
Abstract
Objective:
To evaluate reliability, internal consistency and construct validity of the Posture and Postural Ability Scale for adults with cerebral palsy.
Design:
Psychometric evaluation of a clinical assessment tool.
Setting:
Rehabilitation centres in Sweden and Iceland.
Subjects:
Thirty adults with cerebral palsy aged 19–22 years, six people at each level I–V of the Gross Motor Function Classification System.
Main measures:
The Posture and Postural Ability Scale contains a 7-point ordinal scale for postural ability in supine, prone, sitting and standing, and items for assessment of posture. Posture and postural ability was rated from photos and videos by three independent assessors. Interrater reliability was calculated using weighted kappa. Internal consistency was analysed with Cronbach’s alpha if item deleted and corrected item–total correlation. Construct validity was evaluated based on known groups, using Jonckheere Terpstra for averaged values of the three raters relative to the Gross Motor Function Classification System.
Results:
There was an excellent interrater reliability (kappa = 0.85–0.99) and a high internal consistency (alpha = 0.96–0.97, item–total correlation = 0.60–0.91). Median values differed (P < 0.02) between known groups represented by the levels of gross motor function, showing construct validity for all items.
Conclusion:
The Posture and Postural Ability Scale showed an excellent interrater reliability for experienced raters, a high internal consistency and construct validity. It can detect postural asymmetries in adults with cerebral palsy at all levels of gross motor function.
Introduction
There are few assessment tools for posture and postural ability in lying, sitting and standing for people with severe physical disabilities, and none of them has been evaluated regarding its psychometric properties for adults with cerebral palsy, even though posture is a key problem in adult cerebral palsy. 1
Asymmetric posture is known to cause progressive deformities in immobile people with cerebral palsy due to the effect of gravity.2 –4 However, early detection and preventive treatment can reduce the number of severe contractures, hip dislocations, scoliosis and other fixed deformities.5 –8 As tissue adaptations often occur slowly over time, standardized measurement is crucial to identify the need for treatment and postural support in order to minimize progressive deformities and also to evaluate therapeutic interventions.
The Physical Ability Scale 9 for assessment of postural ability in children with severe disabilities was developed by Noreen Hare during the 1970s and 1980s. This inspired Pountney and co-workers to develop the Chailey Levels of Ability 10 to describe stages of motor development in normal infants and children with motor impairments. Its validity has been evaluated for children and youth with cerebral palsy. 10 These instruments form the basis of the Postural Ability Scale developed by Pauline Pope in the early 1990s 11 to assess both posture and postural ability in people with severe physical disabilities regardless of age and diagnosis. This assessment tool allows postural ability and posture to be assessed separately. It is in clinical use for trained professionals but has not been evaluated for its psychometric properties. During the years 2009–2011, the Postural Ability Scale was developed further by Pope and co-workers (ERB, AA, GJ). The levels of ability were slightly modified and items added to the quality of posture to allow assessment of posture from a sagittal as well as a frontal view. This modified and expanded version. called the Posture and Postural Ability Scale (PPAS) (Table 1), has not previously been tested for reliability or validity.
