
Abstract
Objective:
To investigate the feasibility, acceptability, and safety of a supervised video game exercise program administered via Dance Dance Revolution in individuals with Huntington’s disease.
Design:
A cross-over, controlled, single-blinded, six-week trial.
Setting:
Home-based.
Participants:
Eighteen ambulatory individuals with Huntington’s disease (seven male, mean age 50.7 SD 14.7).
Interventions:
Participants played the Dance Dance Revolution game with supervision and the handheld game without supervision for 45 minutes, two days per week for six weeks.
Outcome measures:
Game play performance and adherence, participant perceptions of the game, safety (vital signs, adverse health changes), spatiotemporal gait measures, Four-Square Step Test, Tinetti Mobility Test, Activities-Specific Balance Confidence Scale, and World Health Organization Quality of Life – Bref, before and after each intervention.
Results:
Most participants improved on game play, enjoyed playing the game, and wanted to continue playing after study completion. After playing Dance Dance Revolution, participants showed significant reductions in double support percentage (adjusted mean difference (95% confidence intervals): –2.54% (–4.75, –0.34) for forward walking and −4.18 (–6.89, –0.48) for backward walking) and those with less severe motor symptoms had reductions in heel-to-heel base of support during forward walking. The remaining measures were not significantly impacted by the intervention.
Conclusion:
Dance Dance Revolution appears to be a feasible, motivating, and safe exercise intervention for individuals with Huntington’s disease.
Introduction
Huntington’s disease is a hereditary disease that causes physical, cognitive, and psychological deterioration. People with Huntington’s disease develop motor symptoms that impair daily activities, increase fall risk, and lower quality of life. 1,2 Balance and gait deficits contribute to falls. 3 These deficits include greater postural sway, delayed balance reactions, slower gait, shortened stride length, widened support base, and increased stance and double support time. 3,4 Individuals with Huntington’s disease also have increased gait parameter variability that may increase fall risk. 3,4 Falls frequently occur when maneuvering around or stepping over obstacles. Thus, interventions that help prevent or ameliorate balance and gait impairments would benefit this population.
There is emerging evidence that exercise improves gait and balance in individuals with Huntington’s disease. Zinzi and colleagues demonstrated that an inpatient multidisciplinary rehabilitation approach lasting three weeks can improve function in mobility and activities of daily living. 5 Several studies have demonstrated the benefits of a physical therapy program incorporating posture, gait. and balance training for improving motor function. 5 –7 Additionally, a home-based strengthening exercise program was shown to improve gait and balance when supervised by a family member or caregiver. 8 However, apathy, depression, motor problems, and inadequate transportation present exercise barriers. 13 Programs that are enjoyable, motivating, and home-based may overcome these barriers. 8
Research has shown that video game-based exercise increases practice volume, attention span and compliance compared with traditional exercise programs. 10,11 Video game play that included dynamic, coordinated exercise significantly improved balance, mobility, fall risk, and cognition in individuals with Parkinson’s disease. 10,12 In the game Dance Dance Revolution, players step to targets in response to visual cues matching a song rhythm. The game incorporates balance training methods (multidirectional stepping), attentional strategies (performance biofeedback), and external cueing (step synchronization to music), which are recommended for individuals with basal ganglia disorders. 13,14 Thus, Dance Dance Revolution may help overcome exercise barriers while targeting motor deficits in people with basal ganglia disorders. To date no studies have examined the use of video games as an exercise intervention in Huntington’s disease.
This study evaluated the feasibility, acceptability, and safety of a supervised video game-based exercise program using Dance Dance Revolution in individuals with Huntington’s disease. We also explored the potential benefits of participation on dynamic balance, gait and mobility, quality of life, fall risk, and neuropsychological functions. We hypothesized that individuals with Huntington’s disease would be able to improve their performance and be motivated to play the video game.
Methods
The university Human Subjects Institutional Review Board approved this study. All participants signed written informed consent and photographic permission forms.
Twenty-four individuals with a diagnosis of Huntington’s disease participated. Participants were ≥ 18 years old, walked 10 m without assistance, and lived within 45 miles from the Center. As this was intended as a feasibility study, ambulatory patients across a wide range of disease severity were included in the study. Individuals with other neurologic diagnoses or conditions that impacted gait, or were unable to understand informed consent or study procedures were excluded.
Demographic information (age, sex, diagnosis date) was obtained. A neurologist (SK) rated participants on the Unified Huntington’s Disease Rating Scale motor section and the Total Functional Capacity Score. 15 The Unified Huntington’s Disease Rating Scale cognitive battery (symbol digit modalities, stroop color, reading and interference, and verbal fluency tests) was administered to measure neuropsychological functions.
