
Abstract
Objective:
To identify predictors of pain and disability in knee osteoarthritis.
Design:
A one-year prospective analysis of determinants of pain and functioning in knee osteoarthritis.
Study setting:
Primary care providers in a medium-sized city.
Patients:
A total of 111 patients aged from 35 to 75 with clinical symptoms and radiographic grading (Kellgren-Lawrence 2–4) of knee osteoarthritis who participated in a randomized controlled trial.
Main measures:
The outcome measures were self-reported pain and function, which were recorded at 0, 3 and 12 months. Disease-specific pain and functioning were assessed using the pain and function subscales of the Western Ontario and McMaster Universities (WOMAC) Osteoarthritis Index. Generic physical and mental functioning were assessed using the RAND-36 subscales for function, and physical and mental component summary scores. Possible baseline predictors for these outcomes were 1) demographic, socioeconomic and disease-related variables, and 2) psychological measures of resources, distress, fear of movement and catastrophizing.
Results:
Multivariate linear mixed model analyses revealed that normal mood at baseline measured with the Beck Anxiety Inventory predicted significantly better results in all measures of pain (WOMAC P=0.02) and function (WOMAC P=0.002, RAND-36 P=0.002) during the one-year follow-up. Psychological resource factors (pain self-efficacy P=0.012, satisfaction with life P=0.002) predicted better function (RAND-36). Pain catastrophizing predicted higher WOMAC pain levels (P=0.013), whereas fear of movement (kinesiophobia) predicted poorer functioning (WOMAC P=0.046, RAND-36 P=0.024).
Conclusions:
Multiple psychological factors in people with knee osteoarthritis pain are associated with the development of disability and longer term worse pain.
Introduction
There is an emerging consensus that the degree of knee pain and disability symptoms among osteoarthritis patients appears to rest upon a complex interaction of factors, including structural damage, peripheral and central pain processing mechanisms, obesity, culture, and demographic as well as psychosocial factors.1,2 For instance, the European Project on Osteoarthritis concluded that advanced age, female gender, lower educational attainment and a higher body mass index were independently associated with disability. 3 With respect to structural damage, it has been shown that pain does not always accompany radiological findings of knee osteoarthritis. 4 Furthermore, the radiographic severity of knee osteoarthritis has been reported to have a weak or no association with disability in these patients. 5
Increasing evidence has suggested the importance of psychological (affective, cognitive, behavioural) variables in explaining and predicting osteoarthritis pain and disability.6,7 According to a population-based survey of individuals living in 17 countries, depression and anxiety disorders occurred significantly more often among those with self-reported arthritis. 8 In a study by Smith and Zautra 9 among women with osteoarthritis, measures of anxiety and depression emerged as independent and significant predictors of current and next week pain, with anxiety having almost twice the effect of depression.
Over the past 15 years, pain-related cognitions, such as pain catastrophizing and self-efficacy, have become a major interest in psychosocial pain research. Pain catastrophizing refers to the tendency to ruminate about pain and magnify it. Somers et al. 10 reported in a cross-sectional setting that pain catastrophizing explained a significant proportion of the variance in measures of pain, psychological disability, physical disability and gait velocity in overweight and obese patients with knee osteoarthritis. Fear of movement or kinesiophobia is another variable used to describe negatively charged emotions towards pain and function. Heuts et al. 11 concluded that pain-related fear was significantly associated with functional limitations among osteoarthritis patients. Self-efficacy, on the other hand, represents a more positive aspect of adjusting to pain. Self-efficacy is a concept used to describe the strength of one’s beliefs in one’s ability to complete tasks and reach goals. According to a systematic review by Benyon et al., 6 there is strong evidence that self-efficacy predicts disability but not pain among osteoarthritis patients.
Several psychological variables have been studied in relation to pain and function among patients with chronic musculoskeletal diseases. However, the number of studies investigating the predictive role of psychological factors in knee osteoarthritis is somewhat scarcer. In this analysis, we assessed whether disease-specific, demographic and psychological factors at baseline predict self-reported pain and function during a one-year follow-up of a randomized controlled trial among patients with knee osteoarthritis. 12
Patients and methods
The study participants were 111 patients with radiologically (Kellgren-Lawrence 2–4) 13 diagnosed knee osteoarthritis and associated pain symptoms. They participated in a randomized controlled trial with a group-based cognitive-behavioural intervention to treat pain, and were followed up for one year. 14 The outcome measures were recorded at 0-, 3-, and 12-month follow-up points using postal questionnaires. The questionnaires included questions about knee pain and physical function, demographic, socioeconomic and disease-related variables and psychological variables.
