
Abstract
Objective:
To assess the treatment integrity of behavioural therapy for low mood in stroke patients with aphasia.
Design:
Participants were recruited to a multicentre randomized controlled trial (Communication and Low Mood; CALM trial) comparing behavioural therapy with a usual care control group.
Subjects:
Of the 51 participants randomly allocated to receive behavioural therapy, 44 participants completed treatment.
Methods:
Participants were assessed on measures of disability, language and mood. The number and length of therapy sessions, and therapist was recorded. Allocation of time to therapy components was compared across three phases of therapy. Associations between levels of disability, aphasia, mood and the therapy patients received were determined. Therapy content was compared between centres and at the beginning and end of the trial.
Results:
The mean number of therapy sessions was 9.1 (range 3–18, SD 2.6) and the mean duration of sessions was 58 minutes (range 30–89 minutes, SD 10.7). Allocation of time to each therapy component significantly differed across the three phases of therapy (P < 0.05). There were no significant associations (P > 0.05) between the length and number of sessions and patients’ aphasia, mood or disability, suggesting similar levels of therapy were provided regardless of patients’ characteristics. The content of therapy showed some differences between centres (P < 0.01) and there was programme drift in some components of therapy.
Conclusions:
The results support the ability of the therapists to deliver behavioural therapy according to the treatment manual. However there were differences between centres and over time in some components of therapy.
Introduction
Studies of psychological therapies after stroke typically lack detailed information on the time spent on different therapy components over the course of treatment and the extent to which therapists adhere to a treatment manual, 1 and this is hindered by the lack of an adequate system to describe complex interventions. 2 In addition to defining treatment it is also essential to assess treatment integrity, defined as the extent to which a treatment is carried out as intended, or as the treatment manual dictates. 3 Integrity evaluations are important in order to monitor and enhance the validity and reliability of therapeutic interventions,4,5 and thus to draw accurate conclusions about treatment efficacy. If treatment effects are found, it is necessary to be clear that these effects are a direct result of the active ingredients of therapy delivered.6–8 Conversely, should null effects be found and integrity levels are unclear, it is necessary to ascertain whether this was due to an ineffective treatment, or an effective one administered inappropriately.9,10 Treatment integrity evaluations also facilitate replication of research studies, by ensuring the documentation and subsequent reporting of the exact content of therapy. 11
Measuring treatment integrity
A number of frameworks have been identified to inform assessments of treatment integrity, although no single method has been widely accepted, resulting in little cross-study consistency. One of the more comprehensive approaches available suggests that checks should be carried out in five areas: study design, training provided for therapists, treatment delivery by therapists, patients’ receipt of treatment, and patients’ enactment of treatment skills. 4 Among the more detailed recommendations 9 is the requirement that a clear description be provided of the areas being tested within the treatment definition. It is also suggested that there should be clear statements relating to the training and experience of therapists and their characteristics. Further recommendations cover the use of treatment manuals, therapist supervision, cues and prompts, verification of treatment, treatment documentation, methods of verification, reporting of integrity evaluations, and using these to interpret findings.
The present study assessed the treatment integrity of behavioural therapy given to stroke patients with aphasia and low mood who were treated as part of a multicentre randomized controlled trial examining the effectiveness of behavioural therapy (Communication and Low Mood study (CALM)). 12 Informed by the frameworks described, our approach to assessing treatment integrity included stating the training of therapists, use of and adherence to the therapy manual, and documentation of therapy content. Competency in delivering the therapy was assessed by examining whether patients’ levels of mood, physical and language ability affected the amount and duration of therapy.
In previous work examining the treatment integrity of behavioural therapy, 13 treatment was divided into phases, reflecting the predicted differences in treatment content between sessions (e.g. where the opening session may feasibly only contain an explanation of treatment rationale). This approach was followed as the CALM study allowed for a variable number of therapy sessions across patients.
It has been proposed that, in measuring treatment integrity, assessments should be made of therapists’ adherence to treatment protocol, as well as their level of competency in delivering complex interventions.6,14,15 In the context of the present study, competence in delivering therapy entails taking into account contextual variables, such as the patient’s level of physical and language disability, as well as their stage in therapy and what gains may already have been achieved.
