
Abstract
This series of articles for rehabilitation in practice aims to cover a knowledge element of the rehabilitation medicine curriculum. Nevertheless they are intended to be of interest to a multidisciplinary audience. The competency addressed in this article is ‘An understanding of the different international models for funding of health care services and casemix systems, as exemplified by those in the US, Australia and the UK.’
Introduction
Health systems around the world are increasingly moving towards payment systems based on a fixed tariff structure for each episode of treatment. The rationale for this approach is to drive up efficiency and to contain costs. 1 – 3 The challenge, however, is to develop a casemix classification which adequately accounts for case complexity (i.e. the differential costs of treating patients with different levels of need), and also commissioning currencies that provide equitable risk-sharing between the purchaser and provider. 3
The term ‘casemix’ is used variously to describe the type of mix of patients treated, 4 in terms of prognosis or resources, depending on the parameter of interest. In the context of healthcare funding models, ‘casemix’ systems classify people into groups that are homogeneous in their use of resources, but a good casemix system also gives meaningful clinical descriptions of these individuals. 5
Casemix information has several uses – it can provide the basis for reimbursement, and also for comparing facilities or programmes, practice patterns and patient outcomes. Casemix information is collected as a standard minimum dataset and, depending on the content of the dataset, it may also be used to benchmark quality and efficiency and for internal management purposes. As well as informing resource allocation, it therefore serves as an information tool that allows policy makers to understand the nature and complexity of healthcare delivery. 4
The aims of this review are (a) to provide an overview of the development of casemix in rehabilitation, (b) to describe the key characteristics of some well-established casemix and payment models in operation around the world and (c)to explore the lessons that may be learned from them and opportunities for future development towards improved models.
Methods
This article provides an educational narrative review, as opposed to a formal systematic review. In order to draw on the relevant literature, we conducted a broad-based search of the major databases (MEDLINE 1950–November 2010 and EMBASE 1980–November 2010) using ‘rehabilitation’ in combination with ‘casemix’ and ‘payment systems’ and related terms. We also searched the internet and used our combined knowledge of the various systems and key authors to expand the reference base.
The language of casemix is full of acronyms that can be confusing for clinicians, but those who wish to explore the literature further will need to be familiar with them. As a service to our readers, we have deliberately included the most commonly used acronyms in this article and a glossary with definitions is provided Appendix 1.
Development of casemix and commissioning currencies
Casemix classification was first pioneered in the United States of America some 40 years ago, 6 and Medicare introduced a ‘Prospective Payment System’ for short-stay acute care hospitals in 1983. The system was based on diagnosis related groups (DRGs), which were designed to measure and classify healthcare activity, based primarily on the diagnosis and the procedures carried out. 7 Each DRG was assigned a ‘fixed tariff’ payment, as patients within each category were considered to be clinically similar and therefore expected to use the same level of hospital resources. Other countries that have since followed on similar lines to introduce DRG-equivalent systems include Australia, Canada, the Nordic countries and several European countries, including Italy, Germany, Hungary and Denmark. 8
The options for commissioning currencies range from a single fixed tariff payment for each episode, regardless of length of stay (‘episode rates’), to payment at a daily rate (‘bed-day’ or ‘per diem’ rates). Both systems present potential opportunities for gaming. Fixed episode payments tend to place the greater share of risk on the provider, and may encourage them to ‘cream-skim’ the easy cases and to discharge too early. Per diem payments may contain insufficient incentives to move the patient on, and so result in unnecessarily long admissions. 3
The principal argument for episode payments is that the majority of the active treatment costs are incurred during the early part of the episode – longer staying patients mainly incurring only ‘hotel costs’ due to largely avoidable delays – so restriction of payment to within a few days either side of the average length of stay provides an incentive towards efficient case throughput. However, while this may be true for acute medical and surgical treatments, it does not necessarily hold good for other areas of healthcare. Figure 1 shows a schematic diagram of the typical cost per day of different types of inpatient episode. In surgical and acute episodes, the majority of the costs are incurred within the first few days as expected, and tail off sharply thereafter. However, in palliative care the daily costs of care rise progressively towards death, while in rehabilitation the cost curve is largely flat – nursing, care and therapy inputs continuing at a similar level throughout the admission. Different payment models are therefore required for these longer term service areas.