The Posture and Postural Ability Scale for assessment of postural ability in standing, sitting, supine and prone, followed by assessment of quality of posture in frontal and sagittal view
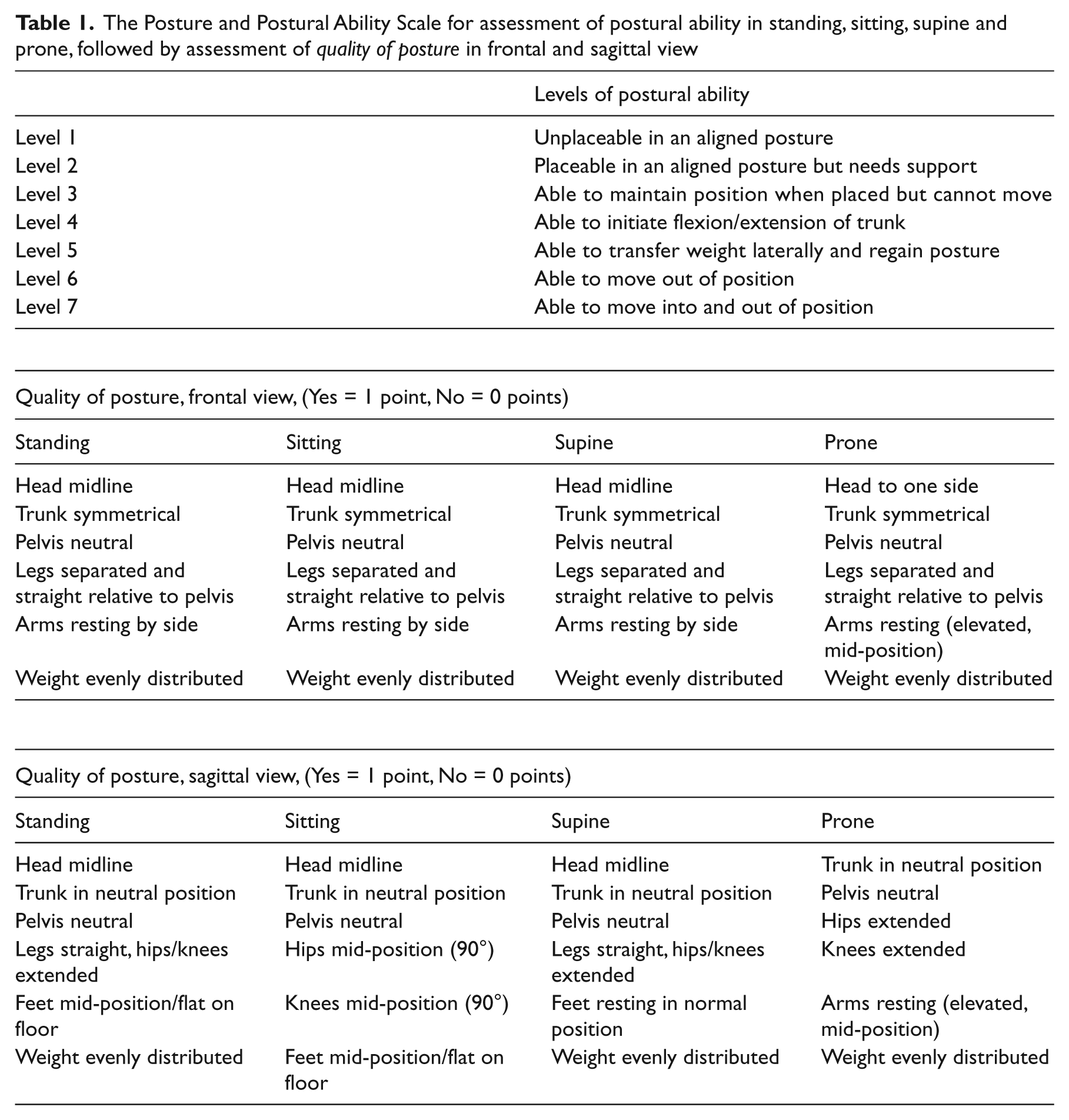
There is no universal definition of posture and postural ability. In this paper, the term ‘posture’, relates to the shape of the body (i.e. the anatomical alignment of the body segments in relation to each other and the supporting surface) and also to the relationship between the body and the environment.11 –13 ‘Postural ability’ refers to the ability to stabilize the body segments relative to each other and to the supporting surface; to get into the most appropriate body configuration for the performance of the particular task and environment. This means control of the centre of gravity relative to the base of support during both static and dynamic conditions.11,12
Our purpose was to evaluate the interrater reliability, internal consistency and construct validity of the Posture and Postural Ability Scale for adults with cerebral palsy.
Methods
Participants were recruited during a project in the south of Sweden in October 2009–October 2010 to expand a National Health Care Program and Quality Register for cerebral palsy,5,6,14 to include adults with cerebral palsy. The subjects who agreed to join the Cerebral Palsy Health Care Program were examined by a physiotherapist and occupational therapist. At the examination the subjects were also asked if they would agree to participate in the psychometric evaluation of the Posture and Postural Ability Scale. All subjects who agreed to participate were included, until six people at each level of the Gross Motor Function Classification System had accepted. One additional client with cerebral palsy was recruited from the Rehabilitation Centre of Excellence in Kópavogur, Iceland. Written consent was collected from all participants or by proxy where the participant was unable to give such consent. Ethical approval for the study was granted by the Medical Research Ethics Committee at Lund University, number 2009/361.
