
Abstract
Objective:
To investigate the short-term effects of the life goal concept on subjective well-being and treatment engagement, and to determine the sample size required for a larger trial.
Design:
A quasi-randomized controlled trial that was not blinded.
Setting:
A subacute rehabilitation ward.
Subjects:
A total of 66 patients were randomized to a goal-setting intervention group with the life goal concept (Life Goal), a standard rehabilitation group with no goal-setting intervention (Control 1), or a goal-setting intervention group without the life goal concept (Control 2).
Interventions:
The goal-setting intervention in the Life Goal and Control 2 was Goal Attainment Scaling. The Life Goal patients were assessed in terms of their life goals, and the hierarchy of goals was explained. The intervention duration was four weeks.
Main measures:
Patients were assessed pre- and post-intervention. The outcome measures were the Hospital Anxiety and Depression Scale, 12-item General Health Questionnaire, Pittsburgh Rehabilitation Participation Scale, and Functional Independence Measure.
Results:
Of the 296 potential participants, 66 were enrolled; Life Goal (n = 22), Control 1 (n = 22) and Control 2 (n = 22). Anxiety was significantly lower in the Life Goal (4.1 ±3.0) than in Control 1 (6.7 ±3.4), but treatment engagement was significantly higher in the Life Goal (5.3 ±0.4) compared with both the Control 1 (4.8 ±0.6) and Control 2 (4.9 ±0.5).
Conclusions:
The life goal concept had a short-term effect on treatment engagement. A sample of 31 patients per group would be required for a fully powered clinical trial.
Introduction
Often when admitted to a rehabilitation ward, a patient expects to achieve a full recovery, but this goal is usually not achievable; for example, some important premorbidity life goals are no longer attainable or are attainable only within limited constraints. This violates patients innate needs for orientation and control, 1 which the patients must regain by adapting their life goals to their changed circumstances. 2 In the field of rehabilitation, the life goal concept is used to assist in this process.3,4,5
The life goal concept was introduced in the 1970s as a dimension of motivation. Life goals are defined as “the desired states that people seek to obtain, maintain or avoid.” 6 Life goals are commonly thought to be derived from core aspects of self-identity and are determined by high-level abstract motivation. Indeed, the consideration of life goals has been deemed important in the delivery of rehabilitation services, in light of the influence of a patient’s life goals on his or her motivation and subjective well-being.3,7,8
The effects of the life goal concept have been investigated using several psychological models. The relationship between life goals and subjective well-being has been investigated using Carver and Scheier’s control-process model.9,10 This model is based on feedback control, such that action is undertaken to minimize the discrepancy between the patient’s current state and his or her goals. The central thesis of this model is that the patient experiences emotional distress if the rate of approach to his/her life goals is different from the desired rate.
The relationship between life goals and motivation has been investigated using Powers’ hierarchical model, 11 which proposes that there is a hierarchy of goals ranging from high-level abstract goals to very concrete goals related to specific actions. In this hierarchy, goals at any level are determined by the goal at the next level up in the hierarchy.12,13 Therefore, recognizing the hierarchy of life goals leads to motivation to engage in the lower-level actions. In their qualitative study regarding the place of life goals in rehabilitation, Martin et al. reported that all of the participants described the value of discussing life goals with staff, and the support of staff such as in the integration of daily activities with the patient’s life goals was important to give patients a sense of motivation and to help them maintain a high level of engagement in daily activities. 14 For this reason, Nair has argued that there should always be an explicit link between rehabilitation goals and the patient’s life goals. 3
In their study of the effect of the life goal concept on the improvement of patient outcomes, McGrath et al. reported that patient-centered goal planning that was focused on life goals decreased anxiety in patients with an acquired brain injury. 9 Coote et al. noted that goal-setting focused on life goals improved the subjective well-being of patients with depression. 15 Stanhope et al. reported that person-centered care focused on life goals improved the treatment engagement of patients with mental illness. 16 However, the effect of adding the life goal concept to the goal-setting used in standard rehabilitation is not clear, because the above studies had no control group and/or there was no structured goal-setting in the control group. 17
In the present study, we attempted to determine the short-term effects of goal-setting focusing on the life goal concept, before a larger trial is undertaken to investigate the effectiveness of the life goal concept in subacute patients. We also calculate the sample size required for a larger trial. We hypothesized that goal-setting with the life goal concept would have beneficial effects on subjective well-being and treatment engagement in comparison with goal-setting without the life goal concept.
Methods
This was a quasi-randomized controlled trial that was not blinded. This study recruited participants from among the patients hospitalized at the Kaifukuki (convalescent) rehabilitation ward of Nishiyamato Rehabilitation Hospital in Nara Prefecture, Japan. Patients in whom the onset of disabling diseases had occurred within the previous one or two months were eligible for admission to the Kaifukuki rehabilitation ward. About 300 patients are admitted to this ward each year. Of these patients, approximately 50% have sustained orthopedic diseases, 40% have had a stroke, a traumatic brain injury, or other neurological diseases, and 10% have disuse syndrome. The duration of physical, occupational, or speech therapy sessions is up to three hours per day in total, and the proportion of therapy time is decided according to the needs of each patient.
The inclusion criteria of the present study included all of the hospitalized patients, because the life goal concept can be applied in a variety of diseases, and it has been proposed that rehabilitation medicine should incorporate broader inclusion criteria. 18 We excluded patients who had severe cognitive dysfunction (Mini-Mental State Examination ≦ 23), 19 those who were to be discharged within four weeks, those with a history of mental illness, severe blindness or hearing impairment, and those from whom consent for participation could not be obtained.