One aspect of treatment delivery that needs to be assessed in integrity evaluations is programme drift, whereby therapists deviate from the therapy manual as treatment progresses. In multicentre studies, or in studies using multiple therapists, checks are essential to determine whether treatments were implemented in the same way across centres or therapists, or that any differences, such as programme drift, are documented and measured. 16 As a result of these checks it is then possible to make a decision on whether or not to include data if treatment has not been delivered in accordance with protocol. 17 Therefore the present study will check for consistency in therapy delivery across centres and across the duration of the trial.
The aims of the present study were: to compare the content of three phases of therapy (beginning middle and end) to determine whether the time spent on different components of therapy changed as therapy progressed; to determine the relation between the number and duration of therapy sessions and language abilities, mood and disability; and to compare the delivery of the intervention between study centres and at the beginning and end of the trial.
In the Communication and Low Mood (CALM) study it was expected that, as the course of therapy progressed, the amount of time spent on different therapy components would change. Certain components, such as explaining the therapy rationale to patients, were expected to be more frequent at the beginning of therapy and to decrease as therapy progressed, whereas the more active ingredients of therapy, such as graded task assignment and problem-solving, were expected to become more frequent as time progressed. It was further predicted that the session length and number of sessions received by patients would vary according to the severity of aphasia and mood problems. Those with greater problems were predicted to require more treatment sessions. As therapists were expected to adhere to a treatment manual it was also predicted that there would be no significant difference between therapists in the content of the intervention provided. In addition, there would be no difference between therapy provided to patients treated earlier in the trial and those treated later in the trial.
Methods
Participants were recruited from the Communication and Low Mood (CALM) study. 12 This was a multicentre randomized controlled trial comparing behavioural therapy with a usual care control group. Participants were eligible for the CALM study if they suffered from aphasia and had low mood, as identified using either the ‘sad’ item of the Visual Analog Mood Scales (VAMS) 18 or the Stroke Aphasic Depression Questionnaire 10-item hospital version (SADQH-10). 19 Patients were excluded if they were blind, deaf, had dementia documented in their medical notes, were unable to speak English prior to stroke, or were receiving treatment for depression at the time of their stroke. Patients were recruited from six centres (Nottingham, Mansfield, Chesterfield, Sheffield, Leicester and Lincoln).
Baseline assessments included the Sheffield Screening Test for Acquired Language Disorders (SST), 20 the Frenchay Aphasia Screening Test reading and writing subtests (FAST), 21 Barthel Index 22 and a picture-based measure of self-esteem (Visual Analogue Self-Esteem Scale (VASES)). 23
Participants allocated to behavioural therapy could receive up to 20 sessions of treatment over three months, with each session lasting approximately one hour. Sessions took place at the participants’ place of residence. Therapy was delivered by one of eight assistant psychologists who each received weekly local supervision from a clinical psychologist, in addition to monthly supervision meetings with a consultant clinical neuropsychologist, which were attended by all study therapists. The delivery of therapy was monitored by observation of therapy sessions by the chief investigator (ST). All therapists were given training by speech and language therapists in communication skills with people with aphasia. Training was also given in delivering behavioural therapy in accordance with the treatment manual. The exact intensity of therapy was left to the discretion of the assistant psychologist. This was a pragmatic trial and therefore needed to reflect clinical practice.
The therapy manual was developed from studies of cognitive behavioural therapy (CBT) for depression in stroke 24 and in older adults, 25 and from guidelines on conducting CBT with people with aphasia. 26 Therapy consisted of behavioural techniques used in the treatment of depression. Treatment strategies focused on maximizing mood-elevating activities and included education, activity monitoring, activity scheduling and graded task assignments. Participants were given homework tasks to complete between sessions, such as attempting an activity or a component of an activity as part of a graded task assignment. The intervention was tailored for the individual’s needs, and communication resources were used as appropriate. For example, pictures and photograph were used to support conversation for identifying and monitoring activities.
