
Abstract
Objective:
Identify the environmental factors that influence stroke-survivors’ reengagement in personally valued activities and determine what specific environmental factors are related to specific valued activity types.
Data sources:
PubMed, CINAHL and PsycINFO were searched until June 2016 using multiple search-terms for stroke, activities, disability, and home and community environments.
Review methods:
An integrated mixed-method systematic review of qualitative, quantitative and mixed-design studies was conducted. Two researchers independently identified relevant studies, assessed their methodological quality and extracted relevant findings. To validly compare and combine the various findings, all findings were classified and grouped by environmental category and level of evidence.
Results:
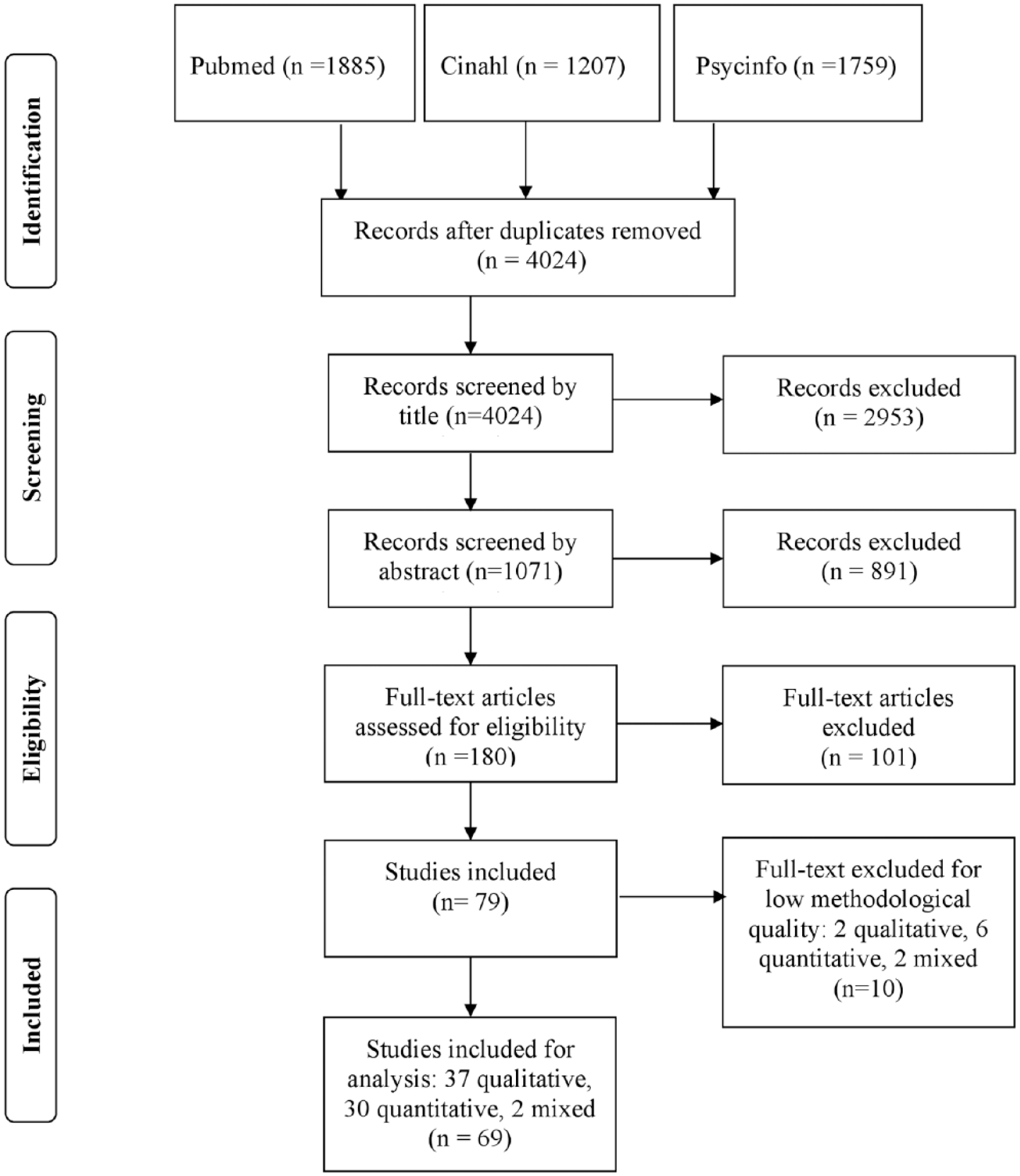
The search yielded 4024 records; 69 studies were included. Most findings came from low-evidence-level studies such as single qualitative studies. All findings were consistent in that the following factors facilitated reengagement post-stroke: personal adapted equipment; accessible environments; transport; services; education and information. Barriers were: others’ negative attitudes and behaviour; long distances and inconvenient environmental conditions (such as bad weather). Each type of valued activity, such as mobility or work, had its own pattern of environmental influences, social support was a facilitator to all types of activities. Although in many qualitative studies others’ attitudes, behaviour and stroke-related knowledge were seen as important for reengagement, these factors were hardly studied quantitatively.