No formal power calculation was performed, because there is no previous study that investigated the effects of subjective well-being and treatment engagement. This study was approved by the ethics committee of Kio University (No. H25-27) and conformed to the principles outlined in the Declaration of Helsinki. This study was not registered with the Clinical Trials Registry.
Immediately after a baseline assessment, the patients were quasi-randomized to three groups by alternate allocation according to their order of hospitalization by a research assistant who was involved in the present study. It was not possible to conceal the group allocation, because the attending therapist was informed of the allocation of each patient by the research assistant so that the assigned intervention would be used. We also used stratified randomization according to the patients’ anxiety, using the patients’ scores on the Hospital Anxiety and Depression Scale (a cut-off score of ⩾8 vs. <8). 20
To examine the effect of adding the life goal concept to the standard rehabilitation goal-setting, we used three groups with different goal-setting interventions. The Control 1 group underwent standard rehabilitation with no structured goal-setting intervention. The Control 2 group underwent Goal Attainment Scaling as the structured goal-setting intervention. 21 The Life Goal group underwent Goal Attainment Scaling in combination with the life goal concept. We used Goal Attainment Scaling in order to unify the goal-setting method in the standard rehabilitation, because the type of goals is set based on the SMART principle (Specific, Measurable, Achievable, Realistic, and Time-phased), 22 and the processes of goal-setting are defined in structured steps.23,24,25
All of the patients received the intervention delivered by multiple therapists three hours a day, six days a week for four weeks. The Control 1 group underwent the standard rehabilitation at our hospital, which provides a treatment that is focused on improving body functions and structures, activities, and participation based on the International Classification of Functioning, Disability and Health. The contents of the standard rehabilitation were specific to each patient; for example, the rehabilitation included a muscle-strengthening exercise, a range-of-motion exercise, task-oriented training, and activities of daily living (ADL) training.
The Control 2 group underwent Goal Attainment Scaling without the life goal concept. We used four steps in the development of Goal Attainment Scaling.23,24 In the first step, therapists set from three to five high-priority goals based on information from the patient and his or her family. In the second step, the therapists graded the attainment of the predicted goal after four weeks. Each goal was graded on a five-point scale according to the method of Krasny-Pacini: 25 “−2” is the baseline level, “−1” represents progression towards the goal without goal attainment, “0” is the expected level after intervention, “+1” represents a better outcome than expected, and “+2” is the best possible outcome that could have been expected for this goal. In the third step, the goals were weighted by importance and difficulty, each of which was graded on a four-point scale ranging from 0 (not at all important/difficult) to 4 (very important/difficult). In the fourth step, the therapists provided feedback on goal attainment to the patient once a week, and they reassessed the patient’s goal attainment after four weeks. The goal attainment level is described by the Goal Attainment Score, which is calculated according to the following formula:
where wi is the weight (importance × difficulty) assigned to the goal area and xi is the attained score for the goal area.
The Life Goal group subjects underwent Goal Attainment Scaling in combination with the life goal concept. The goal-setting focusing on the life goal concept was conducted according to Nair’s method. 3 The patient’s life goals were assessed by the attending therapist using the Rivermead Life Goal Questionnaire. 4 This questionnaire addresses nine aspects or areas of life; residential and domestic arrangements, ability to manage personal care, leisure, work, relationship with partner, family life, contacts with friends, religion or life philosophy, and financial status. The patient rates the importance of his or her life goals on a scale of 0 (no importance), 1 (some importance), 2 (great importance), or 3 (extreme importance), and then the patient selects the three important areas according to the high priority. The patient’s life goals were then shared with the attending therapists, and rehabilitation goals were set with reference to the patient’s life goals. Also, the coherence between the rehabilitation goals and the patient’s life goals was explained to the Life Goal group in addition to the feedback they received once a week. All trial therapists in the present study received a two-hour lecture about Goal Attainment Scaling and goal-setting focusing on the life goal concept. After this lecture, our study’s research group further instructed the therapists who were to provide the patients’ interventions.
We obtained baseline characteristics such as the patient’s age, gender, household composition, time from onset of injury, diagnosis, and Mini-Mental State Examination score from medical records. For the outcome assessments, a preintervention test (pretest) was performed within 10 days after admission, and a postintervention test (posttest) was performed after intervention. As the outcome measures, we used the patients’ scores on the Hospital Anxiety and Depression Scale, the 12-item General Health Questionnaire, the Pittsburgh Rehabilitation Participation Scale, and the Functional Independence Measure. We used the Patient Participation Scale as a questionnaire after the intervention. Although the outcome assessments were done by an attending therapist who was not blinded to the group allocation, the questionnaire was done by research assistants who were blinded to the group allocation.
We used the Hospital Anxiety and Depression Scale and the 12-item General Health Questionnaire as measures of subjective well-being. 26 The Hospital Anxiety and Depression Scale was used to assess the severity of anxiety and depression. 20 In this scale, each item is answered on a four-point scale; the possible anxiety subscale scores range from 0 to 21, and the depression subscale scores range from 0 to 21. The Japanese version of the Hospital Anxiety and Depression Scale has high reliability and validity. 27
The 12-item General Health Questionnaire, which is a modified shorter version of an originally 60-item questionnaire, was used to assess the patients’ emotional well-being. 28 We applied the General Health Questionnaire scoring in which each item’s response categories are coded 0–0–1–1, with the possible scores ranging from 0 to 12. The Japanese version of the 12-item General Health Questionnaire has high reliability and validity. 29
We used the Pittsburgh Rehabilitation Participation Scale to assess the degree of patient engagement in the rehabilitation setting. 30 This assessment is a six-point scale of observed treatment engagement (effort and motivation). Attending therapists rated the patient’s average treatment engagement in the past week. This scale has high reliability and validity, but a Japanese version has not reported the psychometric properties.