Questionnaires for knee pain and physical function
The outcome measures in this analysis were self-reported pain and functioning (physical and mental). The following measures were used: Disease-specific pain and physical functioning were measured with the pain and function subscales (0−100 mm) of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) using the Finnish validated version. 15 The self-reported generic assessments of physical and mental functioning were assessed with the Finnish validated SF-36-item Health Survey RAND-36 16 subscales for function and physical and mental component summary scores. Both orthogonal and oblique assessments 17 for the summary scores were calculated and used in parallel. We used average and SD values of different RAND-36 subscales in the Finnish population when calculating the component summary scores. 16
Possible baseline predictors
Possible baseline predictors for the outcomes were divided into two groups: 1) Demographic, socioeconomic and disease-related variables and 2) psychological measures of resources and coping, fear of movement and catastrophizing and distress. Baseline predictors were transformed to dichotomous variables before the analysis, except for age, which was maintained continuous.
1) Demographic, socioeconomic and disease-related variables
Demographic, socioeconomic and disease-related variables were age (per 10 years), gender, educational level (comprehensive school vs. upper secondary or vocational school), number of comorbidities, prevalent obesity (normal of overweight with body mass index <30.0 kg/m2 vs. obese with body mass index ⩾30.0 kg/m2), 18 working status (employed vs. retired or unemployed), marital status (cohabiting vs. living alone), radiological grade of knee osteoarthritis (Kellgren-Lawrence scale 2 (minimal) vs. 3–4 (moderate or severe)), 13 duration of knee pain symptoms (<6 (median) vs. ⩾6 years), exercise frequency, the group in the randomized controlled trial (intervention vs. control) and time (baseline vs. 3 and 12 months average).
In the transformation to dichotomous variables, we used cut-off values based on classification systems (body mass index, Kellgren-Lawrence scale) or the median of the observations (duration of the knee symptoms). In the case of exercise frequency, the cut-off value (⩾2 times a week vs. ⩽1 times a week) was chosen with respect to the recommendations of the Physical Activity Guidelines for Americans 19 of strength training at least two times a week. The patients were asked to report how often they exercised with the following response alternatives: daily, 4–6 times a week, 2–3 times a week, once a week, 2–3 times a month, or a couple of times a year or less. For the number of comorbidities, the cut-off (0−2 vs. ⩾3) was chosen on the basis of reasonable group sizes and clinical relevance.
2) Psychological variables
Psychological variables were assessed with questionnaires focusing on psychological resources (life satisfaction, sense of coherence, pain self-efficacy), fear and catastrophizing (kinesiophobia and pain catastrophizing) and mood (depressive symptoms, symptoms of anxiety). In the transformation to dichotomous variables, we used clinical cut-offs defined for each questionnaire when available (Life Satisfaction scale, Tampa Scale of Kinesiophobia, Beck Depression Inventory, Beck Anxiety Inventory). Where a cut-off had not been defined, for clinically meaningful comparisons we used data-driven tertile grouping (Sense of Coherence, Pain Self-Efficacy Questionnaire, Pain Catastrophizing Scale).
Life satisfaction was measured with a four-item Life Satisfaction scale 20 (satisfied, scores 4−11 vs. dissatisfied, scores 12−20) 21 . Sense of coherence was evaluated by using the well-validated 13-item version of the Sense of Coherence scale 22 (scores 59−84 vs. lowest tertile, scores 37−58). Pain self-efficacy was assessed with the Finnish version of the Pain Self-Efficacy Questionnaire 23 (scores 41−60 vs. lowest tertile, scores 0−40) and kinesiophobia with the Finnish version of the Tampa Scale of Kinesiophobia 24 (scores 0−36 vs. high degree of kinesiophobia, scores 37−68) 25 . Pain catastrophizing was evaluated by using the Pain Catastrophizing Scale 26 (scores 0−18 vs. highest tertile, scores 19−50).
