
Abstract
Objective:
To evaluate if the Timed Up and Go Test is a useful tool to measure postoperative function and to predict one-year results of rehabilitation in patients operated owing to hip fracture.
Design:
Prospective cohort study.
Setting:
The department of orthopaedic surgery at five hospitals in Norway. Patients were assessed five days postoperatively and after one year.
Subjects:
A total of 684 patients over 60 years with trochanteric or subtrochanteric hip fractures were included. A total of 171 (25%) patients died within a year and 373 (73% of patients still alive) attended follow-up one year after surgery.
Main measures:
Timed Up and Go Test and walking ability.
Results:
A total of 258 (38%) patients passed the postoperative Timed Up and Go Test. A total of 217 (56%) patients with a prefracture independent outdoor walking ability, passed the test. The average Timed Up and Go Test score was 71 seconds. A total of 171 (25%) patients could not rise from a chair without assistance; 8% of the patients with cognitive impairment, and 8% of those admitted from nursing homes, were able to pass the postoperative Timed Up and Go Test. The sensitivity and specificity of the Timed Up and Go Test in predicting walking ability one year after the operation were low. At one year follow-up, 38% of the patients not able to perform the postoperative Timed Up and Go Test, passed the test. A total of 81 (21%) patients did not use any walking-aid, 17 of them did not pass the postoperative Timed Up and Go Test.
Conclusion:
The Timed Up and Go Test performed the fifth postoperative day was not a suitable tool to assess functional mobility for the majority of the patients with hip fractures in our study. Neither was the postoperative Timed Up and Go Test a suitable tool to predict the walking ability one year after the operation.
Introduction
The majority of patients with hip fractures are elderly and need postoperative rehabilitation. Many frail patients also need institutional care. One-year mortality has been reported up to 29%. 1 The most important predictive factors for one year survival and successful rehabilitation are a high level of prefracture physical function, high cognitive and nutritional status and no depression.2–5 These factors, and the patient`s clinical condition postoperatively, must be considered when planning rehabilitation. One of the most popular assessment tools for physical function of the elderly is the Timed Up and Go Test (TUG-test). The test is easy to perform and at a low cost. Initially the TUG-test was used to assess physical function and balance for elderly patients. 6 As a clinical assessment tool, the test has been helpful for measuring change in physical function in rehabilitation programmes for the elderly.7–9 It has also been used as a test to identify persons with increased risk of falling.10,11 The TUG-test has been widely used as an outcome measure in studies of patients with a variety of conditions, for instance Parkinson decease, 12 balance disorders, 13 vertebral fractures, 14 amputations 15 and hip fractures.16,17 Hoang- Kim et al. reported the TUG-test as the most commonly used outcome measure for physical function of patients with hip fracture in scientific studies. 18 Even so, the clinical value of the TUG-test in the early postoperative days for patients with hip fracture, is still poorly documented.
We have performed a prospective randomized controlled trial (RCT) of 684 patients older than 60 years with trochanteric and subtrochanteric fractures, comparing two different implants (a sliding hip screw or an intramedullary nail). 19 Pain and function (TUG-test) were the primary outcome measures. There was no difference between the two operation techniques regarding TUG-test scores. Based on this study, we evaluated the usefulness of a postoperative TUG-test in measuring postoperative functional mobility and predicting walking ability one year after the operation.
Methods
The data used in this study were collected as part of a RCT on patients with trochanteric and subtrochanteric fractures. 19 In the period 2008 to 2010, 684 patients were included from five different hospitals. Patients with pathologic fractures were excluded. A clinical examination and functional assessment was done by a physiotherapist on the fifth day postoperatively, three months and one year after surgery. In the present study, we focused on the results at five days and one year after surgery. In this study, no comparison between different surgical methods was made.
The study was approved by the Regional Committee for Medical and Health Research Ethics. Informed consent was obtained from all patients. If the patient was unable to give informed consent, this was, whenever possible, obtained by relatives. Otherwise, the attending physician would make the inclusion in the best interest of the patient.
The patients residential and cognitive status, ASA-class (comorbidities, as described by the American Society of Anaesthesiologists), 20 and prefracture walking ability were recorded at inclusion.