The Functional Independence Measure was used to assess the patient’s independence in ADL. 31 Each item is answered on a seven-point scale, and the possible scores range from 18 to 126. Higher scores indicate better functional status. The Japanese version of the Functional Independence Measure has high reliability and validity. 32
To assess each patient’s perception about their involvement in the goal-setting process, we used the Patient Participation Scale.33,34 With this scale, the patient chooses from among four options regarding the level of decision-making in the goal-setting: no choice, forced choice, multiple choice, and free choice. High scores indicate a high level of the degree of decision-making related to goal-setting. The psychometric properties of the Patient Participation Scale have not been reported.
Statistics
The normal distributions of all data were tested by the Shapiro–Wilk test. As a result, we used non-parametric tests because there was no normality of the posttest data. We used an analysis of variance for continuous variables and the chi-square test for dichotomous variables to analyze the differences in baseline characteristics. A post hoc analysis was performed using Tukey’s test. We used the Wilcoxon signed-rank test to analyze the pretest vs. posttest differences within the group. We performed a Kruskal–Wallis test to analyze the pretest and posttest differences between the groups. The post hoc analysis was performed using the Steel–Dwass test. We performed Mann–Whitney U-tests to analyze the Goal Attainment Score, the importance of the goals, and the difficulty of the goals between the groups.
The effect sizes (Cohen’s d) were calculated using the pretest and posttest; values for Cohen’s d of 0.2, 0.5, and 0.8 were interpreted as small, moderate, and large, respectively. 35 The statistical power and sample size for a fully powered clinical trial were calculated using the computer program G*Power after the data collection. An intention-to-treat analysis was performed; if a drop-out assessment was not possible, the last available score was continued. The effects were considered significant if the P-value was less than 0.05. All analyses were performed using JMP® 12 (SAS Institute Inc., Cary, NC, USA).
Results
A total of 296 patients were admitted to the rehabilitation ward from September 2013 to August 2014, and 230 patients were excluded because they did not meet the inclusion criteria or declined to participate (Figure 1). Consequently 66 (22.3%) patients were enrolled in this study, and 59 (89.4%) were retained up to the posttest. Of the 66 participants, two Life Goal group patients (both discharged within the first four weeks), three Control 1 group patients (one discharged within the first four weeks, one whose condition deteriorated, and one who declined to participate further), and two Control 2 group patients (one discharged within the first four weeks and one who declined to participate further) were withdrawn from the study before the posttest.
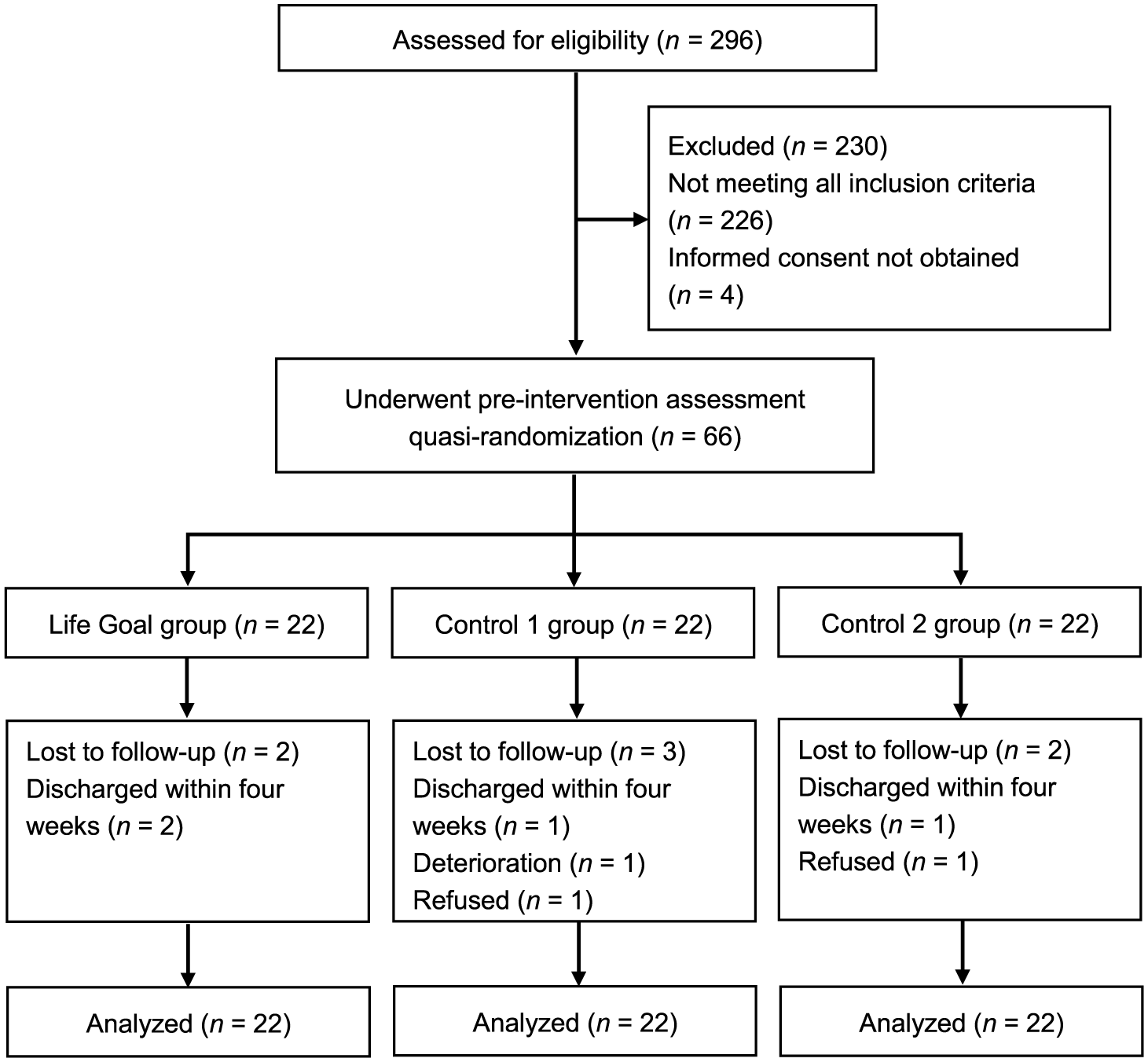
Flow diagram of the patient population.