Depressive symptoms were assessed using the Finnish version of the 21-item Beck Depression Inventory, which has been found valid and reliable. 27 The cut-off point for depression was set at 9/10 (normal mood, scores 0–9 vs. elevated depressions symptoms, scores 10 or more) according to the original formulation by Beck and Beamesderfer). 28 The Beck Anxiety Inventory 29 was used to evaluate the severity of symptoms of anxiety (normal mood, scores 0–7 vs. mild anxiety or more, scores 8–63). 29 Although the Finnish version of the Beck Anxiety Inventory has previously been used in some studies, exact data on its validity and reliability are scarce.
Statistical analysis
All statistical analyses were performed using SPSS (version 22.0, SPSS, Chicago, IL, USA).
Demographic characteristics and baseline data were summarized with descriptive statistics. The number of study patients in this analysis was based on the power calculations for the original randomized controlled trial, 14 where 54 patients per group (two groups) were needed in the comparison of the mean WOMAC pain scores between the groups.
The associations of possible explanatory variables with the outcome variables were assessed with a multivariate linear mixed model, in which the correlation structure of the data due to the multiple measurements (0, 3 and 12 months) could be taken into account. The mixed model has the advantage of using all available data in the analysis, irrespective of whether some data points are missing for a given participant. Separate models were estimated for each outcome. It has been recommended that covariates should be chosen based on their substantive basis and not on a test of differences. 30 Thus, age, gender, educational level, the number of comorbidities, the body mass index, work status, marital status and disease severity were included as covariates based on their associations with the study outcomes in prior research.3,7,31 The covariates were dichotomised (Table 1) before the analysis, except for age, which was maintained continuous (per 10 years). Finally, a model for demographic, socioeconomic and disease-related variables was fitted in the form:
