
Abstract
Purpose:
Approximately 20% of the children and adolescents after mild traumatic brain injury will not fully recover. They suffer long-term postconcussive symptoms and may experience limitations in activities and participation. Research suggests that early psychoeducational interventions may prevent long-term postconcussive symptoms. The Brains Ahead! intervention was developed to prevent long-term symptoms and, furthermore, to establish a more successful return to activities and participation after mild traumatic brain injury in children and adolescents. The intervention is currently being evaluated in a multicenter randomized controlled trial.
Rationale:
Providing individualized information and personal advice in addition to standardized information about the injury and possible consequences early after the injury may enable patients and caregivers to recognize and anticipate on relevant symptoms at an early stage and to prevent problems in activities and participation.
Theory into practice:
The Brains Ahead! intervention is a psychoeducational intervention for children and adolescents who sustained a mild traumatic brain injury and for their caregivers. The patients will receive a partially standardized and partially individualized psychoeducational session and a telephone follow-up within the first two to eight weeks after the injury.
Introduction
Mild traumatic brain injury is the most common cause of acquired brain injury among children and adolescents. There is no international consensus on structural follow-up by a (paediatric) neurologist or rehabilitation physician for this group of patients, despite the fact that approximately 20% of them suffer at long term from a variety of symptoms in the physical, cognitive, emotional or behavioural domains.1–4 As a consequence of these postconcussive symptoms, children may develop limitations in activities and participation, for example, in school and social relations in the long term.5–7
Several studies indicate that early education, reassurance and even early cognitive behavioural approaches may be effective in preventing long-term problems after traumatic brain injury in both children and adults8–10 and, more specifically, after mild traumatic brain injury.11,12 The few available studies including interventions (e.g. psychoeducation) intended to prevent postconcussive symptoms in children and adolescents report positive results. However, these studies are either retrospective or lack a randomized controlled trial design.12–15
We have recently developed the Brains Ahead! psychoeducational intervention. To the authors’ knowledge, this is the first intervention that prospectively intends to prevent long-term problems related to activities and participation in children and adolescents aged 6–18 years following mild traumatic brain injury. 15 The Brains Ahead! psychoeducational intervention combines an inventory of symptoms, psychoeducation and follow-up and involves the child’s family in the process.
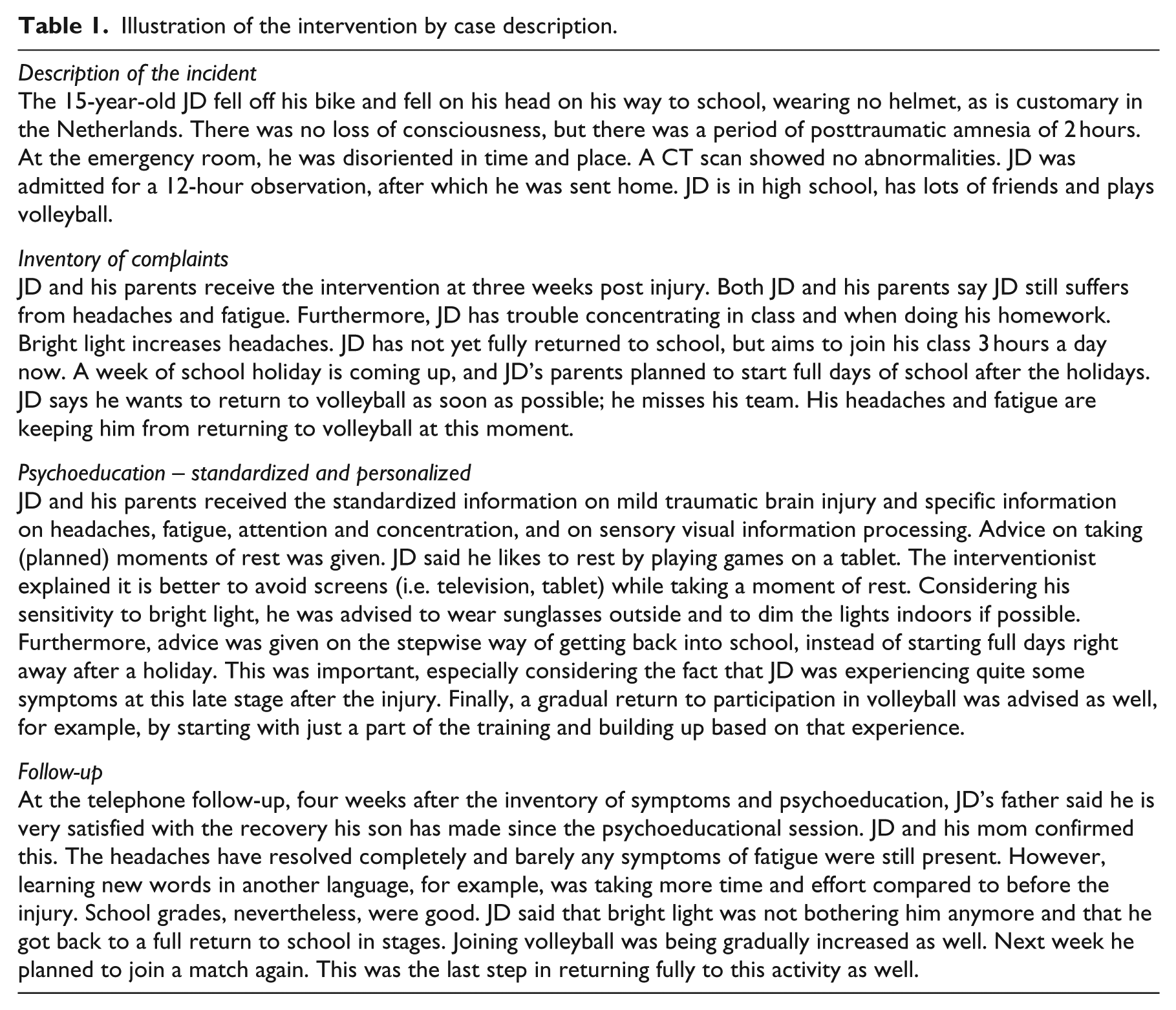