Table 1 provides the baseline characteristics and the Patient Participation Scale scores of all patients. There were no significant differences in these characteristics or scores among the three intervention groups.
Characteristics of the three groups.
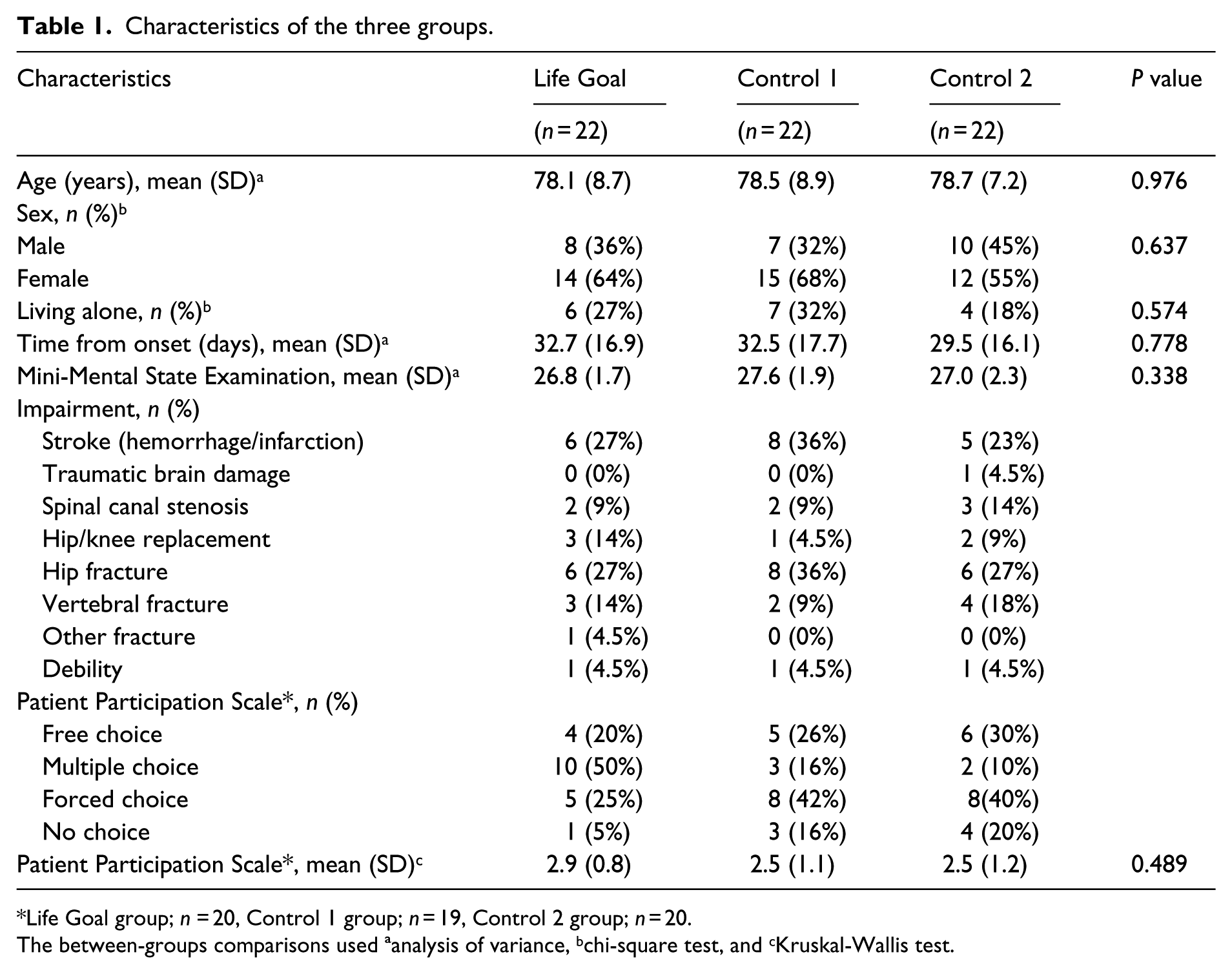
Life Goal group; n = 20, Control 1 group; n = 19, Control 2 group; n = 20.
