
Abstract
Objective:
To examine the validity and sensitivity to change of the Multiple Sclerosis-Fatigue Self-Efficacy scale.
Design:
A validation study nested within a randomized controlled trial.
Setting:
Community setting.
Participants:
Adults with a clinically definite diagnosis of multiple sclerosis and significant fatigue taking part in a randomized controlled trial evaluating a group-based fatigue management programme (FACETS) for people with multiple sclerosis (N=164).
Main measures:
The 9-item Multiple Sclerosis-Fatigue Self-Efficacy scale was completed at baseline, 1-, 4- and 12 months post intervention. Validity, internal consistency and sensitivity to change were examined using classical test theory and Rasch analysis.
Results:
Item 3 was unanswered by 6% of respondents as they did not know any other people with multiple sclerosis; remaining analyses were carried out with this item deleted. All response choices were utilised, no floor or ceiling effects were evident and there were few missing responses. Cronbach’s alphas were high (baseline, 0.89; follow-up 1, 0.93; follow-up 2, 0.94; follow-up 3, 0.90). The Multiple Sclerosis-Fatigue Self-Efficacy scale (8-item) demonstrated good sensitivity to change following attendance of the FACETS programme (within participant effect sizes 0.66 and 0.69 and 0.54 at 1, 4, and 12 months follow-up). Principal Components Analysis yielded one component. In the Rasch analysis two items with disordered thresholds were rescored. Item 8 displayed differential item functioning by disability and was combined into a testlet with item 4, resulting in a unidimensional scale. The sample was well targeted to the scale.
Conclusion:
At a scale level the Multiple Sclerosis-Fatigue Self-Efficacy scale is internally valid and has good sensitivity to change.
Introduction
Fatigue is one of the most commonly reported symptoms of multiple sclerosis. 1 It has a profound impact on all spheres of life,2, 3 both for the person with multiple sclerosis and their relatives, 4 and is one of the key precipitants of early retirement.5, 6 Self-efficacy, the “belief in one’s capabilities to organise and execute the course of action required to produce given attainments” 7 has been identified as a strong predictor of health status in multiple sclerosis. 8 It is also associated with health promoting behaviours such as physical activity. 9 Studies have shown that a higher sense of self-control predicts lower fatigue severity and chronicity, 10 suggesting that increasing self-efficacy related to fatigue could improve quality of life. Thus, self-efficacy is an important domain to measure and manage actively in education, rehabilitation and health promotion programmes. 8
A group-based fatigue management programme for people with multiple sclerosis, partly based on self-efficacy theory, has recently been evaluated in a randomized controlled trial.11–13 We wanted to test whether the intervention did improve self-efficacy. However, existing generic self-efficacy scales14, 15 and multiple sclerosis specific self-efficacy scales16–20 do not have a focus on fatigue and thus may not be specific enough to measure change in this variable in a multiple sclerosis population.
Fatigue self-efficacy scales have been developed for other conditions. For example, in a study considering the effectiveness of a multi-component programme for chronic fatigue syndrome, Goudsmit et al. (2009) 21 modified Lorig’s 6-item Self-Efficacy ‘Other Symptoms’ subscale. 22 Similarly, in the cancer field, the Perceived Self-Efficacy for Fatigue Self-Management scale has been developed. 23 This scale was also adapted from Lorig’s 6-item scale by modifying items to focus on fatigue. 24 While the preliminary psychometric findings from this study suggest the Perceived Self-Efficacy for Fatigue Self-Management scale is a promising tool, it has not been validated in people with multiple sclerosis and does not include items related to several domains likely to be of relevance to people with multiple sclerosis fatigue, such as unpredictability and interference with everyday life.
For our study 12 we adapted the 9-item Control subscale of Schwartz’s Multiple Sclerosis Self- Efficacy 25 scale to form a new Multiple Sclerosis-Fatigue Self-Efficacy scale. The aim of this paper is to report on the scale’s development and validation.
Methods
The Multiple Sclerosis-Fatigue Self-Efficacy scale was developed by altering the wording of 6 of the 9 original Multiple Sclerosis Self-Efficacy scale items to make them fatigue-specific (supplementary material online Appendix). For items 2, 5 and 6 this entailed replacing ‘multiple sclerosis’ with ‘fatigue’ and for items 3, 4 and 9 replacing ‘multiple sclerosis symptoms’ with ‘fatigue’. Items 1, 7, and 8 were not modified. We retained the original response format of the Multiple Sclerosis Self- Efficacy scale, which consists of a 10-point numeric rating scale (ranging from 10-100) with verbal anchors of ‘very uncertain’ (10) and ‘very certain’ (100) and the descriptor ‘moderately uncertain’, at the midpoint (spanning 50 and 60). A summary score is produced by taking the mean of the 9 items. The Multiple Sclerosis-Fatigue Self-Efficacy scale was administered as part of a questionnaire battery presented in a booklet with a 14pt. font size.