Cerebral palsy was defined according to Rosenbaum et al. 1 Exclusion and inclusion criteria were in accordance with the Surveillance of Cerebral Palsy in Europe (SCPE). 15 People with motor impairment and specific neurological signs (ataxia, dyskinesia and/or spasticity) caused by different genetic syndromes before the age of 2 without progressive brain dysfunction were included. Gross motor function was determined according to the expanded and revised version of the Gross Motor Function Classification System, which comprises five levels I–V. 16 The most severe functional limitation is level V, with difficulties controlling head and trunk posture in most positions, and severely limited or no voluntary control of movement.
Posture and postural ability was recorded by photos and videos of the participants. Photos of habitual posture of each individual were taken from a frontal and sagittal view of the whole body in supine, prone, sitting and standing position. Habitual refers to the posture customarily adopted by the individual when instructed to sit, stand or lay down in prone or supine as straight as possible or the posture the body assumes when placed as straight as possible in any of these positions and allowed to settle. The positions were: supine lying on a plinth with arms resting by side; prone lying on a plinth with the head to one side and arms resting in an elevated position (flexion in elbows and abduction, external rotation of shoulders); sitting on a plinth with feet on the floor; standing on the floor. Those who were unable to maintain position independently were provided the manual support needed to stay in position. People who required total body support in standing, such as those classified gross motor function level V, were assessed in a standing brace or on a tilt table. Videos recorded the participants’ postural ability, from the lateral view of the plinth, while instructed to assume and get out of the four positions. If unable to do this they were placed in each position. Assessment of ability was then carried out sequentially corresponding to the points on the Posture and Postural Ability Scale (Table 1).
The Posture and Postural Ability Scale contains a 7-point ordinal scale for the assessment of postural ability in standing, sitting, supine and prone and six items for assessment of quality of posture in the frontal plane and another six items in the sagittal plane (Table 1). Postural symmetry and alignment gives 1 point for each item while asymmetry or deviation from midline gives 0 points. The total score of 0–6 points is calculated separately for each position in the frontal and sagittal plane. Postural ability is rated according to the ordinal scale ranging from unplaceable (level 1) to able to move into and out of position (level 7). The two lower levels of postural ability are in fact a rating of no ability, that is, they are unable to maintain or change position by themselves. The difference between those two levels is whether the person can (level 2) or cannot (level 1) conform to the position when placed by another person (i.e in anatomical alignment when supported). When a person cannot be placed in prone and standing due to hip dislocation or severe contractures, especially of the hip flexors, postural ability is scored as level 1 = unplaceable and posture is scored 0.
Postures and postural abilities of the 30 subjects were assessed from the photos and videos during February 2012 by three experienced physiotherapists independently using the Posture and Postural Ability Scale.
Statistical analysis
Interrater reliability for three independent raters was calculated using weighted kappa scores which takes the degree of disagreement into account. 17 The magnitude of weighted kappa indicates the agreement beyond chance and was interpreted according to the method of Fleiss, 18 where ≤0.40 signifies poor agreement, 0.40–0.75 fair to good agreement and ≥0.75 signifies excellent agreement. The internal consistency of the assessment tool was evaluated through ‘Cronbach’s alpha if item is deleted’ and ‘corrected item–total correlation’ based on averaged values for the three raters. Cronbach’s alpha if item is deleted corresponds to the value achieved if a specific item is removed. 19 The corrected item–total correlation shows the correlation between each item and the total score of the measurement and any item with a value <0.2 should be discarded. 19 For analysis of reliability and consistency all levels of the Gross Motor Function Classification System were combined and 95% non-parametric bootstrap confidence intervals were added based on 1000 re-samples.20,21 Construct validity was evaluated for known groups based on the five levels of gross motor function with median and range. Jonckheere-Terpstra was used for analysis of arithmetic average values given by the raters, and P-values <0.05 were considered significant. The alternative hypothesis of the test is that median values of the scores decrease with decreasing gross motor function. For all statistical computing, R software environment was used.
Results
Postures and postural abilities of 30 adults (15 males, 15 females) with cerebral palsy born 1988–1991 (age range 19–22) were recorded with photos and videos during October 2009–October 2010. The scores varied between participants at different levels of the Gross Motor Function Classification System, with decreasing values at lower levels of gross motor function such as level IV and V. The distribution of scores across the 30 participants were described as median, mean, standard deviation, min, max values, 25th and 75th percentile in all four positions (Table 2). Since every person was assessed by three raters, each missing assessment (photo/position) generated three missing values (Table 2).