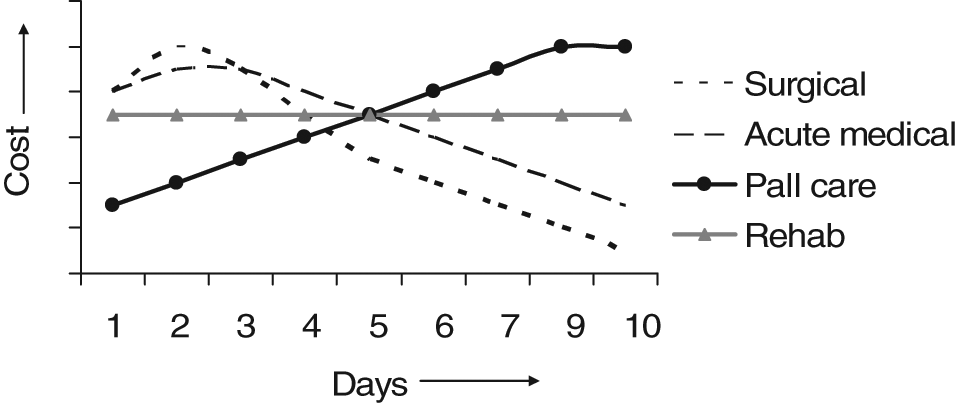
A schematic diagram of cost per day for different types of inpatient episode. In surgical and acute episodes, the majority of the costs are incurred within the first few days and tail off sharply thereafter. In palliative care the daily costs of care rise progressively towards death, while in rehabilitation the cost curve is largely flat. (Reproduced with permission from Prof Kathy Eagar. Australasian Rehabilitation Outcomes Centre (AROC). Data are derived from the Australian National Sub-Acute and Non-Acute Patient Classification System (AN-SNAP) Study 10 ).
Casemix in rehabilitation – international models
Rehabilitation poses some particular challenges for the development of casemix design:
Diagnosis alone is a relatively poor indicator of costs for inpatient rehabilitation, 9,10 where nursing and therapy staff input (as opposed to medical treatments) are the major cost-indicators. 11–13
Cost-efficiency does not always equate with shorter stay. Evidence from the United States and other countries has shown that the introduction of fixed episode payment schemes in rehabilitation may lead to poorer functional outcomes 14 and increased rates of discharge to institutional care, 15 due to pressure for early discharge when reimbursement ceases.
Some patients need longer to achieve maximal independence, but there is also evidence that the resulting savings in the cost of ongoing care can offset the initial investment in rehabilitation by several fold. 16,17
As a result, some healthcare systems have recognized that rigid episode-based reimbursement may be unsuitable for rehabilitation and alternative casemix and payment models are required which are fair to both purchasers and providers and still reward efficiency. Italy has explored a system that links reimbursement to effective stay 18,19 based on the time to reach peak improvement for different groups of conditions, while Australia has developed a ‘weighted blended payment model’ for rehabilitation, which applies a mixture of episode and per diem rates (described in more detail below).
The American system
When the US casemix system was first introduced in the 1980s, medical rehabilitation was excluded from the US-DRGs because it was recognized that rehabilitation inpatients could not be classified reliably by diagnosis alone. 20 The level of functional dependency was considered to be a better cost- indicator, and in the 1990s a classification system based on function (as defined by the Functional Independence Measure (FIM) 21 ) was developed instead. 22 This system of ‘FIM-function-related groups’ (FRGs) was subsequently rederived to predict total rehabilitation costs and renamed ‘casemix groups’ (CMGs). These form the current basis for reimbursement by Medicare for inpatient rehabilitation 3 in the United States.
The In-patient Rehabilitation Facility Prospective Payment System (IRF-PPS) uses a complex casemix classification which is summarized concisely in a recent review by Richard Zorowitz. 2 Each patient is assigned into one of 85 impairment codes, in 21 rehabilitation impairment categories. These are further broken down into casemix groups, based on the FIM-motor score on admission – and in some instances also the FIM-cognitive score and age of the patient, where these are required to provide further definition of costs. Each casemix group also has four levels of comorbidity that represent the presence or absence of medical conditions (e.g. hypertension, diabetes, etc.) and/or complications (e.g. tracheostomy).
Medicare also requires completion of a standardized data set consisting of diagnostic and demographic information (the In-patient Rehabilitation Facility Patient Assessment Instrument (IRF-PAI)) to be completed for each patient within 72 hours of admission, in order to qualify for reimbursement. The FIM is embedded in this tool. Further information may be obtained from the Center for Medicare and Medicaid Services website (www.cms.gov/InpatientRehabFacPPS/).
The Australian System
Development of casemix in Australia followed a broadly similar pattern to that in the United States. Casemix funding for healthcare was first introduced in the state of Victoria in 1993/4, and since then most states have moved towards either casemix-based funding or using casemix to inform the commissioning and budget-setting process. 23 When Australian National Diagnosis-Related Groups (AN-DRGs) were introduced, it was similarly recognized that the costs of subacute care (including rehabilitation medicine, palliative care, psychogeriatric and elderly care evaluation) were not well described by this system. 10 . As in the United States, function-related groups were identified as a better way to determine the differential cost of rehabilitation episodes. 24
Two separate function-related casemix systems have been developed to classify patient episodes for different levels of reimbursement for rehabilitation. The first, published in 1996, is the CRAFT system (Casemix Rehabilitation And Funding Tree), which is based on 12 functional categories determined by the modified Barthel Index. 25 The second, published three years later, is the Australian National Sub-Acute and Non-Acute Patient (AN-SNAP) Classification, which is based on the FIM. 26 Both systems include formal designation of services into level 1 and level 2, on the basis of set criteria for staffing and expertise.