Participants
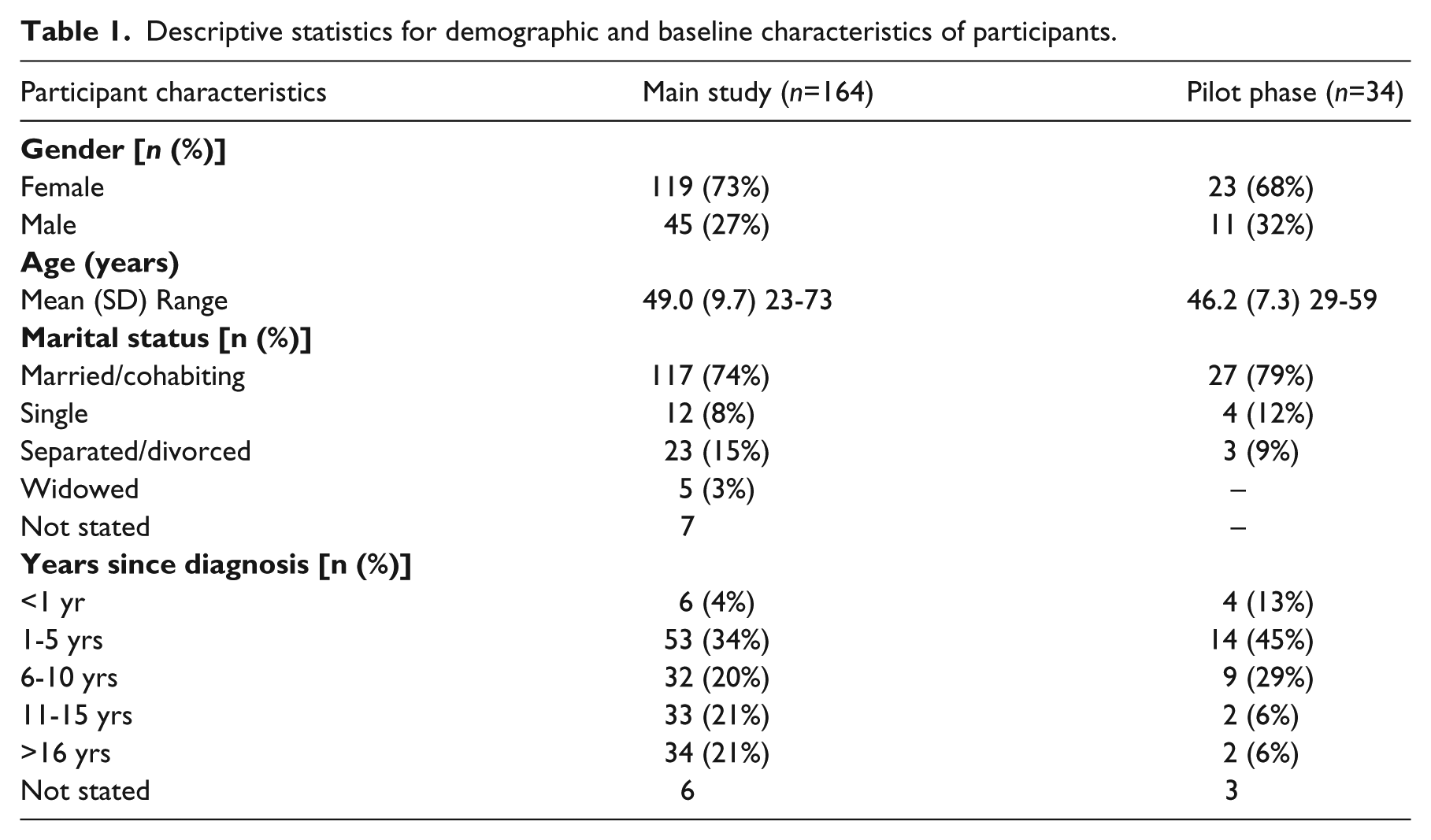
Data from 164 participants who participated in a randomized controlled trial of a group-based fatigue management programme (FACETS)11, 12, 26 were used to explore the validity of the Multiple Sclerosis-Fatigue Self-Efficacy scale. In addition, data from 34 participants who participated in pilot phases of the research were used to consider convergent validity. In the full trial, outcomes were measured 1 week before the start of the 6-week FACETS programme and 1-, 4-and 12 months after its conclusion. Participants assigned to the Usual Care arm completed all outcome measures within an identical time frame to those in the FACETS arm. For a detailed description of participants, recruitment methods, and outcome measures please refer to the published trial protocol and papers.11, 12
Inclusion criteria were: (1) clinically definite diagnosis of multiple sclerosis, (2) reporting significant fatigue impacting on daily life (score on the Fatigue Severity Scale > 4) 27 and (3) ambulatory (score on the Adapted Patient Determined Disease Steps scale <8). 28 Participants were excluded if they: (1) were non-English speaking, (2) had had a relapse requiring corticosteroids within the past 3 months, (3) had started a disease modifying drug or anti-depressant within the past 3 months, (4) were judged by the clinical team to have cognitive deficits such that they could not engage in the group format, (5) had attended a specific fatigue management programme within the past year or had received a specific fatigue intervention from a health professional within the previous 3 months, (6) were currently under the care of a psychiatrist or under the care of addiction services, or (7) were already involved in another research study. Participants were recruited in three UK centres (Poole, Bristol, Southampton/Portsmouth) from primary or secondary care, or via the UK Multiple Sclerosis Society website or newsletters.
Analysis
Data analysis included a consideration of score distributions and internal consistency (Cronbach’s Alpha and item-total correlations). 29 One would expect that scores on the Multiple Sclerosis-Fatigue Self-Efficacy scale would show high associations with scales measuring conceptually similar constructs (convergent validity) but relatively lower associations with those less closely related (discriminant validity). We examined this with data from our pilot phase in which we administered both the Multiple Sclerosis Self-Efficacy scale and the Multiple Sclerosis-Fatigue Self-Efficacy scale (n=34) and with data from our main study (n=164), using Spearman’s Rank correlation coefficients. The hypothesised strength and direction of associations were as follows:
- A strong positive correlation between the Multiple Sclerosis-Fatigue Self-Efficacy scale and the Multiple Sclerosis Self-Efficacy scale.
- A weak positive correlation between the Multiple Sclerosis-Fatigue Self-Efficacy scale and the SF-36 Pain subscale.
- A moderate negative correlation between the Multiple Sclerosis-Fatigue Self-Efficacy scale and the Global Fatigue Severity subscale of the Fatigue Assessment Instrument.
- A moderate positive correlation between the Multiple Sclerosis-Fatigue Self-Efficacy scale and the SF-36 Vitality subscale.
Sensitivity to change was assessed with Cohen’s effect size statistic (considered large if >0.5) 30 using the mean difference from baseline at each follow-up point (1-, 4- and 12 months) divided by the baseline standard deviation. This utilised data from the trial for those participants who attended 4 or more sessions of the six week group-based fatigue management programme (FACETS).
Principal Components Analysis 31 was used to explore dimensionality of the scale with parallel analysis 32 used to help to determine the number of components to retain.