Scores for the Posture and Postural Ability Scale across the 30 participants
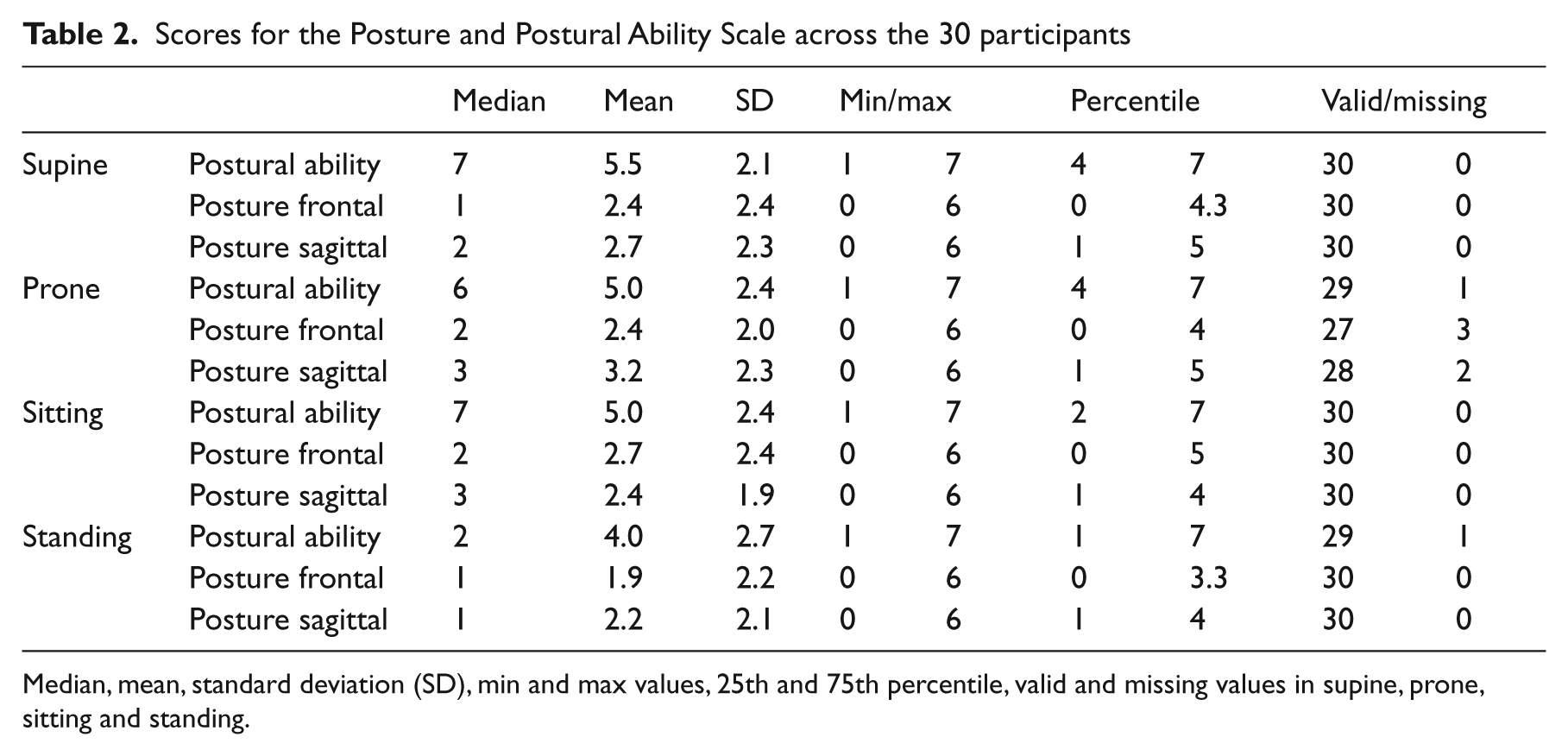
Median, mean, standard deviation (SD), min and max values, 25th and 75th percentile, valid and missing values in supine, prone, sitting and standing.
