abstract
Objective:
To assess the clinical and cost-effectiveness of cognitive rehabilitation for attention and memory problems in people with multiple sclerosis.
Design:
Multicentre, pragmatic, randomized controlled trial.
Setting:
Community
Participants:
People with multiple sclerosis aged 18–69 years, who reported cognitive problems in daily life and had cognitive problems on standardized assessment.
Interventions:
A group cognitive rehabilitation programme delivered in 10 weekly sessions in comparison with usual care.
Main measures:
The primary outcome was the Multiple Sclerosis Impact Scale Psychological subscale at 12 months after randomization. Secondary outcomes included measures of everyday memory problems, mood, fatigue, cognitive abilities and employment at 6 and 12 months after randomization.
Results:
In all, 245 participants were allocated to cognitive rehabilitation and 204 to usual care. Mean Multiple Sclerosis Impact Scale Psychological at 12 months was 22.2 (SD = 6.1) for cognitive rehabilitation and 23.4 (SD = 6.0) for usual care group; adjusted difference −0.6, 95% confidence interval (CI) = −1.5 to 0.3, P = 0.20. No differences were observed in cognitive abilities, fatigue or employment. There were small differences in favour of cognitive rehabilitation for the Multiple Sclerosis Impact Scale Psychological at 6 months and everyday memory and mood at 6 and 12 months. There was no evidence of an effect on costs (−£808; 95% CI = −£2248 to £632) or on quality-adjusted life year gain (0.00; 95% CI = −0.01 to 0.02).
Conclusion:
This rehabilitation programme had no long-term benefits on the impact of multiple sclerosis on quality of life, but there was some evidence of an effect on everyday memory problems and mood.
Introduction
Up to 70% of people with multiple sclerosis experience cognitive problems, which negatively impact on function and quality of life. 1 Cognitive rehabilitation is a structured set of therapeutic activities to retrain cognitive skills or to improve people’s ability to cope with cognitive deficits in daily life. However, the evidence for the effectiveness of cognitive rehabilitation is weak. Several systematic reviews have found some positive effects of cognitive rehabilitation in people with multiple sclerosis, but these are based on poor quality randomized controlled trials (RCTs) with several methodological shortcomings, with review authors suggesting the level of evidence is ‘low’.2–4 No trial has evaluated the cost-effectiveness of cognitive rehabilitation. Therefore, the reviews have concluded that more high-quality trials are needed before firm conclusions can be reached.2–4
Although there is some support for the effectiveness of computerized cognitive rehabilitation to retrain cognitive skills in people with multiple sclerosis, 4 these studies have rarely included any long-term follow-up to assess whether the observed benefits persisted or generalized to daily life. There is less evidence for cognitive rehabilitation to teach people skills to cope with the cognitive impairment and provide aids to enable them to compensate for the loss of cognitive abilities. The ReMIND trial 5 (n = 72) evaluated the effectiveness of two types of group memory rehabilitation programme in neurological patients with memory problems, many of whom had multiple sclerosis (n = 39). The memory rehabilitation programmes focussed either on restitution strategies (e.g. drill and practice exercises and teaching people to break down memory tasks into constituent parts) or compensation strategies (e.g. using external memory aids). The data from the study indicated that the interventions were worthy of further evaluation. Carr et al. 6 (n = 48) combined the restitution and compensation strategies from the ReMIND trial and compared this with usual care for patients with multiple sclerosis. The results showed a beneficial effect on mood, favouring cognitive rehabilitation.
Therefore, the present trial was designed to assess the clinical and cost-effectiveness of this cognitive rehabilitation programme for people with multiple sclerosis.
This article reports the main outcomes with further details available elsewhere. 7
Methods
This was a pragmatic, multicentre, observer-blinded RCT comparing a cognitive rehabilitation programme (intervention) in addition to usual care, with usual care alone (control). The trial was conducted in five sites in England. Participants were identified through United Kingdom National Health Service hospitals, charities (e.g. MS Society) and the United Kingdom MS Register. Ethical approval was granted by West Midlands, South Birmingham Committee (Ref. 14/WM/1083), and the protocol was published 8 and the trial was prospectively registered (ISRCTN09697576/14/08/2014). This work was funded by the National Institute for Health Research Health Technology Assessment programme (project number 12/190/05).
Participants were recruited between 13 March 2015 and 23 March 2017. People with multiple sclerosis were eligible if they were
Aged 18–69 years.
Diagnosed with relapsing–remitting or progressive multiple sclerosis.
Diagnosed at least three months prior to the screening assessment.
Reported having cognitive problems defined as >27 on the patient version of the Multi-ple Sclerosis Neuropsychological Screening Questionnaire. 9
Impaired on at least one of the Brief Repeatable Battery of Neuropsychological tests, 10 defined as performance >1 standard deviation (SD) below the mean of healthy controls, corrected for age and education. 11
Able to attend group sessions.
Able to speak English sufficiently to complete the cognitive assessments.
Gave written informed consent.
Potential participants were excluded if they
Had vision or hearing problems, such that they were unable to complete the cognitive assessments.
Had concurrent severe medical or psychiatric conditions, which prevented them from engaging in treatment.
Were involved in other psychological intervention trials.
Demographic and clinical information were recorded. The Brief Repeatable Battery of Neuropsychological tests 10 and Multiple Sclerosis Neuropsychological Screening Questionnaire 9 were administered by an Assistant Psychologist to check that participants met the inclusion criteria. The postal version of the Guy’s Neurological Disability Scale 12 was administered to record the level of disability.
Eligible participants were then given the following questionnaires to complete in their own time:
Multiple Sclerosis Impact scale 13 version 2, to assess the impact of multiple sclerosis on quality of life.
General Health Questionnaire 30, 14 to detect psychological distress.
Everyday Memory Questionnaire – participant version, 15 to assesses the frequency of cognitive problems in daily life.
Fatigue Severity Scale 16 five-item Rasch-analysed version, to assess fatigue.
Participants were asked to nominate a relative or friend to complete the Everyday Memory Questionnaire – relative version. 15
At a subsequent visit, the Assistant Psychologist administered the following assessments:
Doors and People, 17 an objective measure of memory function.
Trail Making Test, 18 to assess attention and executive abilities.
European Quality-of-Life five-level version (EQ-5D-5L), 19 a generic health-related quality-of-life measure to calculate Quality-Adjusted Life Year scores (QALYs).
