
Abstract
Objective:
To evaluate the use of active controlled motion (ACM) after unstable ankle fractures needing initial partial weight-bearing.
Design:
Prospective randomized controlled trial.
Setting:
Inpatient and outpatient clinic.
Subjects:
A total of 50 patients with unstable ankle fractures and the need for partial weight-bearing for six weeks.
Interventions:
Randomization in two groups: physiotherapy alone or physiotherapy with an additional ACM device.
Main measures:
Follow-up after 6 and 12 weeks. Range of motion, visual analogue scale for foot and ankle (VAS FA), Philip score, Mazur score, American Orthopaedic Foot & Ankle Society (AOFAS) score and dynamic pedobarography.
Results:
Range of motion was better in the ACM group at six weeks (mean 49° ± 11.1° vs. 41.3° ± 8.1°). Questionnaires revealed better outcome after six weeks in the VAS FA (56 ± 13.7 vs. 40.6 ± 10.5), Mazur score (64.4 ± 12.3 vs. 56.7 ± 11) and AOFAS score (71.2 ± 12 vs. 63.6 ± 8.7) (P > 0.02 for all). Better outcome after 12 weeks in all questionnaires (VAS FA, 77.7 ± 13.8 vs. 61.4 ± 16.3; Philip score, 79.1 ± 10.9 vs. 60.1 ± 21.7; Mazur score, 83.9 ± 10.7 vs. 73.1 ± 14.1; AOFAS score, 87.5 ± 7.9 vs. 75.2 ± 11.7) (P < 0.01 for all). Pressure balance was better under the midfoot region after 12 weeks in the ACM group (ΔP 4.4 N vs. 34.0 N; P = 0.01). The ACM group had an earlier return to work after 10.5 (range, 3–17) versus 14.7 (range, 9–26) weeks (P = 0.02).
Conclusion:
The use of ACM for patients needing initial partial weight-bearing after operatively treated unstable ankle fractures in the first six postoperative weeks leads to better clinical and functional results and an earlier return to work.
Introduction
Ankle fractures are common with an incidence of up to 187/100,000/year. 1 There is a bimodal distribution with a peak in younger males under 30 years and females over 60 years. 2 Weber’s classification is widely accepted. 3 Non-operative treatment is only possible in no or minimal (<2 mm) displaced stable fractures without concomitant ligamentous injuries. 4 The aim of an operative treatment should be an early functional postoperative treatment in order to start the rehabilitation process as soon as possible. In the case of concomitant ligamentous injuries (e.g. deltoid ligament or syndesmotic complex), partial weight-bearing with 10–20 kg is necessary for six weeks.5,6
There is almost no information about proprioceptive deficits after ankle fractures and their role in the rehabilitation process. Proprioceptive training of ankle fractures is commonly done with balance boards or balance circles. In patients with need of partial weight-bearing, this is not possible until full weight-bearing is allowed. Usage of an active controlled motion (ACM) device has been shown to decrease the proprioceptive deficit after rupture of the anterior cruciate ligament (ACL) in the knee joint.7 –9 There is no information about possible benefits or harms of ACM after ankle fractures.
The aim of this study was to look for possible beneficial rehabilitation effects in the use of ACM after operatively treated unstable ankle fractures with the need of partial weight-bearing in the first six postoperative weeks.
Patients and methods
This was a prospective, randomized controlled study at a single Level-I trauma center. The study was approved by the local ethics committee (159/10) and follows the Declaration of Helsinki for ethical principles for medical research involving humans. The study was registered at the German Clinical Trials Register using the World Health Organization (WHO) Trial Registration Data Set (DRKS00009979).
Inclusion criteria were as follows: operatively treated unstable ankle fractures as the only injury of the lower extremity with a type B- or C-Fracture in the Weber classification, 3 the need of partial weight-bearing for six weeks, age over 18 years, possibility to perform physiotherapy and ACM and no problems in walking before the injury. After fullfilling the inclusion criteria, the patients were asked to participate in the study. Patient’s consent was taken prior to randomization. Patients were prospectively randomized in two groups by lots: group 1 with regular postoperative physiotherapy (PT group) and group 2 with additional ACM (ACM group).