The content of therapy was documented using record forms completed by therapists at the end of each session and was checked for consistency with the therapy manual. The therapy recording form listed 11 components of therapy: explanation of treatment, assessment, communication, goals, activities, graded task assignment, problem-solving, homework, summary and review, generalization, and ‘other’. These were further broken down into a total of 29 subcomponents (see Appendix, available online). Therapists were required to record the number of 10-minute time intervals spent on each subcomponent of therapy at the end of each session. In addition, details were also recorded of the therapist who delivered the therapy, the study site at which it was administered, the session number, and whether anyone else was present (e.g. a relative) and, if so, whom.
Data analysis
As the number of therapy sessions could vary, the therapy for each participant was divided into three treatment phases to enable assessment of how therapists altered their focus during sessions as therapy progressed. These phases were: the beginning (Phase 1), middle (Phase 2) and end (Phase 3). If the total number of therapy sessions completed was five or more, the first two and last two therapy sessions were pre-allocated to Phases 1 and 3 respectively, and all other remaining sessions allocated to Phase 2. If the number of sessions received was less than five, then the first session was allocated to Phase 1 and the last session allocated to Phase 3.
The total amount of time spent on each component of therapy in each treatment phase, and the mean percentage of time allocated per component for each treatment phase, were then calculated and used to compare therapy content across the three phases.
Spearman’s rank correlations were calculated between mean session length, number of sessions received, and language ability (Frenchay Aphasia Screening Test, Sheffield Screening Test), mood (Visual Analog Mood Scales ‘sad’, Visual Analogue Self-Esteem Scale, Stroke Aphasic Depression Questionnaire) and disability (Barthel).
The delivery of therapy was compared between geographical centres. Patients were grouped according to the centre where they were recruited. As the same therapist covered Mansfield and Chesterfield, these two centres were grouped together. There were insufficient patients recruited from Lincoln or Leicester to include these in this analysis. There were changes of therapist over time in both Nottingham and Sheffield.
Finally, comparisons were conducted between the delivery of therapy for participants recruited earlier in the trial (first half of the sample) as compared with those recruited later (second half of the sample).
Results
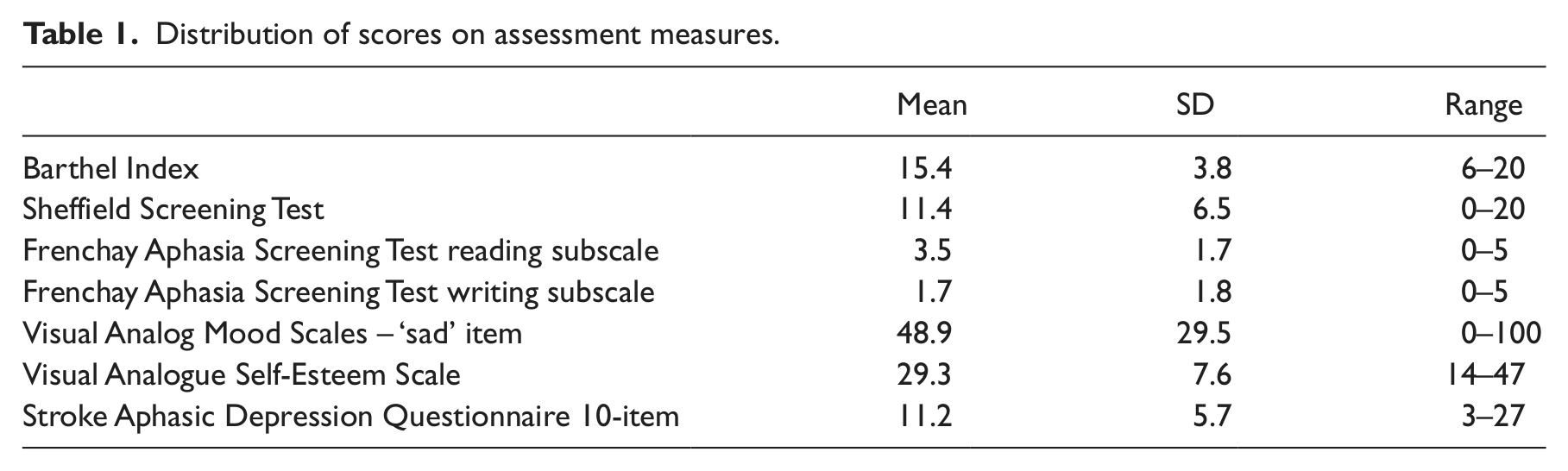
Fifty-one participants were randomly allocated to receive behavioural therapy. Of these, 48 (94%) agreed to receive therapy and 44 (86%) completed the therapy and had therapy records available for analysis. The 44 participants were aged between 42 and 89 years (mean 67.41, SD 14.17) and 25 (57%) were men. Patients received a mean of 9.1 sessions (range 3–18, SD 2.6) and the mean duration of each session was 58 minutes (range 30–89, SD 10.7). The distribution of scores on the assessment measures are shown in Table 1.