Use of Health and Social Services questionnaire to assess healthcare utilization and services provided by charities.
The Assistant Psychologist checked participants’ availability to attend groups, should they be randomized to receive the intervention, and checked their preference to receive the outcome questionnaires by post or on-line.
Groups of 9–11 participants who could potentially attend for treatment at the same time and venue were individually randomized to either intervention or usual care on a 6:5 ratio. Allocation was stratified by recruitment site and minimized by multiple sclerosis type (relapsing–remitting or progressive) and gender. The allocation algorithm was held on a secure server and the Assistant Psychologists at each site used a remote, Internet-based randomization system to obtain treatment allocations for each participant. Assistant psychologists and participants were aware of the group allocation.
Usual care comprised general advice from multiple sclerosis nurse specialists and occupational therapists on how to manage any cognitive difficulties. All participants were notified of information available on the webpages of multiple sclerosis charities, which include suggestions for coping with cognitive problems. All other clinical services, and support from specialist charities, were available as part of usual care. The usual care that participants received was recorded on the Use of Health and Social Services questionnaire.
Cognitive rehabilitation was provided by an Assis-tant Psychologist to groups of four to six participants, who met approximately weekly for 10 sessions. The content of sessions was defined in a treatment manual (see supplementary material), which was developed in a previous study. 6 The intervention included restitution strategies to retrain attention and memory functions and strategies to improve encoding and retrieval. Compensation strategies taught included the use of internal mnemonics (such as chunking) and external devices (such as diaries and mobile phones) and ways of coping with attention and memory problems. Attendance was recorded. If participants missed a session, they could attend early for the following session to catch up on the content they had missed. Homework assignments facilitated individualisation of care and generalization of cognitive strategies to daily life.
Outcomes assessed at 6 and 12 months after randomization included the Multiple Sclerosis Impact Scale, Everyday Memory Questionnaire – participant version, General Health Questionnaire 30, Fatigue Severity Scale, Brief Repeatable Battery of Neuropsychological tests, Doors and People, Trail Making, EQ-5D-5L, Use of Health and Social Services questionnaire and employment status. The Guys Neurological Disability Scale and number of relapses in the previous six months were also recorded. In addition, the participants’ nominated relative or friend completed the Everyday Memory Questionnaire – relative version and Modified Carer Strain Index. 20
Questionnaires were returned by post or completed on-line. Research Assistants, blind to treatment allocation, conducted outcome visits to complete cognitive tests and the Use of Health and Social Services questionnaire.
The Multiple Sclerosis Impact Scale Psychological subscale at the 12-month follow-up was the primary outcome. A difference of 3–3.5 points on the Multiple Sclerosis Impact Scale Psychological subscale was considered clinically meaningful. Based on the Multiple Sclerosis Impact Scale Psychological subscale, 143 participants per group were required to detect a difference of 3 points, assuming an SD of 9, with 80% power and 5% two-sided alpha. However, a clustering effect may be expected to occur in the intervention arm due to the intervention being delivered in groups. Based on an average treatment group size of five evaluable participants and an inter-cluster correlation of 0.1 in the intervention group, an optimal allocation ratio of 6:5 in favour of the intervention group, a total of 336 evaluable patients would provide 80% power to detect such a difference. A total of 400 participants were to be randomized (216 to intervention and 184 to usual care) to allow for non-collection of primary outcome data in 15% of participants.
The planned analyses were summarized in the Statistical Analysis Plan and Health Economic Analysis, which were finalized prior to database lock and release of the treatment allocation codes for analysis. All analyses were conducted using Stata/SE 14.1/15.1.
The analysis was a modified intention-to-treat, that is, analysis according to randomized group regardless of adherence to allocation and including only participants who provided outcome data at follow-up. The difference in mean outcome scores between the two groups at each time point was estimated using a multilevel linear model with site, multiple sclerosis type, gender and baseline score as covariates. Individuals allocated to usual care had no contact with each other, and outcomes in this group were therefore assumed to be independent. However, participants allocated to cognitive rehabilitation received sessions together in groups. Therefore, a fully heteroscedastic model estimated group-level residual variance in the intervention group and also permitted individual-level residual variance to differ between groups. Assumptions for the multilevel linear model were checked using diagnostic plots. Missing baseline scores were imputed for the analysis using the mean score at each site.
The primary health economic outcome consisted of a cost-utility analysis at 12 months. Utility was estimated from EQ-5D-5L responses cross-walked to the 3L value set for England consistent with the guidance from the National Institute for Health and Care Excellence. 21 Cost-utility and cost-effectiveness analyses were undertaken to estimate the incremental cost per QALY gained and incrementally cost per improvement in Multiple Sclerosis Impact Scale Psychological subscale score based on the primary clinical endpoint. Results of the comparative analysis of incremental costs and effects were summarized as incremental cost-effectiveness ratios.
The study was overseen by an independent Trial Steering Committee and Data Monitoring Committee.
Results
Of the 449 participants randomized, 245 were allocated to cognitive rehabilitation and 204 to usual care (see CONSORT diagram, Figure 1).