The Multiple Sclerosis-Fatigue Self-Efficacy scale was tested against the polytomous partial credit Rasch model 33 to examine internal validity. Overall fit to the Rasch model was examined with an item-trait interaction Chi-square test, which should be non-significant. Individual person and item fit residuals should be within the range of -2.5 and 2.5. Person fit and item fit statistics are transformed to approximate a z-score; therefore, when the data fit the Rasch model, the overall distribution statistics for item fit and person fit should have a mean of approximately zero and standard deviation close to 1. 34 Log-transformed item scores generated from the items’ response choices should reflect an increase in the latent trait of self-efficacy to be measured. Thresholds are the points where the probabilities of a response of either 10 or 20, and 20 or 30 (and so forth) are equally likely and therefore threshold locations should be increasing along the trait. When a given level of fatigue self-efficacy is not confirmed by the expected response option to an item, disordered thresholds will be observed. In such cases item categories should be collapsed until they are ordered so that a more precise estimate of individuals’ fatigue self-efficacy can be obtained.
Differential item functioning35, 36 (or bias of the items) was examined with an Analysis of Variance with the following groups as the main factor: age, trial arm, educational attainment, time since diagnosis, marital status, current employment status and level of mobility. Response dependency was examined using a residual correlation of 0.30 below the mean residual as an acceptable cut off. 37
A key requirement of the Rasch model is that the scale is unidimensional. This is examined by creating two subsets of items, which are identified by a Principal Component Analysis of the item residuals, with those loading negatively forming one set and those loading positively forming the second set. 38 Strict unidimensionality is then examined using an independent t-test on the two estimates derived from the subtests for each respondent. If the 95% confidence interval of t-tests includes 5%, unidimensionality is supported. 38
The precision of the scale was examined with the Person Separation Index (similar to a Cronbach’s Alpha), which can range from 0 to 1. 34 Values ≥0.70 allow for group comparisons but for individual clinical use values should be ≥0.85. Testlets were created if problems with response dependency or differential item functioning were found, to test if bias is cancelled out at the test level and also to see if they removed the dependency in the data. 39 Bonferroni corrections were applied to judge the statistical significance of findings. If the scale fits the Rasch model ordinal data arising from the scale are converted onto an interval scale using Rasch analysis software (RUMM2030). 40
Analyses were carried out using SPSS Version 20 41 and RUMM2030. 40
Ethical approval was obtained from the South West-Central Bristol Research Ethics Committee (ref: 08/H0106/2). All participants gave written informed consent before taking part. The trial sponsor was Poole Hospital NHS Foundation Trust.
Results
Participant characteristics are displayed in Table 1.
Descriptive statistics for demographic and baseline characteristics of participants.
Response rate and item distributions
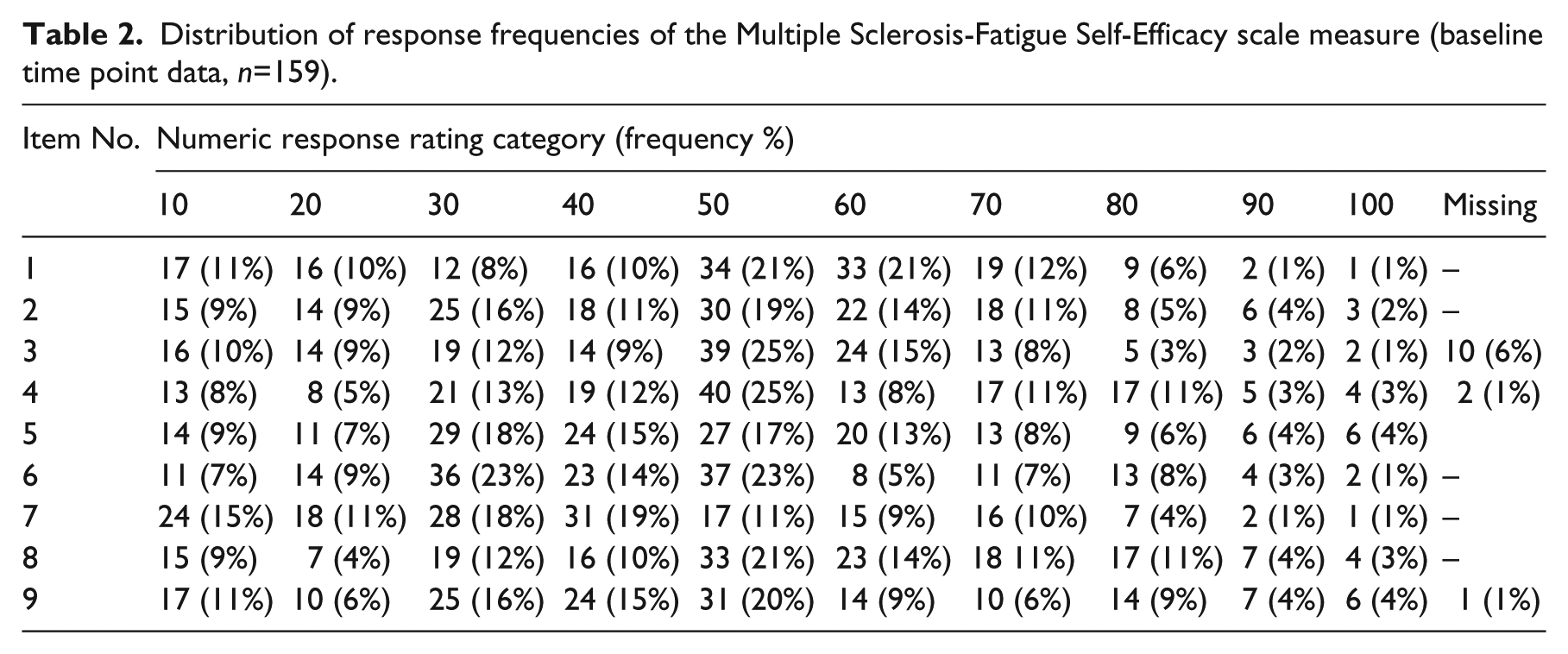
Baseline data on the Multiple Sclerosis-Fatigue Self-Efficacy scale were not available for five people. All response choices for the nine items were utilised and there was no evidence of floor or ceiling effects either at baseline (Table 2) or at subsequent follow-up points. Item 3 had somewhat more missing data, mostly due to respondents not being able to answer as they did not know any other people with multiple sclerosis (6.3%). For this reason the remaining analyses were carried out with item 3 deleted, i.e. testing the 8-item scale. The 8-item Multiple Sclerosis-Fatigue Self-Efficacy scale data followed a normal distribution pattern at baseline (n=159), 1st follow-up (n=146), 2nd follow-up (n=144) and 3rd follow-up (n=131).