Conclusion:
A diversity of environmental factors was related to stroke-survivors’ reengagement. Most findings came from low-evidence-level studies so that evidence on causal relationships was scarce. In future, more higher-level-evidence studies, for example on the attitudes of significant others, should be conducted.
Introduction
After stroke, many stroke-survivors suffer from activity loss,1,2 which is related to a decline in their life satisfaction3,4 and well-being. 5 To enable stroke-survivors to restore at least those activities that they most value, rehabilitation trajectories include many efforts to remediate the functions and skills that underlie these valued activities. 6 However, as many stroke-survivors are left with persisting disability in spite of these efforts,7,8 it is highly relevant that rehabilitation also focuses on the creation of a supportive ‘post-discharge environment’. 9 Reengagement in valued activities may be enhanced by recognising and eliminating barriers and integrating available resources in the stroke-survivor’s environment as part of the rehabilitation programme. So far, however, it remains unclear which environmental features of stroke-survivors’ living environments help or hinder their attempts to resume their valued activities.10,11 This mixed-method systematic review used an integrative design to combine all relevant qualitative and quantitative evidence available on this topic. It aimed to identify the environmental factors that facilitate or hinder stroke-survivors’ reengagement in personally valued activities, and to determine what specific environmental factors are related to specific types of valued activities post-stroke.
In the context of this review, environmental factors included all physical, social and system-related factors that are present in the stroke-survivor’s living environment. These include their housing; city; family and friends as well as the organisational; infrastructural; sociocultural and political features of their community. Valued activities were defined as activities that were voluntary chosen and of specific value to stroke-survivors, for example because these activities were directly related to a stroke-survivor’s valued family role or social position.
Methods
We performed a systematic literature search in Pubmed, Cinahl and Psychinfo from database onset to June 2016 to identify relevant studies. Since there are only a few suitable MeSH headings on environmental factors and relevant keywords vary widely, we needed to use a two-step search strategy. First, we identified all qualitative, quantitative and mixed-design studies on stroke and reengagement in valued activities; then we extracted all the relevant articles on environmental factors. For the full search string (Pubmed), see the appendix (supplementary material).
Two experts in stroke rehabilitation (JZ, SJ) independently identified articles that met the inclusion criteria by title and by abstract. Prior to each inclusion step, a sample of 10 reports was used to verify agreement in applying the inclusion criteria. The inclusion criteria were as follows: non-biomedical, scientific studies of community-dwelling adult stroke-survivors, containing findings on environmental factors that influenced survivors’ reengagement in valued activities, written in English. Because we were specifically interested in environmental factors that influence reengagement in valued activities after stroke and single case studies were expected to also describe environmental factors that are not particularly related to stroke, we excluded single case studies. We also excluded studies about professional health services because the aim was to provide knowledge about environmental factors rather than to present evidence on specific health interventions.
Two researchers (SH, SJ) independently read the full texts and decided whether articles should be included. Disagreement was resolved by discussion. If necessary, they consulted a third subject matter expert (ES), whose decision was final.
The methodological quality of each original study was assessed using the Critical Appraisal Skills Programme (CASP) lists. 12 Each original study was assessed by SH and SJ independently using the specific list per design (qualitative, case control, cohort, randomised controlled trial, systematic review). Any disagreement was resolved by discussion. Percentage scores were calculated based on fulfilled items divided by the total number of relevant items. Studies of sufficient methodological quality (i.e. with CASP scores higher than 65%) were included for further analysis.