Physiotherapy started on the first postoperative day with a daily treatment of 20 minutes during hospitalization with the focus on mobilization of the patient using two crutches and ability to maintain partial weight-bearing. After discharge from the hospital, physiotherapy was performed over 20 minutes two to three times a week for a total of six weeks focusing on the treatment of edema and regaining range of motion (ROM) avoiding forced dorsiflexion.
ACM was performed using the Camoped© device, (Camoped©, OPED® GmbH, Germany). Training started two to five days after the operation depending on the condition of the soft tissue with the patient in a supine position (Supplementary Figure 1). Patients were educated in the usage of the ACM device by the physiotherapist. After discharge from the hospital, the ACM device was delivered to the patient’s home for further training of 20 minutes daily.
In cases where a lag screw was inserted, the screw was removed after six weeks (prior to full weight-bearing). An additional boot (Vacoped©, OPED® GmbH, Germany) was applied for the first six postoperative weeks depending on the surgeon’s preference.
Clinical follow-up was performed 6 and 12 weeks after the operation by two, not blinded, examiners. Besides patient’s characteristics (age, gender, weight, fracture type, return to work, etc.), the active and passive motion of the ankle joint and subtalar joint and the clinical outcome were measured by four different questionnaires at both time points: the visual analogue scale for foot and ankle (VAS FA), 10 the Phillips score, 11 the Mazur score 12 and the AOFAS score. 13
At both follow-ups, dynamic pedography was carried out in an area measuring 1.2 m × 8.0 m with an integrated measuring plate (EMED-M, 38 cm × 42 cm, four sensors per square centimeter, 50 Hz; Novel GmbH, Munich, Germany). The foot was divided into 10 zones (heel, midfoot, metatarsals 1–5, hallux, second toe and toes 3–5) for pressure and contact time during the rollover process. The peak pressures, the contact time during the rollover process and the force–time integrals were analyzed and averaged. Patients were allowed an unlimited number of test walks. At least five accurate measurements per side were carried out, and the average of the values was included in the subsequent analysis using software support (novel database essential© ver. 19.3.20).
Statistical analysis was carried out using IBM SPSS Statistics (version 20; IBM Deutschland Ltd., Ehningen, Germany). For metric data, we used the Shapiro–Wilk test to look for normal distribution. If normal distribution was given, we used the T-test for independent samples, otherwise the Mann–Whitney U test. For categorical data, the chi-square test and Fisher’s exact test were used.
Results
Patients
A total of 50 patients was included in the study and randomized by lot to the two groups. One patient in group 1 (PT group) had to be excluded due to violation against postoperative treatment protocol. There were no differences between the two groups regarding age, gender, height, weight, side, fracture type or type of osteosynthesis (Table 1). At the clinical follow-up, after six weeks a total of 48 patients (24 for both groups) and after 12 weeks a total of 44 patients (22 for both groups) could be examined (Figure 1).
Patient’s data.