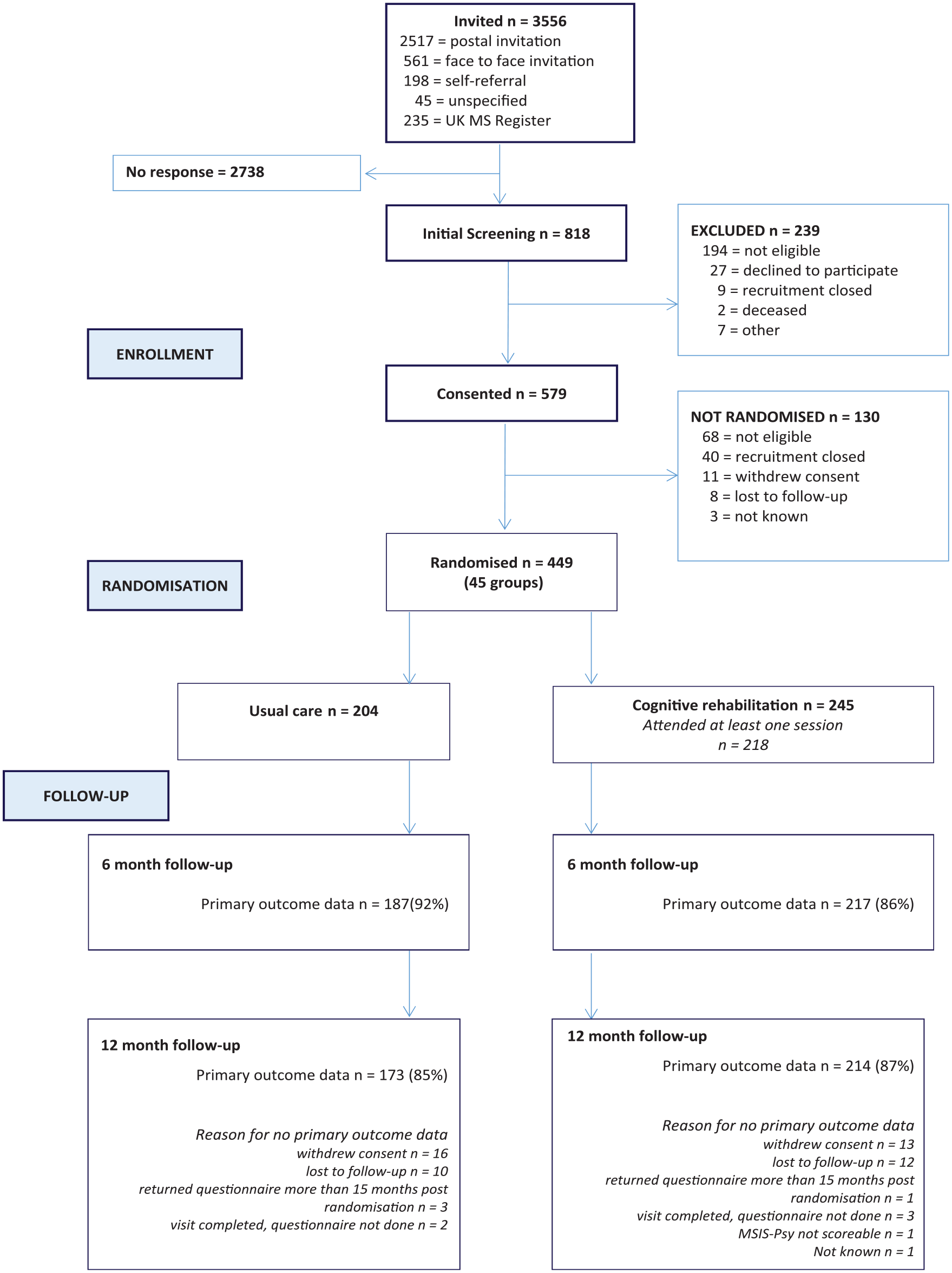
Participant flow.
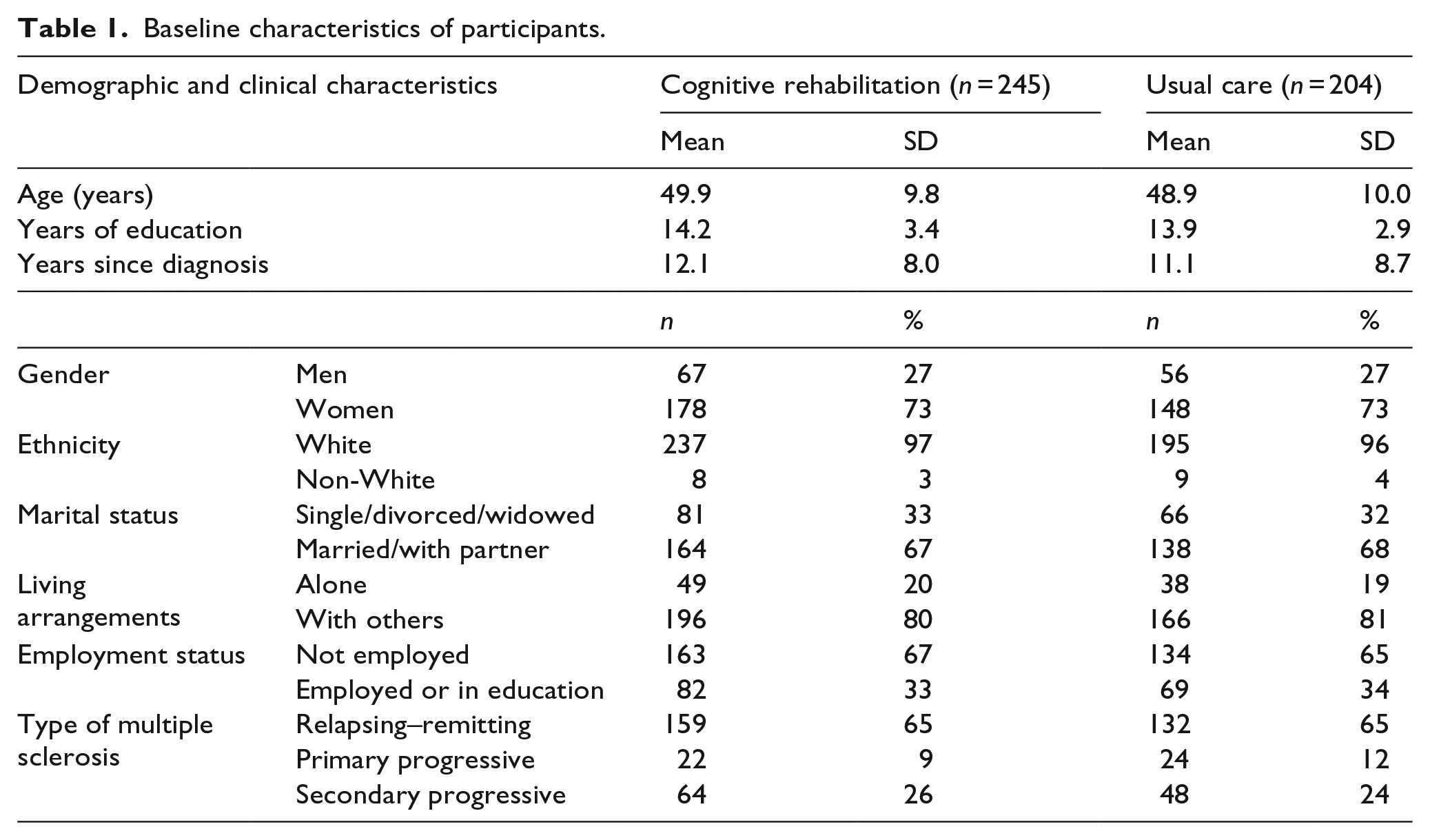
The groups appeared well-matched on baseline characteristics (Table 1) and on baseline scores on questionnaire measures and cognitive tests (Table 2).