The AN-SNAP classification is the more sophisticated of the two systems, and has now been taken up more widely across Australia and New Zealand, although states vary in the extent to which it is actually used for payment, or simply to provide information. The CRAFT classification is still used for the funding of general (but not specialized) rehabilitation units in the state of Victoria, but the AN-SNAP classification is being adopted by the Australian government in its new national casemix funding model to be progressively introduced from 2011.
The first version of the AN-SNAP classification for inpatient rehabilitation was developed in 1999 following analysis of 7397 case episodes. 26 It comprised 32 classes based on 10 principal ‘impairment categories’, subdivided by the FIM-motor subscale – and, in some categories, further subdivided by the FIM-cognitive scale and age. The latest version (AN-SNAP-II) (2006) was developed on analysis of 84 210 case episodes from 120 public and private rehabilitation units. 27 This version uses the same variables, but there are now a total of 45 classes. The classes for the impairment categories of ‘stroke’ and ‘brain dysfunction’ are provided as examples in Table 1. Further information may be obtained from the Australasian Rehabilitation Outcomes Centre (AROC) website (http://chsd.uow.edu.au/aroc).
The AN-SNAP-II casemix classification for stroke and brain injury
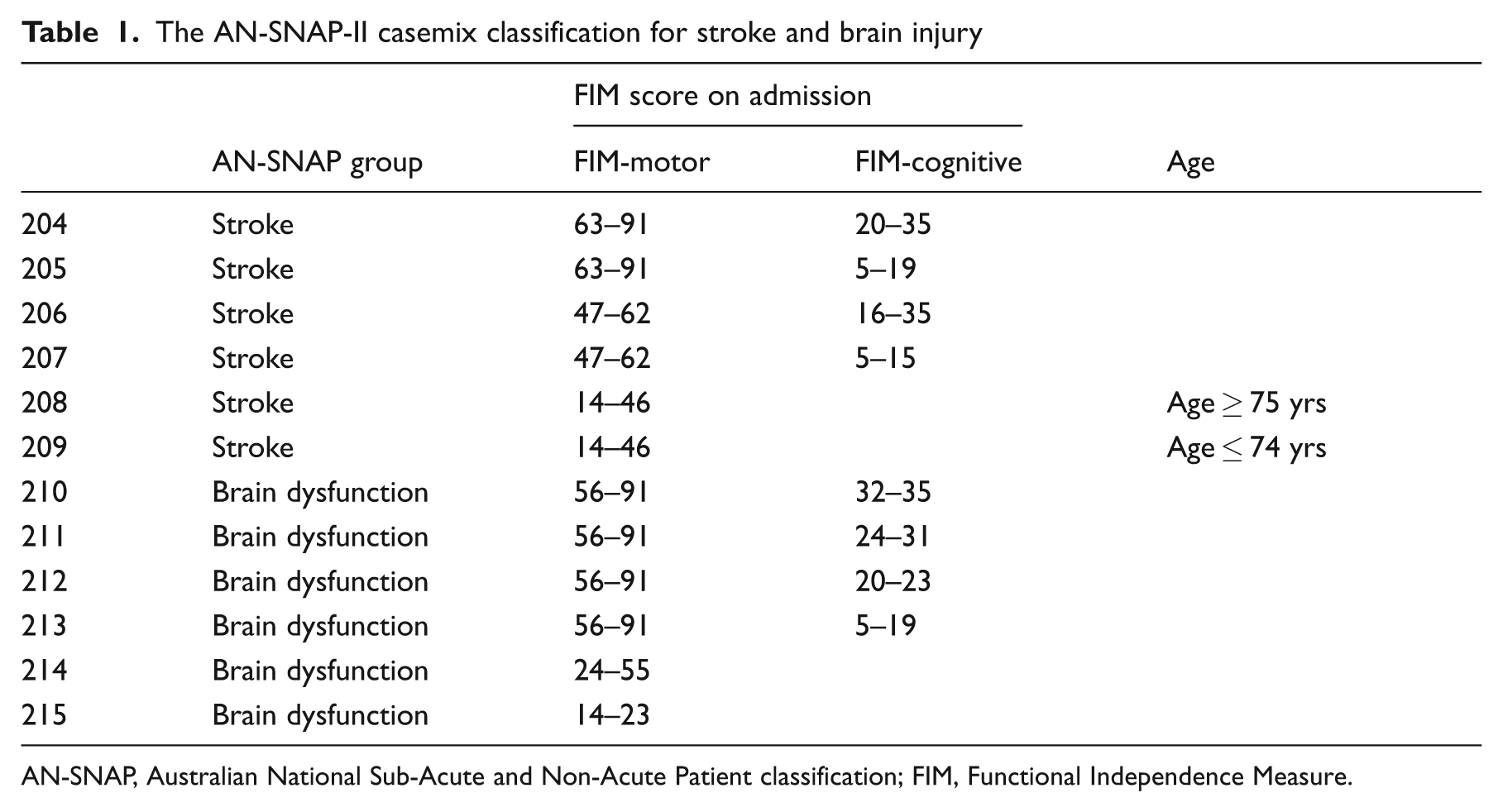
AN-SNAP, Australian National Sub-Acute and Non-Acute Patient classification; FIM, Functional Independence Measure.