Distribution of response frequencies of the Multiple Sclerosis-Fatigue Self-Efficacy scale measure (baseline time point data, n=159).
In terms of the FACETS trial data there were statistically significant differences on the 8-item Multiple Sclerosis-Fatigue Self-Efficacy scale favouring the FACETS arm over the Usual Care arm at 1 month (mean diff (MD) 9, 95% CI (3 to 14), standardised effect size (SES) 0.51, p=0.001). At 4 months follow-up, this difference approached significance (MD 6, 95% CI (0 to 12), SES 0.33, p = 0.07) (Table 3) and a similar SES was obtained at one year (MD 5, 95% CI (-1 to 12), SES 0.30, p = 0.13).
Descriptive statistics and treatment effects of the 8-item Multiple Sclerosis-Fatigue Self-Efficacy scale at each time point (main study)*.
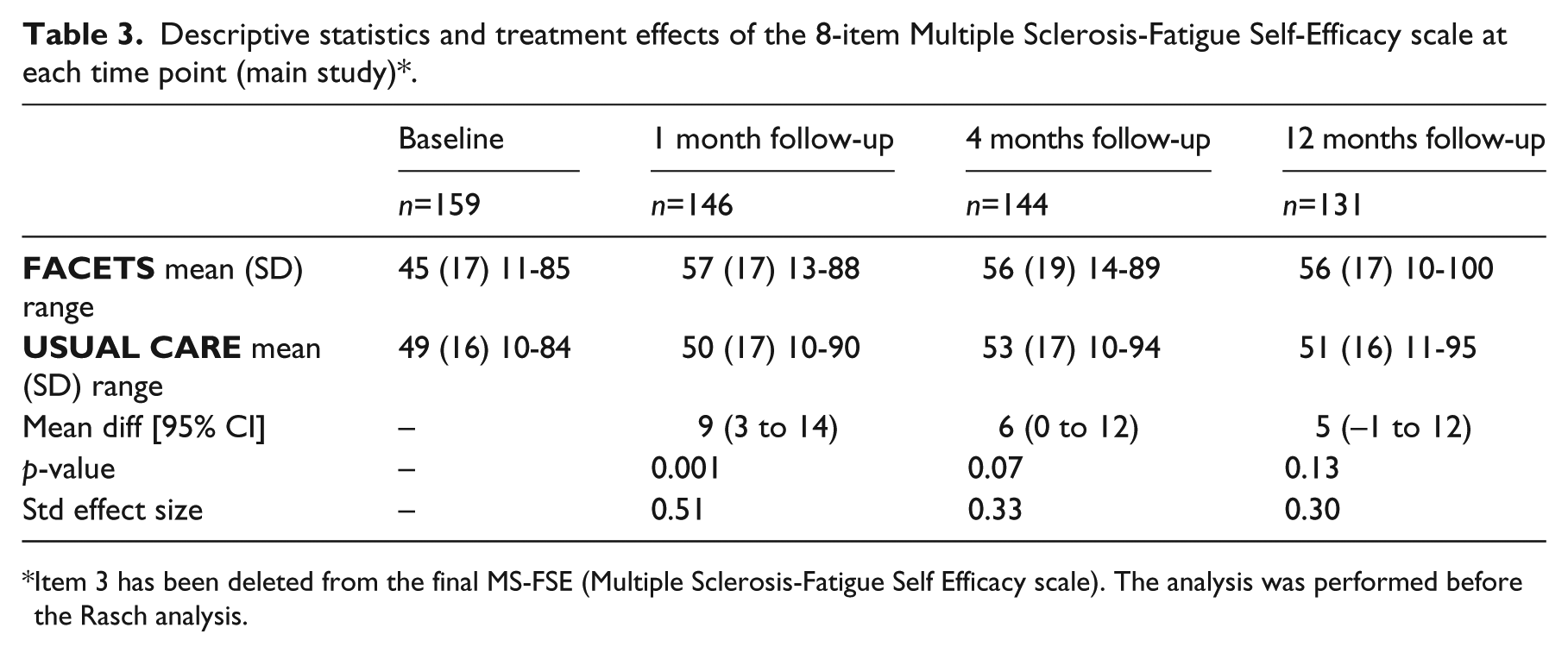
Item 3 has been deleted from the final MS-FSE (Multiple Sclerosis-Fatigue Self Efficacy scale). The analysis was performed before the Rasch analysis.
Sensitivity to change
For those in the FACETS group who attended 4 or more FACETS sessions the mean Multiple Sclerosis-Fatigue Self-Efficacy scale total score improved significantly from baseline to 1 month follow-up (t(63) = -5.44. p < 0.001, SES = 0.66), from baseline to 4 months follow-up (t(61) = −4.77, p < 0.001, SES = 0.69) and from baseline to one year follow-up (t(55) = −4.07, p < 0.001, SES = 0.54).
Multiple Sclerosis-Fatigue Self-Efficacy scale dimensionality
Principal Components Analysis revealed two eigenvalues greater than 1.0 and the break in the scree plot suggested two components should be retained. A parallel analysis, however, indicated that only one was statistically significant and should be retained: i.e. only the first eigenvalue from the actual data is larger than the mean and 95th percentile of the corresponding eigenvalue derived from the 1000 randomly generated datasets. Thus, this analysis suggests a one-factor solution explaining 56.7% of the variance (Table 4).
Factor loadings and total variance explained of the 8-item Multiple Sclerosis-Fatigue Self-Efficacy scale (baseline, n=159)*.