The Brains Ahead! intervention study is part of a larger cohort study with a nested randomized controlled trial. 16 The medial ethics committee of Erasmus University Medical Centre, Rotterdam, and all of the local committees of the participating hospitals approved the study protocol (MEC-2015-047, NL51968.078.14). The study is registered in the Netherlands Trial Register (NTR5153). In this article, the theoretical basis and content of the Brains Ahead! treatment protocol for children and adolescents after mild traumatic brain injury and their primary caregivers are described. The TIDieR checklist for describing interventions was used to structure the article (see Online Appendix 1). Also, a patient case is described to illustrate the intervention (Table 1). Results of this intervention study will be published when the trial is finished.
Illustration of the intervention by case description.
Rationale
Evidence suggests that information and education should always be offered following mild traumatic brain injury in general. Ideally, it should be followed by consultation in which personalized reassurance is given. 15 Therefore, the Brains Ahead! intervention consists of the following three components: (1) inventory of symptoms, (2) psychoeducation and (3) follow-up. Hereafter is explained why these three components were chosen.
After mild traumatic brain injury, most children and their primary caregivers leave the emergency department or the general doctor’s office at best with a leaflet explaining what postconcussive symptoms are in general terms and that these may persist for some time. Structural individual follow-up is almost never offered. Because of the high prevalence of mild traumatic brain injury, a general follow-up guideline for all children could lead to overtreatment, considering that 80% has no persistent postconcussive complaints or symptoms.1–4 However, a not to be neglected 20% of children and adolescents do have lasting and often debilitating postconcussive complaints or symptoms.1–4 For this reason, a stepwise approach in order to identify the children and adolescents that need treatment is urgently needed. 15 The first step in this approach is to explore the symptoms a child may experience after mild traumatic brain injury, for example, using an inventory of symptoms containing the most common symptoms after mild traumatic brain injury, based on the literature.17–24
With regard to treatment, previous intervention studies12,14,15,25–30 consisting of psychoeducation were found to be effective in preventing long-term postconcussive symptoms and functional problems after mild traumatic brain injury in adults and children. A study on long-term problems after mild traumatic brain injury in adults demonstrated that the effect of the education was most profound when administered at the earliest possible stage. 31 The studies that apply these interventions to children have been performed with other patient groups, for example, children with only sports-related concussions,32,33 or more severe brain injuries, 34 or they were limited to case reports. 33 Also, some interventions were focused on preventing long-term postconcussive symptoms and resolving existing postconcussive symptoms and not on preventing problems in activities and participation for children with mild traumatic brain injury.12,15,29,30,35 Despite these limitations, the results of these psychoeducational intervention studies are very promising with respect to decreasing postconcussive symptoms in children with mild traumatic brain injury.9–12,30