While the AN-SNAP classification was originally developed as an episode classification, a more sophisticated ‘blended payment model’ for funding was subsequently developed, which is illustrated in Figure 2. Episode and per diem cost weights are derived from analysis of resource use within each of the AN-SNAP classes. 27 The model is designed to provide incentive to move patients on (as bringing in a new patient will attract a new episode weight), but still provides payment above simple hotel costs for longer episodes.
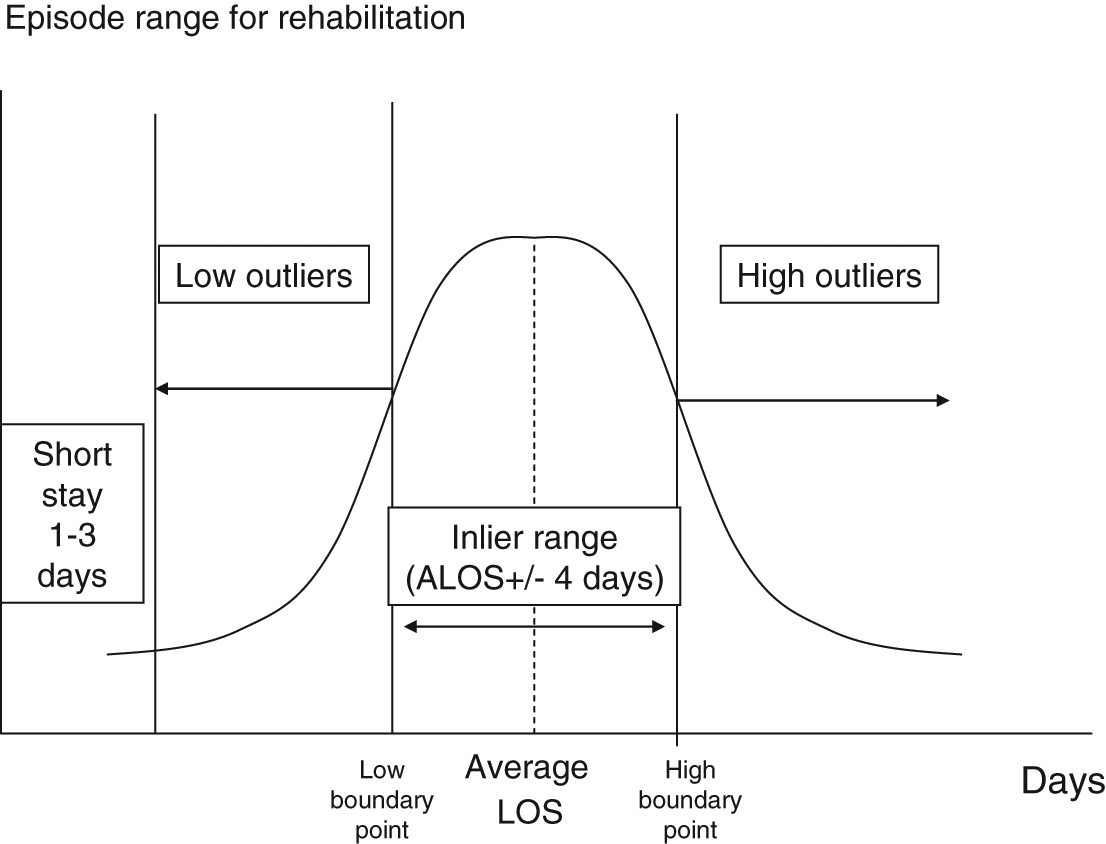
A blended payment model. Patients staying for very short admissions are reimbursed at a standard short-stay rate. Those below the low trim point are reimbursed at the ‘low outlier’ per diem rate. Those with lengths of stay (LOS) within the episode range attract the weighted episode rate plus an ‘inlier per diem’ payment for each day. Those staying beyond the episode period attract the episode rate plus inlier per diem payment for the whole episode period, plus the days beyond the high trim point at the outlier per diem rate. ALOS, average length of stay.
In addition, a 90-day business rule is applied so that, for patients still requiring inpatient rehabilitation beyond 90 days, the episode can be terminated and a new one started following clinical review. 27 The blended payment model has significant advantages over the more rigid US prospective payment system, as it provides flexibility for longer stay rehabilitation programmes, where clinicians and commissioners agree that these are required.
The InterRAI network
The InterRAI network is an international collaborative group of researchers in over 30 countries developing casemix systems in areas of healthcare for persons who are elderly, frail or disabled. The network is not linked to any particular healthcare system or payment model, but has developed a family of instruments with the aim of providing a common language that will produce integrated healthcare information across a range of settings and across international borders.