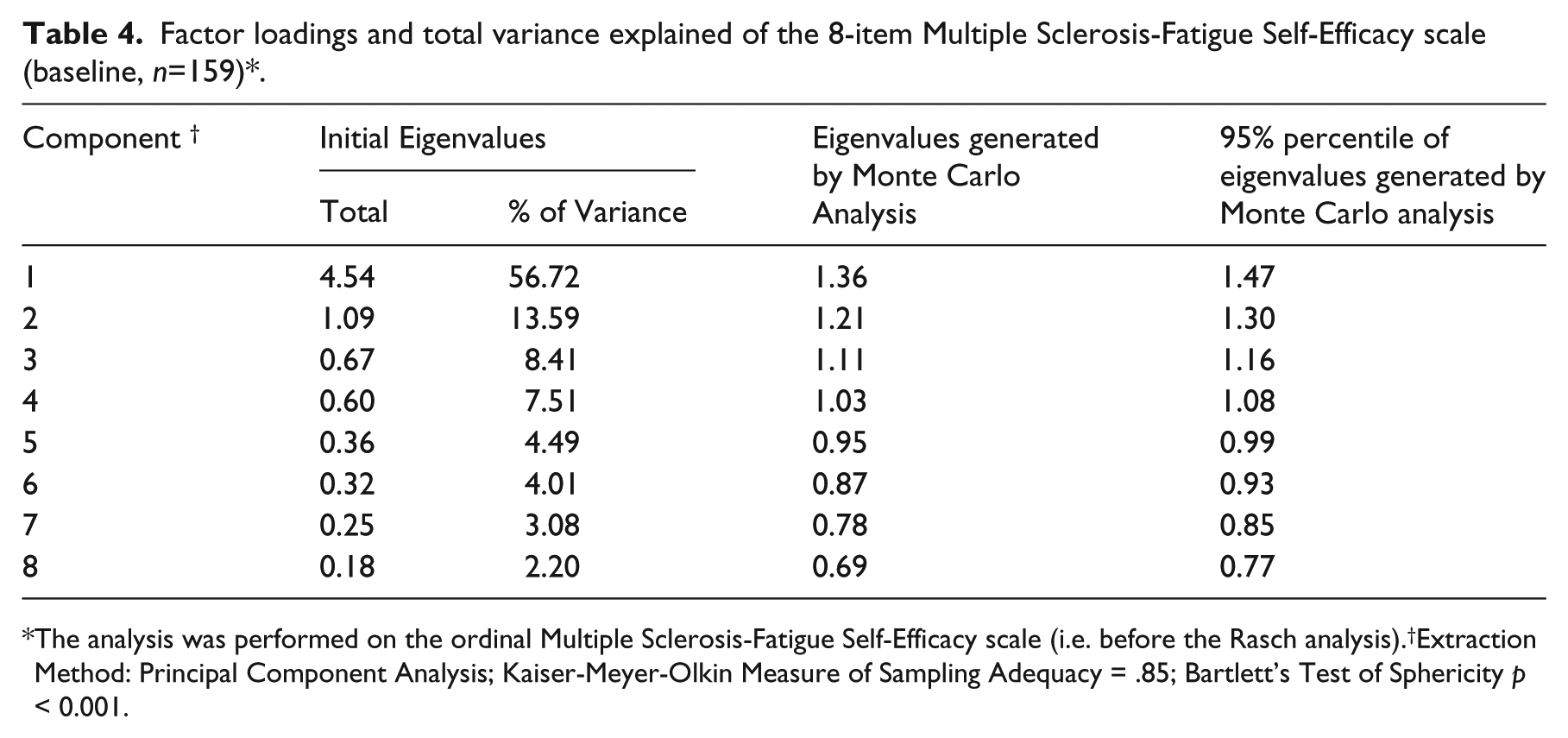
The analysis was performed on the ordinal Multiple Sclerosis-Fatigue Self-Efficacy scale (i.e. before the Rasch analysis).†Extraction Method: Principal Component Analysis; Kaiser-Meyer-Olkin Measure of Sampling Adequacy = .85; Bartlett’s Test of Sphericity p < 0.001.
Internal reliability
Cronbach’s alphas were good for the Fatigue Self- Efficacy Scale (8 item) at all four time points: 0.89 at baseline (n=156), 0.93 at 1 month follow-up (n=145), 0.94 at 4 months follow-up (n=142) and 0.90 at 1 year follow-up (n=129). The sample size at each time point is slightly smaller than in previous reported analyses as Cronbach’s Alpha requires responses to all items. Corrected item-total correlations (Pearson’s) were all high (>0.50) (Table 5). Cronbach’s Alpha would not have been improved had any of the items been deleted.
Item level characteristics 8-item Multiple Sclerosis-Fatigue Self-Efficacy scale (baseline, n=159)*.
