
Abstract
Objectives:
The main objective of this study is to determine the feasibility of recruiting and retaining patients recently diagnosed with thoracic cancer to a trial of short-term integrated rehabilitation; evaluate uptake of theoretically informed components targeting physical function, symptom self-management and participation; estimate sample size requirements for an efficacy trial.
Design:
Parallel group randomized controlled feasibility trial.
Setting:
Three U.K. hospitals.
Participants:
Patients ⩽eight weeks of thoracic cancer diagnosis, Eastern Cooperative Oncology Group Performance Status 0–3, any cancer stage and treatment plan.
Interventions:
Participants randomly allocated (1:1) to short-term integrated rehabilitation and standard care or standard care alone over 30 days.
Main measures:
Primary: participant recruitment and retention, targeting ⩾30% of eligible patients enrolling and ⩾50% of participants reporting outcomes at 30 days. Secondary: intervention fidelity; missing data and performance of outcome measures for self-efficacy, symptoms, physical activity and health-related quality of life.
Results:
Of 159 eligible patients approached, 54 (34%) were recruited. A total of 44 (82%) and 39 (72%) participants reported outcomes at 30 and 60 days, respectively. Intervention fidelity was high. Rehabilitation was delivered across 3 (1–3) sessions over 32 (22–45) days (median (range)). Changes in clinical outcomes were modest but most apparent at 60 days for health-related quality of life: Functional Assessment of Cancer Therapy Lung Cancer score median (interquartile range) change 9.7 (−12.0 to 16.0) rehabilitation versus 2.3 (−15.0 to 14.5) standard care.
Conclusion:
A trial to examine efficacy of short-term integrated rehabilitation for people newly diagnosed with thoracic cancer is feasible. A sample of 336 participants could detect a meaningful effect on health-related quality of life as the primary outcome.
Keywords
Introduction
Worldwide, more people are diagnosed with lung cancer than any other cancer 1 and the incidence of pleural mesothelioma continues to increase. 2 The prevalence of distressing and disabling symptoms in these thoracic cancers is high. 3 , 4 Most people are diagnosed with advanced disease 1 , 2 but strive to maintain normality in daily life. 5 Needs-based cancer rehabilitation is recommended from diagnosis to reduce the impact of cancer and its treatment on functional well-being and to promote independence. 6 However, many people face difficulties accessing rehabilitation due to poor service provision, lack of clinician recognition of functional need 6 and/or negative views of rehabilitation. 7 Although traditional exercise-based interventions are safe and potentially effective in this population, rates of uptake and completion in supervised programmes are generally low. 8 , 9 Symptom management interventions tend to be reactive, targeting patients with well-established symptoms. 10 Indi-vidualized proactive rehabilitation programmes to minimize the impact of thoracic cancer on participation in daily life are lacking. To overcome some of these issues, we have developed a model of short-term integrated rehabilitation drawing on theories of illness, 11 , 12 rehabilitation 13 and behaviour change. 14 Rehabilitation processes, components and outcomes were identified via systematic review 15 and focus groups with patients, carers and healthcare professionals. 16 A manual was produced to support delivery of the intervention by a trained rehabilitation practitioner (e.g. physiotherapist, occupational therapist or dietitian). Short-term integrated rehabilitation aims to support people to self-manage symptoms and immediate functional needs. It also aims to reduce sedentary time to minimize the onset of physical deconditioning. Strategies include maintaining or improving physical activity levels, fitness and participation in daily activities during cancer treatment and beyond.
Before testing the efficacy of short-term integrated rehabilitation in a large-scale trial, we have undertaken this formal feasibility study. We aimed to (1) determine the feasibility of recruiting and retaining people with thoracic cancer to a trial of short-term integrated rehabilitation delivered in the period following diagnosis; (2) to evaluate uptake of theoretically informed, individually tailored intervention components and (3) obtain data on the acceptability of selected outcome measures and (4) estimate sample size requirements for an efficacy trial.
Methods
A multicentre randomized controlled feasibility trial comparing the short-term integrated rehabilitation service plus standard care to standard care took place between February 2018 and April 2019. The protocol was preregistered (ISRCTN 92666109). Ethical approved was granted by the London South East Research Ethics Committee (Ref 17/LO/1871). Reporting follows the CONSORT guidelines and the Template for Intervention Description and Replication (TIDieR) checklist. No changes were made to the design or methods following trial commencement.
Participants were recruited from thoracic oncology, palliative care and respiratory clinics across three U.K. hospitals, two in London and one in Nottingham. Eligible participants were adults, within eight weeks of a clinical or histological diagnosis of primary lung cancer (stage I–IV) or pleural mesothelioma (local or extensive), Eastern Cooperative Oncology Group Performance Status of 0–3 (Supplementary Appendix 1) 17 and the ability to respond to questions in written English (or availability of translators to support this). People already receiving specialist rehabilitation, or who had a coexisting progressive neurological condition (e.g. motor neurone disease), Eastern Cooperative Oncology Group Performance Status 4, not able to complete questionnaires due to cognitive impairment, or with a physician-estimated prognosis of less than one month were excluded. All participants gave written informed consent in accordance with the Good Clinical Practice and the Declaration of Helsinki.