Distribution of scores on assessment measures.
Since the data were not normally distributed, a Kruskal–Wallis one-way ANOVA was performed to compare the three phases of therapy. Results are shown in Table 2. As expected, there were significant differences in all of the therapy components across the phases of therapy. Explanation of treatment, assessment, and goals were most frequent in Phase 1. Activities, graded task assignment, problem-solving and homework were most frequent in Phase 2. Summary and review, generalization and ‘other’ aspects of therapy were most frequent in Phase 3.
Median proportion of time (percentage) spent on components of therapy over the three therapy phases.
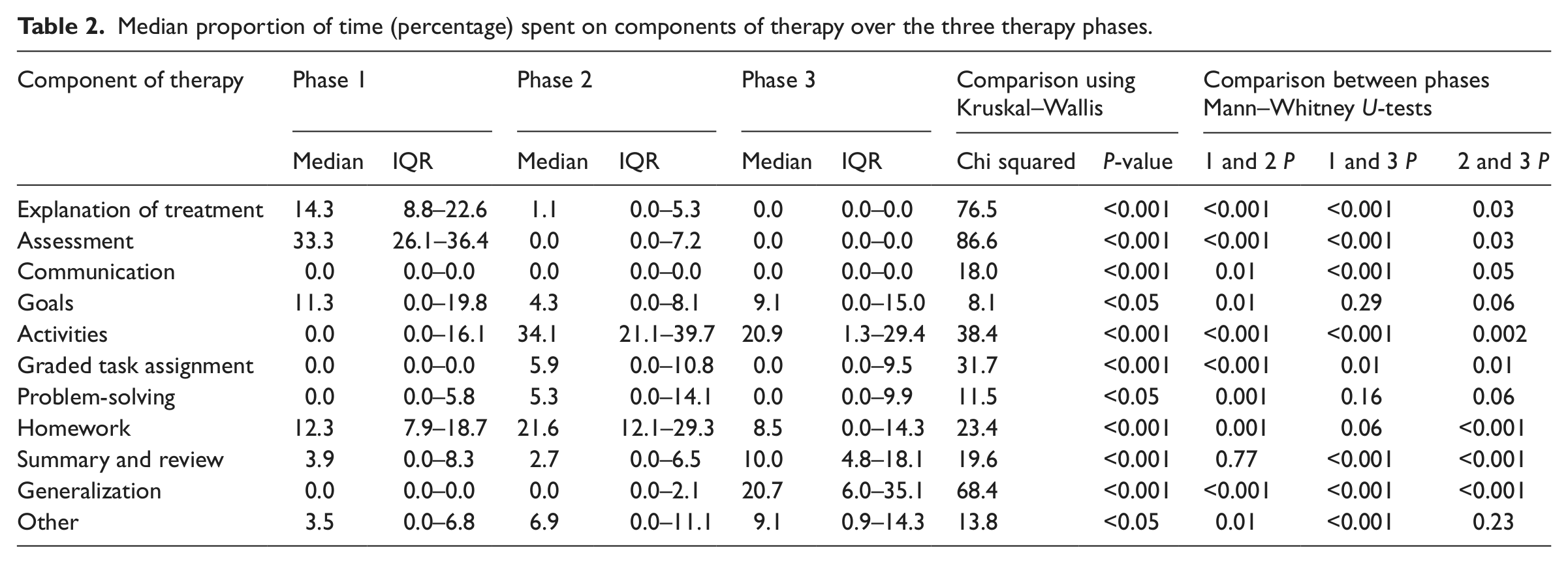
Mann–Whitney comparisons were conducted to compare pairs of phases. Due to the nature of multiple testing, significance was determined if p ≤ 0.02. There were significant differences between phases in the time spent on specific components (see Table 2). Compared with the other phases more time in Phase 1 was spent on explanation of treatment, assessment and communication; more time was spent on activities, graded task assignment and homework in Phase 2; and more time in Phase 3 was spent on summary and review and generalization.
