
Abstract
Objective:
To analyze cost-effectiveness of Pain Exposure Physical Therapy compared to conventional treatment alongside a randomized controlled trial (NCT00817128) in patients with complex regional pain syndrome type 1, where no clinical difference was shown between the two groups in an intention-to-treat analysis.
Design:
Randomized controlled trial with 9 months follow-up.
Setting:
Patients were recruited from hospitals and general practitioners in the region around a university hospital.
Subjects:
A total of 56 patients, 45 (80.4%) female, were randomized. About 4 patients in the intervention and 11 patients in the conventional group switched groups. The mean (SD) age was 44.3 (16.6) years, and in 37 (66.1%) patients, the upper extremity was affected.
Interventions:
Patients received either Pain Exposure Physical Therapy (maximum of five sessions), or conventional treatment conforming with the Dutch multidisciplinary guideline.
Main measures:
For the economic evaluation difference between the groups in health-related quality of life (quality-adjusted life years (QALYs)), and the clinical outcomes Impairment level Sum Score—Restricted Version and Pain Disability was determined based on the intention-to-treat analysis as well as differences in both healthcare-related costs and travel expenses. Cost-effectiveness planes were constructed using bootstrapping to compare effects and costs.
Results:
No significant effects were found for QALYs (mean difference = −0.02; 95% confidence interval (CI) −0.10 to 0.04) and clinical outcomes. A cost minimization analysis showed a significant difference in costs between groups. The conventional treatment was 64% more expensive than the Pain Exposure Physical Therapy.
Conclusion:
This economic analysis shows that Pain Exposure Physical Therapy compared to conventional treatment is cost-effective.
Introduction
A randomized controlled study published in 2015 found no clinical difference between two different types of treatment for people with complex regional pain syndrome type 1, 1 but we did observe a difference in the use of healthcare resources. Because currently there is no effective management available, less economic costs with comparable outcomes are relevant and interesting.
Complex regional pain syndrome type 1 is a debilitating condition that usually develops following injury, but can also arise spontaneously. 2 The disorder is characterized by pain and sensory, autonomic, motor, and/or trophic changes. 3 There is emerging evidence that pain-related fear and avoidance behavior can lead to disease deterioration and the development of chronic pain-related disability.4,5 Despite elaborate research, treatment of complex regional pain syndrome type 1 can still be disappointing and there is a need for more high-quality evidence for the effectiveness of most therapies.6,7
In the present randomized controlled trial, we compared a Pain Exposure Physical Therapy approach to the Dutch conventional guideline-based treatment in patients with complex regional pain syndrome type 1. 1 The guideline includes pharmacological interventions with various drugs and intensive pain-contingent physical therapy sometimes taking a few months or even years. Key element of the Pain Exposure Physical Therapy intervention is to stimulate the use of the affected extremity while simultaneously ignoring the pain.1,8 Although we found no difference in clinical effect between both interventions we expected that early and forced use in daily life, without the use of medication, would lead to lower costs.1,9,10 Pain Exposure Physical Therapy follows a time-contingent treatment scheme with a maximum of five treatment sessions.
Complex regional pain syndrome type 1 is a very costly disorder. Annual costs for chronic regional pain syndrome type 1 in the Netherlands have been estimated between €32.5 million and €47.3 million, including medical costs as well as nonmedical costs and costs of lost productivity.11,12 With this particular study, we investigated the potential cost-effectiveness of Pain Exposure Physical Therapy versus conventional treatment. 8
Methods
Study design and participants
This economic evaluation was conducted alongside a randomized controlled trial with 9 months follow-up.1,8 This trial was prospectively registered at http://www.clinicaltrials.gov, NCT00817128, and at http://www.trialregister.nl, NTR 2090. The study was approved by the regional ethical committee (ABR no: NL24762.091.08).