The TUG-test was used to assess functional mobility. The TUG-test measures the patient’s ability to stand up from a chair with armrests, walk 3 m, turn, walk back and sit down. Human assistance is not permitted. A walking-aid is allowed and the type of walking-aid is recorded. The time needed to perform this task is the TUG-test score. The patient had one trial and the test was considered as passed if the score was less than three minutes and 30 seconds. Reasons for not being able to perform the test were recorded.
Date of death was collected from Statistics Norway.
Descriptive statistics were used to obtain simple frequencies and to calculate percentages of patients within different subgroups of patients. The Pearson’s chi-squared test was used for comparison of categorical variables in independent groups. The one-way analysis of variance (ANOVA) test was used for the analysis of continuous variables. IBM SPSS statistics 21 was used for all analyses.
Results
A total of 38% of the included patients passed the postoperative TUG-test, among whom 9% died during the following year (Figure 1) The group of patients who were able to pass the postoperative TUG-test had a lower one-year mortality rate and loss to follow-up than patients unable to perform the task or not offered the test. They also more frequently passed the TUG-test one year after the operation. This tendency was even more evident for patients with a good score on the postoperative TUG-test (as seen later in Table 3).
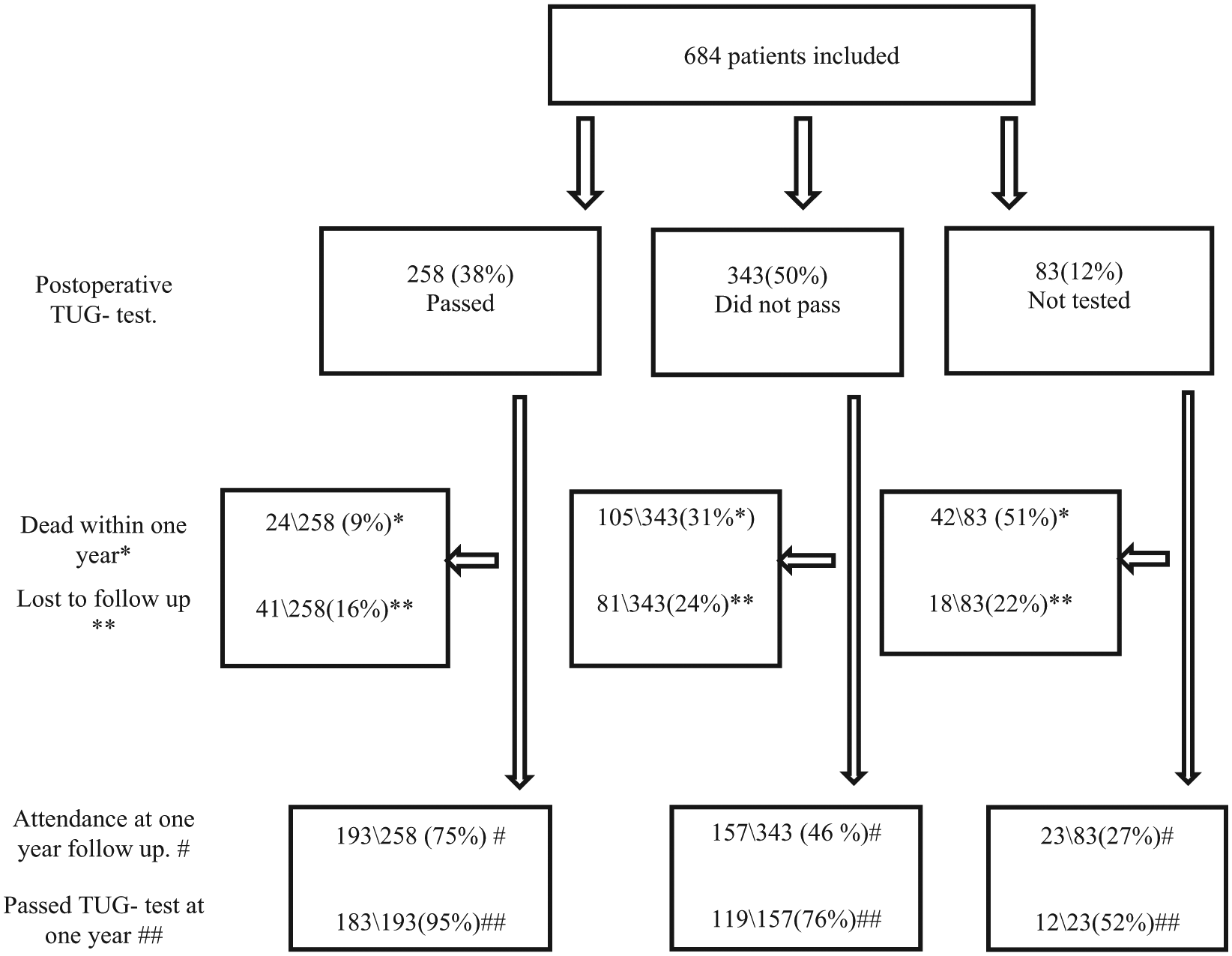
Flow chart of included patients. Patients passing the in-hospital TUG-test, one year mortality, attendance at one year follow-up and patients passing the one-year TUG-test.