Parameter estimates (95% confidence intervals) from multivariate linear mixed models with the following explanatory variables (one model per dependent variable) (i.e. average differences in outcome variables of knee pain and functioning between groups of categorical predictors and average change per single unit of continuous predictors).
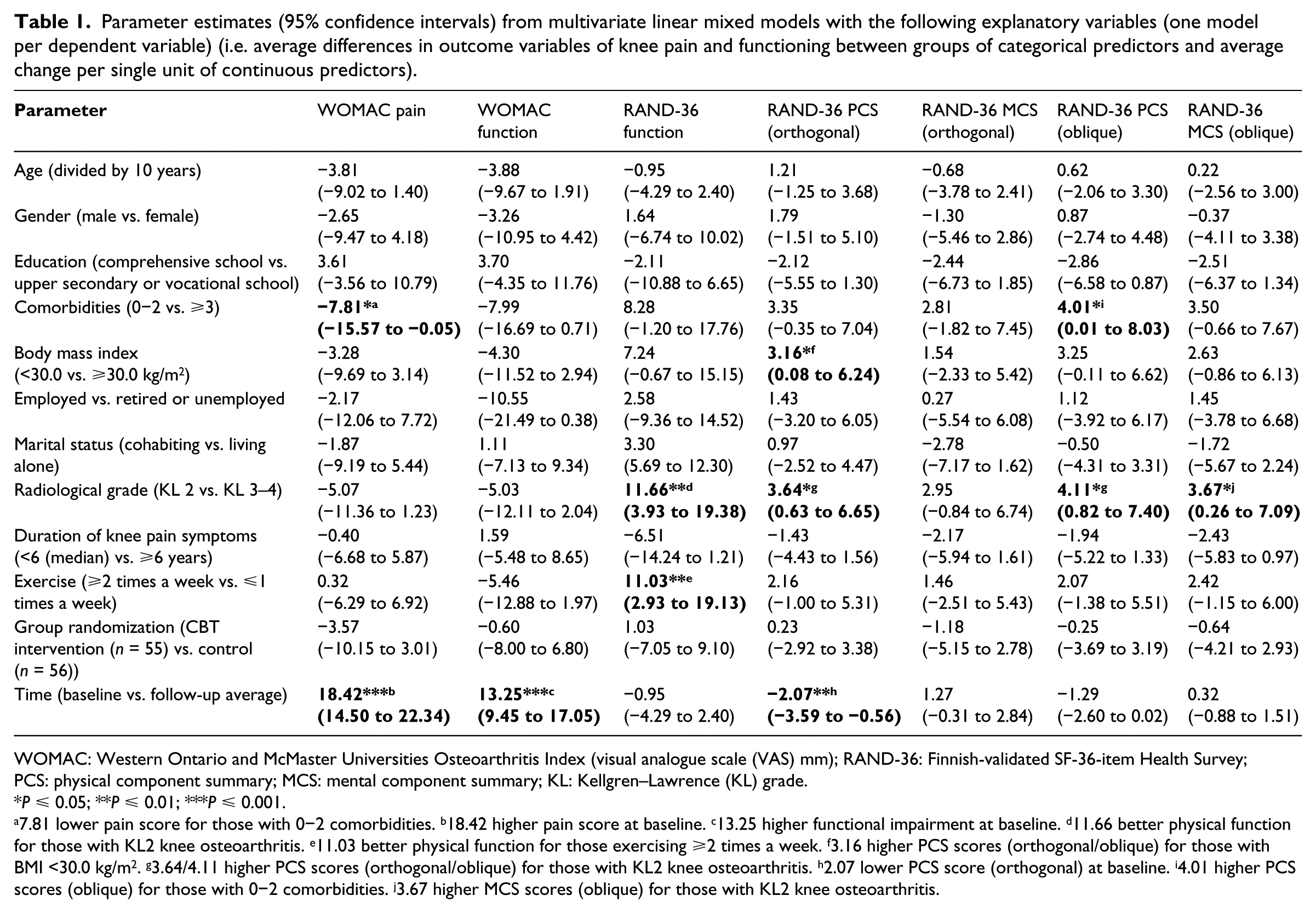
WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index (visual analogue scale (VAS) mm); RAND-36: Finnish-validated SF-36-item Health Survey; PCS: physical component summary; MCS: mental component summary; KL: Kellgren–Lawrence (KL) grade.
P ⩽ 0.05; **P ⩽ 0.01; ***P ⩽ 0.001.
7.81 lower pain score for those with 0−2 comorbidities. b18.42 higher pain score at baseline. c13.25 higher functional impairment at baseline. d11.66 better physical function for those with KL2 knee osteoarthritis. e11.03 better physical function for those exercising ⩾2 times a week. f3.16 higher PCS scores (orthogonal/oblique) for those with BMI <30.0 kg/m2. g3.64/4.11 higher PCS scores (orthogonal/oblique) for those with KL2 knee osteoarthritis. h2.07 lower PCS score (orthogonal) at baseline. i4.01 higher PCS scores (oblique) for those with 0−2 comorbidities. j3.67 higher MCS scores (oblique) for those with KL2 knee osteoarthritis.
Outcome0;3;12 = sex + age + education + comorbidities + body mass index + work status + marital status + radiological grade + duration of knee pain + time+ randomization + time x randomization.
In the same way, a second model was formulated in which life satisfaction, sense of coherence, pain self-efficacy, kinesiophobia, catastrophizing, depressive and anxiety symptoms were included as covariates based on their associations with the study outcomes in prior research.6,7 Again, the covariates were dichotomised (Table 2) before the analysis. Thus, the model for psychological measures was fitted in the form:
Parameter estimates (95% confidence intervals) from multivariate linear mixed models with the following explanatory variables (one model per dependent variable) (i.e. average differences in outcome variables of knee pain and functioning between groups of categorical predictors).