The design of the trial and the primary clinical results are published elsewhere. 1
The cost data were collected after completion of the trial. Patients were recruited from hospitals and general practitioners in the region of the Radboud University Medical Center, in Nijmegen, The Netherlands. Recruitment took place from January 2009 until June 2011. Patients were included if they fulfilled the diagnostic criteria for complex regional pain syndrome type 1 as proposed by Harden et al., 13 age between 18 and 80 years, and first assessment between 3 and 24 months after the inciting event. Patients were excluded if they had complex regional pain syndrome type 1 in more than one extremity, a relapse of complex regional pain syndrome type 1, impairments of the contralateral extremity or prior sympathectomy of the affected extremity, or when they were pregnant or lactating. We used the Consolidated Health Economic Evaluation Reporting Standards Checklist to report the economic analysis. 14
Interventions
Patients were randomly allocated in a 1:1 ratio to receive either Pain Exposure Physical Therapy consisting of a maximum of five physical therapy sessions or conventional guideline-based treatment. More details on the interventions can be found elsewhere.1,9,10,15
Outcome measures
Costs
Cost categories were defined as direct costs, which were healthcare-related costs and travel expenses. These categories included physical therapy consultations, both as part of the allocated intervention and as outpatient physical therapy consultations, general practitioners consultations, consultations of the Pain Treatment Center at our university hospital, consultations of other healthcare providers (e.g. podiatrists, anesthesiologists for Transcutaneous Electrical Nerve Stimulation), medication costs, and travel expenses. Only the costs directly related to the treatment of complex regional pain syndrome type 1 were incorporated in the analyses. Volumes of care were measured using the electronic patient record system and patients’ medical records. Associated costs were verified with individual information from health insurance companies, after patients had given written consent for this. Cost prices were determined using standard unit cost prices according to the Dutch guidelines for costing research and the currency was euro. 16 Travel expenses were calculated by multiplying the total traveled distance from home to the healthcare provider with the standard travel expense rate.
Health-related quality of life
Health-related quality of life was measured with the EuroQol-5D-3 L (EQ-5D), 17 a validated so-called health-related quality-of-life instrument. 18 This instrument is available in a validated Dutch translation. 19 The EQ-5D is a generic health-related quality-of-life instrument comprising five domains: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. The EQ-5D index is obtained by applying predetermined weights to the five domains. This index gives a societal-based global quantification of the patient’s health status on a scale ranging from 0 (death) to 1 (perfect health). Patients were asked to rate their overall health-related quality of life on a visual analog scale consisting of a vertical line ranging from 0 (worst imaginable health status) to 100 (best imaginable).
We converted the EQ-5D score into a utility score using the Dutch algorithm. The utility score has a maximum of 1, indicating optimal health. A utility score of 0 equals death, but the score can also be negative, as some conditions are thought to be worse than death. By multiplying the utility score with the amount of time in which the score is applicable and then aggregate these scores over the relevant timeframe (trapezium method), quality-adjusted life years (QALYs) can be computed. 20
Clinical measurements
We measured the severity of complex regional pain syndrome type 1 using the Impairment level Sum Score—Restricted Version (range of 4–40, with a lower score indicating less impairment), which consisted of three measurement parameters focusing on typical signs and symptoms (pain, active range of motion, and temperature). 21 Pain Disability was measured using the Pain Disability Index. This is a widely used questionnaire for measuring disability related to musculoskeletal pain. It is a seven-item questionnaire with a score ranging from 0 to 70 points that assesses to which extent daily activities are disrupted by pain. A lower score indicates less disability. 22
Data analyses
We analyzed the data according to the intention-to-treat principle. Differences in costs between treatment groups were calculated using a generalized linear model with a log link function and with a gamma distribution to account for skewness in the data. For analyzing health-related quality of life we used univariate analysis of covariance, with treatment as fixed factor and EQ-5D utility at baseline as covariate. The analyses of the clinical outcomes have been described previously. 1 If a significant difference in EQ-5D score is found the “efficiency” decision rule will follow the net monetary benefit approach where the effect difference in QALYs (according to the EQ-5D difference score) will be multiplied with an appropriate willingness to pay for a QALY (as used in the Netherlands). Then the cost difference is subtracted from this score, leading to an incremental net monetary benefit (iNMB), and the result of this iNMB should be larger than zero for being efficient. If no significant difference in EQ-5D is found we use a cost minimization analysis for the criterion “efficiency.” Bootstrapped Incremental Cost-effectiveness Ratios are presented for health-related quality of life, clinical outcomes, and costs.
Results
Participants
A total of 56 patients, mean age 44.3 years (SD, 16.6), 45 female (80.4%), were included in the trial and randomized to either Pain Exposure Physical Therapy or conventional treatment, 4 patients in the Pain Exposure Physical Therapy group, and 11 patients in the conventional treatment group opted out of their assigned treatment and switched groups. These patients were analyzed according to their randomization, following the intention-to-treat principle and were excluded from the per-protocol analysis (Figure 1).