The Posture and Postural Ability Scale showed excellent interrater reliability for the three independent raters with weighted kappa values of 0.85–0.99 (Table 3). There was a high internal consistency for the Posture and Postural Ability Scale for all items (Table 4). Cronbach’s alpha if item deleted was 0.97 for sitting posture sagittal and 0.96 for all other items with a 95% confidence interval of 0.93–0.98 for all items. Corrected item–total correlation varied between 0.60 and 0.91 with the lowest correlation for sitting posture in the sagittal view.
Interrater reliability of the Posture and Postural Ability Scale
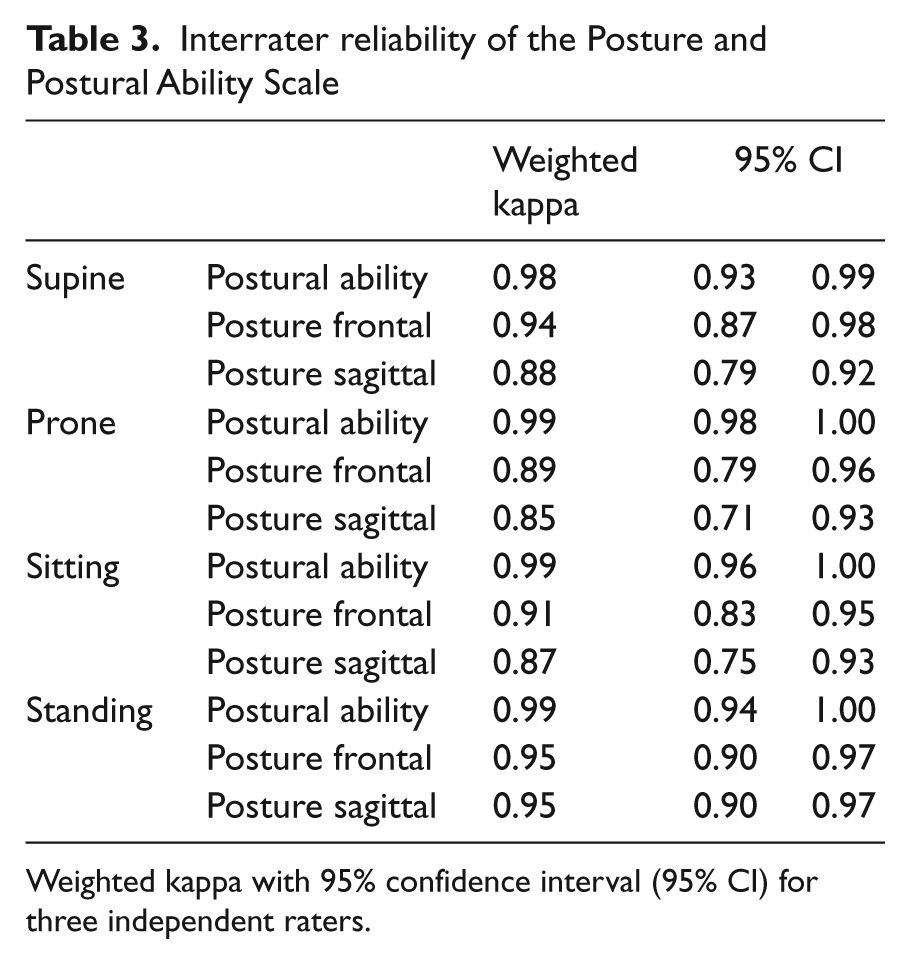
Weighted kappa with 95% confidence interval (95% CI) for three independent raters.