A crossover design was used. Participants entered the Dance Dance Revolution or handheld video game interventions and crossed over after six weeks (Figure 1). Participants were alternately assigned to interventions in cohorts of three, based on home location, to minimize travel time and costs, and ensure researcher availability to conduct sessions.
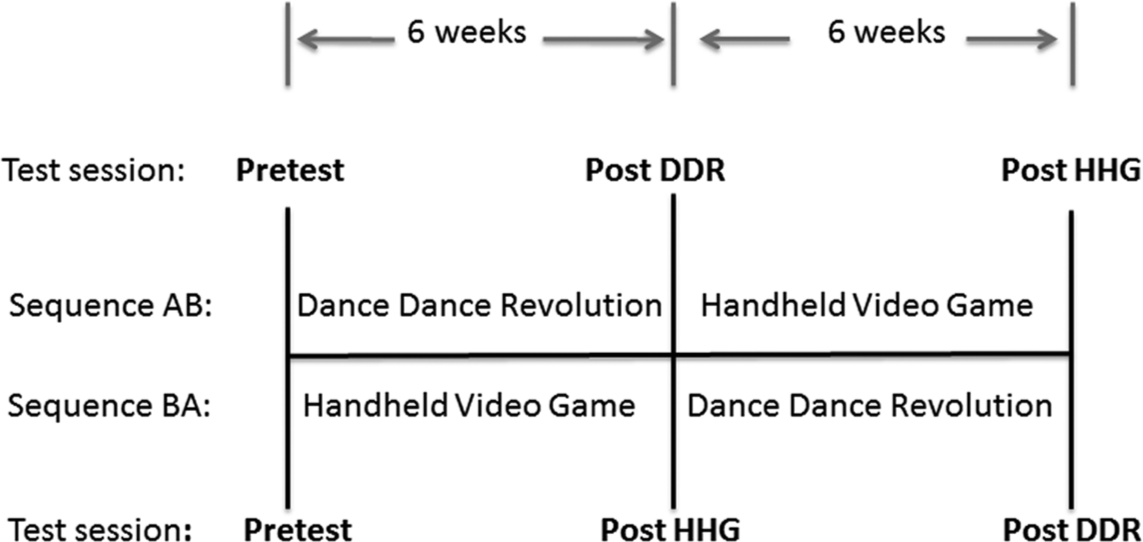
Experimental design.
Dance Dance Revolution and handheld video games were played for 45 minutes, two days per week for six weeks. Dance Dance Revolution (Harmonix Music Systems Incorporated, Cambridge, Massachusetts) game software (Dance Central) was loaded on a computer and played on a dance pad (DDRgame, South El Monte, California) with four multidirectional arrows (Figure 2, available online). Participants pressed the arrows using their feet in response to arrows that appeared on a monitor and that were synchronized to song beats. Success depended upon the participants’ abilities to step on the correct arrow at the correct time. A gage gave performance feedback throughout each song. Three research team members were trained to provide supervision during Dance Dance Revolution game play including selecting songs, setting song speed and progressing it in 25% increments when game performance scored at A or “excellent”, cueing as needed, and ensuring safety.
Handheld video game (i.e. Bingo, Blackjack, Solitaire) play controlled for Dance Dance Revolution effects of using a novel technology and/or a cognitively stimulating activity. Those who could not play the handheld video games owing to manual dexterity or game operation difficulties played card or board games. A researcher made weekly phone calls to monitor game play compliance and provide social contact.
Evaluations were performed before and at the end of each intervention at the clinic (Figure 1). All testing was performed by one researcher (AK) who was blinded to the study arm. The following outcome measures were assessed to explore potential benefits of the Dance Dance Revolution intervention.
To determine feasibility (ability to play game, adherence), game play success was measured by the difficulty of songs played as determined by foot placement patterns, step interval time, and by skill-level measures provided by the Dance Dance Revolution software, including number of correct steps for a given song and maximum combinations (i.e. longest string of correct steps without a misstep within one song). Adherence was measured by the numbers of individuals who completed all treatment sessions.
Acceptability was examined by asking participants at study end whether they liked or were challenged by the game, and if they would consider continuing game play.