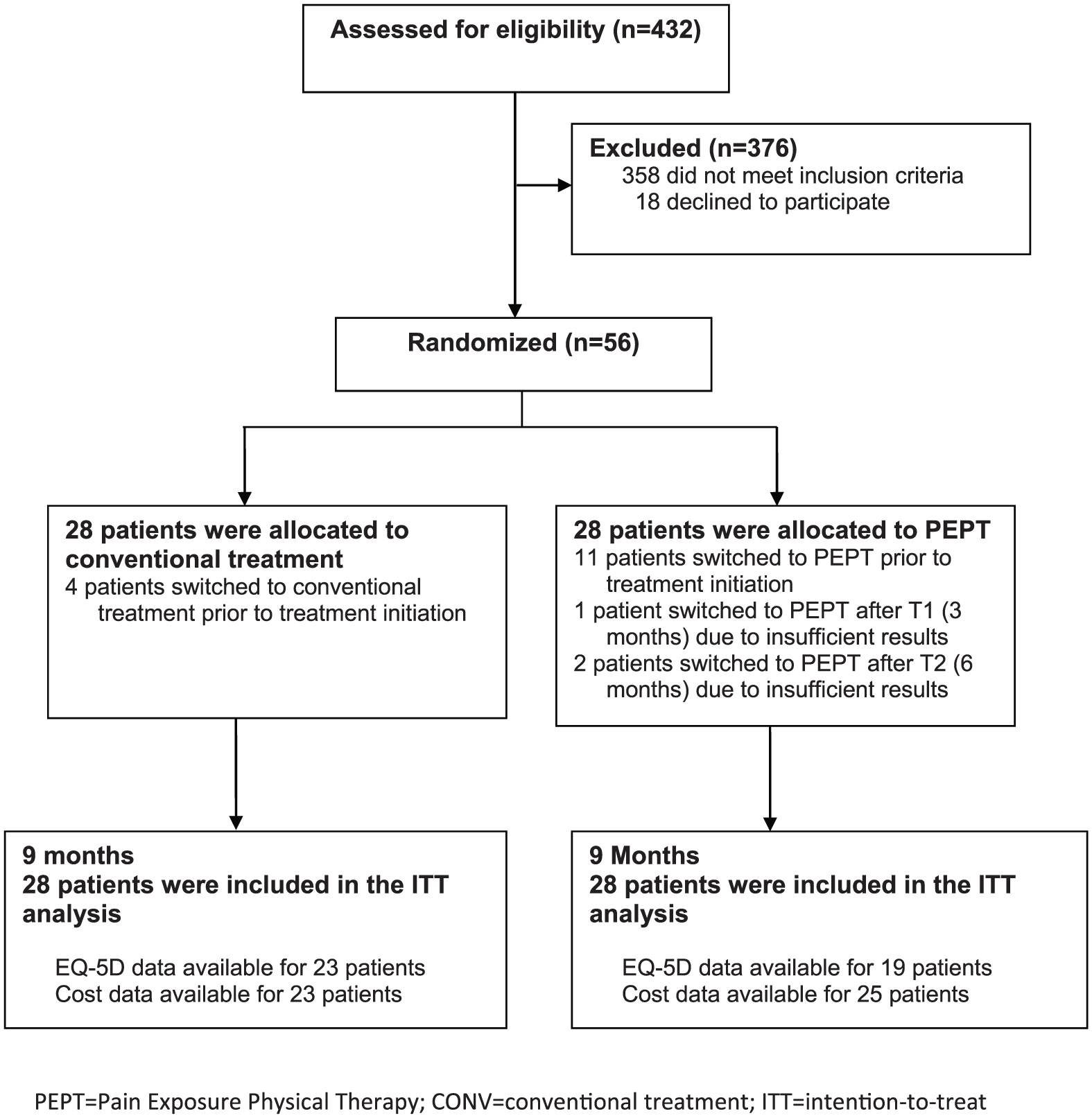
Patient flow.