Following baseline assessment, conducted in hospital outpatients, inpatients or home settings, participants were randomly allocated (1:1 at the individual level) using an independent Web-based randomization system at the King’s Clinical Trials Unit, London, UK. A minimization algorithm was used to maintain balance in both the trial groups for recruitment site, performance status (0–1 or 2–3) and disease stage (I–II or III–IV). Following randomization, the Clinical Trials Unit informed trial staff via secure email. Research nurses, who arranged outcome assessments using self-report mailed questionnaires, were informed of trial entry but not group allocation. Due to the nature of the intervention, it was not possible to maintain allocation blinding for participants and trial physiotherapists (J.B., M.M., L.F. and E.D.). The trial statistician (W.G.) was also blind to group allocation.
All participants received standard care provided by their hospital for their condition. This included surgical, oncology and supportive and palliative care services. No rehabilitation was routinely provided at two sites. One London site provided multiprofessional outpatient-based specialist rehabili-tation for patients attending oncology follow-up clinics with functional needs identified following screening. We planned to recruit participants who were not scheduled or able to attend these clinics within eight weeks of diagnosis.
Participants allocated to short-term integrated re-habilitation (Supplementary Figure 1) were offered up to three sessions with a rehabilitation practitioner (physiotherapists) over six weeks (trained by J.B.). As indicated during model development, 16 a flexible delivery approach was used with appointments lasting up to 1 hour, in the hospital or home setting and scheduled according to participant preference. Where possible, first appointments were face to face. Subsequent appointments were face to face or by telephone according to practical considerations and participant preference. The intervention used a psychologically informed approach 18 to identify immediate functional priorities and concerns, illness understandings and future expectations relating to functional well-being. An intervention manual (https://www.kcl.ac.uk/cicelysaunders/attachments/permalink/Integrated-Short-term-Rehabilitation-for-Thoracic-Cancer-Intervention-Manual) was used to standardize change processes 19 but was unscripted to enable tailoring and adaptation of intervention components to meet the expected variation in function-related needs. Inter-vention components were selected as indicated and included personalized information about the impact of thoracic cancer on function and goal planning for symptom prevention and/or self-management, graded physical activity, home-based exercise and participation and performance in activities of daily living.
Intervention components were delivered using behaviour change techniques 14 to support receipt and enactment. Information booklets, handheld fans and walking aids were offered and provided to support delivery of intervention components. An individual goal-orientated action plan, developed in consultation with each participant and held by them, was reviewed and updated at each session to support enactment. Participants were sign-posted to local hospital, community-based, hospice and charitable services (i.e. local cancer support organizations) as indicated in the manual and where available for on-going support. Those wanting to pursue supervised exercise training to improve fitness were signposted to local exercise services. At discharge, a letter summarizing the participant’s rehabilitation intervention and discharge action plan was sent to the participant and copied to their multiprofessional team for follow-up and onward referrals.
Our primary feasibility outcomes were rates of participant enrolment and retention. Feasibility endpoints, established a priori, were defined as ⩾30% of eligible patients consenting to the trial and ⩾50% of enrolled participants completing clinical outcome measures at 30 days. Secondary feasibility objectives were number of rehabilitation contacts delivered over 30 days, fidelity of service delivery, including use of intervention components and onwards referral to local rehabilitation services and missing data on clinical outcome measures at 30 and 60 days. Participant self-reported experiences were assessed by self-reported questionnaire comprising four items on trial processes from a national experience survey 20 and 10 items on satisfaction with the intervention from the Functional Assessment of Chronic Illness Therapy Treatment/Patient Satisfaction (version 4). 21 Free-text comments were also invited.
Clinical outcomes were assessed at baseline, 30 and 60 days following randomization via self-reported postal questionnaire. Higher scores are better for all measures except the Integrated Palliative Outcome Scale and the Client Services Receipt Inventory. Symptoms and concerns were measured by the Integrated Palliative Outcome Scale (17 items, total score 0–68); 22 physical activity level by the Physical Activity Scale for the Elderly (28 items, 0–400); 23 health-related quality of life measured by the Functional Assessment of Cancer Therapy (FACT) − Lung (total 34 item, 0–136; FACT − Trial Outcome Index (21 items, 0–84); FACT − lung cancer subscale seven items, (0–28); 24 EuroQoL EQ-5D-5L (index values −1 to 1, EQ-VAS 0–100); 25 and confidence measured by the Self-Efficacy Measure for Chronic Disease (6 items, 0–60). 26 The Client Services Receipt Inventory 27 was used to measure resource use relating to hospital and community services, including social care, informal care and equipment provision. No changes were made to outcome assessments during the trial.
As this trial was designed to assess the feasibility of testing the short-term integrated rehabilitation intervention, a formal power calculation around an estimated effect size on clinical outcome was not appropriate. Sample sizes of 24–60 participants have been recommended for feasibility studies. 28 , 29 We took a conservative approach and aimed to recruit up to 60 participants which would allow us to estimate feasibility parameters and outcomes with sufficient precision to inform a future sample size calculation.
Statistical analysis
Data were analysed using SPSS (version 24, Chicago, IL, USA) under intention-to-treat principles. Feasibility outcomes and baseline demographics were summarized using descriptive statistics. Data on treatment fidelity in the intervention group were extracted from case report forms using the Behaviour Change Technique Taxonomy (version 1) 30 by a trained member of the research team (J.B.). Treatment receipt was defined as the participant receiving 1–3 rehabilitation sessions comprising symptom management ± physical activity or exercise ± task performance and participation interventions. Reasons for withdrawal or loss to follow-up from the trial were summarized and classified by attrition due to death (ADD), attrition due to illness (ADI) or attrition at random (AaR). 31 The proportions of participants missing each variable were summarized by group at each time point. All serious adverse events (SAEs) and adverse events (AEs) relating to the intervention were summarized. This trial did not aim to evaluate effectiveness; therefore, clinical outcomes were described by trial group at baseline and both follow-up time points, using standard descriptive statistics, without significance testing.