Data extraction was done by the two researchers (SH, SJ). They independently extracted findings on the influence of environmental factors from all qualitative, quantitative and mixed-design studies. Qualitative data were extracted by identifying all relevant text passages on the facilitating or hindering role of environmental factors on valued activities and by briefly describing their central meaning while staying as close to the original text as possible. In case a direction of influence (facilitator or barrier) was clear in the context of a particular study but was not explicitly described by the author, this was noted. Quantitative findings were extracted by describing relevant results of univariate and bivariate analyses.
An integrated design was used to combine qualitative and quantitative data. In such a design, methodological differences between qualitative and quantitative studies are seen as minimal because both kinds of data are viewed as producing findings that can readily be transformed into each other. 13 After such a data transformation, it becomes possible to synthesise all the findings. 13 In this particular systematic review, we made quantitative findings comparable to qualitative findings by describing whether the quantitative findings referred to a facilitating or a hindering role with regard to reengagement.
We expected that various environmental factors, described in diverse terms, would be present within all the qualitative, quantitative and mixed-design studies. To be able to validly compare the diverse findings and, if suitable, combine them, we classified all the findings by the type of environmental factor they described, using the International Classification of Functioning, Disability and Health (ICF). 14 Categorising findings using an existing classification system can be referred to as directed content analysis and is used when substantial knowledge of existing categories is available. 15 For each environmental factor described in a particular finding, we sought the ICF-environmental category or subcategory that best described its content. In some cases, a global ICF-category best fit the description of such a factor; in other cases, a more refined ICF-category was a better fit. When a suitable ICF-category was not available, the factor was classified as ‘n.c.’ (not covered by the ICF), in accordance with the ICF linking rules. 16
Furthermore, to understand the value of a specific finding as compared to others, we used the Melnyk hierarchy of levels of evidence 17 to arrange our findings. Although there are many hierarchies of evidence available in the literature, 18 this particular hierarchy of evidence encompasses a broad range of evidence, including quantitative and qualitative evidence. 17 See Figure 1 (supplementary material) for this hierarchy (levels ranging from low to high evidence: VII to I). Because we only included literature from scientific, peer-reviewed studies, level VII (evidence from expert opinions) and narrative reviews did not apply to this review study.
After transforming the data and arranging findings by type of environmental category and level of evidence, an overall comparison between all findings arranged under the same, and subsequently under different ICF environmental categories was made. This was done by one researcher (SJ) using thematic analysis 19 while continually checking the study characteristics (see supplementary Tables I-a, II-a and III-a) to confirm it was valid to compare or combine findings. Similarities and inconsistencies between findings (e.g. with regard to the content or the directionality of the environmental influence) as well as the related levels of evidence were noted. In accordance with the lines-of-argument synthesis, 20 the researcher subsequently tried to explain as a whole the findings arranged under the same and under different ICF environmental categories. This resulted in a conclusion about what environmental factors generally facilitate or hinder reengagement in valued activities post-stroke, as well as about the related levels of evidence.
Finally, to be able to draw a more precise conclusion about what specific environmental factors facilitate or hinder the specific types of valued activities that stroke survivors try to resume, the researcher used thematic analysis to subdivide in categories the various activities described in the studies. This resulted in a description of several main types of activities valued by stroke survivors. All the findings from the qualitative, quantitative and mixed-design studies subsequently were arranged by these main types of valued activities. The researcher then described those environmental factors that, according to at least two qualitative/descriptive studies (i.e. two studies with evidence level VI) or according to one or more studies with a higher level of evidence (level V to I), facilitated or hindered a particular main type of activity. When, for a specific main type of valued activity, findings with regard to the influence of a particular environmental factor were contradictory, the factor was not taken into account. All conclusions drawn about the influence of environmental factors in general and about the specific main types of valued activities finally were checked by the other researchers involved in this review study (SH, ES, RS, RN). Disagreement was resolved by discussion.
Results
As shown in Figure 1, we identified 4024 studies, of which 69 fulfilled the inclusion criteria and had CASP scores higher than 65%. Of these, 37 reported qualitative data, 30 reported quantitative data and two had a mixed design. Supplementary Tables I-a, II-a and III-a list all the studies that fulfilled the inclusion criteria, including their methodological quality; characteristics; measures; levels of evidence and extracted study findings (studies with low methodological quality are listed in Tables I-b, II-b and III-b).