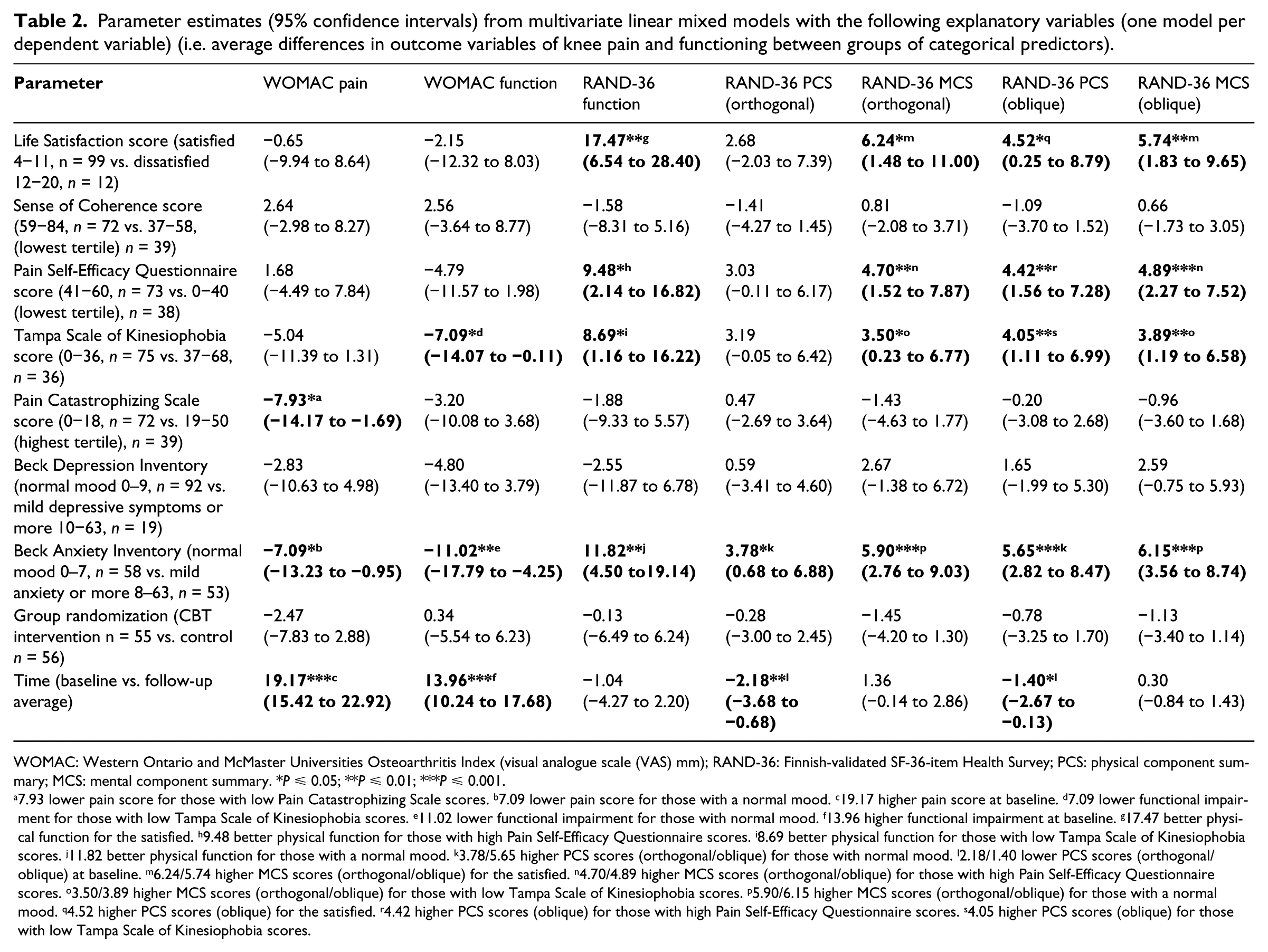
WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index (visual analogue scale (VAS) mm); RAND-36: Finnish-validated SF-36-item Health Survey; PCS: physical component summary; MCS: mental component summary. *P ⩽ 0.05; **P ⩽ 0.01; ***P ⩽ 0.001.
7.93 lower pain score for those with low Pain Catastrophizing Scale scores. b7.09 lower pain score for those with a normal mood. c19.17 higher pain score at baseline. d7.09 lower functional impairment for those with low Tampa Scale of Kinesiophobia scores. e11.02 lower functional impairment for those with normal mood. f13.96 higher functional impairment at baseline. g17.47 better physical function for the satisfied. h9.48 better physical function for those with high Pain Self-Efficacy Questionnaire scores. i8.69 better physical function for those with low Tampa Scale of Kinesiophobia scores. j11.82 better physical function for those with a normal mood. k3.78/5.65 higher PCS scores (orthogonal/oblique) for those with normal mood. l2.18/1.40 lower PCS scores (orthogonal/oblique) at baseline. m6.24/5.74 higher MCS scores (orthogonal/oblique) for the satisfied. n4.70/4.89 higher MCS scores (orthogonal/oblique) for those with high Pain Self-Efficacy Questionnaire scores. o3.50/3.89 higher MCS scores (orthogonal/oblique) for those with low Tampa Scale of Kinesiophobia scores. p5.90/6.15 higher MCS scores (orthogonal/oblique) for those with a normal mood. q4.52 higher PCS scores (oblique) for the satisfied. r4.42 higher PCS scores (oblique) for those with high Pain Self-Efficacy Questionnaire scores. s4.05 higher PCS scores (oblique) for those with low Tampa Scale of Kinesiophobia scores.