The patient’s prefracture characteristics, one year mortality and attendance at one year follow-up are presented in Table 1. A total of 57% of the patients reported a prefracture independent outdoor walking ability. Mortality and loss to follow-up were highest for patients with cognitive impairment, those living in nursing homes and patients with a reported walking ability of only indoors.
Characteristics at inclusion for all patients, for patients that died the first year and for patients attending one year follow-up.
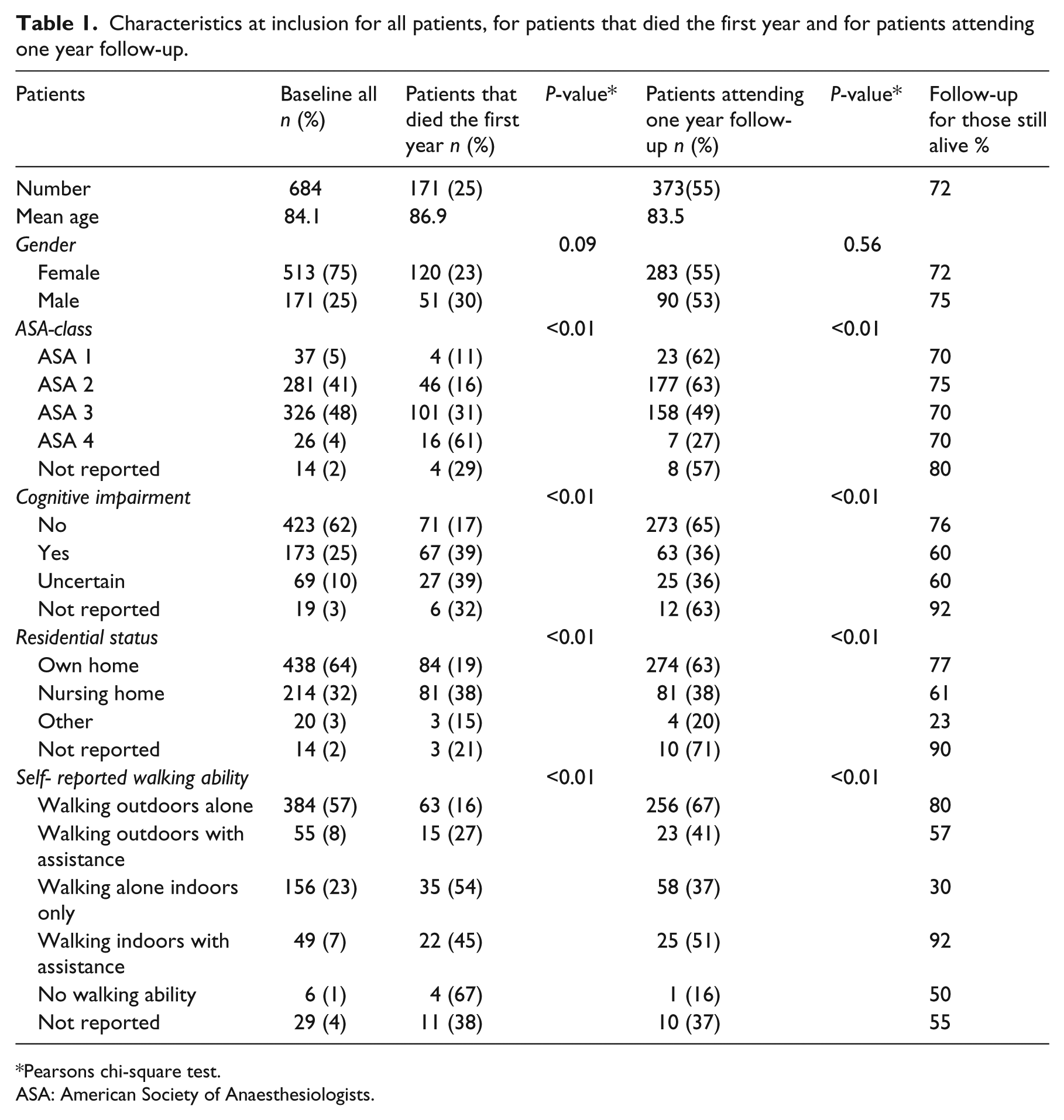
Pearsons chi-square test.