Baseline characteristics of participants.
Baseline scores on Questionnaires and cognitive tests.
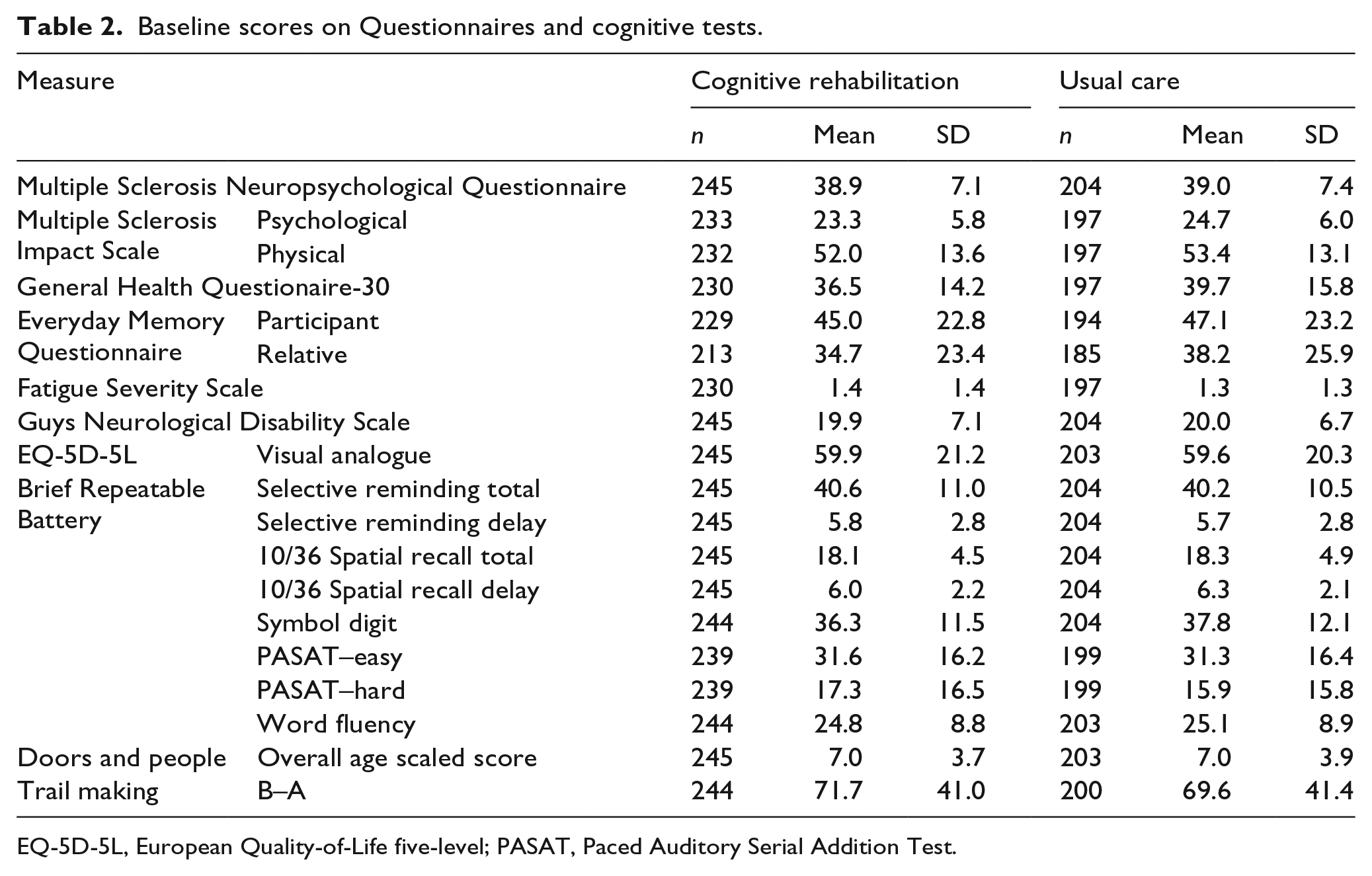
EQ-5D-5L, European Quality-of-Life five-level; PASAT, Paced Auditory Serial Addition Test.
Of the 245 allocated to cognitive rehabilitation, 208 (85%) attended at least three sessions, the minimum number considered likely to effect a change. The mean attendance was 7.7 sessions (SD = 3.5, range = 0–10). Based on the Use of Health and Social Services questionnaire and feedback interviews, participants in the usual care group received no cognitive rehabilitation.
Of the 449 participants, 214 (87%) in the intervention group and 173 (85%) in the control group were included in the primary analysis (see Figure 1).
There was no evidence of any clinically important difference between the groups on the primary outcome, the Multiple Sclerosis Impact Scale Psychological subscale at 12 months (Table 3). Analysis of secondary outcomes showed there was evidence of a small difference on the Multiple Sclerosis Impact Scale Psychological subscale at 6 months favouring cognitive rehabilitation. Differences favouring cognitive rehabilitation were also found on the Everyday Memory Ques-tionnaire–participant and relative versions, and the General Health Questionnaire 30, at both 6 and 12 months (Table 3). There were no differences on the Multiple Sclerosis Impact Scale Physical subscale, cognitive tests, fatigue or Modified Carer Strain Index. Employment status was no different between the groups. The level of disability on the Guys Neurological Disability Scale and number of relapses were similar in the two groups, indicating that results were not due to changes in the physical progression of multiple sclerosis.
Comparison of primary and secondary outcomes at 6- and 12-month follow-up.