Results
Figure 1 shows participant flow through the trial. Between February 2018 and January 2019, 374 patients were screened, of whom 159 (42%) were eligible and 54 (34%) were enrolled. An overall recruitment rate of 4.5 participants per month was achieved with 1–2 accruals per month at each site. Barriers to additional recruitment included personnel absences in the clinical and research teams and changes to site working practices, for example, availability of lung cancer nurse specialists and allocation of space in oncology clinics. Following randomization, 82% and 72% of participants returned follow-up outcome measures at 30 and 60 days, respectively. Attrition was comparable across both groups. In the rehabilitation group, one participant withdrew before receiving the intervention due to rapidly progressing disease and one was lost to follow-up after receiving one rehabilitation contact. In the standard care group two participants were lost to follow-up and one withdrew from the trial. Postal questionnaires from four participants who remained in the trial (three rehabilitation group and one standard care group) were not received at 30 days.
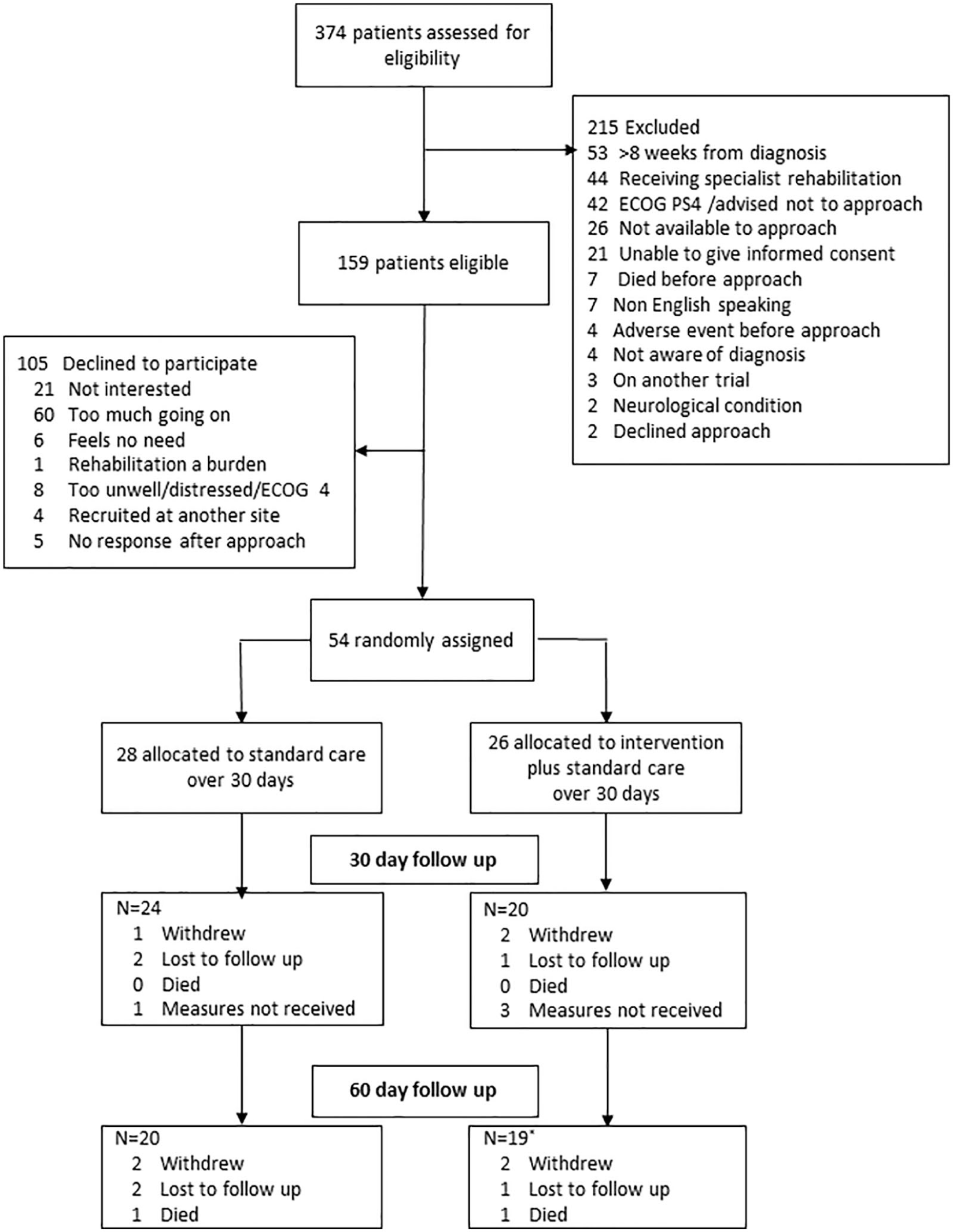
CONSORT flow diagram.
Participants had a median (range) age of 67 (44–85) years and 35 (65%) were men. Most were retired or not employed (32/54, 60%) though some were on sick leave (14/54, 27%) or still working (7/54, 14%). Less than one-quarter of participants lived alone. The majority 37/54 (68%) had non–small cell lung cancer (NSCLC), though small cell lung cancer (SCLC), pleural mesothelioma and neuroendocrine tumours were represented. A total of 39 (72%) participants had stage III–IV disease (27 metastatic), of whom more than half were scheduled for treatment with chemotherapy doublet combinations. Group allocation differences in mesothelioma diagnosis and disease stage were noted (Table 1).