Inclusion of studies.
Of the 37 included high-quality qualitative studies, seven described specific environmental factors and their influence on reengagement21–26 (e.g. the influence of wheelchair use on community reengagement). 21 The other studies focused on stroke-survivors’ reengagement experiences in general. One study 27 was a systematic meta-synthesis (Melnyk evidence level V), one study 28 thematically analysed blogs written by stroke-survivors (level VI). Thirty five studies (level VI) used semi-structured individual or focus group interviews. Additionally, three of these interview studies also used other methods of data collection including diaries, photographs or observations. All qualitative studies reported experiences of stroke-survivors resuming activities according to standards they personally found satisfactory. The participant characteristics of the qualitative studies were variable: some studies researched a specific group such as aphasic or cognitively impaired stroke-survivors, while others studied stroke-survivors ‘in general’. Nine studies included significant others, such as informal caregivers, in addition to stroke-survivors. Reported ages ranged from 18 to 94 years; measurement time-points ranged from a number of weeks to 32 years post-stroke.
Of the 30 included high-quality quantitative studies (13 cross-sectional, 12 cohort, two case control and three randomised controlled trials) three29–31 descriptively reported facilitators and barriers experienced by stroke-survivors. The other studies examined a statistical relationship between environmental factors and valued activities. Reengagement was not quantified uniformly within the studies: it was measured by counting the number of daily activities performed32–35 or the number that could be performed without help;32,34–37 the amount of help needed;32,38–40 the relative difficulty experienced;33,38,40–45 the satisfaction felt with performance;33,46 or by exploring the subjective experience of feeling integrated within one’s living environment.47,48 Melnyk evidence levels varied between the studies: 13 studies had level VI, 14 level IV and three level II. Some studies included a specific group (e.g. wheelchair users), while others included stroke-survivors ‘in general’. Reported ages ranged from 27 to 97 years; measurement time-points ranged from four weeks to 27 years post-stroke.
The two included high-quality mixed-design studies were both cross-sectional (level VI). They combined reengagement measures with open-ended questions. One study examined stroke-survivors with aphasia, while the other examined stroke-survivors ‘in general’. Reported ages ranged from 47 to 81 years; measurement time-points ranged from nine months to one year post-stroke.
For a more detailed description of all the high-quality studies and their findings, see supplementary Tables I-a, II-a and III-a.
Environmental facilitators and barriers to reengagement post-stroke
A variety of facilitators and barriers were described in the included qualitative, quantitative and mixed-design studies. Most findings were related to the social and system-related aspects of stroke-survivors’ living environments (ICF-categories e3-5). They mainly came from low-evidence-level, single qualitative studies (level VI). Findings from controlled trials (level III) or from systematic reviews of randomised controlled trials (level I) were not identified. Supplementary Table IV displays all the environmental factors found in the 69 included studies, as well as the direction of their influence and their level of evidence.
As shown in the first column of Supplementary Table IV, most environmental factors found could be allocated to existing ICF-environmental categories. We added some extra categories (e.g. ‘skills/features of network members’) and refined some existing ICF-categories (e.g. the attitudes category). Within all the original ICF- and new categories, the directions of the environmental influences found (facilitator or barrier) were largely in accordance with each other. For example, regardless of each study’s participants or design, all the findings suggested that personal adapted equipment (e.g. assistive devices or communication aids); accessible environments (e.g. a well-adapted public space, accessible buildings and even terrain); high-quality transport; services, educational opportunities and, in most cases, money and social support were all facilitators to reengagement in valued activities post-stroke. Other people’s negative perceptions, attitudes and behaviours as well as long distances were all barriers to reengagement. A comparison of the findings from different ICF-environmental categories found that reengagement in valued activities is facilitated by access to information (e.g. about alternative transport). Inconvenient, complex and unstable conditions (e.g. bad weather or darkness, crowds, unstable prerequisites at work) generally hinder stroke-survivors’ ability to resume their valued activities.