The between-groups comparisons used ªanalysis of variance, bchi-square test, and cKruskal-Wallis test.
Table 2 shows the comparison of the pretest vs. posttest scores within each of the three groups. The anxiety assessed by the Hospital Anxiety and Depression Scale decreased significantly in the Life Goal group (P = 0.013, d = 0.624) and Control 2 group (P = 0.028, d = 0.500), but the Control 1 group showed no significant difference in their anxiety pretest vs. posttest scores (P = 0.305, d = 0.262). The depression assessed by the Hospital Anxiety and Depression Scale showed no significant pretest vs. posttest difference in the Life Goal group (P = 0.099, d = 0.417), the Control 1 group (P = 0.975, d = 0.150) or Control 2 group (P = 0.106, d = 0.402). The 12-item General Health Questionnaire scores decreased significantly in the Life Goal group (P < 0.001, d = 0.801), the Control 1 group (P = 0.039, d = 0.467) and Control 2 group (P = 0.038, d = 0.488). The Pittsburgh Rehabilitation Participation Scale scores increased significantly in the Life Goal group (P < 0.001, d = 0.818) and Control 2 group (P = 0.043, d = 0.438), but the Control 1 group showed no significant change (P = 0.184, d = 0.226). The Functional Independence Measure increased significantly in the Life Goal group (P < 0.001, d = 1.104), the Control 1 group (P < 0.001, d = 1.125), and Control 2 group (P < 0.001, d = 1.487).
Changes in outcome measures within the three patient groups after four weeks.
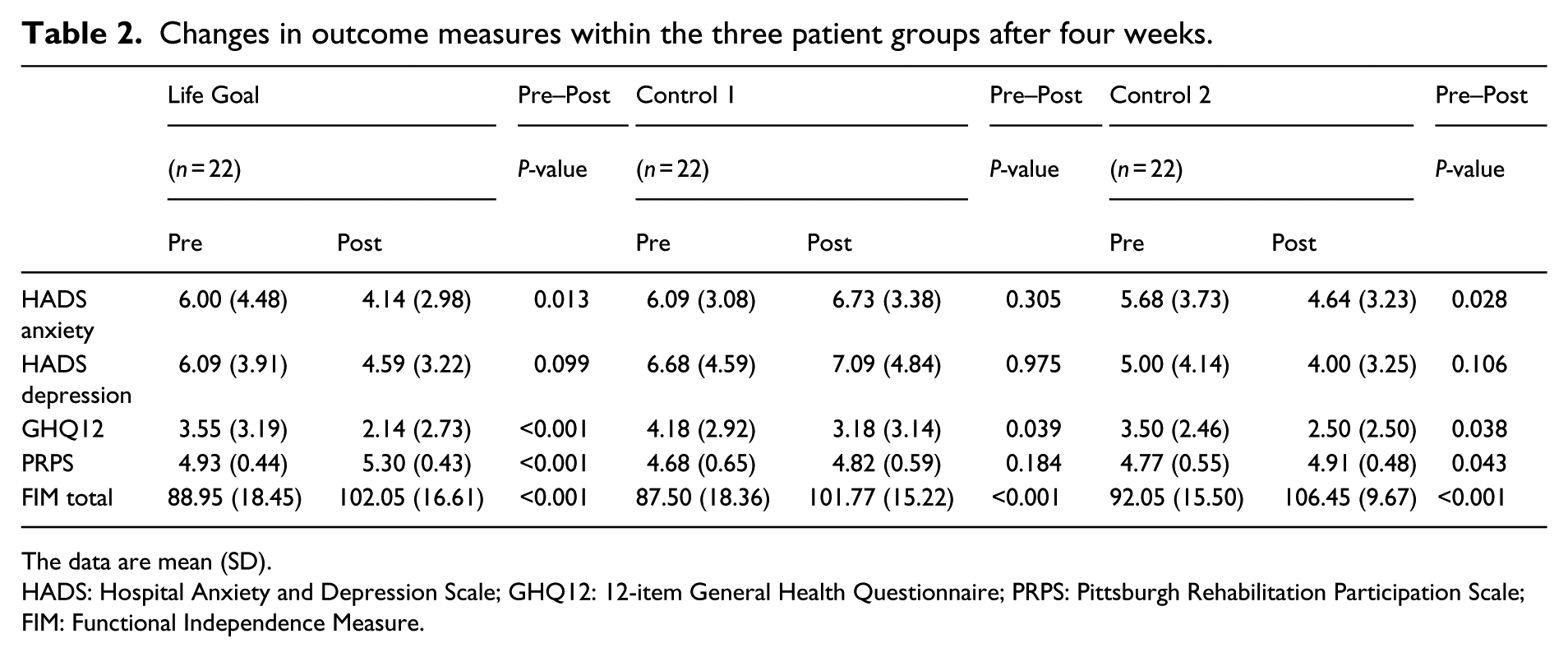
The data are mean (SD).
HADS: Hospital Anxiety and Depression Scale; GHQ12: 12-item General Health Questionnaire; PRPS: Pittsburgh Rehabilitation Participation Scale; FIM: Functional Independence Measure.