Participant baseline characteristics.
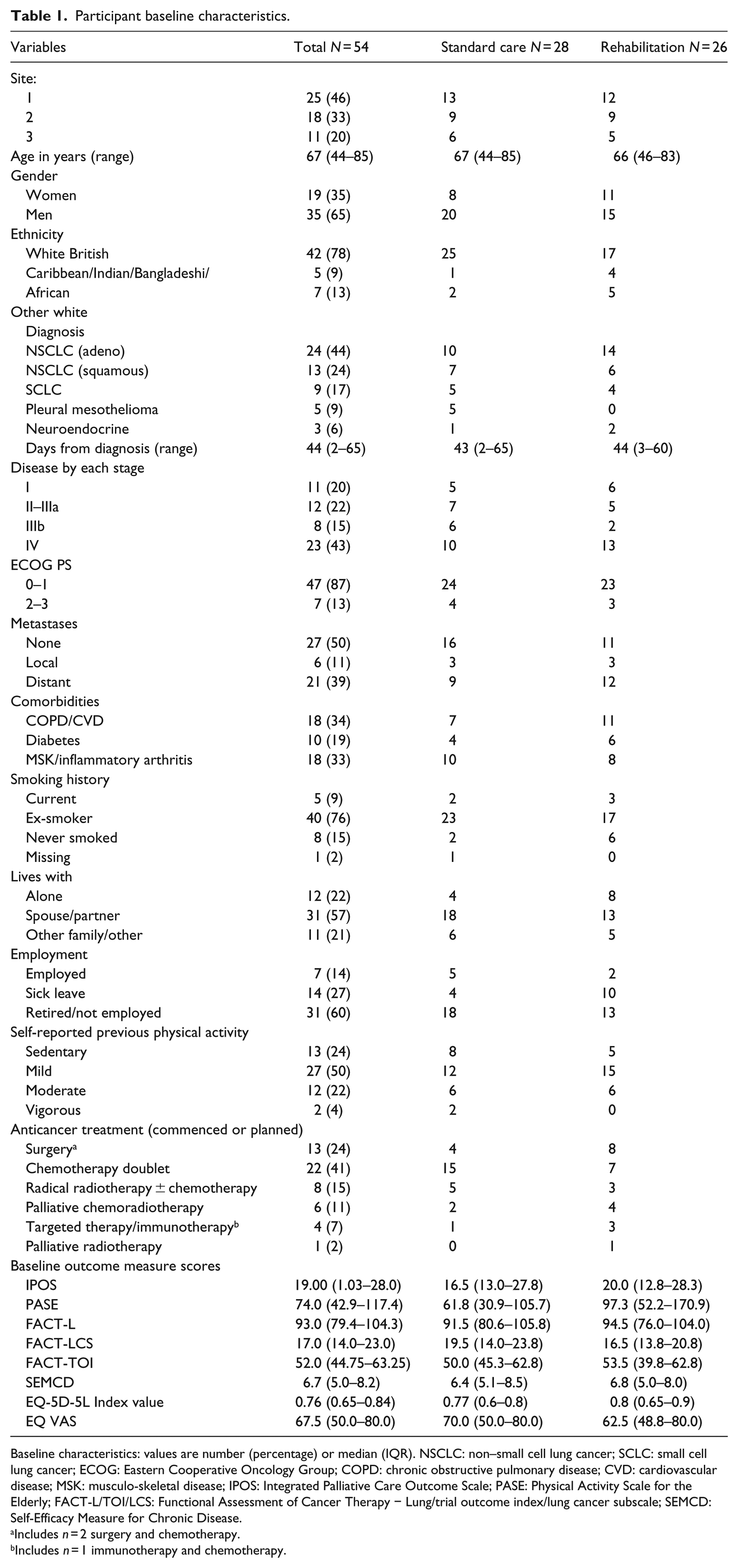
Baseline characteristics: values are number (percentage) or median (IQR). NSCLC: non–small cell lung cancer; SCLC: small cell lung cancer; ECOG: Eastern Cooperative Oncology Group; COPD: chronic obstructive pulmonary disease; CVD: cardiovascular disease; MSK: musculo-skeletal disease; IPOS: Integrated Palliative Care Outcome Scale; PASE: Physical Activity Scale for the Elderly; FACT-L/TOI/LCS: Functional Assessment of Cancer Therapy − Lung/trial outcome index/lung cancer subscale; SEMCD: Self-Efficacy Measure for Chronic Disease.
Includes n = 2 surgery and chemotherapy.
Includes n = 1 immunotherapy and chemotherapy.
Overall engagement with the rehabilitation intervention was high, and it was delivered according to protocol (Table 2). Across the 26 participants allocated to the intervention group, 69 rehabilitation sessions were delivered with a median of three per participant. 21 (84%) participants accessed all three rehabilitation sessions. Two-thirds of rehabilitation sessions were delivered face to face in the home; others occurred in hospital outpatient settings with a single session delivered on a hospital inpatient unit. The median duration of the first session was 1 hour and follow-up sessions, 45 minutes. Two participants declined further sessions, as they perceived no needs or were too busy with appointments, though both remained in the trial.
Intervention fidelity.