Internal consistency of the Posture and Postural Ability Scale
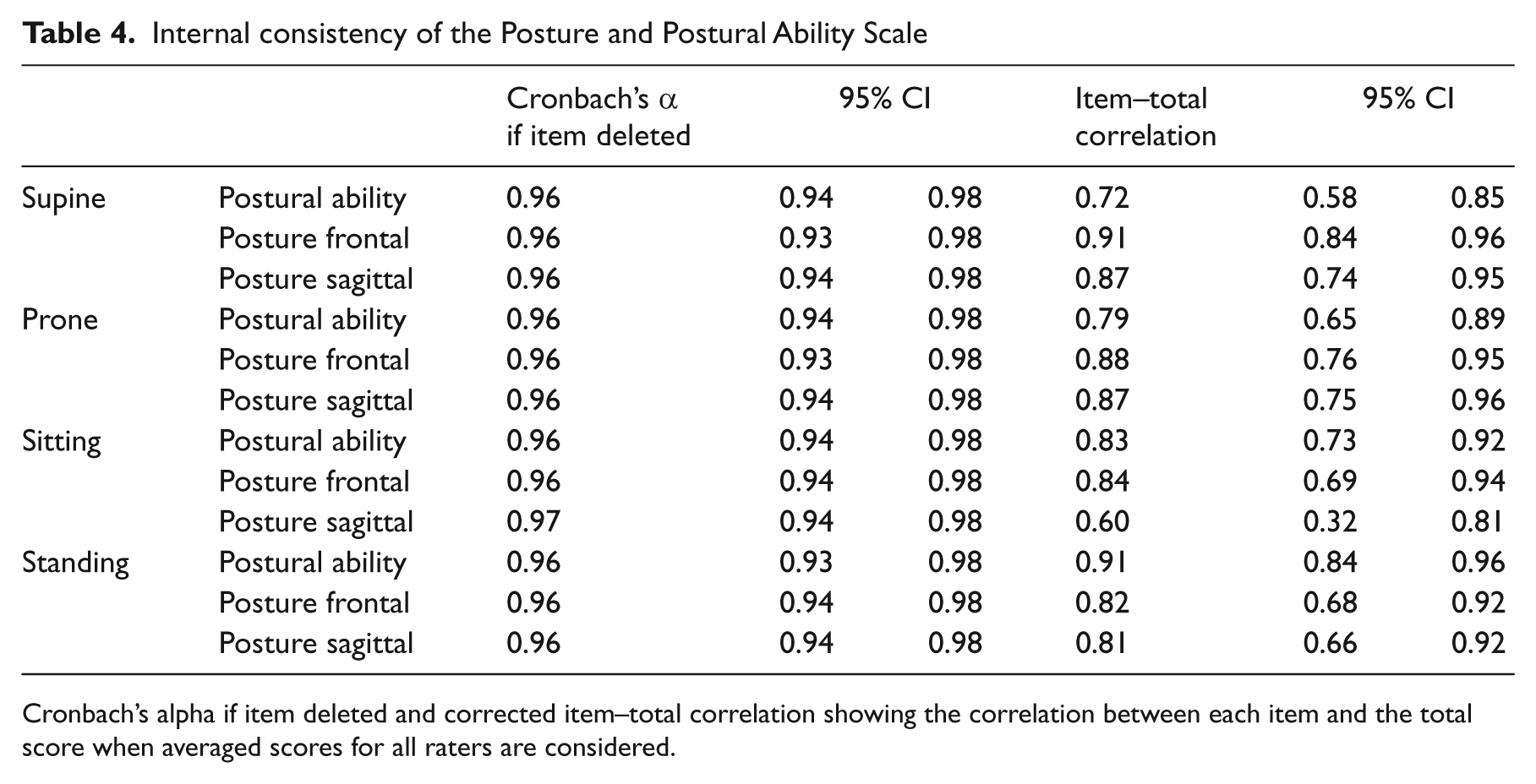
Cronbach’s alpha if item deleted and corrected item–total correlation showing the correlation between each item and the total score when averaged scores for all raters are considered.
The Posture and Postural Ability Scale showed construct validity based on the ability of the assessment tool to differ between known groups represented by the gross motor function levels I–V (Table 5, Figure 1 online). Median values and range in terms of min and max values are presented together with P-values (P < 0.02) calculated with Jonckheere-Terpstra for averaged values (Table 5). Distribution of scores at each level of gross motor function in all four positions is provided for all three raters (Figure 1 online). The Posture and Postural Ability Scale could not identify differences in postural ability between individuals at levels I–II but was able to detect postural asymmetries at all levels.