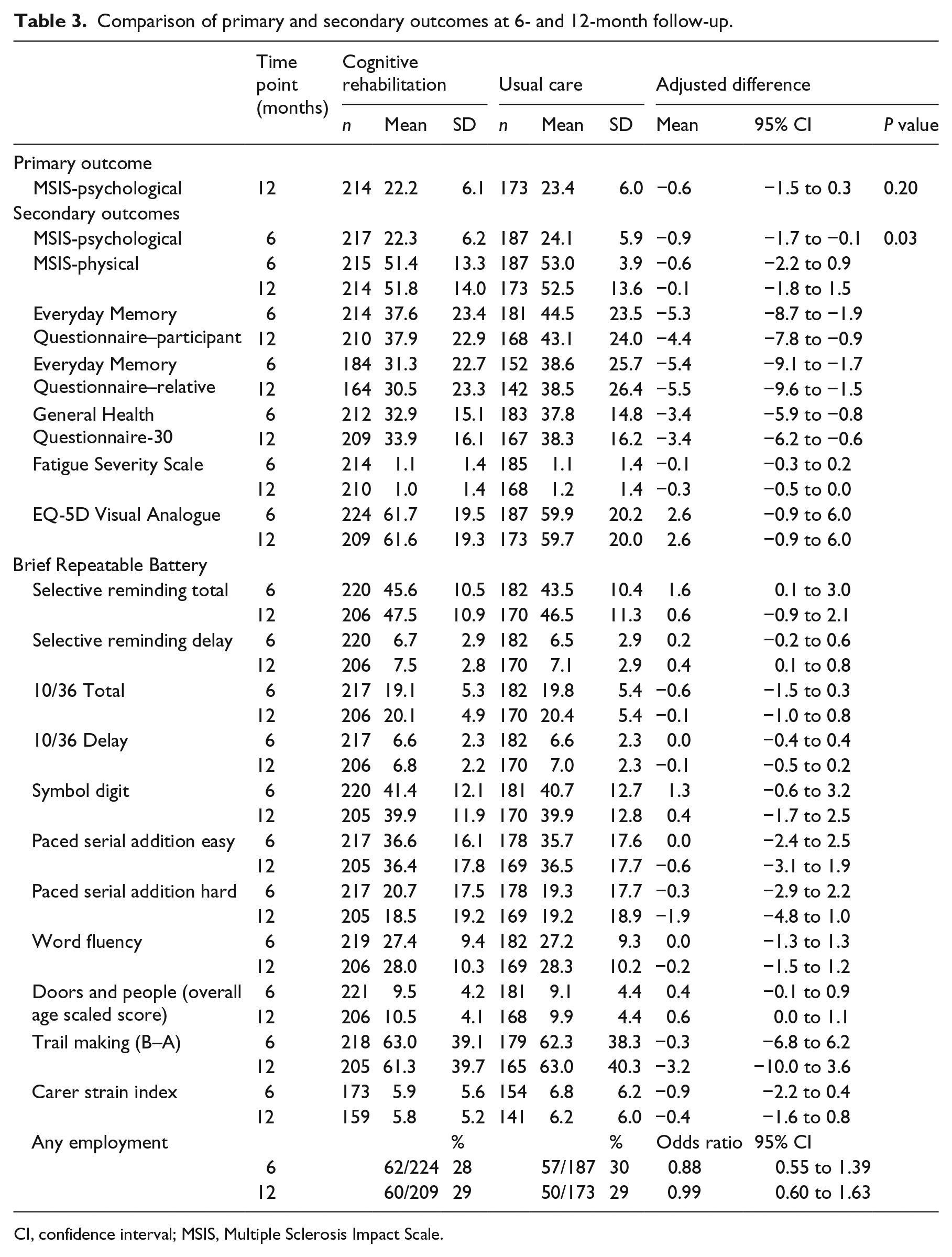
CI, confidence interval; MSIS, Multiple Sclerosis Impact Scale.
No safety concerns were raised and no deaths reported. The cost of delivering the cognitive rehabilitation was estimated at £209 per participant, with 77% of the total cost attributable to the Assistant Psychologist delivering sessions. Mean total costs associated with cognitive rehabilitation of £5885 (n = 208) were over £800 lower than those of usual care £6574 (n = 170), but there was no evidence of a difference (P = 0.27). Despite small QALY gains at 12 months for both groups, there was no evidence of a difference between groups (P = 0.2). The use of multiple imputation to address missing data for both costs and outcomes produced similar results with no evidence of a cost or QALY difference between groups (see Table 4).
Cost- and quality-adjusted life year outcomes at 12-month follow-up.
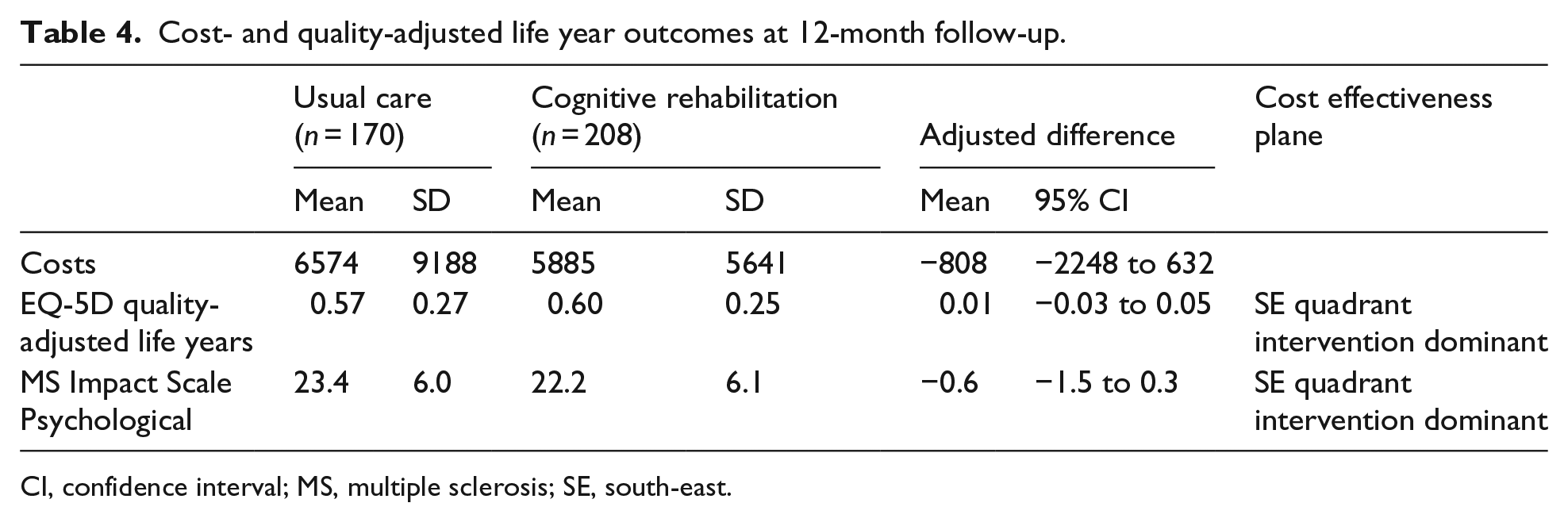
CI, confidence interval; MS, multiple sclerosis; SE, south-east.