ASA: American Society of Anaesthesiologists.
There were significant differences in the patients’ ability to perform the TUG-test according to ASA class, cognitive and residential status, and their reported prefracture walking ability (Table 2). For the mean scores of the TUG-test, however, the differences were less apparent and the confidence intervals were large and overlapping (Table 2). Patients using the high support had a higher TUG-test score (mean 24 seconds slower) than patients using a roller or crutches. A total of 171 patients, not able to pass the test, could not rise from a chair without assistance.
TUG-test results (numbers passed) and TUG-test scores (seconds) according to prefracture characteristics.
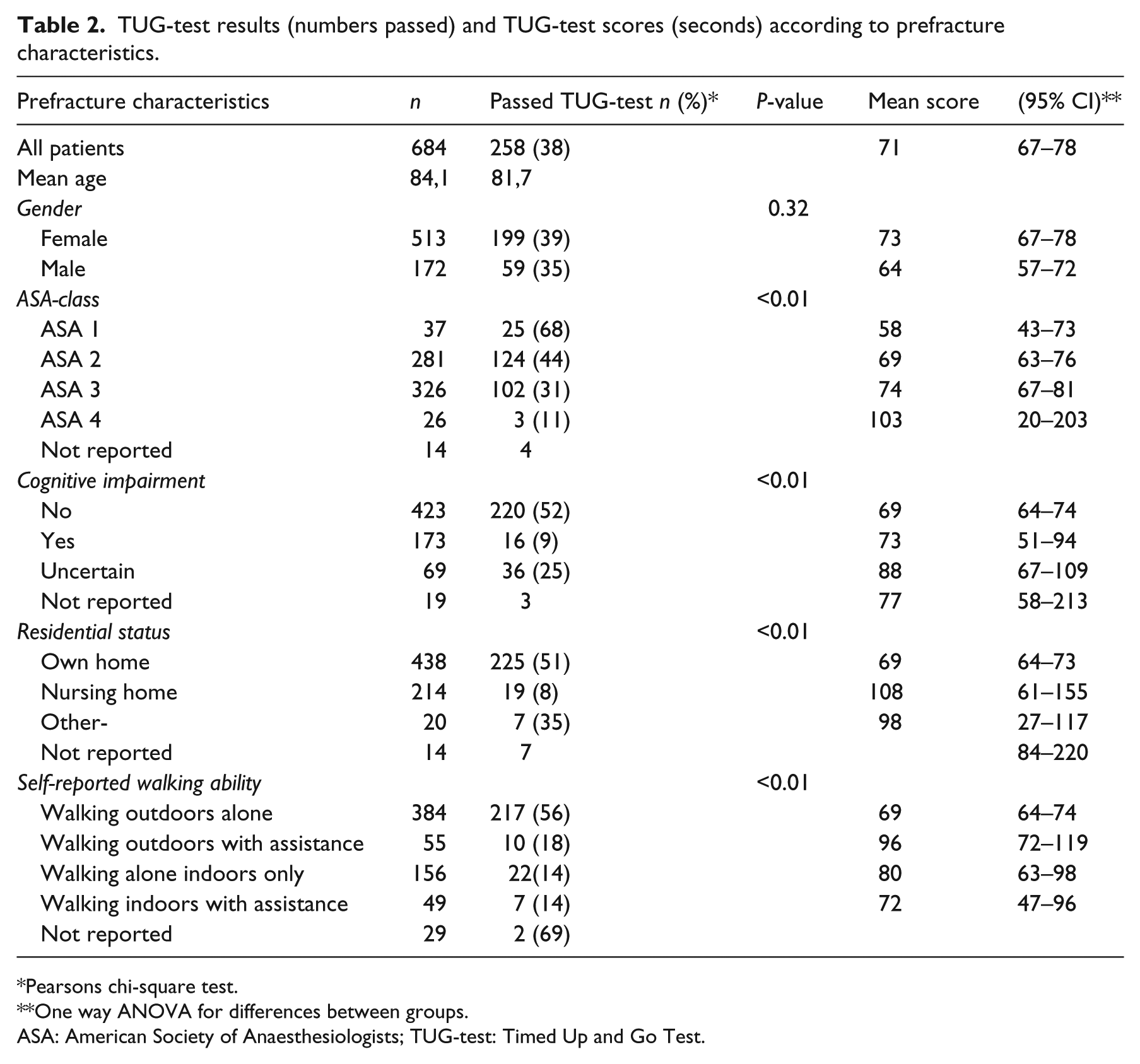
Pearsons chi-square test.
One way ANOVA for differences between groups.
ASA: American Society of Anaesthesiologists; TUG-test: Timed Up and Go Test.
A higher proportion of patients with a high performance at the postoperative TUG-test were living in their own home and had a better walking ability one year after surgery (Table 3). However, 59 patients at follow-up, unable to pass the inhospital TUG-test, regained their ability of outdoor independent walking and 75 were still living in their own homes. In addition, 17 of the 81 patients not using any walking-aid one year after the operation, were unable to perform the inhospital