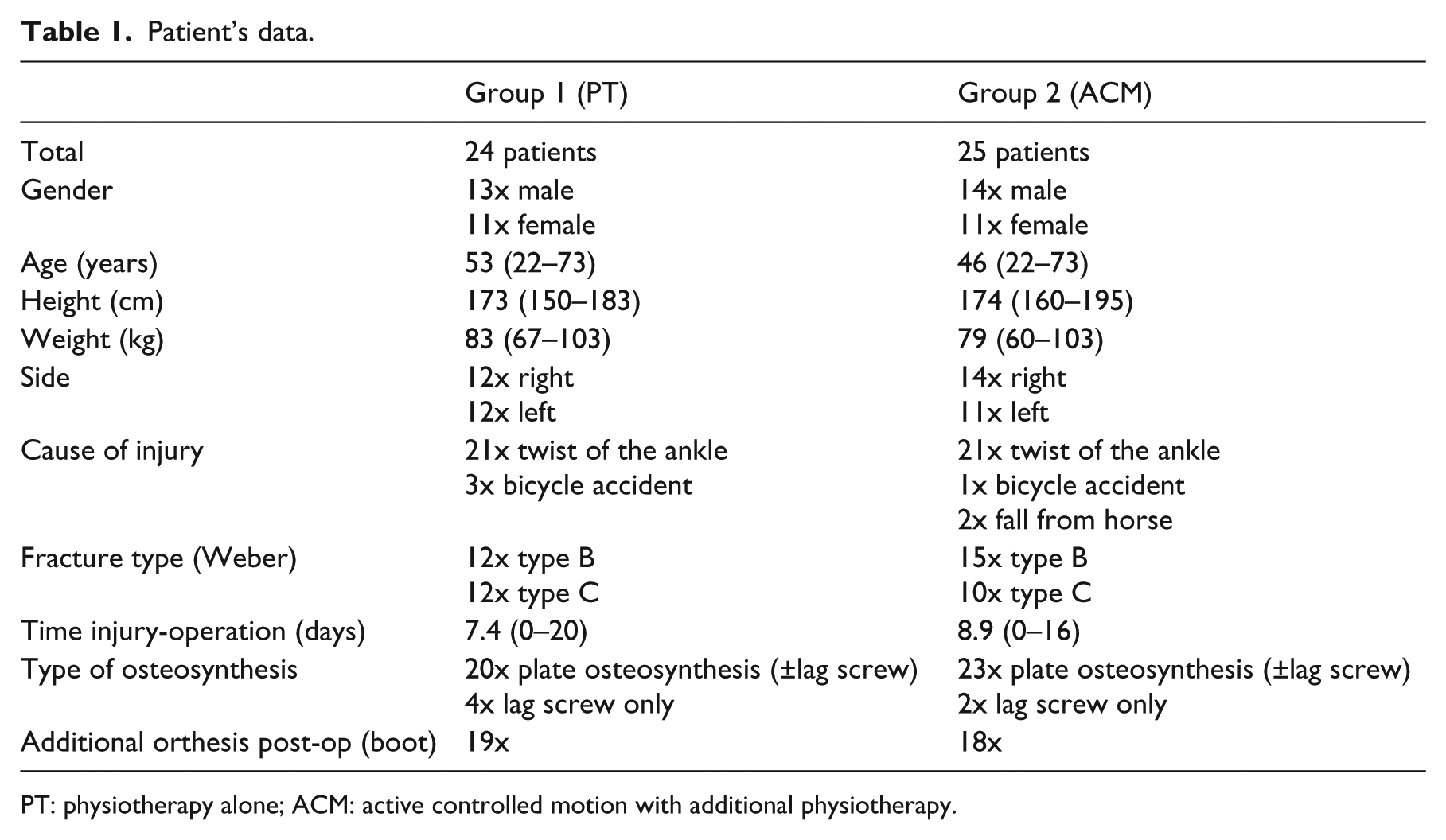
PT: physiotherapy alone; ACM: active controlled motion with additional physiotherapy.