Safety was examined through monitoring of heart rate and blood pressure, and adverse health changes (falls, excessive fatigue, vital signs outside American College of Sports Medicine guidelines) before and after each Dance Dance Revolution game play session. 16
Forward spatiotemporal gait parameters (comfortable speed) were assessed using a 4.9-m computerized GAITRite (CIR Systems, Inc, Haverton, PA) system. GAITRite measures are reliable in Huntington’s disease. 17
To measure gait maneuverability, spatiotemporal gait parameters were assessed during forward and backward walking, and while avoiding three obstacles (i.e. upright tube to step around, foam roll to step over, and low-hanging bar to duck under) placed 1 m apart on the GAITRite walkway (per Lowrey et al. protocol). 18
Forward and backward gait parameter variability was measured by calculating coefficients of variation. Individual step measures were averaged across three walkway trials. 19
The Four-Square Step Test and the Tinetti Mobility Test measured dynamic balance and mobility. The Four-Square Step Test requires rapid multidirectional stepping over a cane and predicts falls in the elderly. 20 The Tinetti Mobility Test consists of balance and gait subscales with higher scores indicating better performance. It is reliable and predicts falls among those with Parkinson’s disease and Huntington’s disease. 21,22
The Activities-Specific Balance Confidence Scale is reliable and valid in elderly 23 and neurological populations. 24 Individuals rate their balance confidence from 1–10 on 16 tasks; higher scores indicate greater confidence and lower fall risk. 23,25,26
Quality of life was measured with the World Health Organization Quality of Life – Bref (WHOQOL-Bref) assessment. 27,28 Responses on 26 items are on a five-point scale (from 1 = very dissatisfied to 5 = very satisfied). The WHOQOL-Bref has good reliability and validity. 27,28
To assess game play improvement, the mean proportion of correct steps per song by participant was calculated for the first and last two sessions, including only songs that were encountered in both sets. Changes in the mean proportions were compared using a paired t-test. A similar approach was used to compare the maximum correct combination of steps. Descriptive statistics were used to describe answers to open-ended questions and safety results.