The best known of the InterRAI casemix systems is the Resource Utilization Groups (RUG-III) which is used in institutional long-term care settings and skilled nursing facilities in the United States and Canada. The current version (5.12) of the RUG-III 28 system uses 108 variables to create either 44 or 34 categories of patients with homogeneous resource patterns (Table 2). The 44-group model comprises seven main clinical groups devised as a hierarchy. Patients are assigned to each group on the basis of clinical characteristics, and each group is divided further by an activities of daily living score. The special rehabilitation group is further divided into five levels of intensity of intervention, while patients with impaired cognition or behavioural problems are categorized on the basis of a nursing rehabilitation score. The RUG-III algorithm explains about 55% of variance in resource use for direct patient care in nursing home residents, 29 and it has been validated in a number of countries through a series of international studies. 30–32 Further information may be obtained from the interRAI website (www.interrai.org).
The 44-group Resource Utilization Group (RUG-III) casemix classification model
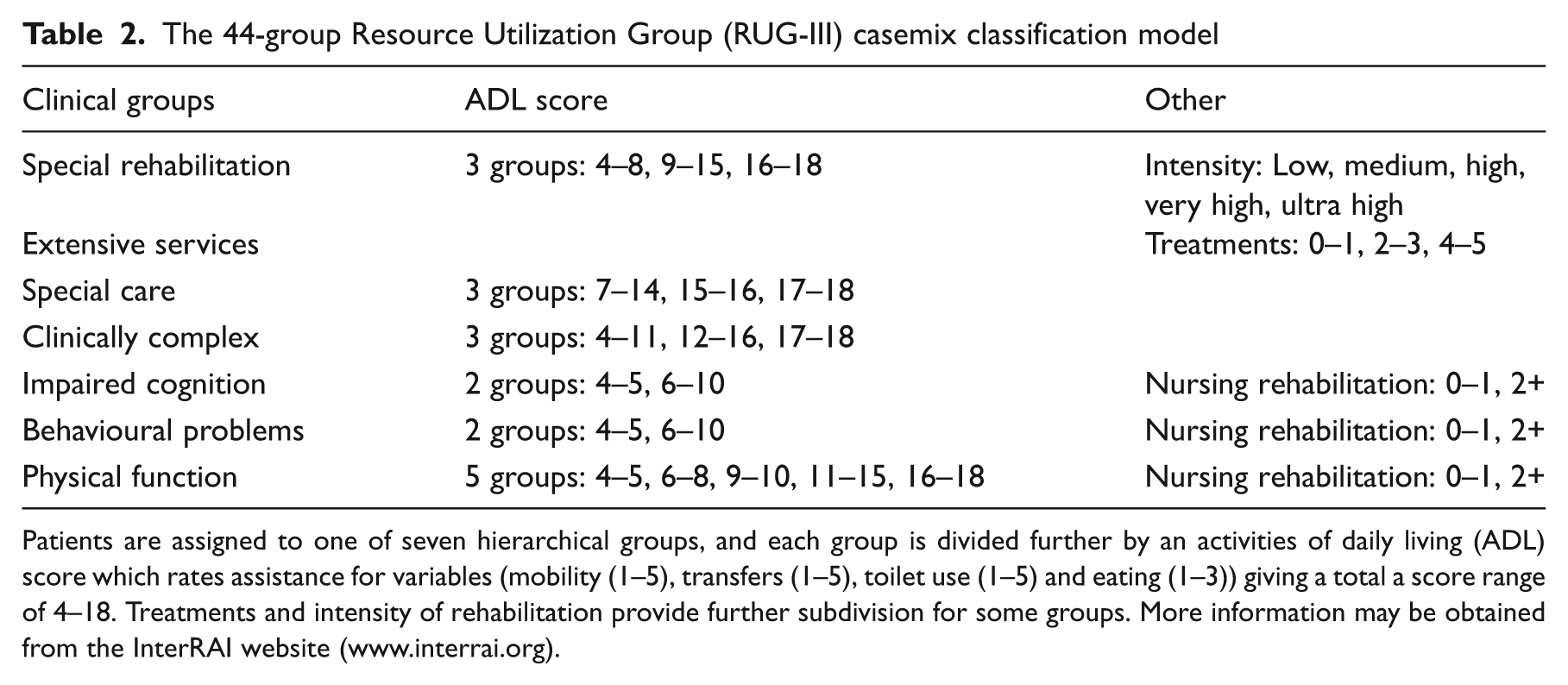
Patients are assigned to one of seven hierarchical groups, and each group is divided further by an activities of daily living (ADL) scorewhich rates assistance for variables (mobility (1–5), transfers (1–5), toilet use (1–5) and eating (1–3)) giving a total a score range of 4–18. Treatments and intensity of rehabilitation provide further subdivision for some groups. More information may be obtained from the InterRAI website (www.interrai.org).
In all, there are currently 12 related assessment systems in the interRAI network, spanning areas that include post acute care, mental health, palliative care and long-term care facilities. However, although the principle underlying this collaborative approach is admirable, many of the tools have been in existence for more than a decade without being widely taken up so far in clinical practice.
Casemix development in the UK
The UK has a very different health culture from that in Australia or the United States. The National Health Service (NHS) provides the most comprehensive publicly funded healthcare system in the world, with the majority of healthcare being provided free at the point of delivery. In addition, a closely integrated social services system provides life-long care and support, which is free to all individuals who are unable to pay for it themselves. In the light of this ongoing responsibility, maximizing functional independence is highly valued.