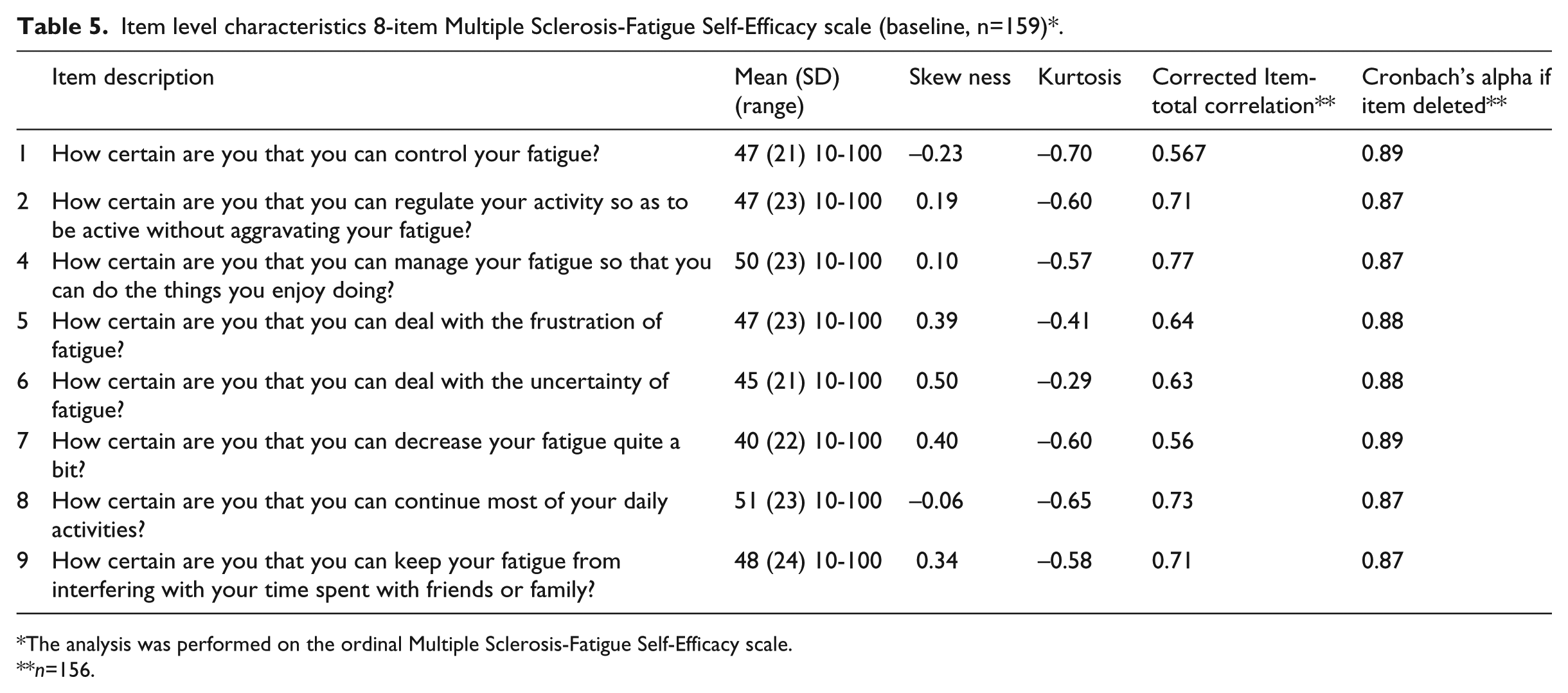
The analysis was performed on the ordinal Multiple Sclerosis-Fatigue Self-Efficacy scale.
n=156.
Convergent and discriminant reliability
As expected, the Multiple Sclerosis-Fatigue Self-Efficacy scale (8-item) had a strong positive association with the Multiple Sclerosis Self-Efficacy scale (rs32 = 0.78, p < 0.001). However, it should be noted that the Multiple Sclerosis Self- Efficacy scale and Multiple Sclerosis-Fatigue Self-Efficacy scale (8-item version) possess three identical items (items 1, 7 and 8). When these items were removed from the Fatigue Self-Efficacy Scale and a revised total score based on the 5 remaining items was calculated, the correlation still remained high (rs32 = 0.77, p <.001). The association between the Pain subscale from the SF-36 and the Multiple Sclerosis-Fatigue Self-Efficacy scale (8-item version) was low and non-significant (rs157= 0.11, p = 0.18). The association with the Global Fatigue Severity subscale of the Fatigue Assessment Instrument was rs157 -0.33 (p = < 0.001) and the correlation with the Vitality subscale of the SF-36 was rs157= 0.33 (p = < 0.001).
Rasch analysis
Initial fit to the Rasch model showed that two items had disordered thresholds (items 1 and 8) (Table 6, Analysis 1, Figure 1). Response categories 20 and 30 for these two items were collapsed. Once satisfactory, data were again fitted to the Rasch model (Table 6, analysis 2). The data did not deviate significantly from the Rasch model (non-significant Chi-square), the mean item fit residual was acceptable, items had satisfactory fit (non-significant Chi-square statistics) although the fit residual for one item was above the acceptable value of 2.5 (2.73). However, the data were not unidimensional and there was response dependency between the residuals of items 5 and 6 and items 8 and 9.
Fit of the Multiple Sclerosis-Fatigue Self-Efficacy scale to the Rasch Model.
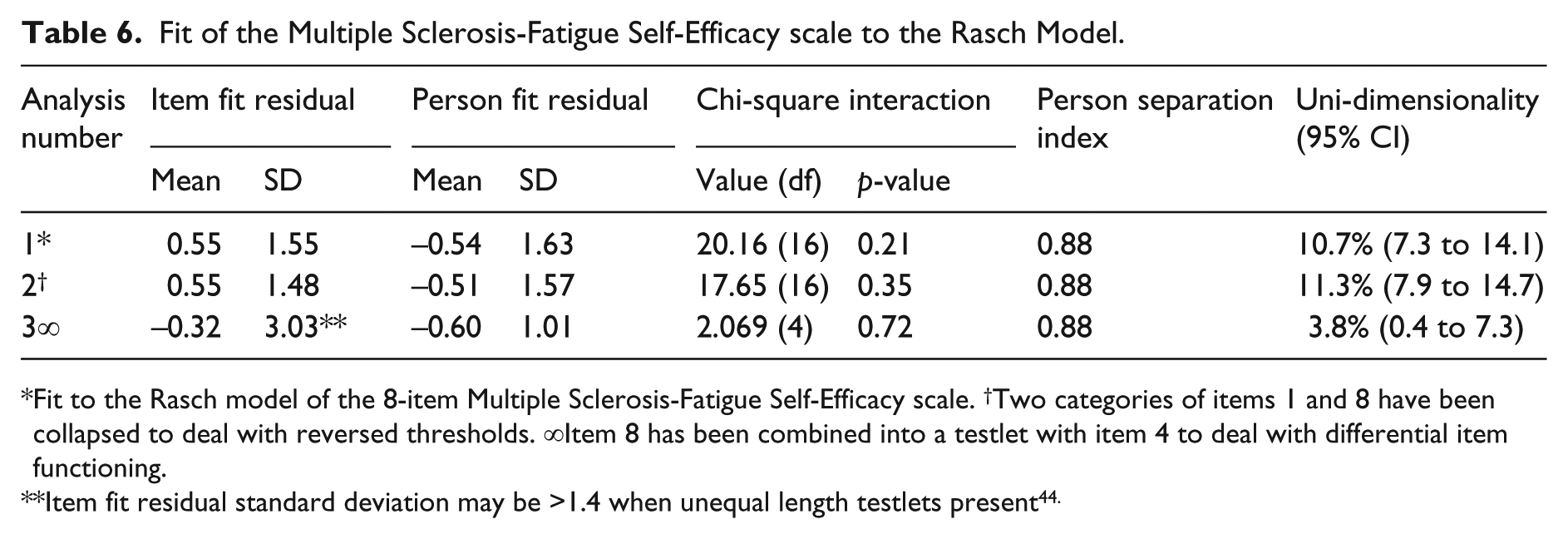
Fit to the Rasch model of the 8-item Multiple Sclerosis-Fatigue Self-Efficacy scale. †Two categories of items 1 and 8 have been collapsed to deal with reversed thresholds. ∞Item 8 has been combined into a testlet with item 4 to deal with differential item functioning.