Spearman’s rank correlations were calculated between the mean number of therapy sessions and mean session length per participant, and their scores on assessments. Results are shown in Table 3. Contrary to our predictions, there were no significant relationships between the severity of communication impairment, disability or severity of mood problems, and either session duration or number of sessions.
Correlations between mean number and duration of therapy sessions and scores on assessment measures.
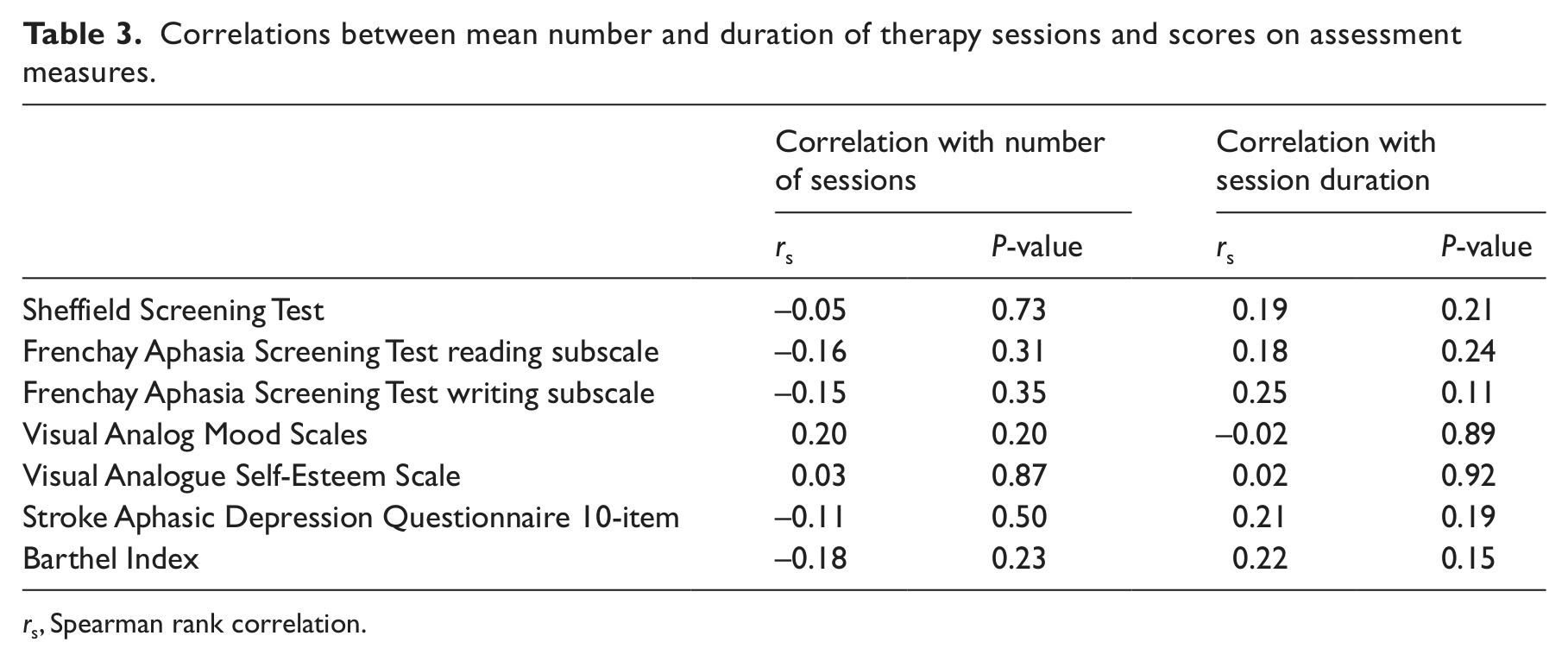
rs, Spearman rank correlation.