The NHS is now moving towards a standard ‘fixed tariff’ payment system along similar lines to the US-style Prospective Payment system. Introduction of the Department of Health’s Payment by Results programme 33 in England represents the biggest change in financial flows in the history of the NHS, and introduces some particular challenges as payment systems change from a ‘block contract’ model (in which the provider is paid a flat annual fee to provide an agreed level of service) to activity-based or ‘cost per case’ model (which reimburse providers on a case-by-case basis).
A trial application of the US-DRGs in the UK acute care sector demonstrated that they did not accurately fit the casemix of the NHS. 34 Instead, the UK scheme introduces a national episode-based tariff for healthcare treatments, based on a casemix classification of healthcare resource groups (HRGs), which are derived from a combination of diagnosis (ICD-10) and procedure (OPCS) codes 35,36 (see glossary of terms in Appendix 1 for further explanation). Like DRGs, HRGs are groups of conditions and interventions that are intended to have similar resource implications. The latest iteration (HRGs version 4) has been expanded significantly to underpin standard tariff payments for NHS treatments. 37 Tariffs for each HRG are determined through analysis of ‘reference costs’, the average cost of treatment spells within each category, reported by healthcare providers. 33
As in other episode-based funding models, the system is intended to reward additional activity and give an incentive to reduce length of stay, so driving up cost-efficiency. However, many specialties have recognized the need for increased ‘granularity’ of the classification to account for the additional costs of treating people with more complex needs. The introduction of mandatory tariffs has been put back in those areas pending further refinement of the casemix model. The Department of Health for England has also accepted the evidence that shorter lengths of stay do not always equate with efficiency, 16,17 and has therefore started to explored alternative payment models for management of long-term conditions, for example in the areas of mental health, palliative care and rehabilitation.
The challenges for rehabilitation
The implementation of standard tariffs for rehabilitation in the UK poses a number of specific challenges:
Existing NHS coding systems, which are based on diagnosis and procedure codes, contain few categories relating to rehabilitation, and even these are poorly reported. There is, therefore, little retrospective national data on which to estimate activity and base tariff prices.
Where data are available, reference costs for rehabilitation show very high levels of variance due to the marked diversity of needs for rehabilitation among patients within each diagnostic grouping.
A further challenge is presented by variation in caseload across different levels of service specialization. Following recommendations from a report by the Royal College of Physicians in the mid 1980s, 38 rehabilitation services have developed on a three-tiered model of local, district and regional services. To gain the advantage of critical mass, complex cases have been clustered into regional (tertiary) centres with specialized staff and facilities. 39 This clustering is feasible in the UK because of the relatively small geographic distances involved. However, it distorts the reference costs, as caseload complexity varies across the different levels of service.
Until recently, these three levels of service had not been formally defined, and it was left up to the provider to classify themselves. In 2009, the UK Department of Health for England published an updated National Definition Set which lays down specific criteria to support formal designation of ‘specialised services’ within in 36 healthcare domains. 40 Definition no. 7 ‘Complex specialized rehabilitation for brain injury and complex disability’ 41 identifies three levels of rehabilitation service:
Level 1 services – are discrete tertiary specialized rehabilitation services, serving a regional catchment of >1 million population.
Level 2 services – are discrete specialist rehabilitation services, led/supported by a consultant specialist in rehabilitation medicine, but operating within a more local, district-level catchment population (typically 350 000–500 000).
Level 3 services – are local non-specialist rehabilitation services, often provided in the context of acute or intermediate care, as opposed to a discrete rehabilitation unit.
In general, level 1 services have been shown to carry a greater proportion of complex cases. 42 However, due to the scarcity of such services, level 2 services in many areas have evolved to serve a supradistrict population (e.g. 600 000–1 million) and also carry a relatively high proportion of complex cases. This has led to calls for more accurate ‘patient level costing’, 43 and a casemix classification based on complexity of needs for rehabilitation, as opposed to simply categorizing by service type.
Development of casemix for rehabilitation in the UK
Until 2003/4, the UK casemix system (HRG version 3) did not include separate codes for rehabilitation. Casemix development for HRGs version 4 led to the inclusion of 23 codes for rehabilitation – three for assessment and 20 for admitted inpatient care 37 (see Box 1). The classification is based on diagnosis alone. However, it has been accepted by the UK Department of Health that further refinement is required for the classification to be fit for the purpose of tariff development. An Expert Reference Panel comprising casemix developers from the NHS Information Centre and clinicians from a wide range of rehabilitation service areas was set up to advise on HRG and tariff development in rehabilitation.