TUG-test. A total of 55 of the patients who attended one year follow-up moved from their own home to nursing homes, and 82 could no longer walk alone outdoors.
Mortality, follow-up, residence and walking ability one year after surgery according to postoperative TUG-test score.
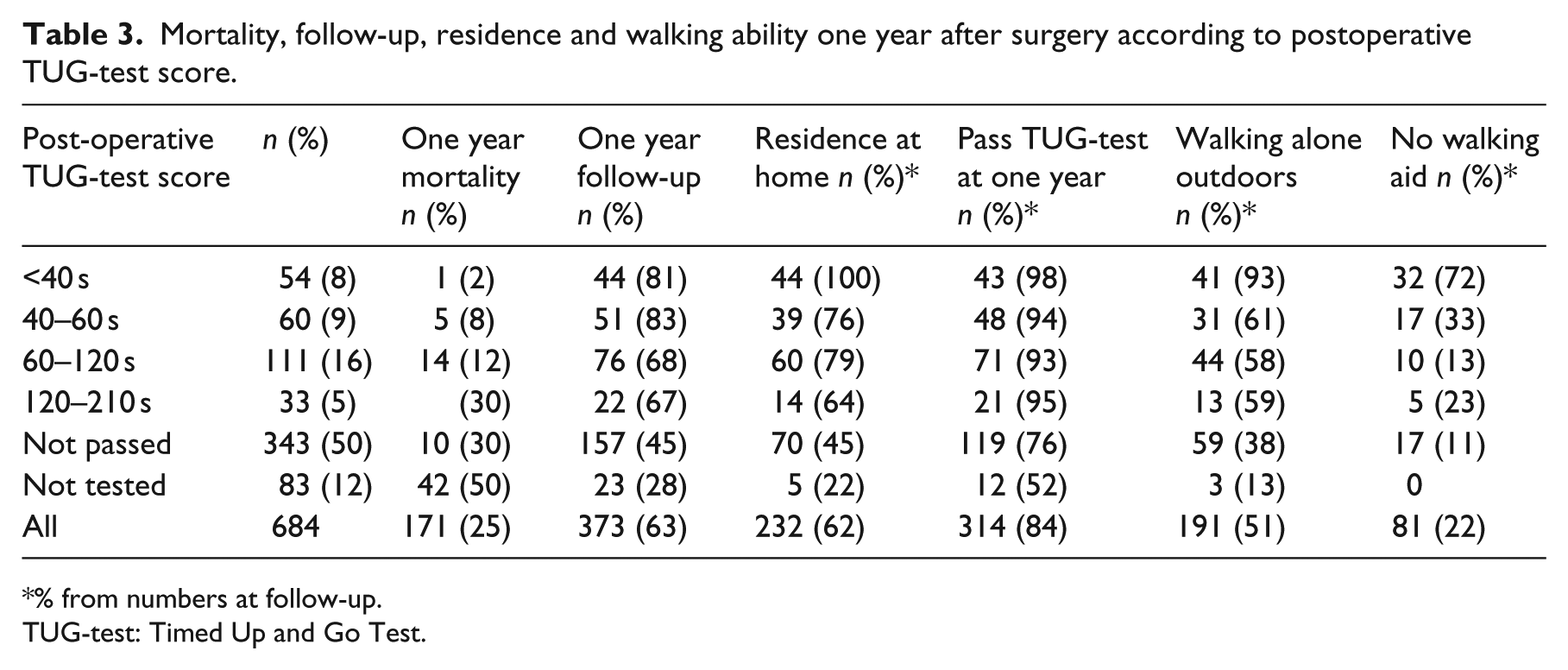
% from numbers at follow-up.
TUG-test: Timed Up and Go Test.
The sensitivity, specificity and overall prediction of the postoperative TUG-test for predicting one year walking ability one year after the operation is presented in Table 4.
Postoperative TUG-test for predicting one year walking ability.
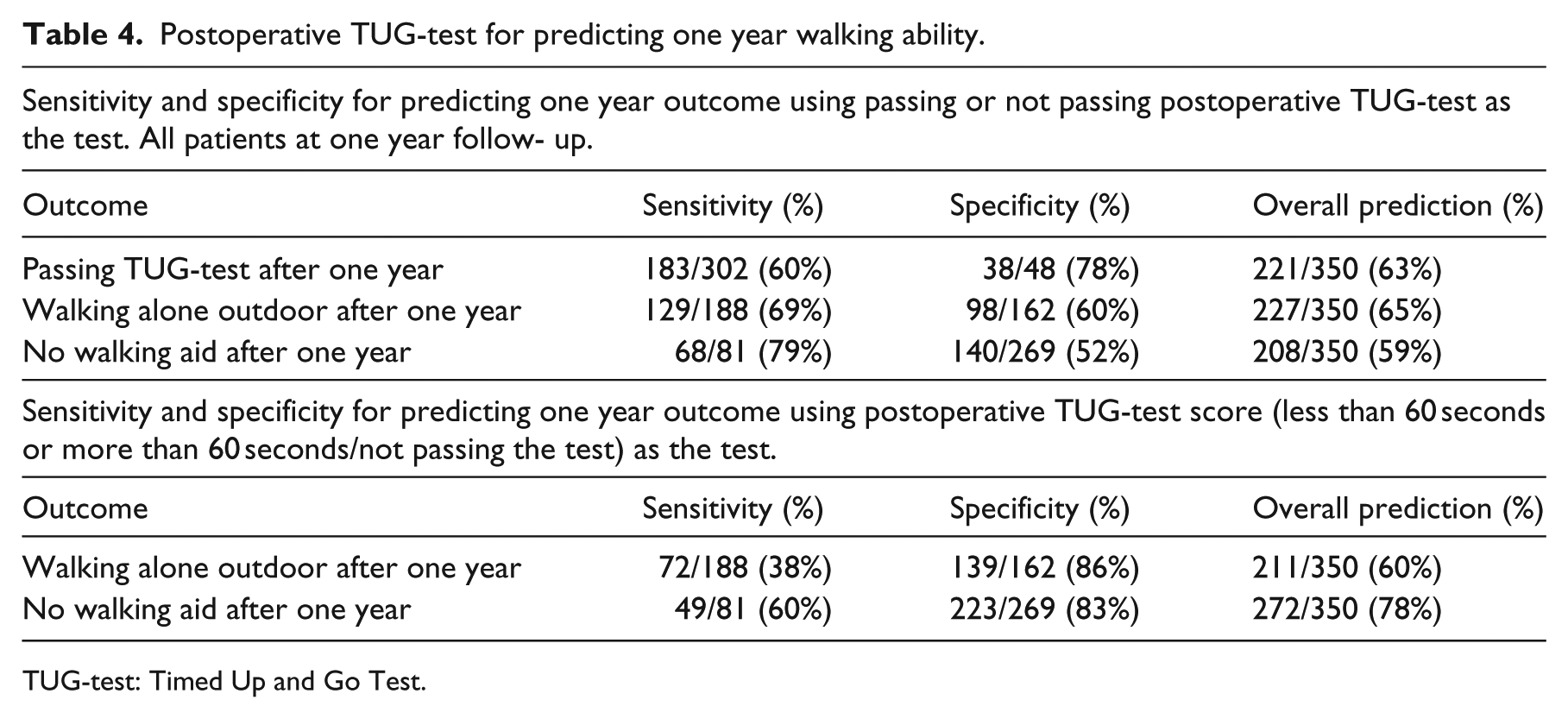
TUG-test: Timed Up and Go Test.