The World Health Organization Collaborating Centre for Neurotrauma Task Force on Mild Traumatic Brain Injury developed guidelines for the content of psychoeducational interventions, such as standardized information about diagnosis, incidence, risk factors, prevention, prognosis and treatment. In addition, they advise that the intervention should also contain individualized information. However, an overload of information makes it difficult to determine what is specifically important. 36 Furthermore, misunderstanding of information may result in anxiety and keeping the child off activities, while a stepwise return to activities in the first days after mild traumatic brain injury was found to have positive effects on participation in the long term. 37 For this reason, information should be relevant to the child’s injury and symptoms and appropriate for the child’s age and situation. 36 Information that is provided verbally, on the day of the injury and in the first days after, is often less well absorbed by caregivers. 12 For this reason, verbal information should be given two or three weeks after the injury, and written information and instructions should be provided additionally.12,36
Caskey and Nance 38 describe a study in which children with mild traumatic brain injury were routinely scheduled for an outpatient follow-up two weeks after the injury. During that visit, postconcussive symptoms were assessed and patients were referred to specialists if needed. The authors describe that patients and their caregivers often were non-compliant with the scheduled follow-up, despite the experience of ongoing persistent symptoms. 38 Possibly, an outpatient follow-up is too time-consuming and less flexible, in comparison with telephone counselling. A follow-up contact by telephone during the first three months post injury was found to be effective in reducing symptoms in children aged 16 years and older and in adults after mild traumatic brain injury. 39 More recently, Nowacki et al. 40 also found effective results after such a follow-up six weeks after mild traumatic brain injury, in children aged 4–18 years.
In summary, all described interventions are mostly directed towards the reduction of postconcussive symptoms and to a lesser extent to improvement in activities and participation. The psychoeducational part of the Brains Ahead! intervention provides standardized and personalized information on how to deal with symptoms after mild traumatic brain injury and advice on the stepwise return to participation in activities is provided. We expect that our approach prevents postconcussive symptoms over the long term and will have a positive effect on the improvement of activities and participation after mild traumatic brain injury. 15
Procedures
In order to illustrate the use of the intervention in practice, we described the case of JD and his parents who underwent the intervention as part of the randomized controlled trial (Table 1). Signed informed consent for participation in the intervention study was received as well as additional consent for this anonymized use of the description of their experiences throughout the intervention procedure. The characteristics of the Brains Ahead! intervention, including timeline, components, content and duration per component, are presented in Table 2. Further details on the study design and procedures are published elsewhere. 16
Characteristics of the Brains Ahead! intervention.
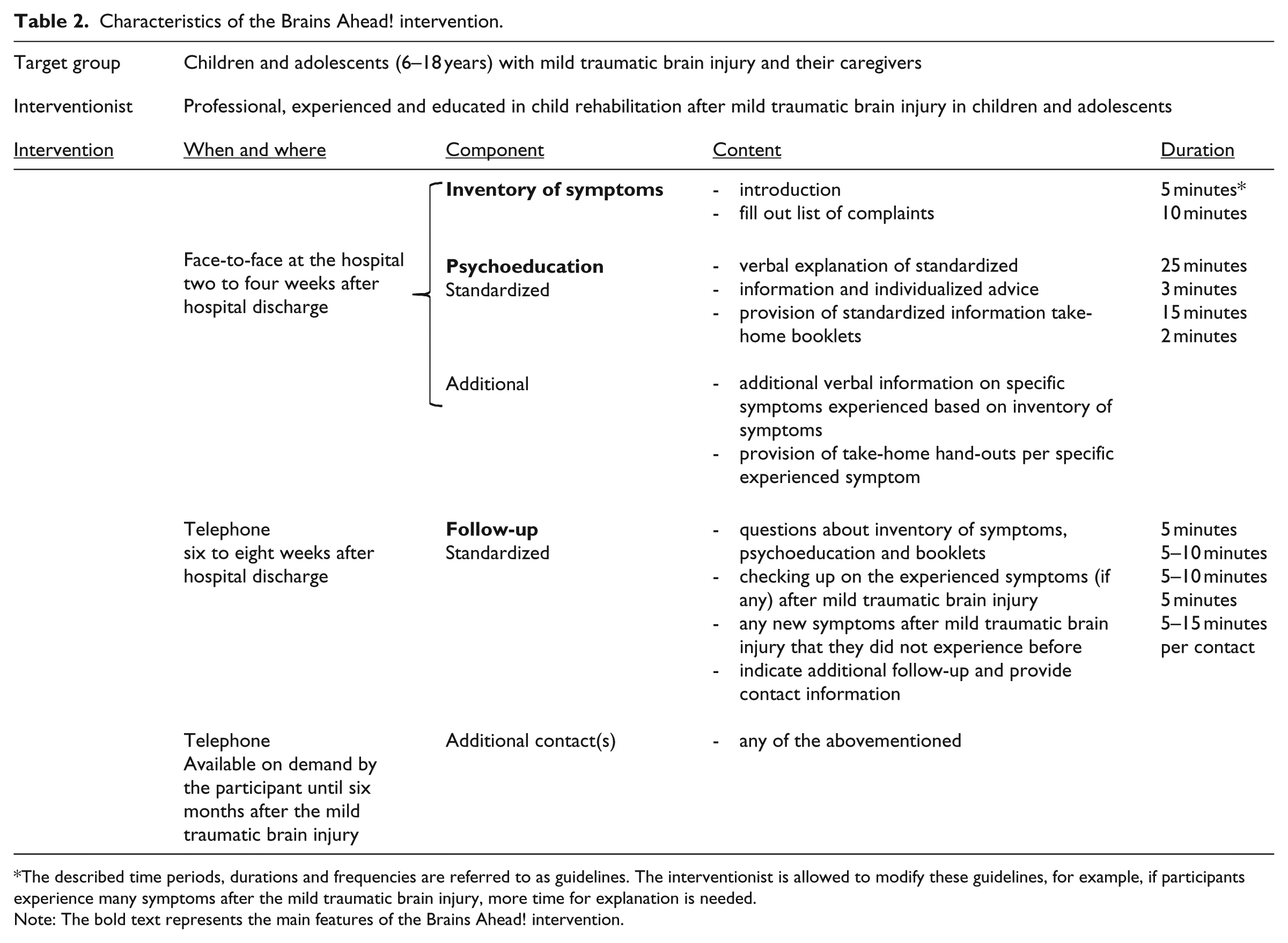
The described time periods, durations and frequencies are referred to as guidelines. The interventionist is allowed to modify these guidelines, for example, if participants experience many symptoms after the mild traumatic brain injury, more time for explanation is needed.