Health-related quality of life and clinical outcomes
Data on health-related quality of life were available for 42 patients (23 in the Pain Exposure Physical Therapy group and 19 in the conventional treatment group). The EQ-5D increased by 0.23 points in the Pain Exposure Physical Therapy group and 0.27 points in the conventional treatment group after 9 months (Table 1). The difference in mean QALY was −0.02 (95% confidence interval (CI) −0.10 to 0.04), which is not statistically significant. The non-significant results for the clinical outcomes Impairment level Sum Score and Pain Disability have been presented elsewhere. 1
Descriptive data of the outcome measures.
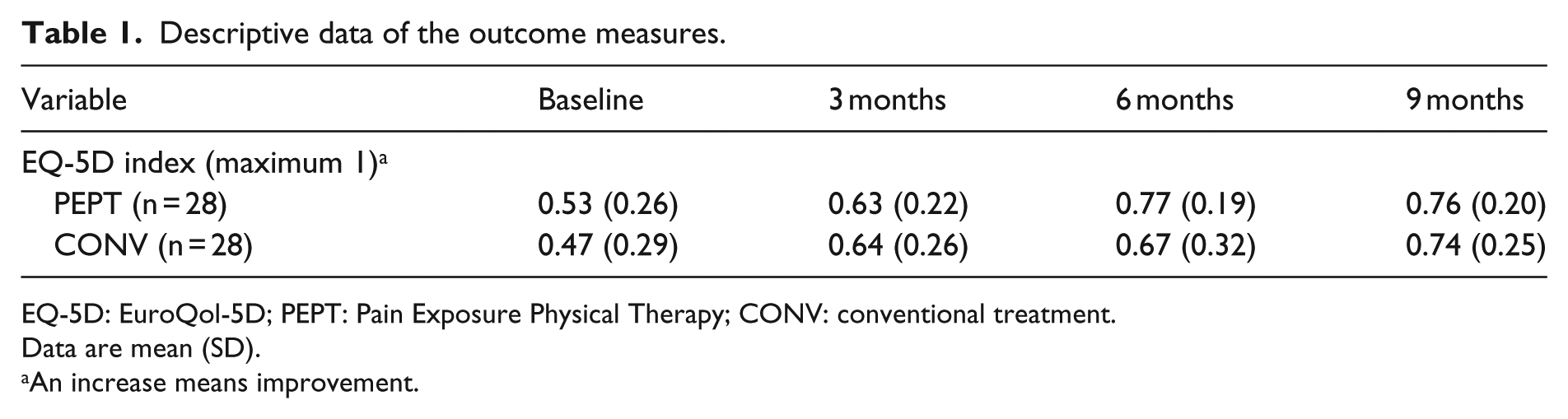
EQ-5D: EuroQol-5D; PEPT: Pain Exposure Physical Therapy; CONV: conventional treatment.
Data are mean (SD).
An increase means improvement.
Costs and health services used
The cost minimization analysis (as there were no significant differences in EQ-5D results and clinical outcomes) showed that conventional treatment was 1.64 (95% CI 1.05 to 2.56) times more expensive than Pain Exposure Physical Therapy. Thus, the mean cost of conventional treatment was €2783 or 64% greater compared to the Pain Exposure Physical Therapy group cost of €1695. The mean costs per cost category are shown in Table 2 and in Supplementary Appendix 1.
Cost data for different cost categories.