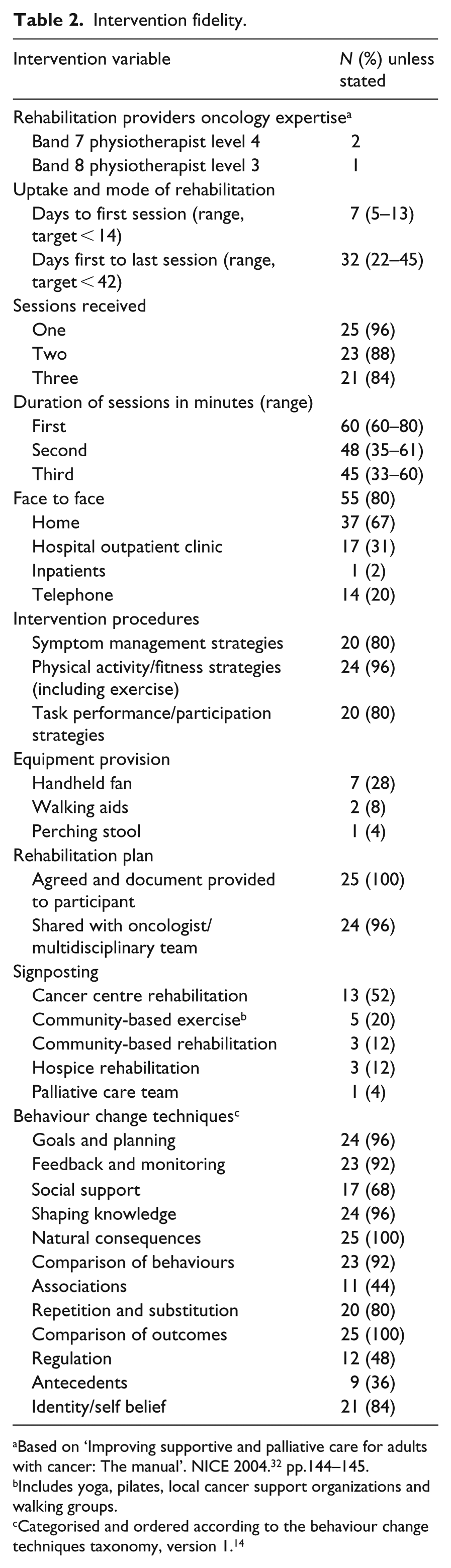
Based on ‘Improving supportive and palliative care for adults with cancer: The manual’. NICE 2004. 32 pp.144–145.
Includes yoga, pilates, local cancer support organizations and walking groups.
Categorised and ordered according to the behaviour change techniques taxonomy, version 1. 14
Most participants engaged with all core intervention components; physical activity and exercise (24/25, 96%), symptom self-management (20/25, 80%) and task performance/participation (20/25, 80%). Interventions frequently accepted by participants were home-based exercise or physical activity programmes and self-management strategies for fatigue and breathlessness. Few participants reported current problems managing personal activities of daily living, though 20/25 (80%) and 16/25 (64%) were provided with strategies to support work/leisure or domestic activities, respectively.
Regarding the use of behaviour change techniques, 14 ‘credible source’ and ‘information about health consequences’ were used to support intervention delivery in all participants (Supplementary Table 1). Behaviour-change techniques relating to goal setting, action planning, feedback and self-monitoring, instruction, practice and ‘verbal persuasion about capability’ were used with over three-quarters of participants. Strategies to reduce negative emotions supported intervention delivery and enactment of rehabilitation plans in 12/25 (48%) participants. Nine interventions delivered (9/26, 36%) included ‘adding objects to the environment’ (handheld fans and assistive devices), though restructuring of the physical and social environment did not take place. Evaluation of participant enactment of rehabilitation plans was clearly documented in most follow-up sessions.
No SAEs related to the intervention occurred. Two participants died following disease progressions, and seven participants were admitted to hospital relating to disease and oncology treatments (disease progression n = 3; sepsis, anaemia, pulmonary embolus, blocked stent, all n = 1). Six intervention group participants reported transitional worsening of symptoms following exercise or walking activities, two reported delayed onset muscle soreness and one had a non-injurious fall from a bicycle.
Rates of missing data items in returned questionnaires were low (Supplementary Table 2). Postal questionnaires from four participants who remained in the trial were not received at 30 days. One participant engaged with the intervention, but outcome measures were not received.
The item most frequently missed were FACT − Lung item ‘satisfaction with sex life’ (50%) and items in the Client Services Receipt Inventory relating to personal care (45%) and rehabilitation services (physiotherapy, occupational therapy and dietitian, 27%–36%). The Physical Activity Scale for the Elderly questionnaire allocates a score of −1 to a weighted domain containing missing items, so all obtained questionnaires were scored despite missing items in 6 (14%) and 5 (13%) questionnaires at 30 and 60 days, respectively.
Trial participation satisfaction was high in both groups (median 12) with a wider range of scores in the standard care group. Free-text comments from 15 participants described mostly positive experiences. Two intervention and three standard care group participants felt the questionnaires were too long or hard to fill in. Two standard care participants were unhappy with group allocation. Satisfaction with the rehabilitation intervention was also high with a maximum obtainable median score of 27 (range: 23–27). A total of 14 participants completed free-text comments describing the impact of the intervention and the involvement of family members during intervention delivery. Participants valued the practical advice and face-to-face contact, reporting that the experience had been ‘helpful’, ‘useful’, ‘educational’ and ‘empowering’. Two would have preferred more sessions. Nine commented that they valued involvement of a family member, while three reported feeling able to talk more freely without family member present.