Outcome0;3;12 = Life Satisfaction + Sense of Coherence + Pain Self-Efficacy Questionnaire + Tampa Scale of Kinesiophobia + Pain Catastrophizing Scale + Beck Depression Inventory + Beck Anxiety Inventory+ time+ randomization + time x randomization.
The time-by-treatment interaction in both models addresses the question of whether the groups differed in the change between the measurement points. A non-significant time-by-treatment interaction suggests that the changes over the follow-up period cannot be distinguished from sampling error. Since the time-by-treatment interaction was non-significant in all outcomes, we decided to remove the term from both of the models. As group randomization did not show any significance as a covariate in either of the models, one can conclude that the intervention of the original randomized controlled trial did not have any effect on the outcome variables. Thus, the term could also have been removed from the mixed model analysis. However, we decided to keep it for reasons of clarity.
Results
The baseline characteristics of the study patients are presented in Table 3. The associations of baseline variables (predictors) with the outcome variables have been described in Tables 1 and 2.
Baseline characteristics (means or %) of the 111 patients (SD or n).
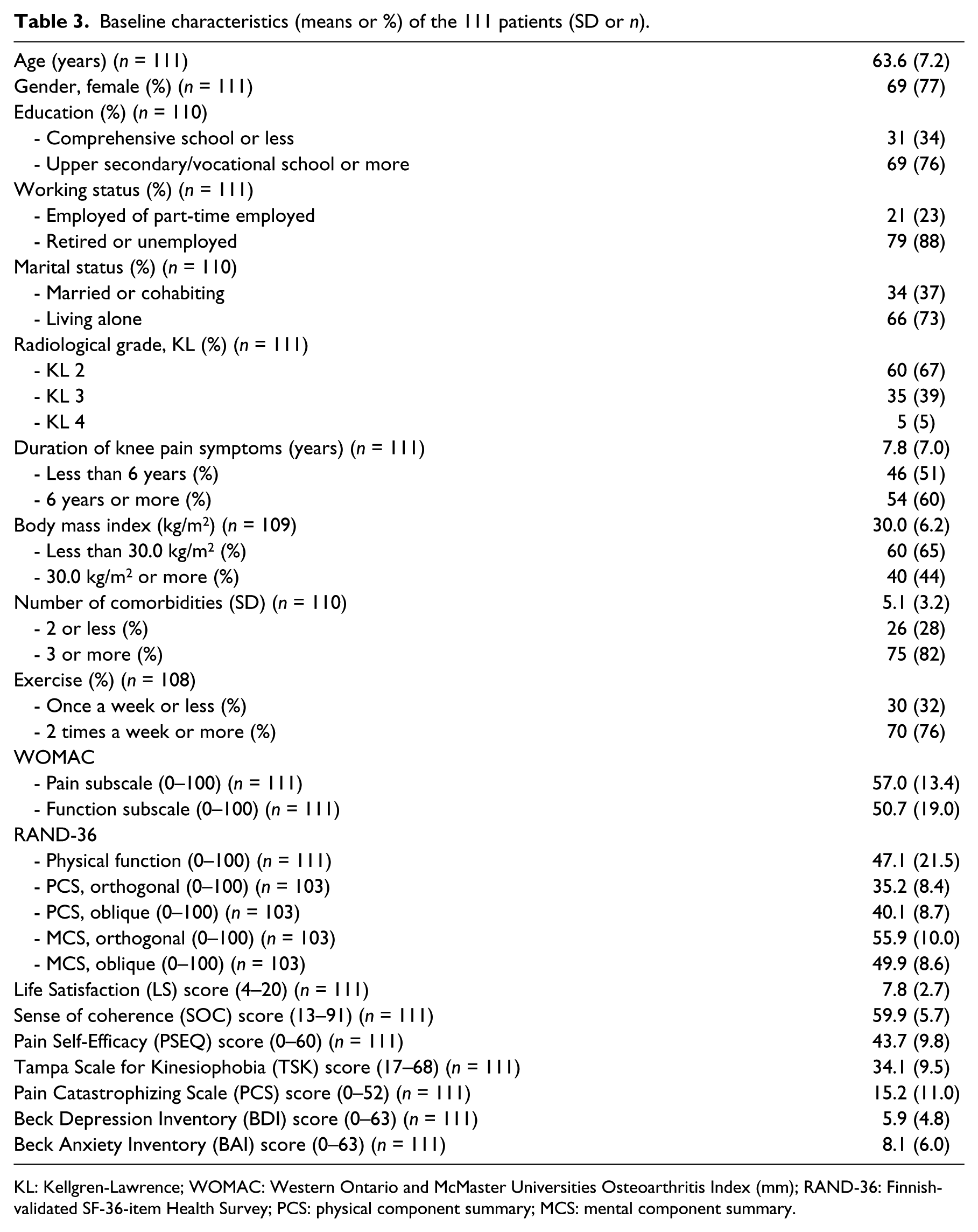
KL: Kellgren-Lawrence; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index (mm); RAND-36: Finnish-validated SF-36-item Health Survey; PCS: physical component summary; MCS: mental component summary.
Multivariate linear mixed model analyses revealed that normal mood at baseline measured with the Beck Anxiety Inventory predicted significantly better results in all of the outcome measures during the one-year follow-up. Strong pain self-efficacy and satisfaction with life predicted significantly better scores in RAND-36 function, mental and physical component summaries. High scores in the Pain Catastrophizing Scale predicted significantly higher WOMAC pain levels. Low kinesiophobia scores, on the other hand, predicted significantly lower impairment in WOMAC function and better scores in RAND-36 function, mental and physical component summaries.