In accordance with the crossover design, a mixed-effects regression model evaluated the intervention effect while adjusting for period, treatment, sequence, participant age, and the baseline outcome value. 29 A random effect for participant was included to account for the dependence of the repeated measures. All comparisons were considered exploratory and hypothesis generating; no adjustments were made in these analyses for multiplicity. All gait parameters and their coefficients of variation were analyzed for forward and backward walking, but velocity was the only measure analyzed for the obstacle condition. Comparisons of the outcomes by intervention group prior to crossover were conducted using a linear regression model adjusting for age and the baseline value of the outcome. After the initial analysis, possible differential treatment effects of disease severity were evaluated for gait and non-gait outcome measures by including a dichotomous indicator of motor burden of disease severity (Unified Huntington’s Disease Rating Scale motor score ≤ 42 versus Unified Huntington’s Disease Rating Scale motor score > 42) and an interaction between this indicator and the intervention. The Unified Huntington’s Disease Rating Scale motor score represents the motor disability; scores below 42 out of 124 represent less motor impairment, while higher scores indicate increased disability and fall risk. 22 The Unified Huntington’s Disease Rating Scale motor score correlates strongly with the Total Functional Capacity Score, a measure of functional burden of disease.
Results
Of the 24 participants who entered the study, six participants did not receive the Dance Dance Revolution intervention owing to other medical or scheduling problems (n = 5) or for unknown reasons (n = 1) (Figure 3). Participant characteristics are described in Table 1.
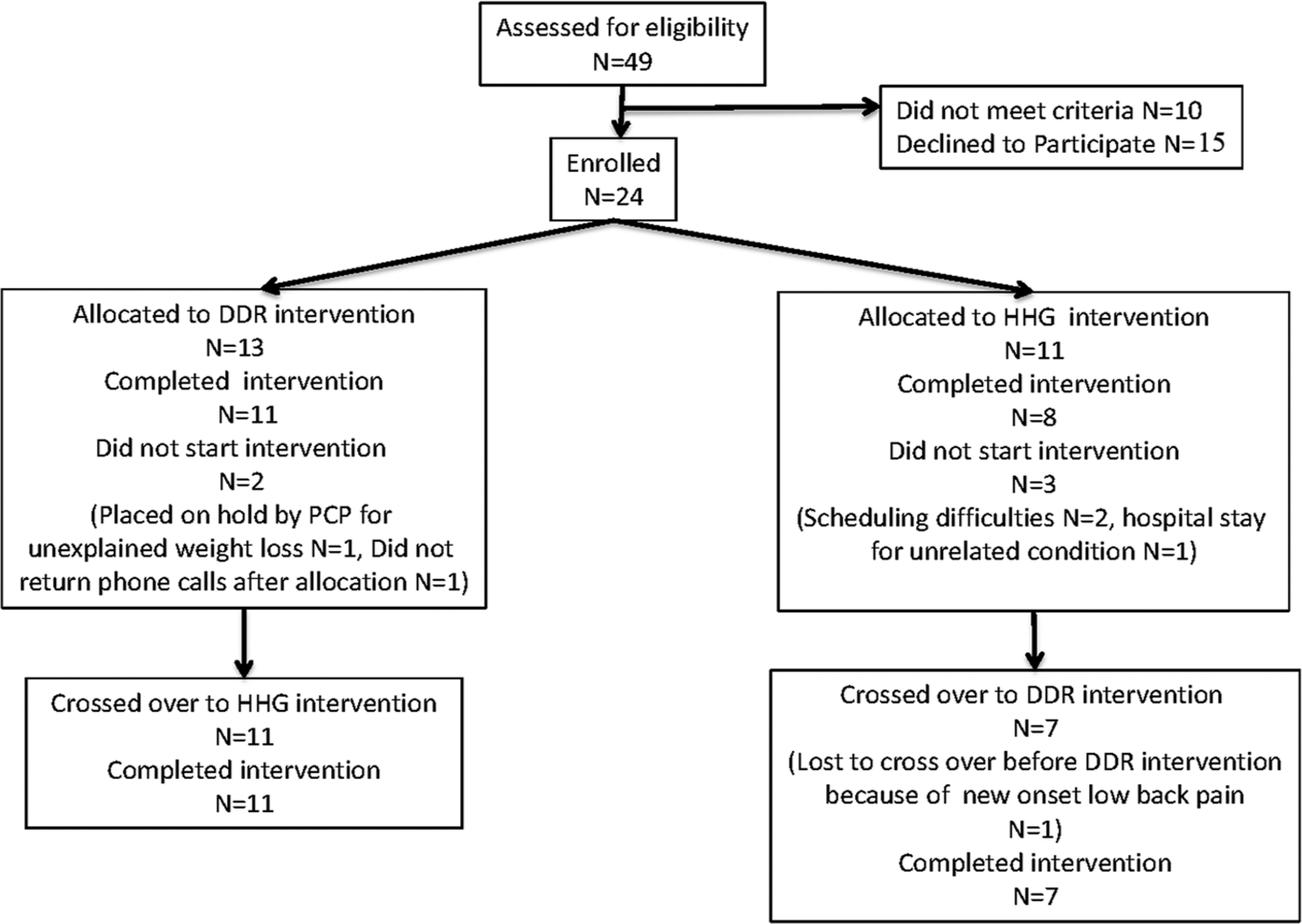
Flow diagram illustrating participant recruitment, treatment allocation, and tracking over the course of the study.
Participant characteristics.
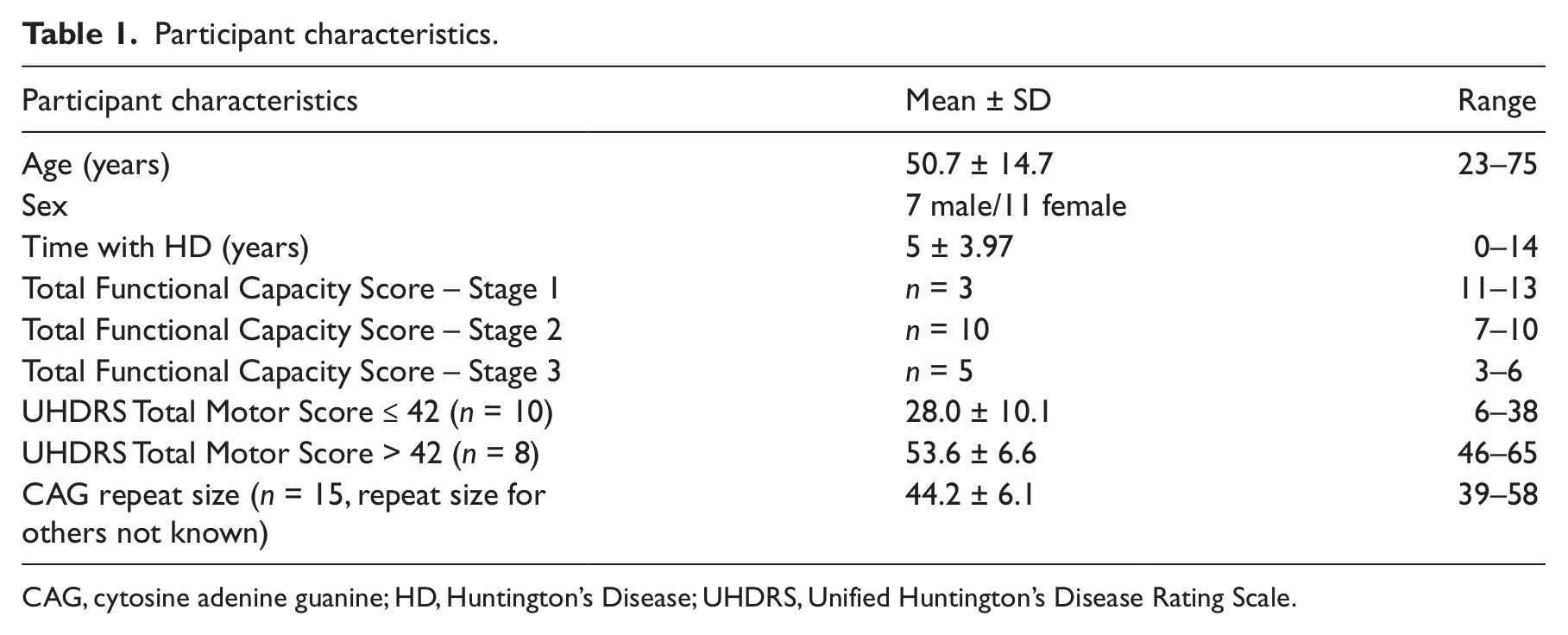
CAG, cytosine adenine guanine; HD, Huntington’s Disease; UHDRS, Unified Huntington’s Disease Rating Scale.