However, we also found some inconsistencies with regard to directionally or content of the findings. First, although most findings suggested that wheelchairs were related to better reengagement, in work situations they were mainly seen as a barrier that made it difficult to socialise with colleagues or do heavy work. 49 Second, some qualitative studies found living in a rural area (instead of an urban area) to be a facilitator to reengagement.50,51 This was in line with the finding that crowds 52 and fast-moving traffic53,54 were seen as barriers to reengagement. However, it was not consistent with the finding that uneven terrain, 55 soil, 51 farm animals, 51 long distances54–58 or poor geographic coverage of public transport57,59 were also seen as barriers. In addition, quantitative studies found no significant relationship between type of living area and reengagement post-stroke.34,39 As a whole, these findings may suggest that the disadvantages of living in a rural area largely outweighs the advantages.
In several cases inconsistency between findings from qualitative and quantitative studies was present. For example, according to many qualitative studies,25,26,50,52,53,58,60–63 the availability of spouses, family and friends was related to better stroke-survivors’ reengagement. However, most cross-sectional or cohort studies did not confirm a relationship between the presence of spouses, family or friends and reengagement in valued activities.33,34,38,39,45,46,64–66 Sometimes, their presence was even found to worsen reengagement. 67 For a detailed description of the similarities and inconsistencies between findings and related levels of evidence, see Supplementary Table IV, last column; ‘synthesis’.
Environmental influences per specific type of valued activity
Thematic analysis revealed that valued activities could be divided into the following categories: reengagement in valued activities in general (studies about outdoor and indoor activities); 22,25,26,32,33,35–46,48,60–64,67–72 social and community reengagement (studies about social activities outside the home and in the community);21,23,27, 28,34,47,50,52,55,58,73,74 mobility (studies about moving around as a meaningful activity)29,51,53,54,56,57,59 and work.24,49,65,66,75–86 Some single remaining studies on activities such as eating, exercise or leisure30,31,87–90 did not fit this format. In all the types of valued activities social support was identified as a facilitator to reengagement. In most cases, adequate transport was recognised as being facilitating while others’ unsupportive attitudes and behaviours were seen as hindering to most types of valued activities.
Each type of valued activity also had its own pattern of influencing environmental factors. Studies on reengagement in valued activities in general, exclusively found the following facilitators: powered wheelchairs, home adaptations and adequate services, while studies on social and community reengagement exclusively found adaptation for communication and information access to be important. Studies on mobility specifically mentioned different aspects of traffic, public transport, the behaviour of bus drivers, distances and costs, while studies on work exclusively found features of the job itself to be relevant. In relatively many studies on social and community reengagement and on work, others’ attitudes, behaviours and stroke-related knowledge were seen as important for reengagement.
Supplementary Table V displays all the environmental factors that influence a particular type of valued activity (according to non-contradictory findings of at least two studies at level VI, or according to at least one study with a higher level of evidence). The table also shows all the related levels of evidence.
Discussion
This review identified an extensive list of environmental factors that may influence a stroke-survivor’s reengagement in valued activities. The majority of the findings were related to the social and system-related aspects of stroke-survivors’ living environments, such as the availability of family and friends and the quality of organisations and community services. Although different types of valued activities each had their own patterns of environmental influences, social support was identified as important to all types of activities. In relatively many studies on social and community reengagement and on work, the attitudes, behaviours and stroke-related knowledge of familiar other people were seen as important for reengagement in stroke-survivors’ valued activities. When in complex social environments such as the community or the workplace, others’ willingness to adapt to the stroke-survivor, their encouragement and their knowledge about stroke are probably crucial to enable stroke-survivors to resume their activities. However, quantitative higher-level studies rarely studied the impact of these factors on reengagement. Since a range of negative individual and societal attitudes and behaviours seems to hinder reengagement in disabilities, 91 it is of the utmost importance to better examine and understand the influence of these attitudes and behaviours and the convictions and gaps in knowledge that underlie them.
This study used the ICF-environmental categories and the Melnyk levels of evidence to classify and compare findings. Most findings fit the ICF. However, the ICF was not refined enough to allocate specific features, skills or attitudes and behaviours of others (e.g. others’ fatigue, problem-solving skills or willingness). Some other factors, such as ‘time’, could not be linked to any existing ICF-chapter at all. In future, the ICF could be improved by further mapping such factors, so that a comprehensive and consistent set of relevant environmental factors will become available to clinicians and researchers. Other authors91,92 have confirmed the necessity to add additional factors, such as time.