Table 3 displays change in outcomes at 30 and 60 days. Baseline scores (Table 1) were comparable across both groups for all measures except the Physical Activity Scale for the Elderly, which indicated the rehabilitation group were more physically active. Overall, participants were generally sedentary, reported moderate symptom burden (Integrated Palliative Outcome Scale, median (interquartile range (IQR)) score: 19 (13–28)) and reported having confidence to manage their disease (Self-Efficacy Measure for Chronic Disease 6.7 (5.0–8.2)). Client Services Receipt Inventory data indicate that about half of all participants were receiving support with personal care.
Participant self-reported outcome data at 30 and 60 days: median (IQR).
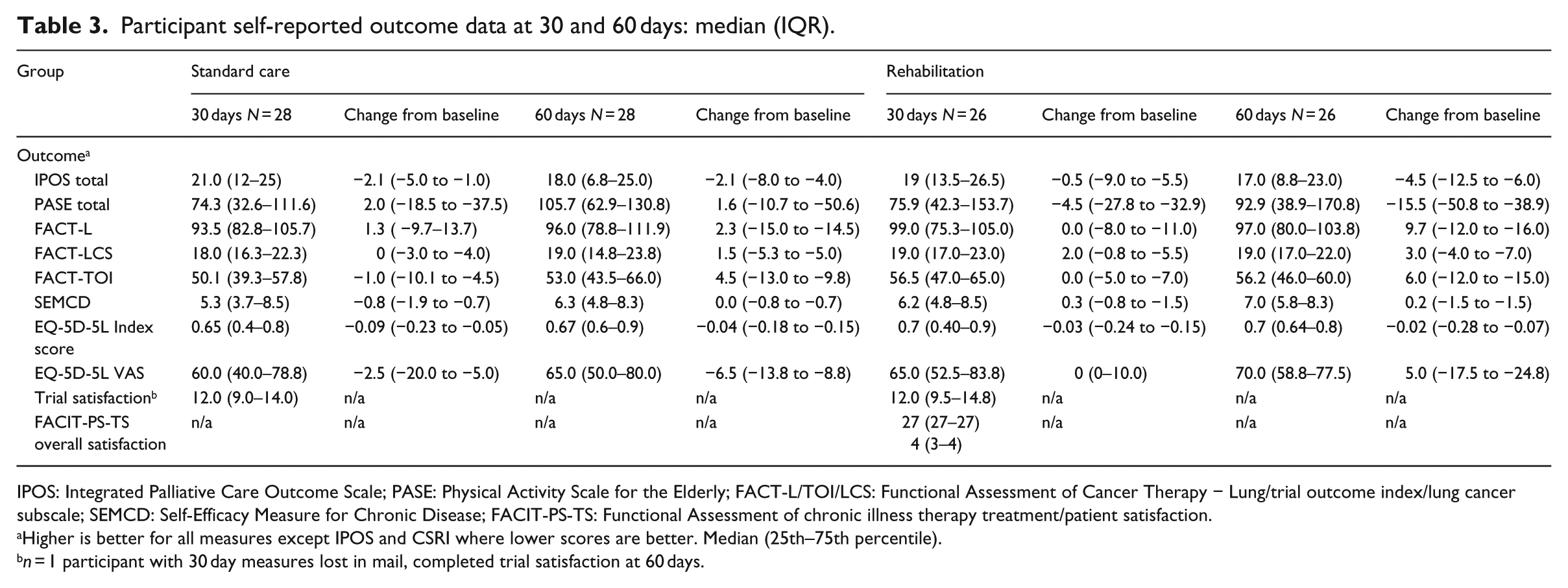
IPOS: Integrated Palliative Care Outcome Scale; PASE: Physical Activity Scale for the Elderly; FACT-L/TOI/LCS: Functional Assessment of Cancer Therapy − Lung/trial outcome index/lung cancer subscale; SEMCD: Self-Efficacy Measure for Chronic Disease; FACIT-PS-TS: Functional Assessment of chronic illness therapy treatment/patient satisfaction.
Higher is better for all measures except IPOS and CSRI where lower scores are better. Median (25th–75th percentile).
n = 1 participant with 30 day measures lost in mail, completed trial satisfaction at 60 days.
Changes over time were modest at both time points and a large degree of heterogeneity was evident (Table 3). Change was most apparent for physical activity level and health-related quality of life. Changes in Physical Activity Scale for the Elderly scores were small in both groups at 30 and 60 days, with slightly higher scores in the standard care group at 60 days (median (IQR) 1.6 (−10.7 to 50.6)) and worsening scores for rehabilitation at 60 days (−15.5 (−50.8 to 38.9)). This contrasted with health-related quality of life scores which favoured the rehabilitation group. At 60 days, FACT − Lung scores improved by a median of 9.7 (−12.0 to 16.0) compared to 2.3 (−15.0 to 14.5) with standard care. Similarly, the FACT − Trial Outcome Index rehabilitation group scores improved by 6 (−12 to 15.0) as compared to 4.5 (−13.0 to 9.8) with standard care. Despite comparable reductions in the EQ-5D utility index in both groups, a small worsening in EQ-VAS median score was observed in the standard care group at 30 and 60 days (−2.5 (−20.0 to 5.0) and −6.5 (−13.8 to 8.8)) as compared to no change then a small improvement (0 (0–10) and 5.0 (−17.5 to 24.8)) in the rehabilitation group. Symptoms reduced by a small amount at 30 days in both groups though by 60 days, scores had improved by a median (IQR) of −4.5 (−12.5 to 6.0) in the rehabilitation group and −2.1 (−8.0 to 4.0) in the standard care group.