Participants demonstrated significant improvements in mean proportion of correct steps and mean maximum correct combinations from the first two to the last two sessions (Table 2). Most participants initially played the Dance Dance Revolution using song–dance combinations that were categorized as “easy” and game speed was slowed from 1.0 (full speed) to between 0.25 and 0.75 settings. All but the three most severely affected individuals improved to playing the “easy” songs at 75% or full speed. As participants improved their game-play skills, they required less cueing and demonstrated fewer episodes of imbalance. All participants completed 100% of all Dance Dance Revolution and handheld video game sessions.
Dance Dance Revolution game play performance.
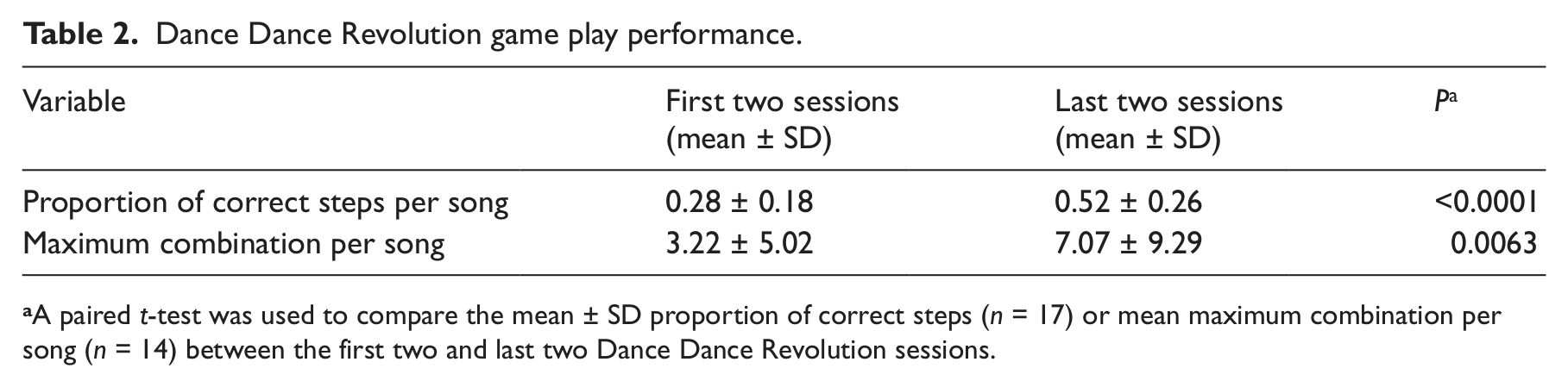
A paired t-test was used to compare the mean ± SD proportion of correct steps (n = 17) or mean maximum combination per song (n = 14) between the first two and last two Dance Dance Revolution sessions.
At the completion of the study, most participants (17/18, 94%) reported that the game was fun, motivating, and more mentally than physically challenging. Participants took few or no rest breaks during game play indicating that the game held their attention and did not overly fatigue them. One person who reported not liking the game stated that the game was not exercise and wanted more current music. The majority (17/18, 94%) of participants reported wanting to continue the game after study completion and we confirmed that four individuals purchased the game.
There were no falls or incidents requiring medical attention related to Dance Dance Revolution game play. Only two participants, with the greatest motor impairments, had loss of balance occurrences that required researcher intervention. Vital signs remained stable and well within acceptable limits per American College of Sports Medicine guidelines 16 for all participants.