Those with fewer comorbidities reported lower WOMAC pain levels and higher scores in the RAND-36 physical component summary. A lower radiological grade predicted better results in RAND-36 function, mental and physical component summaries. Those exercising more achieved better RAND-36 function scores, while those with a lower body mass index had better physical component summary scores.
Discussion
The current analysis revealed the significance of anxiety symptoms as predictors of knee osteoarthritis pain and function: Mixed model analysis showed that normal mood in the Beck Anxiety Inventory at baseline predicted better results in all outcomes of pain and function during the one-year follow-up. Moreover, the predictive role of baseline psychological resource factors for measures of function was highlighted in the follow-up of these patients. Additionally, negatively charged emotions and expectations towards pain were found to be important predictive factors in knee osteoarthritis symptoms.
The role of anxiety symptoms in predicting knee osteoarthritis pain and functional impairment has been well established.8,9 Generally, anxiety disorders among primary care patients with chronic pain have been found common, and the number of disorders adversely associated with impairment in health related quality of life and RAND-36 mental component summary scores. 32 Among other affective variables, depressive symptoms have been demonstrated to have an association with knee pain and activity limitations.8,9 However, in the current analysis, depressive symptoms did not have any predictive value for self-reported pain or function. One reason for this may be the low baseline levels of depressive symptoms among the study patients, with only 19 reporting at least mild depression. This, in turn, may result from the recruitment process of the original randomized controlled trial: The candidates had to take the initiative to participate in the study. In addition, severe psychiatric conditions were criteria for exclusion.