Construct validity of the Posture and Postural Ability Scale
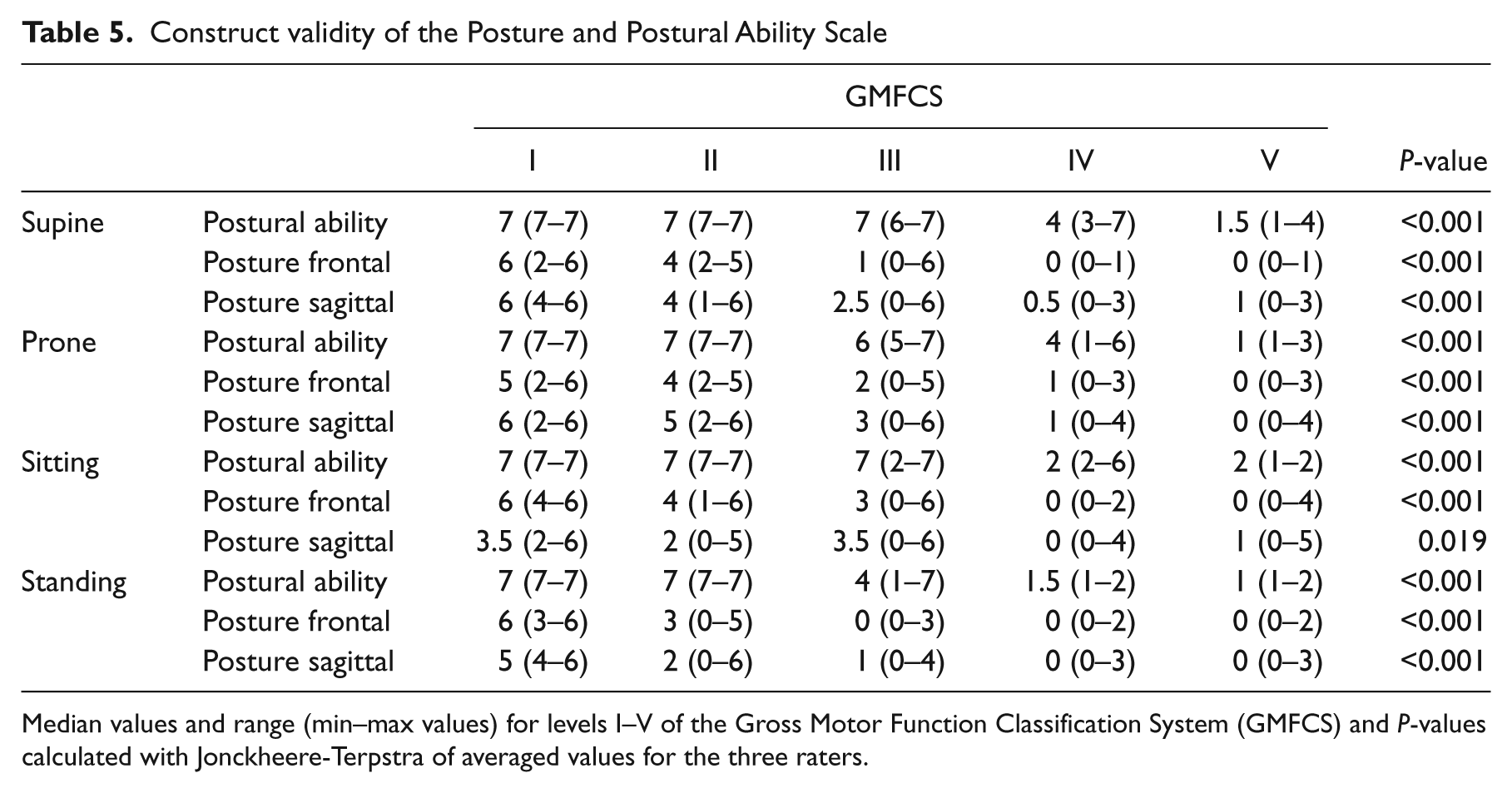
Median values and range (min–max values) for levels I–V of the Gross Motor Function Classification System (GMFCS) and P-values calculated with Jonckheere-Terpstra of averaged values for the three raters.
Discussion
The Posture and Postural Ability Scale showed an excellent interrater reliability, a high internal consistency and good construct validity for adults with cerebral palsy. This is, to our knowledge, the first study evaluating an assessment tool for posture and postural ability in lying, sitting and standing position for adults.