GAITRite outcome data was eliminated for one participant who consistently exhibited an abnormal gait during testing sessions on the walkway that did not reflect his usual walking pattern. One participant could not walk backward. Thus, 17 participants were included in the GAITRite analysis (n = 16 for backward condition). No significant changes were seen after the Dance Dance Revolution intervention compared with the handheld video game for velocity (forward, backward, or obstacle conditions) or for stride length, swing percentage, and heel-to-heel base of support (forward and backward) (Table 3). However, significant improvement was observed for double support percentage forward (2.54% reduction, p = 0.03) and backward walking (4.18% reduction, p = 0.01). In evaluating intervention effectiveness depending on severity of motor impairment, a significant interaction was observed for forward heel-to-heel base of support (p = 0.05). Participants with less severe motor symptoms experienced a reduction of 1.01 cm (13.40 versus 14.41, 95% confidence intervals (CIs) for difference: –2.29, 0.27) after the intervention, while those with greater impairments showed an increase of 1.07 cm (11.16 versus 10.09, 95% CIs for difference: –0.51, 2.66). There were no differences between the treatments in forward and backward walking step time, stride length, swing, and double support time coefficients of variation.
Gait and dynamic balance measures.
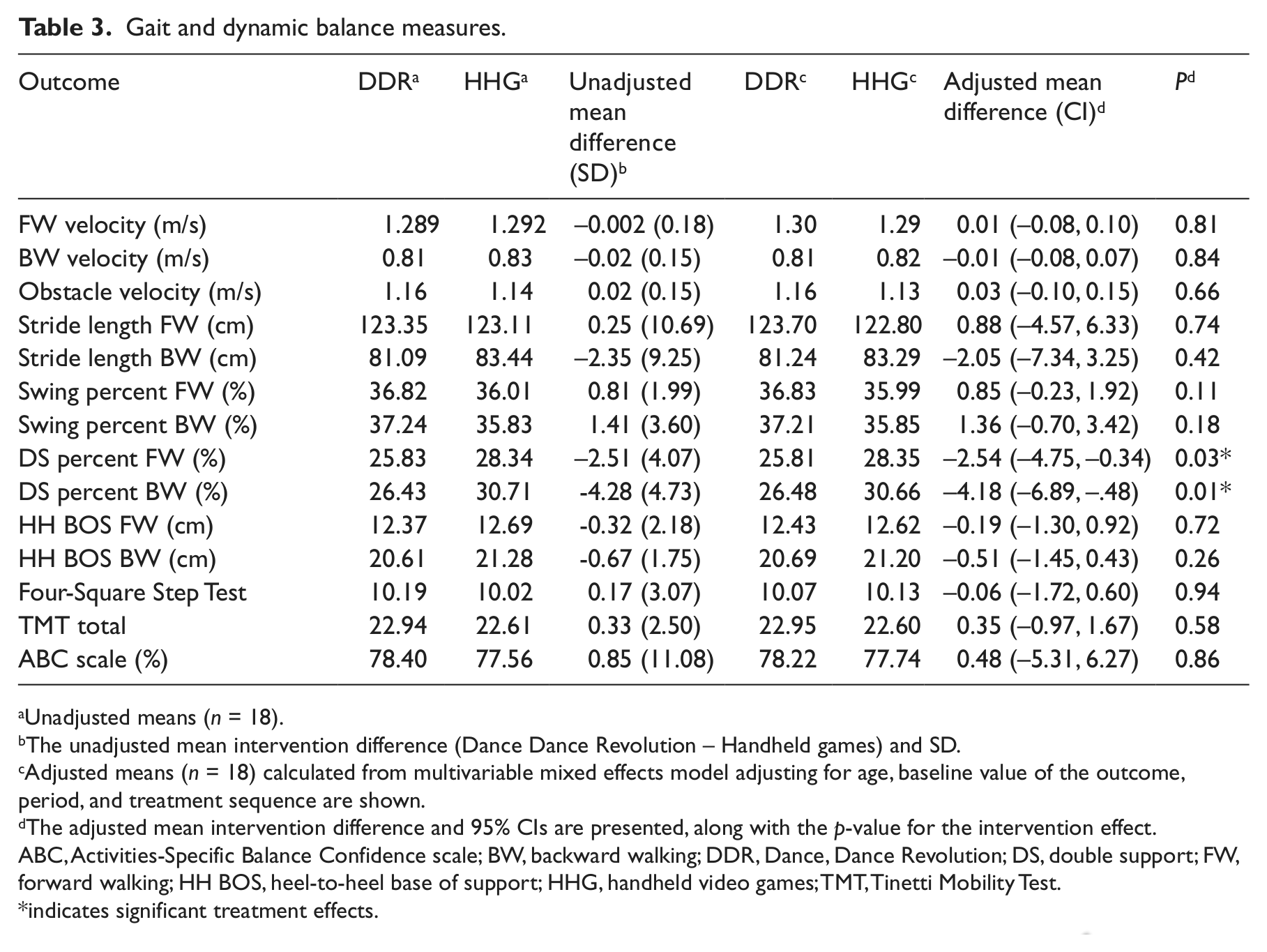
Unadjusted means (n = 18).