Lower scores on the Multiple Sclerosis Impact Scale Psychological subscale represent less psychological impact of multiple sclerosis on quality of life; therefore, negative incremental differences favour the intervention. Positive incremental QALY differences favour the intervention.
The cost-effectiveness plane for the EQ-5D (Figure 2) shows a distribution of estimates centred in the bottom right hand quadrant consistent with cognitive rehabilitation dominating usual care.
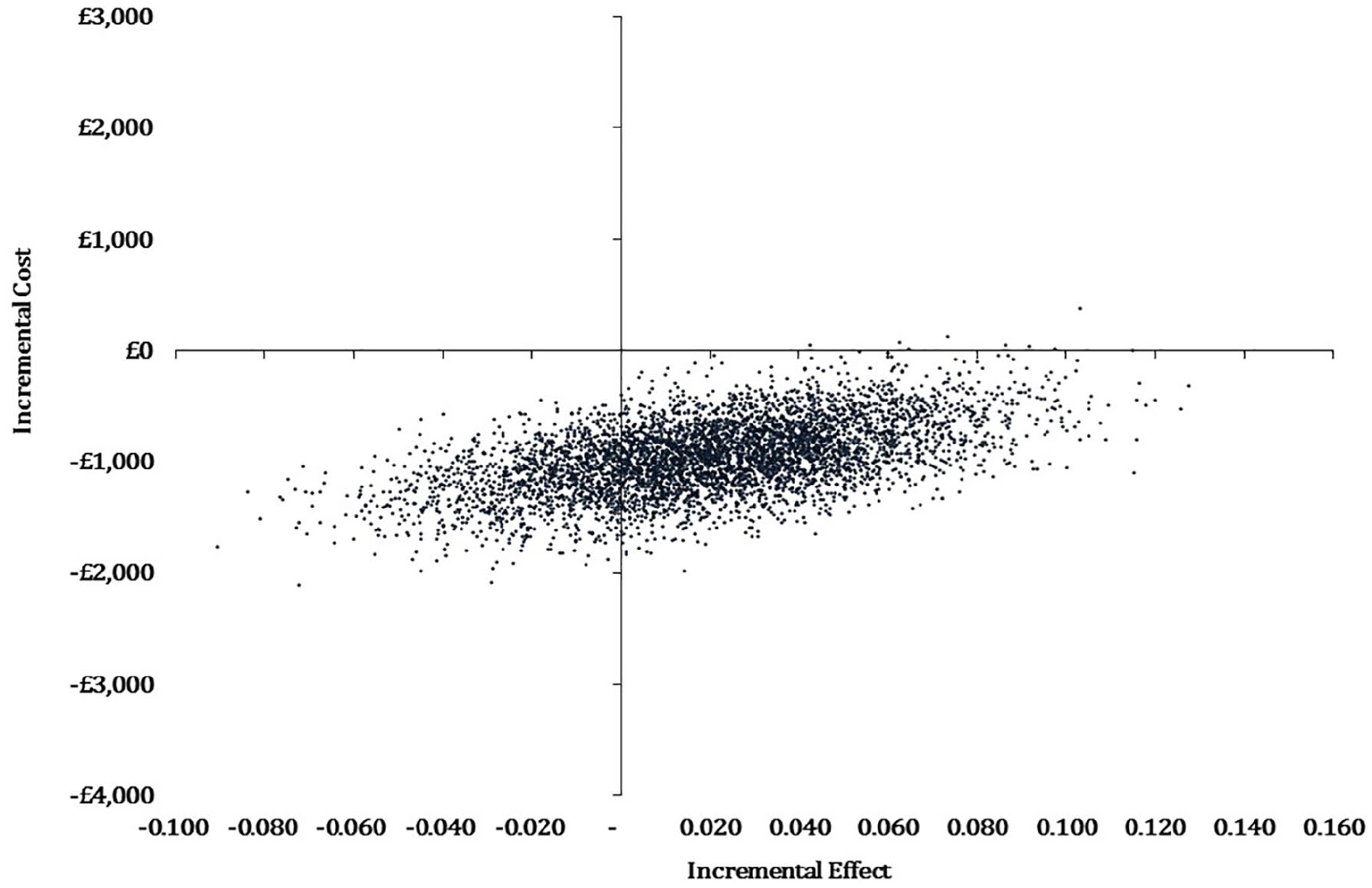
Cost-effectiveness plane for EQ-5D-5L QALYs at 12 months.
The cost-effectiveness acceptability curve (Figure 3) shows a high probability of the intervention being cost-effective at willingness-to-pay thresholds between £0 and £100,000. At a willingness-to-pay threshold of £30,000 per QALY gained, cognitive rehabilitation has a 97% probability of being cost-effective.