A limitation of the study is that all three raters participated in the development of the Posture and Postural Ability Scale; they have long clinical experience and are specialized in posture management. Further research is needed to examine interrater reliability for trained practitioners not involved in the modification of the assessment tool. A further limitation is that the ratings were based on photos and videos. This removes some variability that arises in clinical practice. Photos provide reflection of the posture at just one point in time. However, the condition of people with severe disabilities may alter during the day due to fatigue, pain, etc. It may also change over time, making a measurement on different occasions such as test–retest and intrarater reliability more difficult to interpret. Therefore we chose to evaluate agreement between different raters and used photos and videos to standardize the occasion and minimize disagreement due to different performances and circumstances.
Internal consistency represents the average of the correlations among all items. The scale demonstrated a high internal consistency for all items, where Cronbach’s alpha if item deleted was 0.96–0.97, which exceeds the 0.8 recommended by Streiner and Norman. 19 Corrected item–total correlation showed a slightly lower value for sitting posture in the sagittal view compared to the other items. This is probably explained by the fact that the height of the plinth was not optimal in some photos, which affected the ratings of hips and knees mid-position. An adjustable plinth is not always available in clinical practice. If the plinth is not adjustable or if using a chair, it would be best to provide additional support for the feet when needed.
Construct validity was evaluated through its ability to differ between known groups in terms of the gross motor function levels in cerebral palsy. The expanded and revised version of the Gross Motor Classification System has been developed for children with cerebral palsy with the oldest age band 12–18 years, but some studies have shown validity and reliability for use of this classification in adults with cerebral palsy as well.22 –24 According to this classification, individuals at levels I and II can walk and stand unsupported. The highest level of the Posture and Postural Ability Scale is to move into and out of position and therefore the assessment tool was not expected to differ between gross motor function levels I and II in postural ability. The distribution of individuals at maximum and minimum score showed an anticipated ceiling effect for postural ability in all four positions for adults at level I–II, while the floor effect was higher for posture, indicating a better quantity in terms of ability than quality of posture. This indicates a need for assessing posture and postural ability separately and as distinct from gross motor function, in order to detect postural asymmetries and identify need for postural support. A strength of the Posture and Postural Ability Scale is that it identified postural asymmetries and deviations at all levels of gross motor function in this study of adults with cerebral palsy.
The Posture and Postural Ability Scale was sensitive to detect small postural asymmetries and deviations and is likely to detect postural asymmetries at an early stage. The assessment tool has no grading and cannot differ between a mild, moderate or severe deviation. The rationale is that any deviation will increase by forces imposed by gravity so it is clinically relevant to detect asymmetric posture early in order to apply the appropriate intervention to minimize progressive deformities.
The Posture and Postural Ability Scale does not require any special equipment and is easy to use in a clinical setting. It provides important information of the need for postural support and where it needs to be applied. Although the instrument has been used in clinical practice for different client groups, further research to evaluate its psychometric properties for people with diagnoses other than cerebral palsy is desirable. All assessment tools for posture and postural ability currently used in clinical practice require additional training of the professional intending to use them.
In conclusion, the Posture and Postural Ability Scale shows an excellent interrater reliability for experienced raters, a high internal consistency and good construct validity. It can detect postural asymmetries at all levels of gross motor function in adults with cerebral palsy. The results show an anticipated ceiling effect for postural ability at gross motor function level I–II. Further research is needed to examine interrater reliability for trained professionals not involved with modification of the assessment tool, as well as its application to other client groups.
Clinical messages
This evaluation is based on photos and videos of posture and postural ability in adults with cerebral palsy.
The Posture and Postural Ability Scale shows excellent interrater reliability, high internal consistency and construct validity.
It can detect postural asymmetries at all levels of gross motor function in adults with cerebral palsy.
Footnotes
Acknowledgements
The authors would like to thank Pauline Pope, London, for her endless work and support in developing and modifying the PPAS and for proof-reading the manuscript.
Authors’ contributions
ERB designed the study, developed the instrument, collected the data, rated the subjects, analysed the results and wrote the manuscript. AA and GJ developed the instrument, rated the subjects and revised the manuscript. TC made the statistical calculations, analysed the data, provided the dot plots and revised the manuscript. ACJ revised the manuscript. GH designed the study and actively improved and revised the manuscript. All authors approved the final draft.
Conflict of interest
The authors declare that they have no conflicts of interests.
Funding
This study was supported by the Faculty of Medicine, Lund University, Stiftelsen för bistånd åt rörelsehindrade i Skåne, the Linnea and Josef Carlsson Foundation and the Norrbacka Eugenia Foundation.