The unadjusted mean intervention difference (Dance Dance Revolution – Handheld games) and SD.
Adjusted means (n = 18) calculated from multivariable mixed effects model adjusting for age, baseline value of the outcome, period, and treatment sequence are shown.
The adjusted mean intervention difference and 95% CIs are presented, along with the p-value for the intervention effect.
ABC, Activities-Specific Balance Confidence scale; BW, backward walking; DDR, Dance, Dance Revolution; DS, double support; FW, forward walking; HH BOS, heel-to-heel base of support; HHG, handheld video games; TMT, Tinetti Mobility Test.
indicates significant treatment effects.
Owing to incomplete data, the participant numbers included in analysis of non-gait measures was as follows: 18 for Activities-Specific Balance Confidence Scale and Tinetti Mobility Test, and 17 for the Four-Square Step Test and WHOQOL-Bref. There were no significant treatment effects observed for the Tinetti Mobility Test, Four-Square Step Test, Activities-Specific Balance Confidence Scale, and WHOQOL-Bref between the Dance Dance Revolution and handheld video game interventions, and no significant differential treatment effects by disease severity.
Comparisons of gait and non-gait outcomes by intervention group (Dance Dance Revolution versus handheld games) prior to crossover showed no significant differences (results not shown).
Discussion
This is the first study to use a video game-based exercise treatment in individuals with Huntington’s disease. A supervised exercise intervention using Dance Dance Revolution appears to be feasible, acceptable, and safe in individuals with Huntington’s disease. Most participants improved on game play and the compliance rate was high, indicating that Dance Dance Revolution may be useful as a motivating exercise intervention for this population. The game can be easily performed by individuals with early stage Huntington’s disease at home, but supervision of those with more severe motor impairments to prevent falls is recommended. Following the six-week, twice weekly, home-based Dance Dance Revolution intervention, significant changes were noted in dynamic balance during walking, as measured by double support percentage and those with less severe motor symptoms had reductions in heel-to-heel base of support during forward walking. However, the Dance Dance Revolution intervention, as applied in this six-week study, did not significantly impact functional mobility, balance confidence, or quality of life.
A total of 88% of participants improved their game play performance from first to last sessions. The continuous feedback provided to the participants during game play (e.g. auditory and visual feedback of the word “excellent” when they accurately stepped on a target at the correct time) and summary feedback about how many correct steps and combinations of steps they achieved, may have facilitated motor learning and led to improved game performance. High attention levels, as shown by the participants’ reluctance to stop playing the game for rest breaks and exercise compliance, may also have facilitated motor learning. Participants enjoyed playing Dance Dance Revolution and may have been motivated to perform well through the positive feedback that they received throughout the exercise sessions. Our finding of high attention and compliance with video game-based exercise is supported by previous studies 10,11 and is especially striking given the high level of apathy that is typically found in individuals with Huntington’s disease. Improved Dance Dance Revolution performance may be clinically important since studies have shown that individuals with basal ganglia disorders have difficulty initiating and learning sequences of movements. 30 –33 Studies to test whether video game play might be an effective method to teach complex motor sequences to people with Huntington’s disease could provide useful information to clinicians.
The Dance Dance Revolution game can be safely performed by individuals with Huntington’s disease as demonstrated by the fact that no adverse health changes related to game play occurred. No abnormal heart rate and blood pressure values were recorded in response to Dance Dance Revolution play. In general, individuals with less severe motor impairments were able to play the game without loss of balance occurrences requiring physical assistance to prevent falls, while those with more severe motor impairments required supervision. Based on these findings, we suggest that individuals with Huntington’s disease be evaluated by a physical therapist before starting the game to determine their abilities to play the game safely and to assist with song selection and song speed settings. Individuals at earlier stages of the disease may be able to safely play the game in their homes without supervision, while those with more advanced disease may require direct supervision by a therapist or trained individual to prevent falls.