Discussion
This trial has found that it is feasible to recruit and retain people newly diagnosed with thoracic cancer to a randomized controlled trial of short-term integrated rehabilitation versus standard care. Data relating to recruitment, retention and engagement with the rehabilitation intervention suggest that the trial was well designed and implemented and that this model of rehabilitation is acceptable and accessible for patients across a range of clinical and demographic characteristics. The primary feasibility outcomes were achieved: 34% of eligible participants were recruited and 82% were retained on trial for 30 days.
Low baseline levels of physical activity indicate that the sample was representative of the population. 33 Engagement with the rehabilitation intervention and intervention fidelity was high. More than 96% of participants allocated to receive rehabilitation accessed at least one session of rehabilitation, and more than 75% accessed each of the three core intervention components. Low levels of missing data in the clinical outcomes suggest that measures were acceptable to participants and have potential to be used in a future trial (see supplementary material). However, unclear or missing data in the self-reported Client Services Receipt Inventory domains relating to physiotherapy, occupational therapy, inpatient and outpatient rehabilitation meant that it was difficult to quantify and evaluate access to rehabilitation services. Participants rarely completed number of contacts, duration of intervention or provided information to enable assessment of contamination.
The trial did not aim to test effectiveness, and inferential statistical tests were not conducted. It is however of interest that changes in median scores at day 30 and day 60 were higher in the rehabilitation group for all measures except EQ-5D-5L index scores and Physical Activity Scale for the Elderly. Modest changes observed in clinical outcome measures were larger in FACT–Lung and EQ VAS. Changes in Physical Activity Scale for the Elderly scores were less than the minimally important difference for this population. 23 During development work, confidence was identified as a key modifiable factor regardless of participant disease stage or performance status; 16 however, minimal changes were observed in Self-Efficacy Measure for Chronic Disease scores.
This theory-based model of short-term integrated rehabilitation differs from other rehabilitation interventions tested in people with thoracic cancer in key areas. It brings together strategies to optimize physical function, symptom self-management and participation in valued daily activities. Rehabilitation interventions delivered following diagnosis have the potential to minimize the impact of disease and treatment-related symptoms, such as breathlessness and fatigue, on symptom experience, functional independence in activities of daily living and quality of life. 6 The majority of research studies focus on exercise interventions for people on curative treatment pathways. 9 Exercise was prescribed during short-term integrated rehabilitation when participants were willing to engage, but if not, other rehabilitation components, including preventive strategies were used to optimize physical activity levels and to minimize the onset of symptoms developing alongside physical deconditioning. Holistic breathlessness services improve distress relating to refractory breathlessness 10 but have not yet been tested in people mainly limited by exertional breathlessness, as reported by participants in this trial.
The trial has several strengths. First, we were able to recruit and retain participants with a diverse range of demographic characteristics, disease stage and comorbidities on all thoracic cancer treatment pathways. The recruitment and retention rates indicate that the trial design and research personnel were able to address some of the barriers influencing participation in rehabilitation and exercise-based interventions in people with thoracic cancer. 16 , 34 Few participants declined for reasons relating to rehabilitation being a burden or unnecessary as found in a large mixed-methods study, where receptiveness to rehabilitation was low across all participants with mild to severe levels of disability. 7 Most participants in this trial declined, as they had too much going on or were not interested; findings congruent with previous studies. Although continuing with normal life following diagnosis is important to patients, 5 it cannot be assumed that they will want to have any functional concerns met by health providers. Brown et al. 35 found that people with lung cancer may prefer to access functional support from their own family.
The trial has addressed uncertainties surrounding the delivery of rehabilitation interventions at a time when patients are coming to terms emotionally with their new life situation while undergoing a busy and potentially arduous oncology treatment schedule. 36 As prioritized in trial development work, 15 , 16 we were able to deliver and test an inclusive, flexible and tailored model of rehabilitation to address the heterogeneity of functional need. The model of short-term integrated rehabilitation echoes effective and valued components of holistic breathlessness services. It was delivered by an expert provider, integrated with busy treatment schedules and focused on participants’ immediate functional concerns and priorities. 10
The comparability of groups at baseline indicates that the randomization system and minimization categories worked well. However, all mesothelioma participants were randomized to receive standard care. In view of the changing treatment options and outcomes dependent on histological diagnosis, minimizing for diagnosis should be considered in a larger trial. Although the rehabilitation model was designed to be inclusive and accessible for participants with an Eastern Cooperative Oncology Group Performance Status of 0–3, it is disappointing that few disabled participants were recruited with most participants having an Eastern Cooperative Oncology Group Performance Status 0–1. The performance status of those declining to participate was not always available, so it is not known if participants with a performance status of 2–3 were approached and declined or if they were not identified during screening. Recruitment strategies in future trials need to consider how this group may be better represented in the sample, for example, asking people with a performance status of 2–3 to review trial recruitment materials and processes.