Item fit residual standard deviation may be >1.4 when unequal length testlets present 44 .
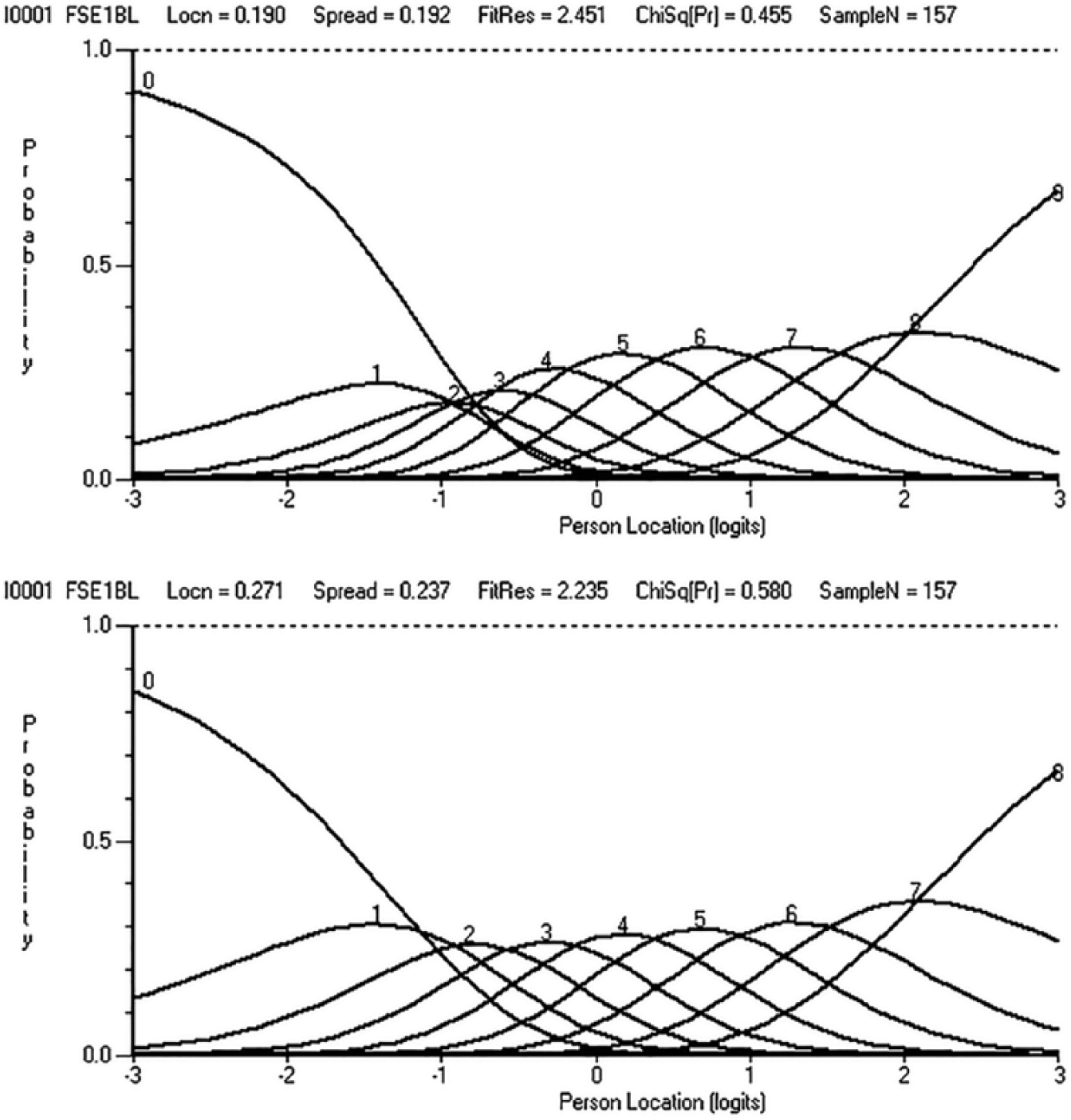
Threshold ordering item 1 (baseline data).
One item displayed significant uniform differential item functioning by level of disability (item 8). This item was combined into a testlet with an item that displayed non-significant differential item functioning in the opposite direction (item 4), with the remaining 6 items combined into a second testlet. This resulted in a unidimensional scale, with satisfactory fit to the Rasch model (Table 6, analysis 3). The A-statistic provides an indication of the variance that is lost once testlets are created; in our case A=1.0, suggesting the two testlets explained the same amount of variance in the data as the original 8-item scale. 42 A person separation index of 0.92 suggests the scale is suitable for group and individual use. 34 The person-item threshold map demonstrates a good spread of item thresholds and people along the construct of self-efficacy (Figure 2).