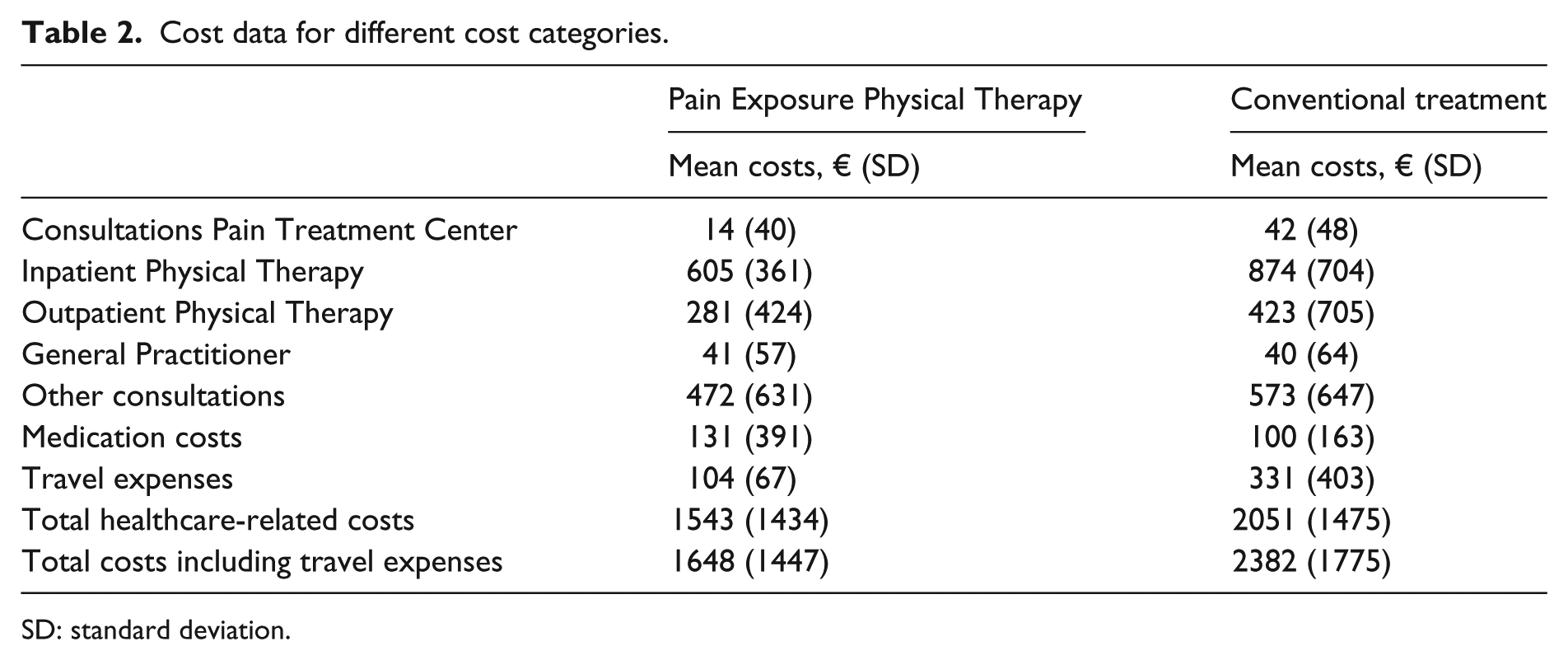
SD: standard deviation.
The Pain Exposure Physical Therapy intervention needed on the average 3.7 (SD 1.7) physical therapy treatment sessions (with two therapists) compared to 9.6 (SD 12.7) treatment sessions in the conventional treatment group. Besides the allocated intervention the participants in the Pain Exposure Physical Therapy group had on the average 5.7 (SD 8.9) outpatient physical therapy consultations, 2.9 (SD 3.0) general practitioner consultations, 2.0 (SD 1.9) visits to medical specialists, and 0.4 (SD 1.2) consultations of the Pain Treatment Center at our University Hospital. Besides the allocated intervention, the participants in the conventional treatment group had on the average 6.2 (SD 5.0) outpatient physical therapy consultations, 3.3 (SD 3.6) general practitioner consultations, 2.2 (SD 2.0) visits to medical specialists, and 1.3 (SD 1.5) consultations at the Pain Treatment Center at our university hospital.
Cost-effectiveness planes are presented in Figure 2. The planes show that Pain Exposure Physical Therapy is cheaper and that there is a trend favoring this intervention for EQ-5D, and in particular Pain Disability, since point estimates are mainly located in the dominant quadrant of the cost-effectiveness planes (i.e. more effective and less costive).