The constraints of delivering the intervention in a feasibility trial meant that integration with other oncology services was harder to achieve than was anticipated. To optimize accessibility and to reduce participant burden, we aimed to deliver the intervention alongside scheduled hospital appointments. This presented challenges as intervention providers were based off site, and scheduled hospital appointments were frequently booked or changed at short notice. Attendance at thoracic cancer multiprofessional team meetings across three sites was not possible with the available trial personnel. Changes in working practices at two hospital sites meant clinic space was not always available. In addition, some participants had gaps between appointments longer than the six-week intervention delivery period. Delivering the intervention in the hospital setting was more achievable when participants were attending for daily radiotherapy or weekly chemotherapy. Some participants treated with surgery lived too far for home visits and had no postoperative appointments within the trial period and were therefore unable to enroll in the trial. Other integration strategies were achieved. These included providing participants with a written rehabilitation plan which they were encouraged to share with other healthcare professionals involved in their care. A discharge letter summarizing the intervention and rehabilitation plan was sent to each participant on discharge and copied to their oncologist and case-notes.
The findings of this feasibility trial have implications for future research and clinical practice. High levels of participant retention, intervention fidelity and rates of data completeness with few non-SAEs suggest that the trial processes, intervention and outcome measures were acceptable to participants. Training members of the usual healthcare team in screening for and delivering the intervention in a full trial should improve capacity to deliver the intervention alongside schedules appointments and reduce performance bias. The design of a full trial should consider how to reach participants with Eastern Cooperative Oncology Group Performance Status 2–3 and those living further away from the recruiting centres.
Identifying a primary outcome for trials of rehabilitation interventions in this population is challenging, limited in part by the availability of suitable measures. 37 The findings suggest that the more discrete measures (physical activity and confidence) were not relevant to all participants. The inclusive approach to eligibility, heterogeneity of the population, bi-directionality of functional trajectories, mean that the health-related quality of life measure is more able to capture the impact of the short-term integrated rehabilitation intervention and should be considered as primary outcomes for a future trial. This is in line with the findings of a recent trial of home-based rehabilitation for people with inoperable lung cancer. Edbrooke et al. 37 observed significant improvements in health-related quality of life and symptom levels with no changes in the primary outcome, physical function as measured by the 6-minute walking test.
An estimated sample size for a future trial was calculated based on the observed changes in FACT–Lung. Assuming a difference of 6 points, which is similar to the point estimate of effect we observed, and allowing for 25% attrition, 336 participants would be required to reliably detect this difference (80% power, P = 0.05) in an efficacy trial.
If shown to be effective, this model of rehabilitation would provide proactive support around the time of diagnosis for people with thoracic cancer. It would provide a route to consecutively screen patients and shift the focus of rehabilitation towards self-management and maintaining rather than regaining function. Furthermore, it can contribute to the integration of rehabilitation into oncology services.
This study has found that it is feasible to deliver and test a new, theory-based model of rehabilitation that differs from exercise interventions typically tested in people newly diagnosed with thoracic cancer. It is an inclusive intervention which addresses the heterogeneity of functional need and barriers to rehabilitation observed in people newly diagnosed with thoracic cancer. We were able to deliver and test the new model in a feasibility trial, and efficacy testing is now warranted.
Clinical messages
It is feasible to deliver and test short-term integrated rehabilitation for thoracic cancer in a randomized controlled trial in the period following diagnosis.
A sample size of 336 would be needed to detect a clinically important difference in health-related quality of life in an efficacy trial.
Supplemental Material
Supplemental_Material – Supplemental material for Short-term integrated rehabilitation for people with newly diagnosed thoracic cancer: a multi-centre randomized controlled feasibility trial
Supplemental material, Supplemental_Material for Short-term integrated rehabilitation for people with newly diagnosed thoracic cancer: a multi-centre randomized controlled feasibility trial by Joanne Bayly, Lucy Fettes, Eleanor Douglas, Maria J Teixiera, Nicola Peat, India Tunnard, Vishit Patel, Wei Gao, Andrew Wilcock, Irene J Higginson and Matthew Maddocks in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors would like to thank all the people who participated in the trial and their families. They thank members of the Cicely Saunders Public and Patient Involvement Forum for their involvement during the development and conduct of this trial. In particular, they would like to thank Lesley Smith, for her insightful contributions to the design of the participant information leaflets and for her attendance and input at the research ethics committee meeting. They thank Evelyn Burssens, Cathann Manderson, Sarah Schofield, Param Kaler, Alexander Chan, Pippa Labuc, Faye Dickinson and clinicians at the three sites for their support with screening and recruitment and Fern Brookes for supporting trial administration.
Authors contributions
J.B., M.M., I.J.H. and A.W. initiated, designed and obtained funding for the trial; J.B. had overall responsibility for the conduct of the trial under the supervision of M.M., I.J.H. and A.W.; J.B., L.F., E.D. M.J.T. and IT undertook data collection; J.B., M.M. and W.G. designed the statistical analysis which was undertaken by J.B. under the supervision of M.M., W.G. with support from V.P. J.B. wrote the manuscript and all co-authors contributed to critically revising it.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: J.B. is funded by a National Institute for Health Research (NIHR) Clinical Doctoral Research Award (ICA-CDRF-2015-01-008) for this research project. M.M. is supported by an NIHR Career Development Fellowship (CDF-2017-10-009) I.J.H. is an NIHR Emeritus Senior Investigator. This research was supported by the National Institute for Health Research Collaboration for Leadership in Applied Health Research South London (NIHR CLAHRC South London), now recommissioned as NIHR Applied Research Collaboration South London. This publication presents independent research. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Data accessibility statement
Data will be made available on request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.