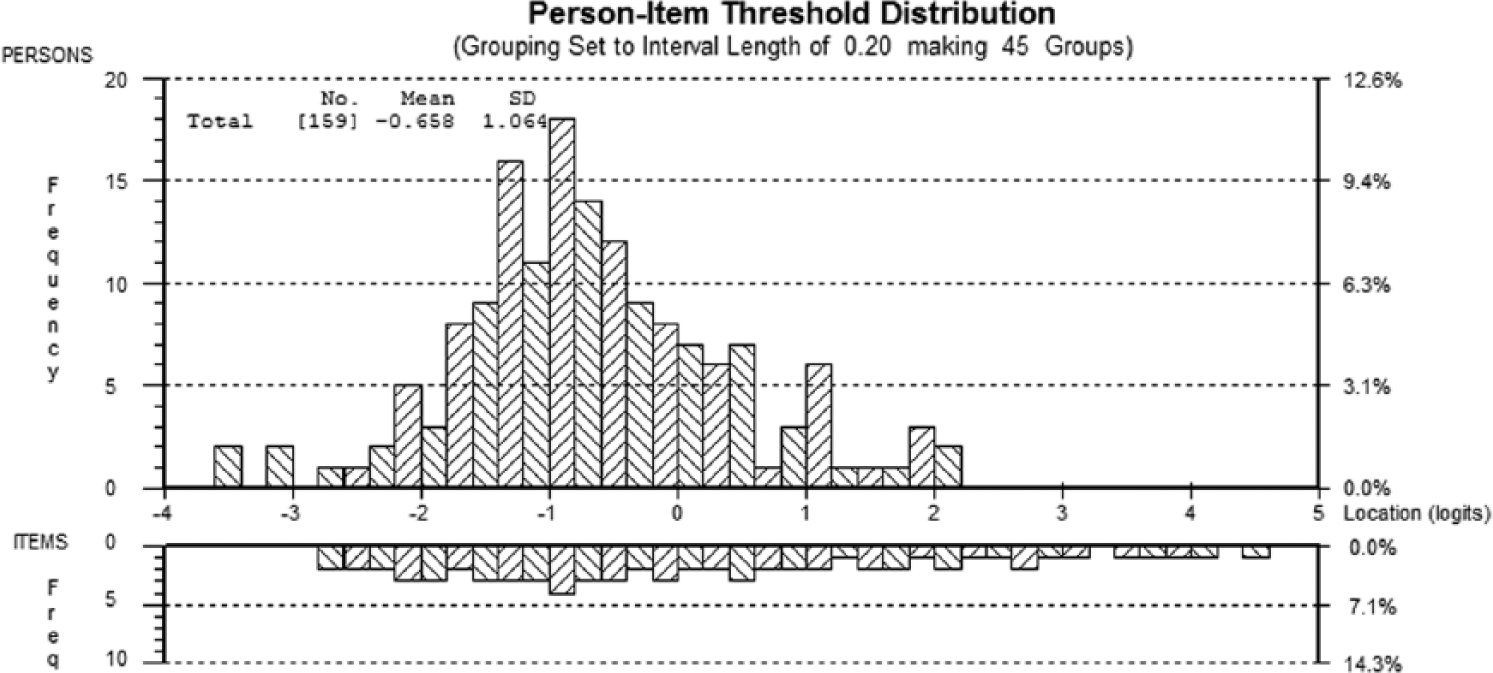
Person item threshold distribution 8-item Multiple Sclerosis-Fatigue Self-Efficacy scale.
Discussion
We have adapted a widely used measure of self-efficacy for people with multiple sclerosis to measure fatigue self-efficacy. Six percent of participants left item 3 blank because they felt it was not applicable. Consequently, these were not data missing at random, which Rasch analysis could have dealt with, but missing in a systematic way because participants were not able to answer the item. For this reason we deleted it from the 9-item scale. The 8-item scale demonstrated low levels of missing data, satisfactory internal consistency, convergent and discriminant validity, and sensitivity to change. Parallel analysis indicated one component. Our within participant effect sizes for the Multiple Sclerosis-Fatigue Self-Efficacy scale were higher than that found for the Multiple Sclerosis Self-Efficacy scale (0.52) in a study of a brief cognitive behavioural programme for people with multiple sclerosis. 18 Similarly, our effect sizes were higher than that found for the Liverpool Self-Efficacy Scale following a lay-led self-management programme (0.16) for people with multiple sclerosis. 43 Evidence for convergent validity was obtained with the Multiple Sclerosis-Fatigue Self-Efficacy scale correlating very highly with the most conceptually similar scale, the Multiple Sclerosis Self-Efficacy scale, and less so with measures of fatigue and pain. All 8-items had corrected item-total correlations > 0.5. Once two items (1 and 8) with disordered thresholds were rescored and the differential item functioning of item 4 was addressed via creation of a testlet, a unidimensional scale was achieved with a satisfactory fit to the Rasch model. This suggests that the initial lack of unidimensionality observed was spurious and driven by differential item functioning.
While other self-efficacy scales for fatigue have been developed 21, 23 they have not been validated in multiple sclerosis populations and have not included items related to unpredictability and interference with everyday life; domains likely to be highly relevant to people with multiple sclerosis. A strength of this study is that we have adapted an existing widely used scale in multiple sclerosis rather than developing a new measure. The Multiple Sclerosis-Fatigue Self-Efficacy scale drew upon items from Lorig’s Arthritis Self-Efficacy scale, which in turn was developed through consultation with patients and physicians and through study of four groups of patients. This ensures the patient centredness of the tool. Other strengths include the fact that as the sample was part of a multi-centre RCT the numbers are relatively large and include a range of disease type and duration. A limitation is that we do not have any information about those who did not wish to take part in the trial. Therefore, we cannot comment if there could be a response bias towards those with more self-efficacy. Another limitation is that we only have convergent validity data (correlating scores on the Multiple Sclerosis Self-Efficacy scale and the Multiple Sclerosis-Fatigue Self-Efficacy scale) on a relatively small sample (n=34) from our pilot work. Furthermore, we were unable to carry out a test-retest analysis for the Multiple Sclerosis-Fatigue Self-Efficacy scale. Finally, the scale will need language and cultural validation testing prior to use in languages other than English.
In conclusion, the Multiple Sclerosis-Fatigue Self-Efficacy scale is a valid and responsive scale that can be used for the measurement of self-efficacy in people with multiple sclerosis fatigue. A conversion table for converting raw scores on the Multiple Sclerosis-Fatigue Self-Efficacy scale to an interval scale is available from the authors.
Clinical message
The new Multiple Sclerosis-Fatigue Self-Efficacy scale is valid and able to measure change over time in people with multiple sclerosis.
Footnotes
Acknowledgements
Thanks to all the participants who took part and to the clinicians who identified the potential participants for the trial.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research was funded by the Multiple Sclerosis Society in the UK (grant number 846/06). The FACETS trial is included in the National Institute of Health Research Clinical Research Network (NIHR CRN) portfolio (ID 4843) and the ISRCTN is 76517470.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.