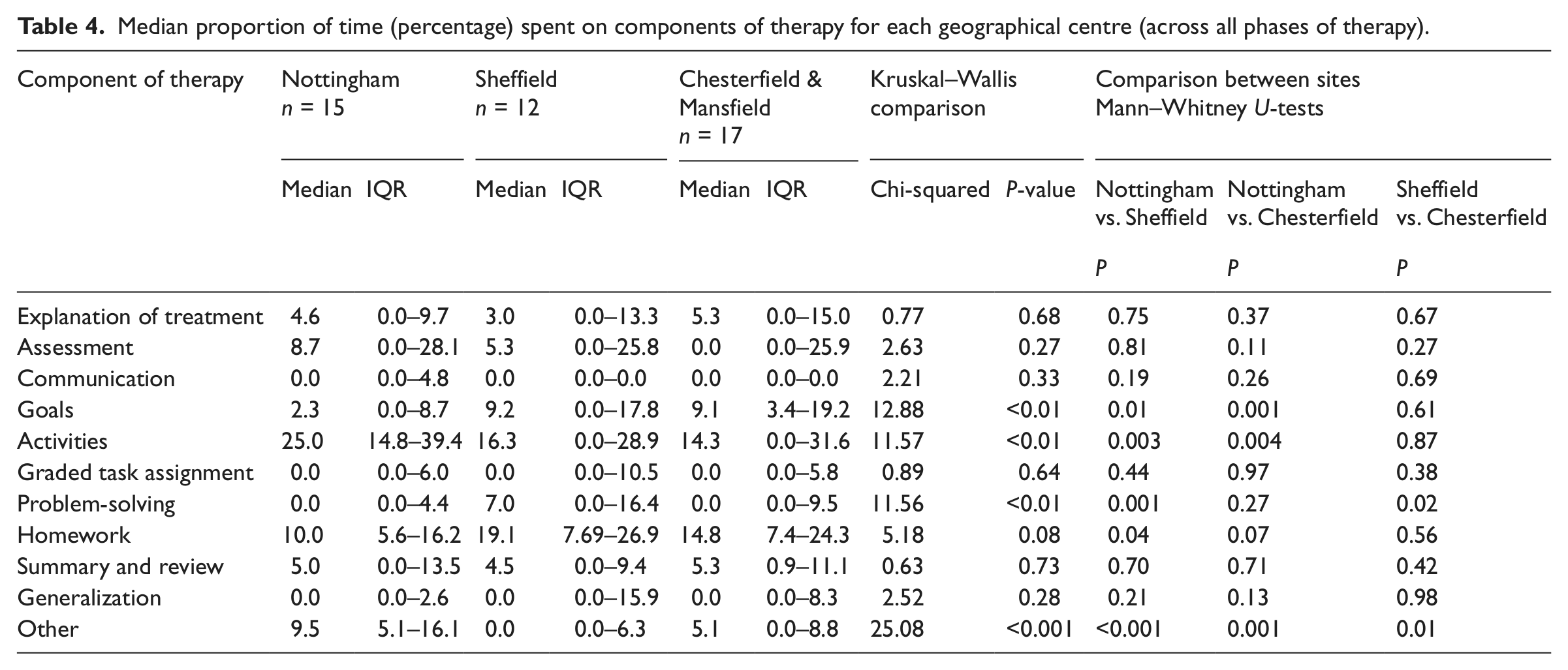
A Kruskal–Wallis one-way ANOVA was performed to compare content of therapy across the three geographical centres, and Mann–Whitney comparisons were conducted to compare pairs of centres. Results are shown in Table 4. Contrary to our expectations, there were significant differences between centres in the amounts of time spent setting goals, activities, problem-solving and other (P < 0.01). Nottingham therapists spent significantly less time goal-setting than therapists in Sheffield or Mansfield and Chesterfield. The Nottingham therapists spent significantly more time giving participants activities to do. Sheffield patients spent significantly more time on problem-solving than patients in either of the other centres.
Median proportion of time (percentage) spent on components of therapy for each geographical centre (across all phases of therapy).