Following the Dance Dance Revolution exercise intervention, individuals with Huntington’s disease spent significantly less time in double support during forward and backward walking and those with less severe motor symptoms had reductions in their heel-to-heel base of support. Since the time spent with both feet on the ground (double support) and heel-to-heel base of support tends to increase in individuals with poor balance, 34 these findings suggest that the Dance Dance Revolution intervention led to improved dynamic balance during walking. No minimal detectable change values for double support time or heel-to-heel base of support have been published for individuals with Huntington’s disease. However, studies in individuals with stroke 35 and in the elderly 36 have reported between-session forward walking double support time minimal detectable changes of 4.2% and 2.0%, respectively, raising the possibility that the changes produced by the Dance Dance Revolution intervention are real. Repetitive practice of weight shifts and multidirectional stepping at different speeds, and with stops and starts during game play, may have contributed to improved balance. In support of this hypothesis are reported balance and gait improvements following a short duration, intensive tango program with similar dance elements as Dance Dance Revolution in individuals with Parkinson’s disease. 37 Improved balance during walking may have clinical implications, since individuals with Huntington’s disease often fall while performing challenging balance activities (turning, stepping over objects, negotiating stairs, and stepping or walking backward). A new dance-pad stepping test based on Dance Dance Revolution correlated moderately with fall risk measures in elderly individuals. 38 Additional research is needed to determine whether dynamic balance gains with the Dance Dance Revolution intervention translate to fall reductions.
The Dance Dance Revolution intervention did not impact functional mobility as measured by gait velocity and the Tinetti Mobility Test. The lack of improvement in these measures may be related to the fact that Dance Dance Revolution game play did not involve elements measured by these assessment tools (walking, getting up and down from chairs, or turning). Therefore, it is not surprising that there was limited transfer of training to performance on these tests. Participation in a video game-based exercise program, in which participants moved a center-of-pressure position signal to targets, resulted in improved balance but not gait in frail community-dwelling older adults. 39 Practice of Dance Dance Revolution may need to be coupled with functional training for balance gains to improve walking speed and chair transfers. Another explanation is that the Dance Dance Revolution intervention intensity and duration of this study was insufficient to impact functional mobility. In comparison to the 12 sessions of Dance Dance Revolution over six weeks delivered in this study, treatment lengths to improve balance and mobility in other neurological populations were 24–36 sessions over 8–12 weeks. 5,40,41 It is possible that increasing frequency and duration would lead to improved outcomes.
In general, participants with more severe motor impairments did not respond as well to Dance Dance Revolution treatment as those with lesser impairments. One explanation is that more impaired participants were not able to play the game as well and therefore performed fewer step repetitions. Cognitive impairment negatively impacts motor performance and cognitive deficits in some participants may have prevented game play at a level sufficient to effect motor behavior changes. 42 In support of this hypothesis is our finding that individuals with higher Unified Huntington’s Disease Rating Scale motor scores (> 42) tended to have worse performance on the Unified Huntington’s Disease Rating Scale cognitive battery. Alternatively the treatment may have resulted in participants becoming more aware of their deficits and fall risk. As impaired safety awareness is a common problem in Huntington’s Disease, an increased awareness resulting in compensatory measures (widened base of support, slower gait) to reduce fall risk would be a positive finding. Thus, the Dance Dance Revolution treatment may have differing effects on individuals depending on their motor symptom severity.
No differences in the Four-Square Step Test, Activities-Specific Balance Confidence Scale, and WHOQOL-Bref after the Dance Dance Revolution intervention were found. Significance may not have been achieved in the Four-Square Step Test because some participants had difficulty learning the stepping pattern and needed verbal guidance to complete this test accurately. Therefore, test results may reflect cognitive status as well as physical skills in individuals with Huntington’s disease. Cognitive status may also have negatively impacted the ability to accurately complete the Activities-Specific Balance Confidence Scale and WHOQOL-Bref questionnaires, as some participants seemed to perseverate on answers when completing these two measures.
Limitations to this study include the small training dosage and sample size, no randomization process, lack of washout periods between interventions, and lack of information about whether treatment effects transferred to daily activities. Adherence and game performance may have been positively influenced during the Dance Dance Revolution intervention by the one-on-one attention of the researcher coming to the participants’ homes to assist them in game play. The handheld video game sessions were not supervised and therefore the attention received during the handheld video intervention did not match that received during the Dance Dance Revolution intervention. However, a researcher spoke with each participant weekly and participants were encouraged to play the games with family members and friends to help compensate for the lack of supervision. Larger clinical trials that incorporate a social contact control group are needed to determine any specific benefits incurred from attention and social interaction.
Clinical messages
The video game Dance Dance Revolution motivates individuals in early to middle Huntington’s disease to exercise, and is safely performed with appropriate supervision.
A six-week Dance Dance Revolution intervention improved double support percentage during walking, suggesting that a larger randomized two-group study with 45 patients per arm may be warranted.
Footnotes
Acknowledgements
We would like to thank Dr Karen Thomas for study suggestions.
Conflict of interest
The Authors declare that there is no conflict of interest.
Funding
This study was funded by a 2008-2009 HSG/HSC Clinical Research Award from the Huntington Study Group/ Huntington Society of Canada and the Robert A Vaughan Family Fund.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.