Rehabilitation Healthcare Resource Groups (HRGs) version 4
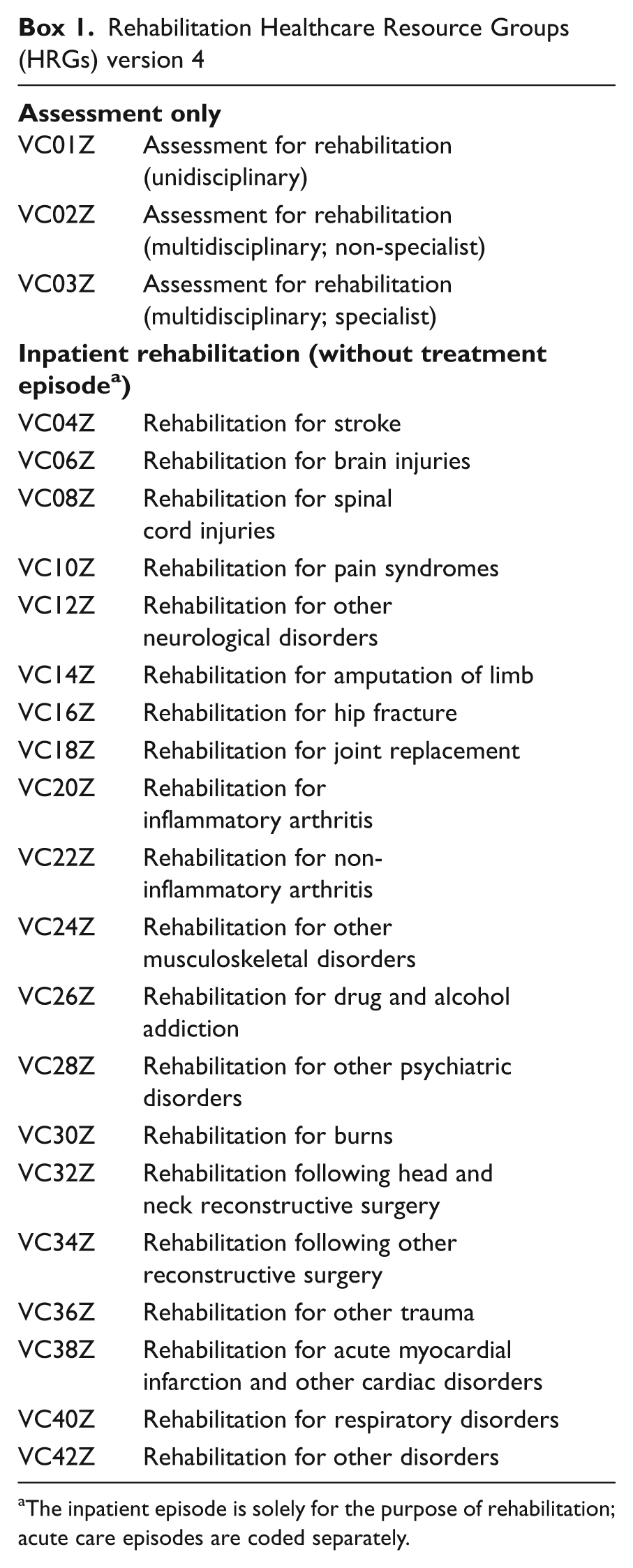
The inpatient episode is solely for the purpose of rehabilitation; acute care episodes are coded separately.
Preliminary exploration of the various existing international models revealed that none were immediately suitable for implementation in the UK. Casemix classifications based on measures of physical dependency (e.g. the FIM) may work reasonably well in the context of short-stay level 3 services where acute stroke and orthopaedic rehabilitation form the bulk of the caseload, and patients have reasonably predictable requirements for intervention. However, they work less well in specialist level 1 and 2 programmes, where the predominant focus in the UK is on neurological rehabilitation. For patients with brain injury and other complex neurological disabilities, physical dependency is a much less good predictor of rehabilitation needs.
Although the FIM correlates broadly with needs for basic care in hospital and community settings, 12,13 it does not directly measure the requirement for nursing, and correlates only weakly with the need for therapy and medical intervention. 44 It is also relatively insensitive in patients with predominantly cognitive/behavioural problems following brain injury, whose primary needs are for supervision as opposed to physical assistance. 45
The InterRAI RUG-III system was also explored, as it includes a crude measure of intensity of intervention and an earlier investigation had shown that it had potential as a casemix system for geriatric services in the UK. 32 However, it was found to have limited application in the context of complex specialized rehabilitation because of ceiling effects and, once again, the primary focus of this system is on physical dependency.
Therefore, although existing classifications provided a useful model to build on, they were not in themselves fit for purpose as a casemix and costing model for the UK. Instead, a different casemix classification is proposed, based on complexity of needs for rehabilitation (including care, nursing, therapy and medical intervention) as measured by the Rehabilitation Complexity Scale. 42,44 The weighted per diem payment model has been developed in the context of neurological rehabilitation, but application is expected in other areas of rehabilitation, once it has been validated in this context. The model applies a simple five-tier multilevel tariff through serial complexity ratings, so that the level of reimbursement changes with the requirement for intervention as the episode progresses. A companion paper 46 provides further detail of the model, and the proposed methods for collecting costing and casemix data.