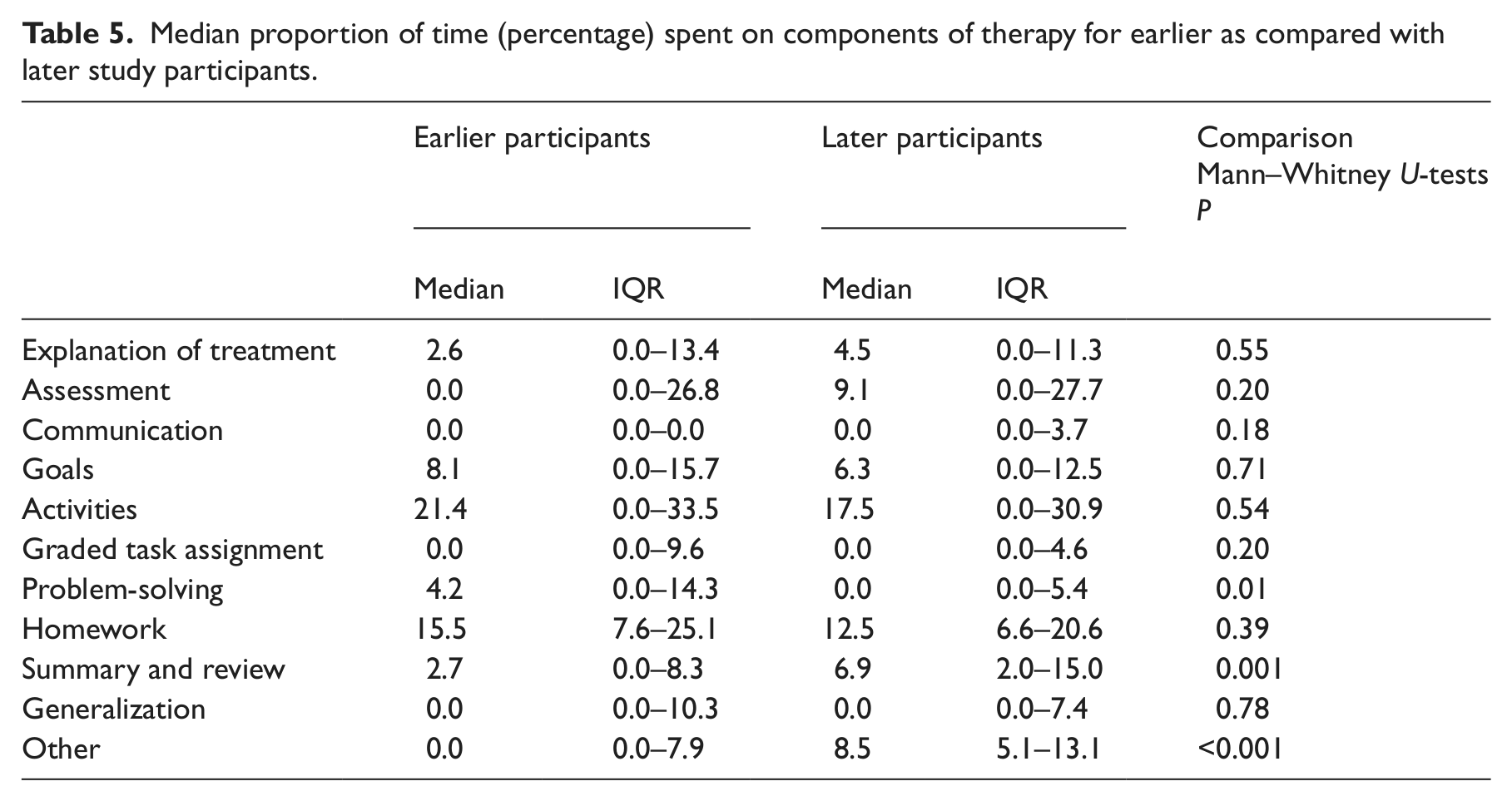
Finally, comparisons were carried out of the content of therapy provided to patients recruited earlier in the study (first half of the sample) compared with those recruited later in the study (second half of the sample). Results are shown in Table 5. In contrast to our expectations, there were significant differences between the amounts of time spent on problem-solving, with more time being spent on this earlier in the study (P < 0.01), and between the amounts of time spent on summary and review and ‘other’ (P < 0.001), with more time being spent on these activities later in the study.
Median proportion of time (percentage) spent on components of therapy for earlier as compared with later study participants.