Discussion
The main finding of the present study was that an early postoperative TUG-test after a hip fracture was not a suited tool to assess physical function for the majority of the patients. Altogether no more than 38% of the patients and only a little more than half of the patients admitted from their own home, passed the postoperative TUG-test. Of the patients unable to pass the postoperative TUG-test and attending the one year follow-up, 38% regained an independent outdoor walking ability and 45% were still living in their own home. Based on our study, the sensitivity and specificity of the early postoperative TUG-test were not sufficiently high to predict future walking ability in patients with hip fractures. A TUG-test score lower than 60 seconds was associated with a better ambulatory and residential status one year after the fracture. This, however, applied only to 114 (17%) of all patients.
A limitation of this study was that only 55% of the included patients attended the one year follow-up. A total of 25% of the patients in our study were, however, died within one year after the fracture, and 73% of the survivors attended the follow-up. Patients attending the one year follow-up had a higher prefracture physical and cognitive function and better residential status compared with the drop-outs. Even within this somewhat selected group of patients, physical function declined. One year after their fracture, one-fourth of the follow- up attenders had moved to nursing homes and one-third had lost their ability to walk alone outdoors.
A small number of patients in the study were not asked to perform the postoperative TUG-test, some for medical reasons and some for practical reasons. Of these patients, 50% died within the first year.
The postoperative TUG-test was performed the fifth postoperative day whenever possible. If this was not possible, some patients were tested the fourth day and some a few days later. This also might have influenced the results.
The use of walking- aids was not standardized in our study. Kristensen et al. 21 found TUG-test scores for patients with hip fracture to be dependent on the type of walking-aid used. In our study, nearly 60% of the patients used the high support on wheels at the postoperative testing. There is a possibility that even fewer patients would have passed the test at this stage if we had used a roller (which is less supportive) as a standard walking-aid, as suggested by Kristensen et al. 21 The lack of standardization regarding the time after the operation of performing the TUG-test, and the different walking-aids used, represent weaknesses of this study. The need for walking support will, during rehabilitation after hip fracture, normally change over time. Some of these patients will need a permanent walking-aid, this might be a high support, a roller, crutches or a stick. This further complicates the comparison of TUG-test scores for hip-fracture patients in rehabilitation.
In contrast to other studies5,22 we included persons admitted from nursing homes (32%), patients with cognitive impairment (25%) and patients unable to walk independently outdoors (43%). According to Kristensen’s study of factors influencing the TUG-test scores, 23 these factors would negatively influence the TUG-test results. It is hardly surprising that the TUG-test was particularly ill suited for these frail patients. Inclusion of these patients partly explains the overall poor inhospital TUG-test results in the present study.
This assumption is supported by our own analyses. Prefracture characteristics, such as ASA class or cognitive status, were important in determining whether the patients were able to pass the TUG-test or not. However, for patients who did pass the TUG-test, the early test scores did not seem to be related to the prefracture characteristics. The variation in TUG-test score was quite wide, and there was a major overlap between the ranges in TUG-score between different subgroups (e.g. different ASA subgroups, Table 2).