In summary, the development of casemix in rehabilitation poses similar challenges for healthcare systems all around the world. Well-established casemix systems in the United States and Australia have afforded valuable lessons for other countries to learn from but have not provided all the answers. A range of casemix and payment models is required to cater for different healthcare cultures. Casemix tools must be simple and timely for clinicians to apply in routine practice, but must also capture all the key cost-determinants to allow fair payment for treatment of patients with complex needs. The UK approach may have wider application in other socially supported systems of healthcare.
Clinical messages
The majority of casemix systems for rehabilitation around the world are based on measures of physical dependency (e.g. the FIM or other ADL scales).
These may work reasonably well in high turnover settings, but do not adequately describe cost variation in complex neurological rehabilitation.
An alternative model, capturing the requirements for medical and therapy intervention as well as care, is proposed for patients with complex needs.
Footnotes
Appendix
Glossary of acronyms and terms used in this article and commonly used in casemix
| Acronym | Full name | Explanation |
|---|---|---|
| ADL | Activities of daily living | A term used in healthcare to refer to everyday self-care activities, e.g. washing, dressing, etc. |
| AN-DRG | Australian National Diagnosis-Related Groups | The original casemix classification system for acute inpatient services in Australia. It has since been superseded by the Australian Refined DRG system (AR-DRG) |
| AN-SNAP | Australian National Sub-Acute and Non-Acute Patient | The casemix classification for subacute care in Australia. AN-SNAP-II is the latest version, published in 2006 |
| AROC | Australasian Rehabilitation Outcomes Centre | The organization responsible for maintaining the datasets and tools for collation of data for rehabilitation services in Australia and New Zealand |
| CfH | NHS Connecting for Health | An agency of the UK Department of Health, which has the responsibility of delivering the NHS National Programme for Information Technology in England |
| CMS | Casemix system | A system that classifies people into groups that are homogeneous in their use of resources |
| BI | Barthel Index | A simple 10-item measure of physical disability, used in some casemix classifications (e.g. in the state of Victoria, Australia) |
| CMG | Case-Mix Groups | The casemix classification used in the US Inpatient Rehabilitation Facility Prospective Payment Scheme |
| DRGs | Diagnosis-Related Groups | A casemix system with classes defined mostly by principal diagnosis and procedures |
| FIM | Functional Independence Measure | An 18-item global measure of functional independence which is widely used to support casemix classification by dividing patients into groups of differing dependency |
| FIM-motor | Functional Independence Measure – Motor | The 13-item subscale of the FIM which records physical (motor) function |
| FIM-cognitive | Functional Independence Measure – Cognitive | The 5-item subscale of the FIM which records cognitive and communicative function |
| FRGs | Function-Related Groups | A casemix classification which separates cases into different groups, based on their level of functional independence – for example as measured by the FIM or Barthel Index |
| HRGs | Healthcare Resource Groups | The casemix classification system for healthcare services in the UK |
| IRF | Inpatient Rehabilitation Facility | A rehabilitation service in the United States offering post-acute inpatient rehabilitation |
| IRF-PAI | Inpatient Rehabilitation Facility Patient Assessment Instrument | A standardized dataset used by Medicare and Medicaid as the minimum dataset of demographic, diagnostic and functional information for in-patient rehabilitation in the United States. It is used to collect and collate casemix data |
| ICD-10 | The 10th International Classification of Diseases | An international clinical coding system for classification of diseases, developed by the World Health Organization |
| OPCS | Office of Population Censuses and Surveys | The UK office for national statistics |
| OPCS-4 | OPCS Classification of Surgical Operations and Procedures (4th revision) | A clinical coding system used in the UK for operations, procedures and interventions carried out during an episode of healthcare |
| PPS | Prospective Payment System | A system of fixed episode-based tariffs by which healthcare services are reimbursed for treatment in the United States |
| NHS | National Health Service (UK) | The system which provides publicly funded healthcare services in the UK |
| NHS IC | NHS Information Centre for Health and Social Care | A special health authority of the NHS in England which provides an authoritative source of health and social care information for the NHS and is resposnible for casemix and data sets |
| PLICS | Patient Level Information and Costing System | A system for measuring the resources consumed by individual patients |
| RCS | Rehabilitation Complexity Scale | A simple measure of complexity of needs for rehabilitation – subdivided into four subscales reflecting care, nursing, therapy and medical needs |
| RUG-III | Resource Utilization Groups | A casemix classification systems based on use of resources, which was developed through the InterRAI network and used in North American long-term care facilities |
| SCG | Specialised Commissioning Group (UK) | A body which provides collaborative commissioning of specialized services across a health region in the UK which includes a catchment population usually in excess of 1 million |
| SNF | Skilled Nursing Facility | The term for a specialist nursing home in North America |

Ethics approval
None required.
Conflict of interest
Professor Turner-Stokes chairs the expert reference panel for HRGs in rehabilitation, which is an honorary position. None of the authors has any personal financial interests in the work undertaken. We are not aware of any other competing or conflicts of interest.
Funding
This article presents independent research commissioned by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research funding scheme (RP-PG-0407-10185). The views expressed in this article are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. Financial support for the preparation of this manuscript was also provided by the Dunhill Medical Trust, the Luff Foundation.