Discussion
In a multicentre randomized controlled trial of behavioural therapy for low mood in stroke patients with aphasia, the mean number of therapy sessions received by patients was nine, with a mean duration of 58 minutes. The therapists focused on different components of behavioural therapy over time as treatment progressed. There were no significant associations between the severity of aphasia, level of disability, or severity of mood disorder and the length of sessions or the number of sessions received. There was evidence of some differences between centres and programme drift in some components of therapy.
The mean number and duration of therapy sessions is in accordance with the treatment manual, which states as a guideline that up to 20 sessions of therapy may be given but provides the example structure for 10 therapy sessions of approximately one hour long. Significant differences were observed between the times spent on the 11 components of therapy over the three therapy phases At the beginning of therapy, the majority of time was spent explaining the therapy rationale, assessing the needs of the patient, determining how best to communicate with them and discussing the goals of therapy. In the middle phase, most time was spent identifying and reviewing the patients’ activities, designing graded task assignments, teaching problem-solving and reviewing homework. As therapy was being concluded, generalizing and summarizing therapy, as well as covering any outstanding issues, were carried out. These results demonstrated that therapists altered the amount of time spent on each component of therapy as therapy progressed, following the structure of the behavioural therapy programme outlined in the manual.
Relatively little time was spent on ‘communication’ (establishing intact communication skills, developing communication resources and practicing communication skills) over all three of the therapy phases. This means that the emphasis was on treating the mood disorder rather than helping with the communication problem, in accordance with the goal of the behavioural therapy intervention. However it is possible that therapists’ competence in supported communication may have influenced the amount of time that was spent on communication and this was not assessed in the present study. The finding that the number and duration of therapy session was not associated with the severity of aphasia, level of disability, or severity of mood disorder could be due to the content of therapy being changed according to the nature of participants’ difficulties rather than the format of sessions.
There were some differences between centres in the delivery of the intervention. The characteristics of the participants did not differ significantly between these centres and so this suggests variation in the way therapists delivered therapy for the same type of participant. It was not specified in the manual exactly how much time should be dedicated to each element, and so variations may not necessarily reflect deviation from the manual. In addition, the sample sizes are small so these may be chance observations. There were also some differences in therapy delivered early in the study as compared with that delivered later. However, the therapists also changed over time in both Nottingham and Sheffield, so these differences may reflect differences between therapists rather than programme drift over time. Again these occurred on components that were not constrained by the manual. It also may be that therapy needs to be delivered flexibly according to the needs of the patient, as would occur in usual clinical practice. However, it suggests that more detail could be included in the balance of these components across sessions in order to ensure a more consistent delivery of the intervention in future research.
A number of limitations in this study should be recognized. Video recording would have reduced reliance upon therapists’ self-reporting and accurate completion of therapy forms, which was a potential source of error since records were completed retrospectively at the end of therapy sessions. Such monitoring of sessions would also have allowed for inter-rater reliability of the therapy descriptions to be assessed. However, video recording was not feasible, since therapy was conducted in participants’ own homes, and may have affected participants’ engagement in therapy. The use of a recording form is comparable to the approach taken in other studies describing other rehabilitation interventions.27–29 In addition the sample sizes are small when comparisons were conducted between centres. We also did not evaluate other aspects of treatment integrity such as therapist competence.
The therapists administering behavioural therapy in this study demonstrated adherence to the treatment manual. This investigation used a detailed and replicable method of assessing therapist adherence and adheres to recommendations found in the literature.4,6,9 It also provides a summary of the content of the intervention. The findings suggest that further detail could be added to the therapy manual to increase the consistency in the delivery of the intervention, particularly in relation to goal-setting, activity-setting and problem-solving, as these differed between centres.
As some differences across centres were found, this suggests that there needs to be more rigorous monitoring of therapy content both across therapists and across centres over time, to ensure consistency of delivery of treatment in multicentre studies or those with multiple therapists.
Clinical messages
Therapists demonstrated adherence to the behavioural therapy manual.
Therapists focused on different components of behavioural therapy over time as treatment progressed.
Some differences between centres and programme drift suggest the need to add detail to the manual and systematically monitor therapy across therapists and centres over time.
Footnotes
Conflict of interest
None declared.
Funding
The funding was provided by The Stroke Association, UK (TSA 2007/03).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.