The importance of psychological resource factors was emphasized in relation to measures of function of knee osteoarthritis patients. Pain self-efficacy and satisfaction with life both predicted better generic measures of function (RAND-36 function, mental and physical component summaries) in the follow-up. According to previous research findings, strong pain self-efficacy appears to enhance and maintain the long-term effects of rehabilitation, 33 while weak pain self-efficacy has, in contrast, been found predictive of long-term disability and depression. 34 Satisfaction with life, on the other hand, has been found to be a powerful predictor of various health risks and health-related adversities among persons with musculoskeletal disorders, such as the length of sick-leave 35 and poorer postoperative recovery. 36
Negatively charged expectations toward pain and function, that is, kinesiophobia and catastrophizing, were also important predictors of knee osteoarthritis symptoms. A low tendency for pain catastrophizing predicted less pain (WOMAC), while low scores in the Tampa Scale of Kinesiophobia predicted better generic (RAND-36 function, mental and physical summaries) and disease-specific (WOMAC) function. Findings from previous research have also supported the importance of pain catastrophizing in predicting pain and explaining disability and psychological distress in knee osteoarthritis patients.10,37 Moreover, kinesiophobia has been reported to influence function in osteoarthritis patients. 38
Among the factors associated with a healthy lifestyle, we found that a lower body mass index predicted a better physical component summary score (RAND-36). Earlier findings by Edwards et al. 3 demonstrated an association between a higher body mass index and lower objectively measured physical performance. Furthermore, the benefits of exercise training in reducing pain and improving function have been well established in knee osteoarthritis patients. 39 In the current study, those exercising more frequently had significantly better RAND-36 function scores.
In our analysis, the number of comorbidities was found to predict both pain (WOMAC) and generic function (RAND-36 physical component summary). Earlier studies 31 have reported similar findings. Among the disease-related variables, the radiographic severity of knee osteoarthritis had predictive value for generic measures of function (RAND-36 function, mental and physical summaries). However, findings from previous studies have been somewhat contradictory on this matter. 5 Additionally, baseline values for WOMAC pain and function and RAND-36 physical component summaries were significantly better than follow-up average values, a phenomenon demonstrated in several previous studies among osteoarthritis patients. 40
The strengths of the present study include the repeated examination of a number of pain, function and psychological outcomes and the use of X-ray with at least Kellgren-Lawrence 2 13 scale knee osteoarthritis to confirm the diagnosis of knee osteoarthritis. Furthermore, the study sample can be considered representative of ordinary community-dwelling knee osteoarthritis patients, as most of the participants (77%, n = 86) were enrolled in the study as a result of a previous referral to a knee X-ray by their general practitioners. On the other hand, a central limitation of this analysis could be the fact that the study patients were too tightly selected due to the inclusion criteria of the original randomized controlled trial. Firstly, the patients had to have quite a high WOMAC pain subscale level (VAS ⩾40/100 mm) to be included. Almost half of the study candidates (47%, n = 209) had to be excluded because their WOMAC pain level was too low. 14 Secondly, the recruitment process may have resulted in the selection of patients who were more active and better off in some aspects of psychological well-being than the average knee osteoarthritis patient.
The current analysis added to the limited number of prospective studies concerning the impact of psychological factors on pain and function in knee osteoarthritis patients. To our knowledge, the results provided some new information on the predictive role of pain catastrophizing, kinesiophobia and life satisfaction in self-reported pain and function in this particular patient group. Moreover, the finding that the radiographic severity of knee osteoarthritis had predictive value for generic measures of function was interesting. In general, the results call for the routine assessment of multiple psychological factors in knee osteoarthritis to identify those patients or sub-groups of patients who need additional behavioural and psychological attention.10,41 Not taking these factors into considerations will probably contribute to prolonged disability and further pain.
Clinical messages
Among knee osteoarthritis patients, the absence of anxiety symptoms at baseline was a strong predictor of milder pain and better function during the follow-up.
Life satisfaction and pain self-efficacy predicted better function among knee osteoarthritis patients.
A low level of pain catastrophizing and kinesiophobia predicted milder symptoms of knee osteoarthritis.
Footnotes
Acknowledgements
We thank the physicians who helped with patient recruitment at Kuopio Health Centre and Kuopio University Hospital, data manager Pauli Kuosmanen of Kuopio Health Centre for technical support, statistician Tuomas Selander of Kuopio University Hospital for advice in statistical matters, and Professor Olli-Pekka Ryynänen of Kuopio University Hospital Primary Health Care Unit for creating the code for randomization. Finally, we thank the study patients for making this trial possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Research Ethics Committee of the Hospital District of Northern Savo approved the protocol (reference number 14/2011). Written informed consent was obtained from all patients.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has been supported by an EVO and a VTR grant from Kuopio University Hospital and a grant from the North Savo Regional Fund of the Finnish Cultural Foundation.