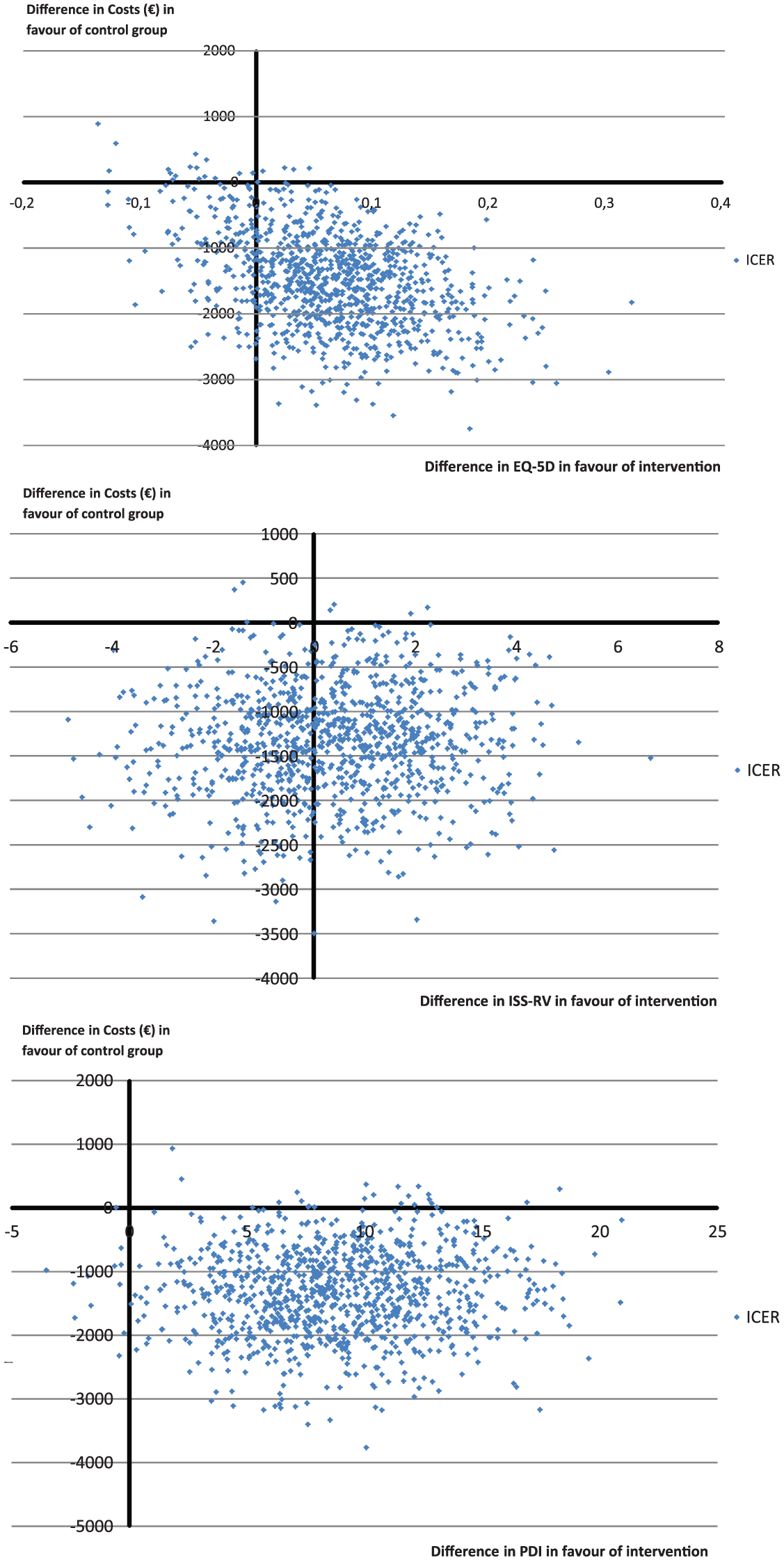
Cost-effectiveness planes.
Discussion
This economic analysis shows that Pain Exposure Physical Therapy is cost-effective as it saves costs when compared to conventional treatment in patients with complex regional pain syndrome type 1. Patients in the group receiving the new therapy made fewer visits to see healthcare professionals. Similar to the findings of the effectiveness study, in which we found no significant clinical effects, there was no significant difference in health-related quality of life between groups. 1 Calculated according to the intention-to-treat principle, Pain Exposure Physical Therapy was on average €1088 less costly than conventional treatment.
The strengths of the study are its randomized prospective design, the relatively long follow-up period (i.e. 9 months), blinded collection of cost data 21 and the fact that this is the first trial comparing Pain Exposure Physical Therapy to conventional treatment in complex regional pain syndrome type 1. The number of patients switching between groups and the lack of data on productivity losses are limitations of this study.