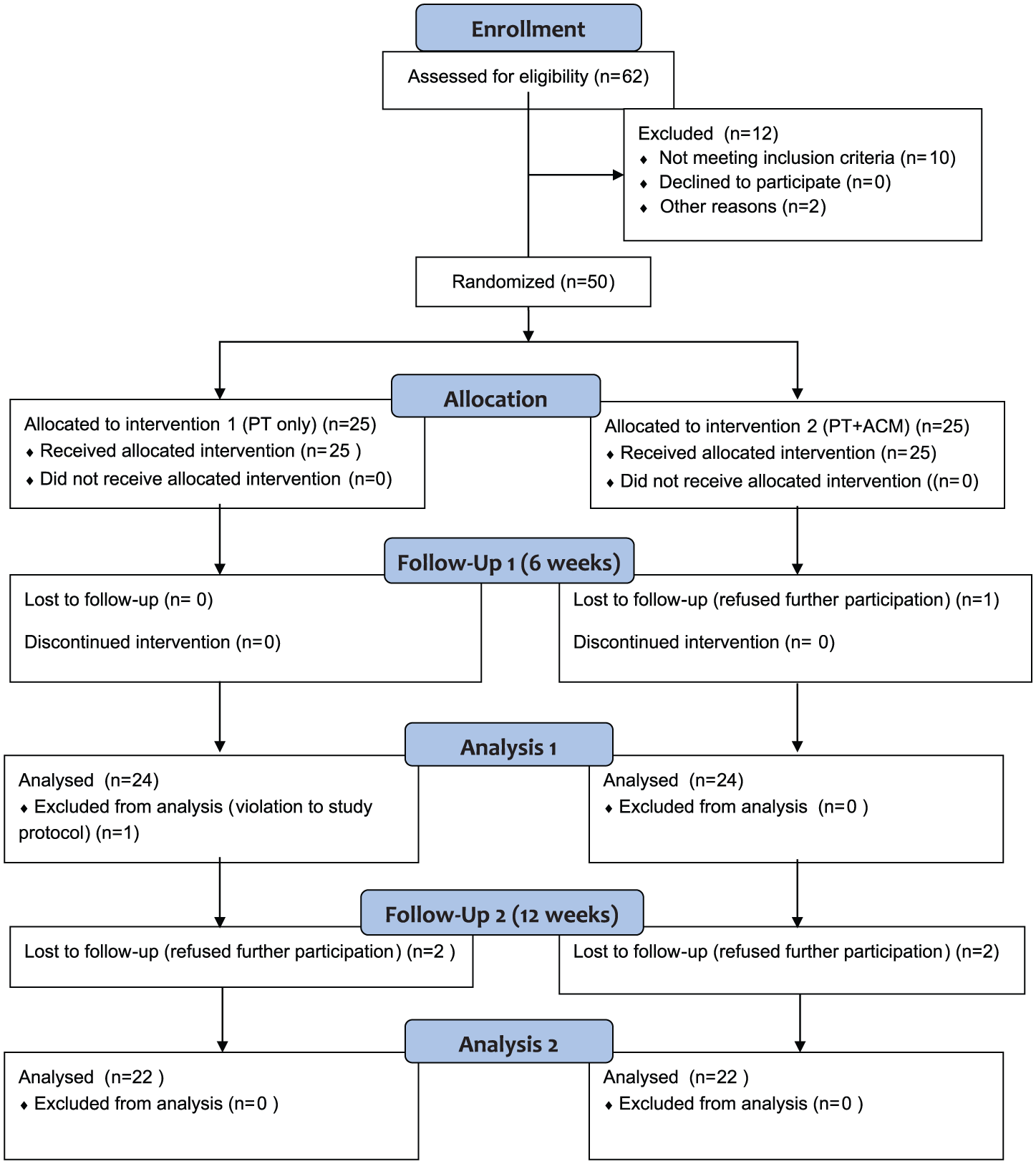
Flow diagram according to CONSORT.
Full weight-bearing
At the follow-up when full weight-bearing was allowed (after six weeks), 13 patients (54%) in group 1 (PT) were able to put full weight on the injured leg whereas in group 2 (ACM) 22 patients (88%) were able to perform full weight-bearing (88%) (P < 0.02).
ROM
There was a better motion in the ankle joint and the subtalar joint in group 2 (ACM) compared to group 1 (PT) after 6 and 12 weeks compared to the uninjured side.
Questionnaires
There were better functional results for the VAS FA, Mazur score and AOFAS score after 6 and 12 weeks and better results in the Philip score after 12 weeks.
Return to work
The mean time of returning to work in group 1 (PT) was 14.7 (range, 9–26) weeks and in group 2 (ACM) 10.5 (range, 3–17) weeks (P = 0.02). The results of ROM, the questionnaires and return to work are summarized in Table 2.
Results of the two groups regarding range of motion (ROM), questionnaires and time until return to work.