Note: The bold text represents the main features of the Brains Ahead! intervention.
Target group
The intervention is designed for children and adolescents aged from 6 to 18 years, diagnosed with mild traumatic brain injury at the emergency room, and their caregivers. In this study, the intervention was offered to patients from two participating centres (Erasmus University Hospital, Rotterdam, and Amphia Hospital, Breda). The caregiver was defined as a parent or guardian. Diagnosis of mild traumatic brain injury is based on the criteria established by the American Congress of Rehabilitation Medicine and the World Health Organization Collaborating Centre for Neurotrauma Task Force on Mild Traumatic Brain Injury 41 (see ref. 41, p.266).
Materials
The psychoeducation is administered using a presentation on a laptop and a standardized booklet containing information to take home. There is a booklet for parents, a booklet for children aged 6–12 years and a booklet for children aged 12–18 years.
Location and therapist
The inventory of complaints and psychoeducational session takes place in the hospital where the child was seen on the emergency department at the time of the injury. The intervention is administered by a professional, experienced and educated in paediatric rehabilitation after mild traumatic brain injury in children and adolescents.
Treatment sessions
Session 1: inventory of complaints and psychoeducation
The goal of the inventory of symptoms is to enable focused psychoeducation with additional information on postconcussive symptoms that the patient may experience. A list of common symptoms after mild traumatic brain injury, based on the most common symptoms after mild traumatic brain injury according to the literature,17–24 is discussed with the child and his or her caregivers in order to discover what is relevant (e.g. does the child experience this symptom or not) for the child’s personal situation. The list contains the following symptoms: (1) headache, mental fatigue, sleep, tension and stress; (2) difficulties with attention and concentration; (3) impaired efficiency and speed of information processing; (4) difficulties learning new information; (5) impaired memory; (6) difficulties with movement (motor skills and balance); (7) difficulties with executive skills (planning, impulsivity); (8) changes in personal and social skills; (9) changes in language and speech and (10) impaired use of senses (seeing, hearing, feeling, smelling and tasting).
The aim of the psychoeducation is to provide information and advice about mild traumatic brain injury as well as to prevent long-term problems in activities and participation. Psychoeducation contains standardized information on the causes, incidence and possible consequences of mild traumatic brain injury, information and advice about returning to activities and participation, sensory sensitivity and load-bearing capacity after mild traumatic brain injury, and is based on the literature.1,9,11,12,15,29,36,39 The information is administered verbally by the interventionist and is the same for every participant. This standardized information is also given to the participants in a booklet to take home. There are three versions of the booklet: one for the caregivers, one for children aged 6–12 years and one for children aged 12–18 years.