Table 3 shows the results of our comparison of the pretest and posttest scores among the three intervention groups. The analyses showed no significant differences in any of the pretest scores among the groups. In the comparison of the posttest scores among the groups, the anxiety scores showed a significant difference (χ2 = 8.162, P = 0.017) and the post hoc test showed a significant difference between the Life Goal group and the Control 1 group (P = 0.017, d = 0.813), but no significant difference was revealed between the Life Goal group and the Control 2 group (P = 0.879, d = 0.161), or between the Control 1 group and the Control 2 group (P = 0.098, d = 0.632).
Comparison of pre- and posttest among three groups in outcome measures.
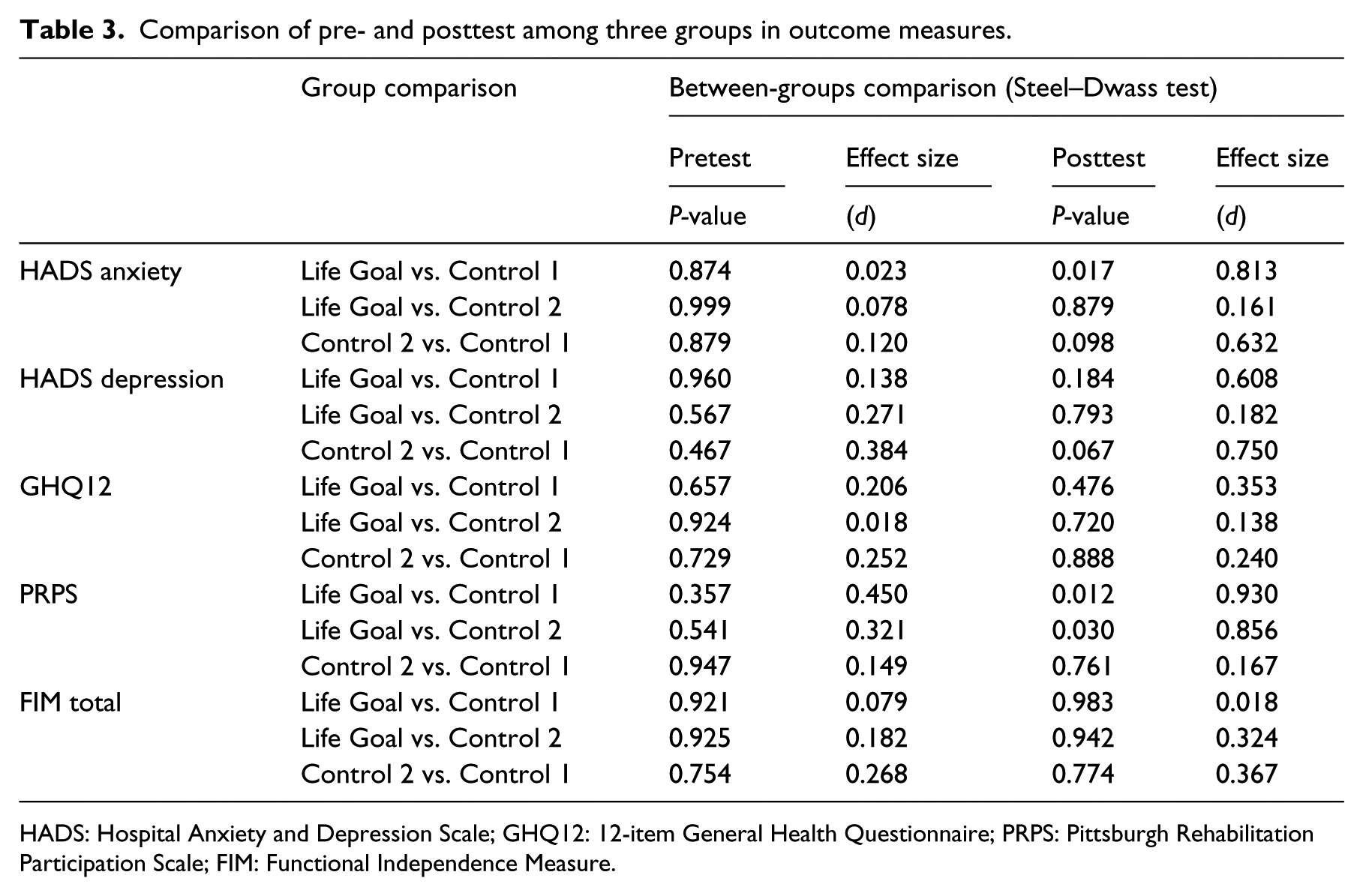
HADS: Hospital Anxiety and Depression Scale; GHQ12: 12-item General Health Questionnaire; PRPS: Pittsburgh Rehabilitation Participation Scale; FIM: Functional Independence Measure.
The Pittsburgh Rehabilitation Participation Scale showed a significant difference (χ2 = 10.163, P = 0.006) and the post hoc test showed significant differences between the Life Goal group and the Control 1 group (P = 0.012, d = 0.930) and between the Life Goal group and the Control 2 group (P = 0.030, d = 0.856), but no significant difference between the Control 1 group and the Control 2 group (P = 0.761, d = 0.167). The 12-item General Health Questionnaire and the Functional Independence Measure showed no significant differences in the comparison of the posttest scores between the groups.
Table 4 provides the results of our comparison of the Goal Attainment Scaling and the number of goals for each domain between the Life Goal group and the Control 2 group. No significant differences in the Goal Attainment Score, importance, or difficulty of goals were observed between these two groups. The numbers of goals for each domain were largely similar in content between the Life Goal and the Control 2 groups.