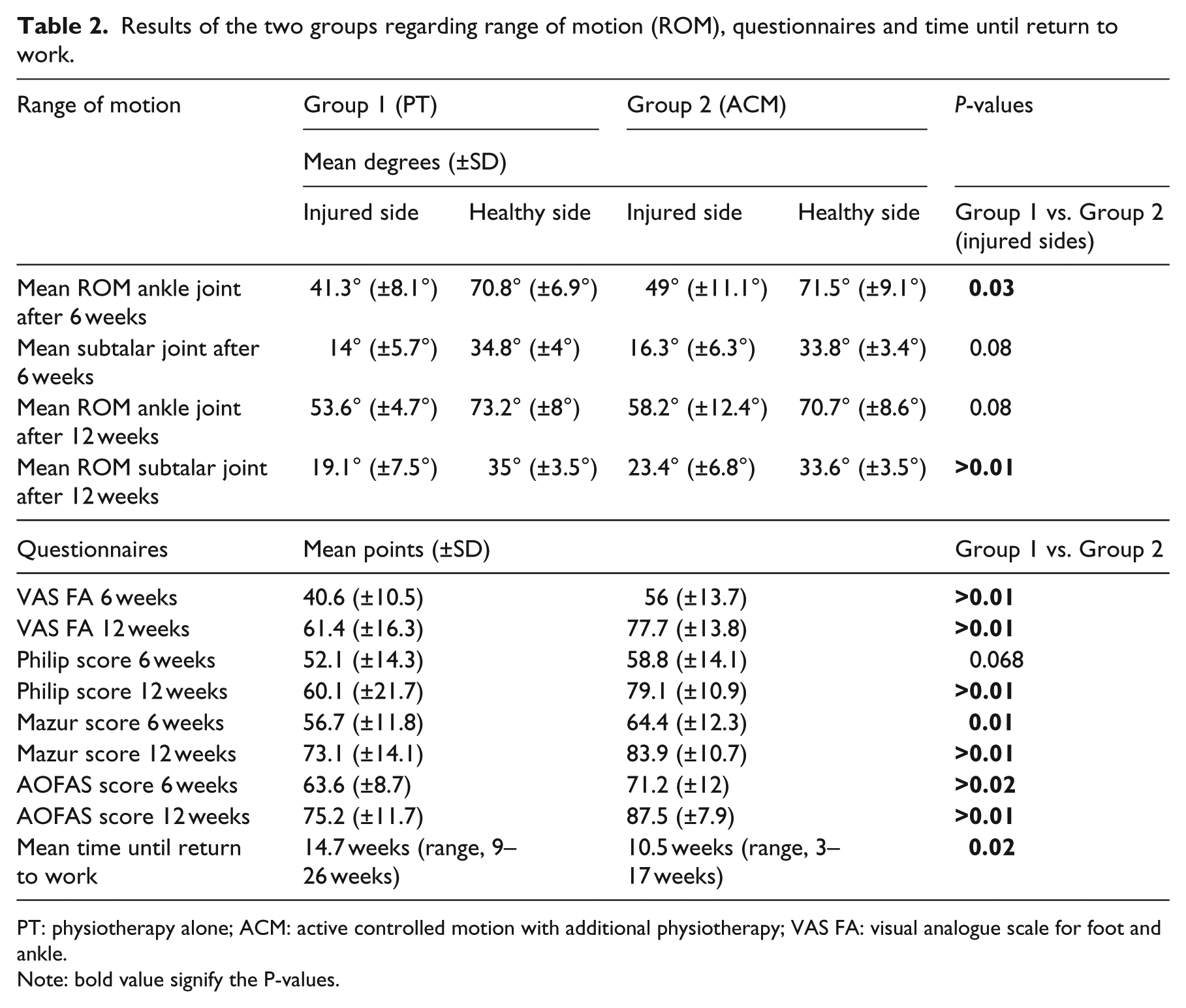
PT: physiotherapy alone; ACM: active controlled motion with additional physiotherapy; VAS FA: visual analogue scale for foot and ankle.