For patients admitted from their own home, the results at the postoperative TUG-test was poorer in our study compared with a similar study from Hvidovre. In that study, 61% of the patients were able to perform the TUG-test the day before discharge from hospital (6–19 days postoperatively). 23 This is probably the main reason for the better results in their study. Our results were based on an examination the fifth postoperative day. Probably for the same reason, patients in our study that did pass, also had a mean TUG-test score 30 seconds higher. Siu et al. 24 found that the average day of mobilization beyond a chair was 5.2 days after surgery. In our study, 50% of the patients not passing the TUG-test, were not able to rise from a chair without assistance. Kristensen et al. 23 also found the TUG-scores were influenced by the type of fracture. Patients with femoral neck fractures had better results than patients with trochanteric or subtrochanteric fractures. All patients in our study had trochanteric or subtrochanteric fractures, and this possibly also contributed to the low number of patients able to perform the TUG-test, and the poorer scores for those who passed the test.
Prefracture patient characteristics were important variables for predicting the one-year outcome. Patients with high age, patients living in nursing homes, patients being cognitive impaired and those with a poor prefracture physical function had a higher percentage both of mortality as well as loss to follow-up. These factors for increased one-year mortality was in accordance with other studies.1,3–5,24
In a recent study of 56 patients with hip fracture, Laflamme tested the TUG-test’s predictive value for future ambulation. 22 Patients with a score below 58 seconds a few days postoperatively, had nine times higher probability of returning to their prefracture level of walking without a walking-aid. This is also supported by our study. A total of 52% of the patients at one year follow-up, with a postoperative score less than 60 seconds (17% of all patients) used no walking-aid one year after surgery and almost all the patients with a score less than 40 seconds (8% of all patients) used no walking aid. The TUG-test’s prediction of high future function were high for patients with a score better than 60 seconds. However, one-third of the patients at follow-up, unable to pass the postoperative test, also achieved the ability of independent outdoor walking. A total of 17 (20%) of the patients that used no walking-aid one year after surgery did not pass the postoperative test.
Owing to the low number of patients able to perform the TUG-test at this early stage, and the low correspondence with previous walking ability, the TUG-test should not be used for assigning patients to different levels of rehabilitation, as it may deprive patients who have the ability to regain physical function from high level rehabilitation.
In a recent article, Hoang- Kim et al. 25 advocated standardized measurements of physical function for RCT studies. Physical performance tests are not recommended for patients with hip fracture because of the frailty and comorbidities of these patients. As only 38% of all included patients in our study passed the inhospital TUG-test, we have come to the same conclusion. In future research on patients with hip fracture, these limitations of the TUG-test should be considered.
Clinical messages
The early postoperative TUG-test for patients with hip fracture:
is not suited to assess physical function for all patients;
should not be used to assign patients to different levels of rehabilitation – passing the early TUG-test has low specificity of predicting long-term physical function for all patients;
predicts high physical function for patients with scores below 60 seconds.
Footnotes
Acknowledgements
We want to thank Rolf-Moe-Nilssen for his contribution in the early stage of this study. His great knowledge of the TUG-test was important. We also want to appreciate all the contributors in the primary study for their efforts in collecting the data. We also want to thank the leader of the Physiotherapy Department, Else Sterndorff for allowing time to perform the study and the writing.
Conflict of interest
The authors declare that there is no conflict of interest.
Contributors
HN initiated this study, performed the analysing and wrote most of the article. KM was the leader of the original study, has been a mentor and a discussion partner in the whole process: from selection of data to analyses and presentation. He also was an active partner in the writing process. JMF also took a part in the original study. His contribution towards selection, analyses and presentation of data has been great. He also took part in the writing process.
Funding
The primary RCT study (TRIGEN INTERTAN intramedullary nail versus sliding hip screw: A prospective, randomized multicentre study on pain, function, and complications in 684 patients with trochanteric and subtrochanteric fractures with 1 year follow up) was supported by Smith & Nephew, but otherwise the company had no influence on the study protocol, the performance of the study, data analysis or presentation of the results. The leader of this RCT study, Kjell Matre, received a research grant from the Regional Health Board of Western Norway.
The present study was supported by The Norwegian Fund for Postgraduate Training in Physiotherapy.