Comparison of the Goal Attainment Scaling between the Life Goal group and the Control 2 group.
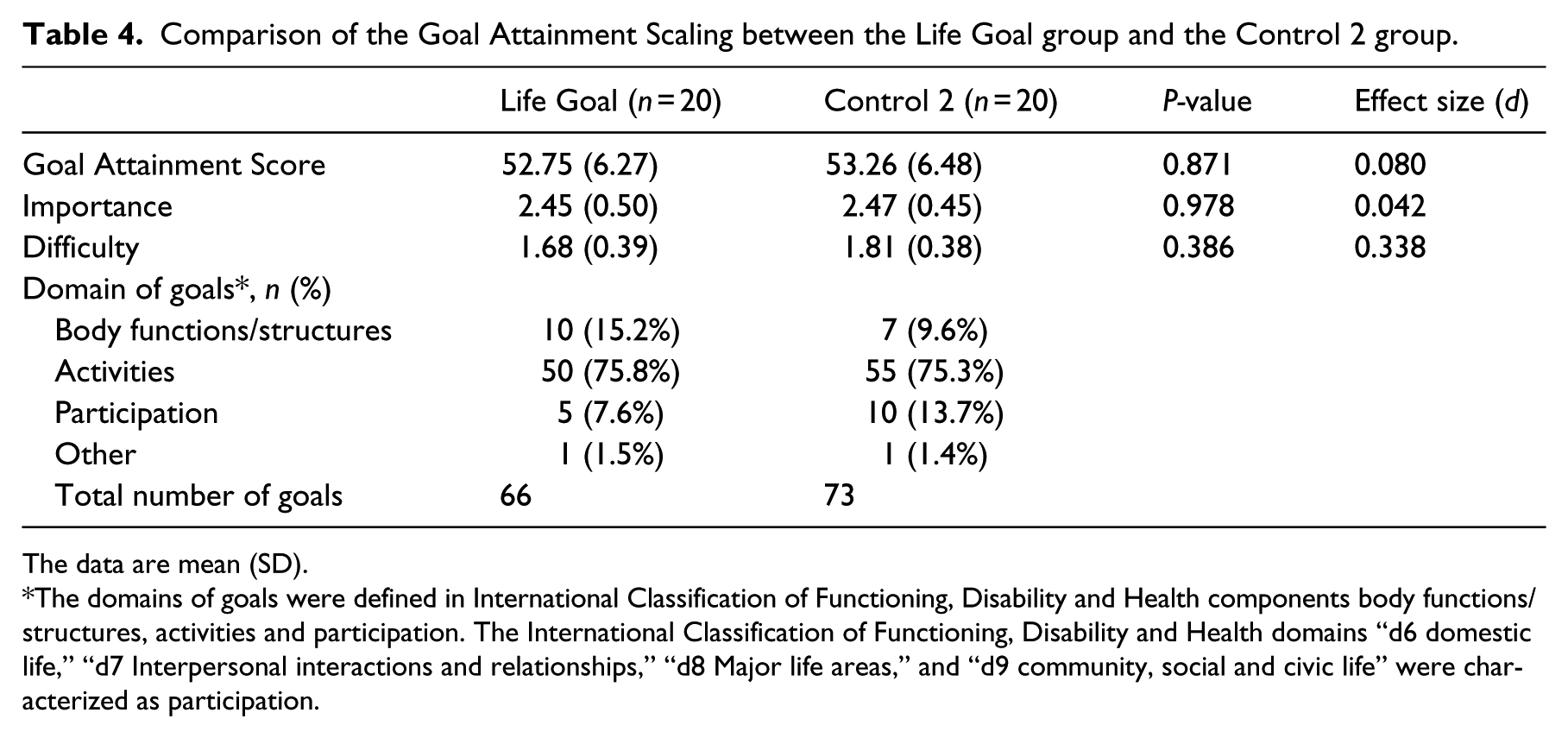
The data are mean (SD).
The domains of goals were defined in International Classification of Functioning, Disability and Health components body functions/structures, activities and participation. The International Classification of Functioning, Disability and Health domains “d6 domestic life,” “d7 Interpersonal interactions and relationships,” “d8 Major life areas,” and “d9 community, social and civic life” were characterized as participation.
We focused on the Pittsburgh Rehabilitation Participation Scale to estimate the required sample size for a fully powered clinical trial. The difference in the posttest scores on this scale between the Life Goal group and the Control 1 group was 0.48 points, and the effect size was 0.930; the statistical power was 72%. The difference in the posttest score on this scale between the Life Goal group and the Control 2 group was 0.39 points, and the effect size was 0.856; the statistical power was 63%. Based on these results, we calculated a required sample size of 31 patients per group (power 80%; alpha 0.016) for a fully powered clinical trial.
Discussion
We investigated the short-term effects of goal-setting focusing on the life goal concept on the subjective well-being and treatment engagement among patients in a subacute rehabilitation ward. Our results supported the hypothesized effect of the life goal concept on treatment engagement, but it did not completely support the hypothesis on the effect of subjective well-being.