To individualize the treatment, customized information is provided by the interventionist. In case the child experiences symptoms after the mild traumatic brain injury – based on the inventory of symptoms – additional information, specific to these symptoms, is given, both verbally and on paper. For every individual symptom, standardized information is available. Furthermore, individualized advice can be provided on returning to activities and participation, based on the individuals’ daily life and goals, such as returning to school, sports and hobbies or work.
Session 2: follow-up
The aim of the follow-up is to provide customized treatment, based on the individual questions of participants and possible symptoms the patient may be experiencing after mild traumatic brain injury, without overloading them with excessive information.
During the standardized follow-up by telephone, the interventionist asks participants whether there are any questions about the inventory of symptoms and information that was given during the psychoeducation. Furthermore, the interventionist inquires about specific symptoms experienced (if any) after the mild traumatic brain injury. In case new common postconcussive symptoms have occurred, participants receive a short explanation on these symptoms by telephone and are sent extra standardized information about these specific symptoms. In cases where there was doubt about the relation between the mild traumatic brain injury and the new occurring symptoms, participants were advised to consult their general practitioner.
Additional session(s)
The additional follow-up can be used by participants on their own initiative. Based on the fact that 20% suffer from long-term symptoms after mild traumatic brain injury, this follow-up was offered as an option for avoiding overtreatment. The interventionist can be contacted by email for this additional follow-up, for example, in case new symptoms occur, or if questions about the consequences of mild traumatic brain injury arise at a later stage after the standardized follow-up. The interventionist responds within two workdays after receiving the email. The interventionist registers the number and content of the additional follow-up contacts. There is no limit on the number of additional follow-up contacts. However, the interventionist advises the participant and caregivers to contact their general practitioner when four additional follow-up contacts occur – or earlier, based on professional, clinical opinion.
Practical issues
The intervention has been developed in such a way that – if the intervention is proven to be effective – it can easily be implemented in hospital discharge routines and also in general practices. However, time consumption and cost-effectiveness issues may affect the implementation of the intervention, especially in the emergency room.
Discussion
To our knowledge, the Brains Ahead! intervention is the first standardized psychoeducational intervention combined with an individual approach and follow-up for children and their caregivers, provided at an early stage after mild traumatic brain injury in order to help prevent long-term problems concerning activities and participation.
The early stage after injury at which the intervention is administered may help answer questions about what patients and their caregivers may expect after a mild traumatic brain injury and prevent the patient from experiencing long-term symptoms after the injury and from making steady progress towards a full return to school and other activities and is, therefore, considered a strength of the intervention.42–44 Another strength of the intervention is that it is designed to meet patients’ individual needs. Patients and their caregivers are protected from an information overload and receive enough individualized information to guide them in the first period after mild traumatic brain injury.
The usual care in many countries for children with mild traumatic brain injury consists of short hospitalization or immediate discharge. 45 At discharge, they often receive a concise information brochure to take home, with recommendations to return to the general practitioner or hospital in case of frequent vomiting, increasing drowsiness and/or an increase in other complaints during the following days. 16 In comparison with this usual care, the Brains Ahead! intervention is more time-consuming and labour-intensive. However, if this approach proves to be effective, a web-based psychoeducational intervention with optional features in order to meet the child’s personalized needs may provide a solution for this in the future. The age of the target group of the Brains Ahead! intervention was set at 6–18 years, because one of the main purposes of our study was to examine the effects of the intervention on activities and participation both from the parental perspective and from the child’s perspective. 16 If we would have included younger children, we could not use our selected outcome measures. This may be considered a limitation since it reduces generalizability for its use in younger children. One might want to examine the effects of the intervention for children aged 0–6, which seems quite possible when administering the intervention to the caregiver only and measuring outcome in the caregivers only considering the level of understanding of the child itself. We recognize that some patients may not need an intervention after mild traumatic brain injury, because approximately 80% may not experience any symptoms at all. However, around 20% may suffer from symptoms at six months post injury and beyond, related to reduced activities and participation.1–4 Therefore, another part of the Brains Ahead! study is to investigate the possible predictive factors for outcome after mild traumatic brain injury and to identify which patients are at risk for long-term problems. The results of the Brains Ahead! study on the possible predictive factors for outcome after mild traumatic brain injury, the effectiveness of the intervention and the evaluation of the intervention process will be presented in ensuing papers.
Clinical message
The Brains Ahead! intervention combines an inventory of symptoms, standardized and personalized psychoeducation and follow-up and involves the child’s caregiver in the process.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Johanna Kinderfonds (Award Number 2012/0040-1552) and the Revalidatiefonds (Award Number R2012175).