The levels of evidence found in this review were generally low: most findings on environmental factors and stroke-survivors’ valued activities came from single qualitative and cross-sectional studies (level VI). We found no studies with an evidence level of III or I. As a result, although we gained some insight into the environmental factors related to stroke-survivors’ reengagement in valued activities, there is a lack of knowledge about causal relationships between environmental factors and reengagement. Further research should address this knowledge gap, for example by developing an educational programme for family members, friends and colleagues on how best to support stroke-survivors’ reengagement and evaluating this programme in a controlled trial.
There is also a scarcity of high-level evidence on the influence of environmental factors on conditions other than stroke. In one of the few review studies done on environmental factors, Heinemann et al. 93 found a set of environmental factors that were relevant to stroke, traumatic brain injury and spinal cord injury. That review found that the following factors influence reengagement: assistive technology; the built and natural environments; the social environment; services, systems and policies; access to information and technology, and economic quality of life. These categories largely match the findings in our study, although we found some inconsistencies between qualitative and quantitative evidence (e.g. about the availability of spouses, family or friends).
With regard to such inconsistencies, a recent narrative review of the influence of the environment on reengagement 94 found that, although disabled people had identified several environmental facilitators and barriers to their reengagement, a corresponding facilitating or hindering environment generally did not lead to greater or lower reengagement outcomes. It could be that these facilitators and barriers were not strong enough to actually make a difference 94 or that the measures used to capture the difference were not sensitive enough to register it. However, it could also be due to a difference in underlying ideas about what is ‘optimal’ in respect to reengagement. As was shown in our review study, quantitative studies often see independence or easy performance as ideal, whereas for stroke-survivors themselves, reengagement is primarily about feeling respected and being a valued member of society. 95 Perhaps the availability of significant others (e.g. spouses or colleagues) does not always add to stroke-survivors’ objective levels of independence or easy performance, but it nevertheless seems vital for stroke-survivors to feel included within family, work or society.
Future research should clarify the inconsistency between outcomes from qualitative and quantitative research. Developing quantitative measures that reflect the meaning of optimal reengagement as it is understood by stroke-survivors could help make qualitative and quantitative findings more comparable.
Clinicians can use the findings from this review to verify barriers and resources present in the living environments of stroke-survivors. Because these findings came from studies with various objectives, inclusion criteria and designs, not all of them apply to all stroke-survivors in all circumstances. It is nevertheless worthwhile for clinicians to keep the findings of this review in mind, as it can draw their attention to those environmental factors that are often experienced as facilitators or barriers in reengagement in general, as well as in more specific types of valued activities. Apart from this, clinicians should be aware that what stroke-survivors perceive as optimal with regard to reengagement does not always mirror existing clinical measures. Depending on the aim of treatment, clinicians should consider using both objective and subjective measures to examine stroke-survivors’ ability to reengage in their valued activities.
Strengths and limitations
To our knowledge, this is the first mixed-method systematic review of environmental determinants of valued activities post-stroke. The strength of this study was the broad search; by using a comprehensive combination of keywords related to common activities and contexts, we were able to collect a relevant data set that can inform clinical practice and research. Since we chose not to include studies about professional services, the data about services, systems and policies are incomplete.
Another strength was the integrative approach we used to combine qualitative and quantitative findings, which resulted in a detailed picture of knowledge available on environmental factors and reengagement post-stroke. However, the original studies used different terminology, measurements and methods of analysis. The quantitative studies analysed a set of pre-set environmental factors, while most of the qualitative studies let the environmental factors emerge from the data. The methods used in the qualitative studies furthermore varied in the extent to which they interpreted or just described the data. We therefore had to be cautious about which findings could be compared or combined, and what final conclusions could be drawn.
Because of the diversity of the included studies and the low levels of evidence found, the conclusions of this review may be considered global or preliminary by nature. Nevertheless, in the absence of more precise research findings, our results provide a good first indication of environmental factors that play a role in stroke-survivors’ valued activities.
Clinical messages
There is inconsistency between what stroke-survivors see as ‘optimal’ with regard to their reengagement in valued activities and what is measured by commonly used participation measures.
Others’ positive attitudes and behaviours seem to be especially crucial for stroke-survivors to enable them to become reengaged in social, community and work-related activities.
Footnotes
Acknowledgements
We thank Dr Yvonne Heerkens for her advice on the application of the ICF.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a HAN University of Applied Sciences PhD scholarship.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.