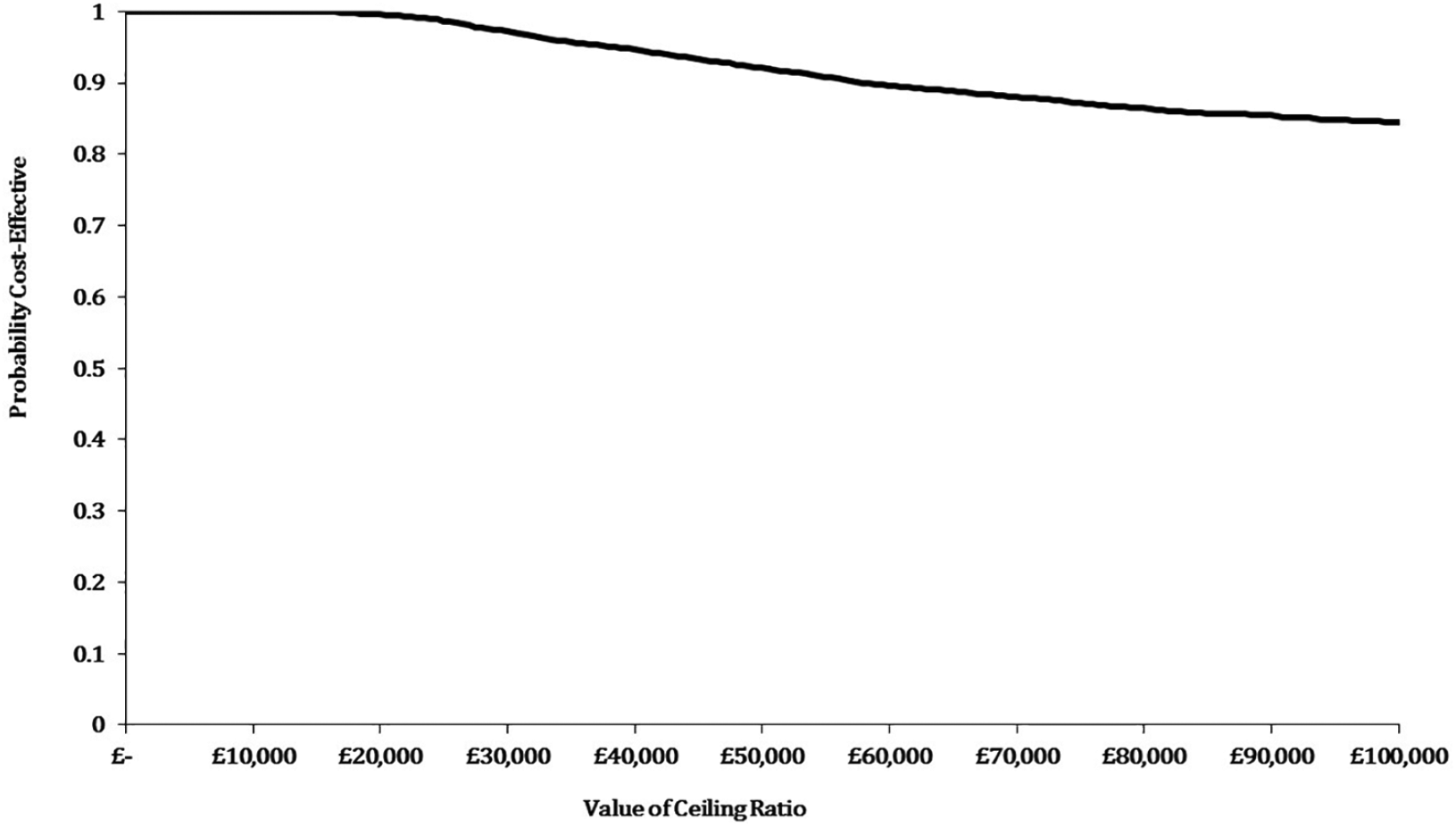
Cost-effectiveness acceptability curve for EQ-5D-5L QALYs at 12 months.
Discussion
This cognitive rehabilitation programme provided in addition to usual care did not reduce the psychological impact of multiple sclerosis on quality of life at 12 months compared to usual care alone, but there was a small reduction in the psychological impact of multiple sclerosis at 6 months. Thus, there was some evidence to suggest that cognitive rehabilitation improved quality of life in the short term, but the effects were not maintained over time. There were differences between groups in the frequency of subjective complaints of cognitive problems from both people with multiple sclerosis and their relatives and mood at both the 6- and 12-month follow-ups favouring the cognitive rehabilitation group.
Strengths of the study included a large sample size (with previous studies of cognitive rehabilitation having a mean of 42 participants) 2 and good attendance at sessions, so most people received most of the intervention. The attendance rate was consistent with the pilot study; 6 however, many studies do not report attendance rates, 22 so direct comparisons of attendance rates across trials are limited. The reasons for non-attendance reflect aspects of daily life unrelated to cognitive problems, such as illness and holidays, rather than not wanting to continue in the group.
There are, however, some limitations to the study. The lack of information on demographic characteristics of those who did not wish to take part limits the ability to determine the proportion of people who would be eligible for the treatment if it were routinely available. As a pragmatic trial, the inclusion criteria were intentionally broad to involve all those who might be treated in clinical practice, thereby increasing generalizability of the findings. However, almost half of those excluded was due to scoring too low on the Multiple Sclerosis Neuropsychological Screening Questionnaire, yet they believed they had cognitive difficulties. In the pilot study, 6 participants were recruited if they reported cognitive problems in daily life and no standardized assessment was used. The Multiple Sclerosis Neuropsychological Screening Questionnaire was used to provide a more replicable criterion. However, the cut-off of >27 was based on the original validation study 11 and lower cut-offs have been recommended subsequently.23–25 Therefore, the sample included those with relatively severe cognitive problems in daily life, and these people may benefit less from the intervention. 26
The primary outcome was the Multiple Sclerosis Impact Scale Psychological subscale, which was developed specifically for people with multiple sclerosis, and includes items on mood, coping and cognition; it has good psychometric properties and has been shown to be sensitive to the effects of rehabilitation. However, even on the Psychological subscale, some items are unlikely to be directly influenced by cognitive rehabilitation (such as ‘feeling unwell’ or ‘problems sleeping’). Impact of multiple sclerosis and quality of life are multidomain constructs, and changing the impact of multiple sclerosis on quality of life, although desirable, may be unrealistic for interventions that focus on specific symptoms of multiple sclerosis. The research funder’s commissioning brief indicated that quality of life in the longer term was an important outcome, and therefore, the Multiple Sclerosis Impact Scale Psychological subscale at 12-month follow-up was used.
These findings are consistent with previous cognitive rehabilitation research in people with multiple sclerosis,27,28 in that they show benefits of cognitive rehabilitation that focusses on teaching strategies to cope with cognitive impairments in daily life on measures of memory problems in daily life. However, comparison with the ReMemBrIn trial, 26 which evaluated the same intervention in people with traumatic brain injury, suggested that those with multiple sclerosis responded better than those with traumatic brain injury. One possible reason is that usual care for people with traumatic brain injury in the United Kingdom often includes cognitive rehabilitation, whereas it does not for people with multiple sclerosis.
The finding of a beneficial effect on mood supports our pilot trial 6 and the multiple sclerosis subgroup analysis of that trial, 29 both of which used a similar treatment approach, and with a previous study of group treatment. 27 A strong relationship has previously been documented 30 between subjective cognitive problems and mood in people with multiple sclerosis. The beneficial effect on mood could therefore be partly attributable to the social contact afforded by attending sessions rather than the content of the intervention. However, it seems more likely that the change in mood was in response to changes in everyday memory because relatives’ reports of the frequency of everyday memory problems also showed a difference between groups, favouring the intervention group.