Note: bold value signify the P-values.
Dynamic pedobarography
There were no differences in the pedobarographic findings after six weeks between the both groups. After 12 weeks, there was less difference in the pressure under the midfoot region in group 2 (ACM) with an average pressure of 132 (±66.9) N for the injured side and 136.4 (±69.6) N for the healthy side compared to an average of 160.9 (±77.2) N for the injured side and an average of 194.9 (±75.2) N for the healthy side in group 1 (PT).
Discussion
In our study, the use of an ACM device showed considerable improvement in the clinical outcome after unstable ankle fractures with the need of partial weight-bearing.
Ankle fractures are frequent and can make up costs of more than US$2.100 in the initial treatment. 14 Despite an initial fast recovery, regain of the function decelerates over the time and can even be incomplete two years after the fracture. 15 In the clinical practice, patients show restricted ROM of the ankle joint and subtalar joint leading to toddling or limping.
The need and the effects of different rehabilitation programs are still controversial: Nilsson et al. 16 showed positive effects of an individually suited training program in patients younger than 40 years. Moseley et al. 17 could not show additional benefits of a supervised exercise program after immobilization for ankle fractures. Injuries of the ankle joint not only lead to fractures but also to deficits in proprioception. Han et al. described the influence of proprioception after ankle injury and alleged that there is no “general” proprioception in humans. He states that every joint has a specific one.18,19
Neuromuscular training is commonly used in rehabilitation after injuries of the lower extremity and has shown positive effects.20 –23 The common problem in all these rehabilitation programs is the limitation of the beginning moment: as most of the unstable ankle fractures are immobilized and only allowed partial weight-bearing for the first six weeks, there is a delay for the beginning of rehabilitation and training and items as a training disk cannot be used during this time.
After a rupture of the ACL in the knee joint, there is no correlation between the objective mechanical instability and the subjective instability of the patient. However, there is a correlation between the proprioception and the subjective instability of the patient. Usage of an ACM device can decrease the proprioceptive deficit.7 –9 Training can start with minimal delay of two to five days after the operation even when the ankle is immobilized in a boot—which also seems to be superior to immobilization in a cast and is widely used nowadays. 24 ACM offers the opportunity of starting the rehabilitation process right away without a delay for the first six weeks.
In extension to previous authors, we were able to show a beneficial effect of rehabilitation program after ankle injury. In contrast to other studies, the rehabilitation program using ACM started right after the operation although the affected limb was immobilized and partial weight-bearing was performed. We found a better ROM and better functional results in the questionnaires at 6 and 12 weeks postoperative. As the results in dynamic pedobarography showed nearly no differences between the two groups, we interpret these findings in a better subjective usage of the affected limb which could indicate a better proprioception. As the group using ACM had an earlier return to work by four weeks compared to the control group, the use of ACM implicates reduced socio-economic costs after sustaining an unstable ankle fracture: the costs for the device were €375 (US$425) per patient for the whole six-week period. The average socio-economic loss for a single missed working day in Germany is €193 (US$220). 25 As patients were already educated in the usage of the device by the physiotherapist during hospitalization, they could carry on the training right after discharge of the hospital with the ACM device being delivered to the patient’s home by a commercial parcel service. The device used in this study is easily available, very feasible and acceptance in patients and physiotherapists was high.
Although this was a prospective randomized controlled trial, it has some limitations: due to the use of ACM, the participants could not be blinded. Due to the study design, it remains unclear whether it is a reduced lack of proprioception causing the better functional results of the patients or the additional daily exercise. Further studies focusing on proprioception and the use of ACM after injuries of the lower extremities are needed.
Clinical Messages
In people with an unstable ankle fracture treated with initial partial weight-bearing, the use of ‘active controlled motion’ (continuous passive movement) is associated with improved clinical outcomes including quicker return to work.
Footnotes
Acknowledgements
This study was conducted in compliance with the current laws applying in Germany.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.