Directly after randomization but prior to treatment initiation, 14 patients deviated from the trial protocol and received a different treatment than to which they were assigned. The exact reason why this happened is unknown, but it stresses the importance of a thorough and careful explanation of what patients might expect when they participate in a randomized controlled trial. 1 Perhaps, this is particularly important in patients who suffer from a debilitating and very painful condition such as complex regional pain syndrome type 1. As a result, the primary intention-to-treat analysis was based on mixed groups and this may have yielded a conservative effect estimate. Further, not all patients who were allocated to the intervention group and received Pain Exposure Physical Therapy adhered to the treatment protocol. Nine patients received some form of medication or other conventional treatment. Most of this treatment was prescribed by their general practitioners, who were not involved in the trial. It was often not clear whether this medication was primarily related to complex regional pain syndrome type 1, but it could have had an effect on the patients’ complaints. That is why we included these costs in the analyses.
Regarding generalizability, the conventional treatment adhered to the Dutch national guideline, and although this guideline was based on internationally published research articles, 15 standard treatment may be different in other countries.
The difference in medication costs turned out to be smaller than anticipated, and even reversed in the intention-to-treat analysis probably due to the reasons described above. The difference in travel expenses is due to fewer consultations, both with the physical therapist and the anesthesiologist, in the Pain Exposure Physical Therapy group. The difference in physical therapy costs are relatively small, because in Pain Exposure Physical Therapy there are two physical therapists working together throughout each treatment session.
We initially intended to collect the cost data from the patients themselves. However, this turned out to be logistically unfeasible and resulted in data that were too incomplete. We therefore decided to collect the required information directly from the hospital administration system and from health insurance companies after informed consent of the patients involved. This allowed for reliable overviews of the actual healthcare costs. Unfortunately, we did not receive the required information on healthcare costs from all the contacted health insurance companies. That is why cost data were available for only 48 out of the 56 patients. These data were missing at random, because they did not correlate with the measured value. Therefore, we did not impute missing data and we only used the data available for our cost-effectiveness analysis.
For the cost-analysis, we did not include costs caused by omission to work or productivity losses. Although we cannot make a substantiated statement, Pain Exposure Physical Therapy seems to be more relevant for society because of the shorter duration of treatment and perhaps quicker return to work.
As mentioned before, this is the first trial studying the effects and cost-effectiveness of Pain Exposure Physical Therapy in patients with complex regional pain syndrome type 1. The Cochrane systematic review on physical therapy in patients with complex regional pain syndrome type 1 found 18 randomized trial studying a variety of physical therapy interventions such as electrotherapy modalities (ultrasound, transcutaneous electrical neurostimulation (TENS), laser, interferential therapy, and pulsed electromagnetic field therapy), both supervised and non-supervised exercise (active, active-assisted, passive, stretching, strengthening, mobilizing, and functional), manual lymphatic drainage, pain management advice, and sensory-motor rehabilitation strategies (graded motor imagery, mirror therapy, virtual body swapping, and tactile sensory discrimination training). 23 About 15 of the 18 trials had high risk of bias. There was very-low-quality evidence suggesting that cortically oriented grade motor imagery and mirror therapy might be useful to improve pain and disability. 23 None of the trials studied Pain Exposure Physical Therapy, and only one study investigated cost-effectiveness and found that physical therapy was cost-effective compared to occupational therapy and usual care.11,23
In conclusion, we can state the analysis of our trial was hampered by the proportion of patients who switched groups prior to treatment initiation and the lack of data on productivity losses. Despite that, the results are in line with previously reported positive studies on this intervention by our group.9,10 The differences in costs are in favor of the intervention group. Pain Exposure Physical Therapy can be considered a promising treatment for complex regional pain syndrome type 1, but its (cost)effectiveness needs to be further explored in sufficiently powered and methodologically sound randomized controlled trials.
Clinical Messages
Pain exposure physical therapy is less costly than conventional guideline-based care while reaching the same benefits in patients suffering from complex regional pain syndrome type 1.
These benefits can be achieved by a maximum of five physiotherapy sessions (provided by two physiotherapists) using the Pain Exposure Physical Therapy approach.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Netherlands Organization for Health Research and Development (ZonMw; 1709901004) funded this study. The funder had no role in the study design, data collection, data analysis, data interpretation, or writing of the report.
Supplementary Material
Because participants gave informed consent specifically for this study, and the final data set is only available for reuse after informed consent of the participants.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.