The results indicated that the intervention had no effect on cognitive impairment, as assessed on cognitive tests. In most studies which show changes in cognitive function, the intervention comprises direct retraining of cognitive skills. The focus of the intervention in the cognitive rehabilitation for attention and memory in people with multiple sclerosis (CRAMMS) trial was on learning to cope with cognitive problems, and therefore, cognitive abilities would not necessarily be expected to change. There was also no evidence to suggest that the intervention exacerbated fatigue-related problems, which is positive and consistent with previous trials of cognitive rehabilitation. 2
The incremental cost-effectiveness analysis indicates that cognitive rehabilitation was less costly and more effective than usual care, suggesting dominance of the intervention. However, differences in both costs and effects were small with no evidence of a difference between groups. The key cost drivers were medications and social services; however, for each component of the Use of Health and Social Services Questionnaire, outliers had a substantial impact on the mean value, with a few high-cost users increasing the average cost resulting in high SDs.
Overall, the trial showed no effect of cognitive rehabilitation on the psychological impact of multiple sclerosis on quality of life in the long term, but there were modest benefits in the short term and a reduction in self-reported cognitive problems in daily life and improved mood. Future research should investigate whether there are subgroups who benefit from this intervention and ways in which the effects of cognitive rehabilitation can be maintained over time, such as including booster sessions or additional on-line support. In addition, evaluating the intervention in a less cognitively impaired sample would identify whether earlier intervention would be beneficial. Incorporating this trial in Cochrane review meta-analyses may provide more robust and reliable data to inform a future model-based economic analysis.
Clinical messages
We found no long-term effect of this cognitive rehabilitation programme on the impact of multiple sclerosis on quality of life.
Cognitive rehabilitation improved memory problems in daily life and mood.
Supplemental Material
CRAMMS_FACILITATORS_MANUAL_ – Supplemental material for Cognitive rehabilitation for attention and memory in people with multiple sclerosis: a randomized controlled trial (CRAMMS)
Supplemental material, CRAMMS_FACILITATORS_MANUAL_ for Cognitive rehabilitation for attention and memory in people with multiple sclerosis: a randomized controlled trial (CRAMMS) by Nadina B Lincoln, Lucy E Bradshaw, Cris S Constantinescu, Florence Day, Avril ER Drummond, Deborah Fitzsimmons, Shaun Harris, Alan A Montgomery and Roshan das Nair in Clinical Rehabilitation
Supplemental Material
CRAMMS_PATIENT_WORKBOOK – Supplemental material for Cognitive rehabilitation for attention and memory in people with multiple sclerosis: a randomized controlled trial (CRAMMS)
Supplemental material, CRAMMS_PATIENT_WORKBOOK for Cognitive rehabilitation for attention and memory in people with multiple sclerosis: a randomized controlled trial (CRAMMS) by Nadina B Lincoln, Lucy E Bradshaw, Cris S Constantinescu, Florence Day, Avril ER Drummond, Deborah Fitzsimmons, Shaun Harris, Alan A Montgomery and Roshan das Nair in Clinical Rehabilitation
Footnotes
Acknowledgements
We thank all those who took part in the trial and the CRAMMS Trial Collaborative Group including our Patient and Public Involvement collaborators (Miriam Morgan, Julia Scott, Susan Evans, Shirlee McKeown and Trishna Bharadia), site lead investigators (Perry Moore, Carolyn Young, Basil Sharrack, Claire Isaac, David Griffths, Vera Fixter, Laura Hanley and Stephen Evans), Participant Identification Centre leads (Lena Palmer, Tracy Tyrell, Shannon Gaughan, Gemma Elliot, Sophie Keogh, Helen Oldknow, Catherine Edwards and Nigel Schofield), assistant psychologists (Sara Clarke, Kara Crossley, Holly Griffiths, Cara Knight, Kristy Martin, Alexandra Cunliffe, Catherine Pollard, John Wilson, Emma Trigg, Serena Vanzan, Joanna Dalton and Stephanie Pegnall), outcome assessors (Hannah Carpenter, Heather Cogger, Rachel Harnell, Olga Klein, Jacqueline Mhizha-Murira, Katie Powers and Luke Squires), trial and data management team (Kirsty Sprange, Amy Evans, Jo Hobbs, Natalie Wakefield, Brian Barnes, Monica Crone, Matthew Foster, Chris Rumsey and Alexandra Erven), Trial Steering Committee (Rona Moss-Morris, Audrey Bowen and Rory O’Connor) and Data Monitoring Committee (Jenny Freeman, Rod Taylor and Anita Rose).
Author contributions
N.B.L. was the chief investigator and coauthored the final report. L.E.B. analysed the clinical effectiveness data and prepared the results for publication. C.S.C. contributed to the development of the grant application and trial protocol and contributed important intellectual content to the report. F.D. contributed to preparation of the final report. A.E.R.D. contributed to the development of the grant application and trial protocol and contributed important intellectual content to the report. D.F. oversaw the health economics analysis and contributed important intellectual content to the report. S.H. analysed the health economics data and contributed important intellectual content to the report. A.A.M. contributed to the development of the grant application and trial protocol, oversaw the clinical effectiveness analysis and contributed important intellectual content to the report. R.d.N. was the co-chief investigator and coauthored the final report.
Declaration of conflicting interests
C.S.C. reports grants and personal fees from GW (UK), Morphosys (Germany) and Roche (Switzerland) and grants from Sanofi Pasteur MSD (France), outside the submitted work. A.E.R.D. reports membership of the National Institute for Health Research (NIHR) Clinical academic lectureships panel. A.A.M. reports membership of the National Institute for Health Research Health Technology Assessment Clinical Evaluation and Trials Board. R.d.N. reports membership of the NIHR Health Services & Delivery Research committee and is the Chair of the NIHR Research for Patient Benefit East Midlands Research Advisory Committee. He has received funding to prepare and deliver lectures on cognitive rehabilitation in multiple sclerosis from Novartis and Biogen. The other authors report no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the National Institute for Health Research (NIHR) Health Technology Assessment programme (project number 12/190/05). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Supplemental material
Supplemental material for this article is available on-line.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.