We used the Hospital Anxiety and Depression Scale and the 12-item General Health Questionnaire for assessing subjective well-being, and these two outcome measures showed different results. The anxiety scores decreased significantly in only the patients who received the structured goal-setting intervention, i.e. the Life Goal group and the Control 2 group. LaFerriere et al. reported that with the use of the Goal Attainment Scaling, the effects on anxiety, depression, and self-esteem were greater than those observed without structured goal-setting. 21 Anxiety is defined as a sustained feeling of apprehension or dread about an uncertain future threat, 36 and many patients in a rehabilitation program have experienced emotional distress owing to the slowing, interruption, or uncertainty of the rate of approach to personally meaningful goals. 9 We therefore conclude that the structured goal-setting intervention in the present study helped the patients cope with emotional distress by getting accurate feedback about their performance and progress. Moreover, the Life Goal group showed a larger effect size compared with the Control 2 group. Brunstein et al. contended that the progress toward motive-congruent goals was associated with daily experiences of subjective well-being. 37 We thus speculated that a focus on coherence between a patient’s motive and rehabilitation goals is more effective in anxiety.
On the other hand, the 12-item General Health Questionnaire scores were significantly improved in all three groups in the present study. O’Connor et al. reported that their patients’ ADLs and emotional well-being were significantly improved during hospitalization, but the patients’ anxiety scores showed no significant change. 38 In the present study, the Functional Independence Measure scores were also improved in all three groups. Thus, if a study’s subjects are recruited from among the patients in a subacute rehabilitation ward, the effect of emotional well-being is likely to be dependent on the improvement of ADL rather than the effect of the goal-setting intervention.
With regard to treatment engagement, the Pittsburgh Rehabilitation Participation Scale score increased significantly only in patients who received the combination of goal-setting intervention and the life goal concept. Coppack et al. reported that a goal-setting intervention using performance profiling has the potential to improve adherence in clinical rehabilitation, 39 and we agree that it is important that the values and priorities of the patient are included in rehabilitation goals. In this study, the Patient Participation Scale showed no significant differences among the groups. On the other hand, in the comparison of items in the Patient Participation Scale between the groups, the Life Goal patients tended to rate many of the multiple choice items compared with the other groups. Therefore, the treatment engagement might have been influenced by the method of the decision-making process in the goal-setting more than the level of decision-making in the goal-setting. However, it is not yet known which specific type of communication is important, because the assessment of communication between the patient and therapist in the decision-making process was not performed.
The Goal Attainment Score and the number of goals for each domain showed no significant differences between the groups. This means that even if the therapist knew a patient’s life goals, the therapist may not have used the goals directly in devising the patient’s rehabilitation goals. Nevertheless, the Life Goals group showed a higher treatment engagement than the other two groups. Sheldon et al. reported that the coherence of life goals and the daily goals was associated with high motivation and positive emotion. 40 In addition, patient engagement in the rehabilitation setting is considered to be dependent on the coherence between the rehabilitation goals and the patient’s life goals. 3 We thus propose that an intervention process that includes an assessment of life goals and an explanation of goal hierarchy is effective for increasing treatment engagement.
In our within-group comparisons, the Functional Independence Measure scores increased significantly in all groups, but no significant difference was observed among the groups in the posttest scores. With respect to the relevance of ADL and treatment engagement, Lenze et al. reported that there was a significant difference in ADL (not only treatment engagement) in their intervention designed to increase patient engagement compared with the control group. 41 However, since in the present study the intervention period was only four weeks in patients with subacute disorders, the improvement of their ADL is likely to have depended on natural recovery rather than treatment engagement.
Based on the Pittsburgh Rehabilitation Participation Scale results, we estimated that a sample of 31 patients per group would be required for a larger study. However, we would need much larger samples to test effects on subjective well-being, because the Hospital Anxiety and Depression Scale and the 12-item General Health Questionnaire have low statistical power.
Study limitations
This study has a number of limitations. First, the study design was a quasi-randomized controlled trial that was not blinded, and it was not possible to conceal the group allocations. This design may be not sufficient to prove the efficacy of the life goal concept.
Second, the lecture about Goal Attainment Scaling and goal-setting focusing on the life goal concept was conducted for all of the therapists who participated in the study, because all of the therapists had to perform all interventions. For this reason, a bias might have occurred owing to the application of principles across different groups. However, the concealment of group allocation and the bias caused by the lecture may be addressed by a cluster randomized clinical trial design.
Third, we employed the Pittsburgh Rehabilitation Participation Scale to measure the patient engagement in the rehabilitation setting, because we considered that the use of the life goal concept affects the motivation for the individual rehabilitation goals rather than the motivation for exercise. The Pittsburgh Rehabilitation Participation Scale is a single-item scale designed to capture the therapist’s perception of the patient’s participation in the treatment session. For this reason, the patient’s own motivation was unknown. However, it may be difficult to assess the patients’ own motivation because the purpose and goals of rehabilitation are different for each patient.
Fourth, the generalizability of the interventions might be limited given that over 75% of the candidate patients were deemed ineligible to join the present study. Also, many of the ineligible patients had cognitive dysfunction. However, we considered the exclusion criteria of the present study were appropriate because cognitive impairment was reported to be a limitation of the goal-setting intervention. 42
Clinical messages
Goal-setting focused on the life goal concept resulted in better treatment engagement compared with the goal-setting in standard rehabilitation.
The coherence between the rehabilitation goals and the patient’s life goals may be important to the improvement of treatment engagement.
Footnotes
Acknowledgements
We thank our research assistants Tomoki Katayama, Haruhiko Kishi, Kento Kano, and all the staff of the Nishiyamato Rehabilitation Hospital who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.