
Abstract
Introduction
The prevalence of visual impairment increases significantly with age. 1 – 3 Worldwide about 314 million adults are visually impaired of whom 82% are aged 50 years and older 4 and it is expected that this number will double in the next 25 years.5,6 Visual impairment results in functional limitations and these consequently have a continuous negative effect on both older adults’ quality of life 7 – 10 and their performance of everyday activities. 11 – 13 In visually-impaired people particularly the level of mobility decreases, which hampers the ability to travel independently and to conduct activities in daily life outside the home. 14 – 16
Independent travel in the environment requires skills of orientation and mobility. Orientation is the ability to recognize and establish a position in relation to the environment, whereas mobility is the physical ability to move in an orderly, efficient and safe manner through the environment. 17 It is important for visually-impaired older adults to learn new orientation and mobility skills to compensate for reduced visual information, in order to maintain and regain independence during everyday activities.17,18 Therefore, orientation and mobility training, which is considered a necessary component of rehabilitation for partially-sighted and blind persons, aims to help them regain their independence by teaching them to manage both simple and complex tasks of daily life safely and effectively. 19 These tasks may include using the stairs, crossing a road, or walking in an unknown neighbourhood. Orientation and mobility training is often supplemented by the use of travel aids, such as the long cane or the identification cane.17,20 In particular, the identification cane, a short (approximately 35 inches) white cane with red straps, can be a useful travel aid for partially-sighted older adults enabling them to be recognizable in the environment and to cross a street safely and independently.21,22 Compared with the long cane (approximately 45 to 65 inches) that is used by visually-impaired persons who need assistance to anticipate what is ahead, the identification cane is used by persons who have some remaining travel vision to detect steps and obstacles while walking. Obviously orientation and mobility training in the use of these canes differs regarding techniques and intensity. 23
The benefits of orientation and mobility training in general have been the object of study. There is evidence that visually-impaired older adults benefit from orientation and mobility training in the use of travel aids (e.g. long cane or guide dog) and show improvements in quality of life. 24 Nevertheless, these evaluation studies have substantial limitations, such as the lack of a control group19,25 or randomization, 17 or the inclusion of rather small study populations.17,26 Evidence on the effectiveness of training in use of the identification cane seems to be lacking, however.
The objective of the present study is to describe the development, content, feasibility and effectiveness of existing orientation and mobility training in the use of the identification cane for partially-sighted adults worldwide. Given the differences in orientation and mobility training concerning different mobility aids 23 we only focused on the identification cane in this systematic review.
Design and methods
A systematic bibliographic database search in PubMed (1953–2010), PsychInfo (1806–2010), ERIC (1966–2010), CINAHL (1982–2010) and the Cochrane Library was performed on 28 February 2010. The following search terms were used to define the population: ‘visually impaired persons’, ‘vision disorders’, ‘low vision’, ‘visual loss’, ‘visual impairment’, ‘visually impaired’, ‘partially sighted’, ‘sighted’ or ‘partial vision’. These were combined with search terms used to define the intervention: ‘health services’, ‘rehabilitation’, ‘rehabilitation of vision impaired’, ‘occupational therapy’, ‘orientation’, ‘spatial orientation’, ‘wayfinding’, ‘mobility limitation’, ‘physical mobility’, ‘orientation and mobility’, ‘visual impaired mobility’, ‘travel’, ‘travel training’, ‘locomotion’, ‘education’, ‘training’ or ‘teaching materials’. Lastly, the search was combined with the following search terms: ‘cane’, ‘identification cane’ or ‘symbol cane’. The complete search strategy is available via the corresponding author; Appendix 1 shows the applied search strategy in the PubMed database. The expert consultation included 42 experts of orientation and mobility research and practice originating from nine different countries. The experts participated in the 13th International Mobility Conference 2009 ‘More than a cane’ or were obtained by a snowball method via these participants (i.e. each participant was requested to forward contact information of other potential experts, and so forth). The experts were asked to forward information with regard to studies on the effectiveness or feasibility of orientation and mobility training in identification cane use, as well as existing protocols or materials used to teach clients the use of the identification cane. Contact addresses of the experts concerned at the time of the search are available via the corresponding author. Hand-searching reference lists from potentially relevant papers was performed to find additional literature.
Only papers that were targeted at partially-sighted adults aged 18 years or older were included. Furthermore, the inclusion of papers was restricted to interventions consisting of orientation and mobility training in the use of the identification cane. Papers were included if they described one of the following: the development, the content, the feasibility, or the effectiveness of orientation and mobility training in the use of the identification cane. There was no restriction as regards the type of outcome measures. Papers that were targeted at a population of totally blind, deaf-blind, or intellectually disabled persons were excluded. In addition, only papers written in English, German, Spanish or Dutch were included.
Abstracts were cross-checked by author names and titles to insure that only unique abstracts were analyzed. Two authors (JB and GZ) independently checked whether the abstracts matched the selection criteria. Full-text papers were obtained for potentially relevant papers. Data from all included papers were independently extracted (JB and GZ). In addition to general characteristics (i.e. source, type of paper, systematic evaluation, objective of the orientation and mobility training, target group and facilitator), information was gathered on the development (i.e. developer and development methods), content (i.e. number of sessions, duration, frequency, format, setting, techniques and themes), feasibility (i.e. performance of the intervention according to protocol, reasons for drop-out, feasibility of the intervention, and provision of recommendations), and effectiveness (i.e. outcome and follow-up measurements) of the orientation and mobility training. Further, methodological quality was assessed from scientific papers (i.e. randomization, treatment allocation, similar groups at baseline, blinding of patient, blinding of care provider, blinding of outcome assessor, co-interventions avoided or similar, compliance, drop-out rate, timing of outcome assessment, and intention-to-treat analysis) with the Updated Method Guidelines for Systematic Reviews in the Cochrane Collaboration Back Review Group. 27 Owing to the diversity of the identified literature resulting from multiple sources, a qualitative data analysis method was used to synthesize the findings. Reviewers were not blinded to authors’ names, institution, or journal of publication. Disagreement was resolved by consensus of a third party (GK).
Results
The systematic bibliographic database search identified 206 abstracts (Figure 1). Since the identified abstracts included a number of
consolidated abstracts resulting from conference proceedings or progression reports, an additional
112 abstracts were identified, resulting in a total of 318 abstracts. After the exclusion of 70
duplicate abstracts, 248 potentially relevant abstracts were screened for the inclusion criteria.
Two hundred and thirty-two abstracts did not meet one or more inclusion criteria. Full-text papers
were obtained for the remaining 16 abstracts. None of the 16 potentially relevant full-text papers
entered the data extraction, since they were either not available (n = 3) or did not meet one or
more inclusion criteria (n = 13). The expert consultation resulted in 54 documents. Two documents
were duplicates and after screening for inclusion criteria another 46 documents were excluded. Six
documents met the inclusion criteria.17,28–
33
Additionally, hand-searching reference
lists from potentially relevant papers did not result in any new findings. Progress of search for relevant papers.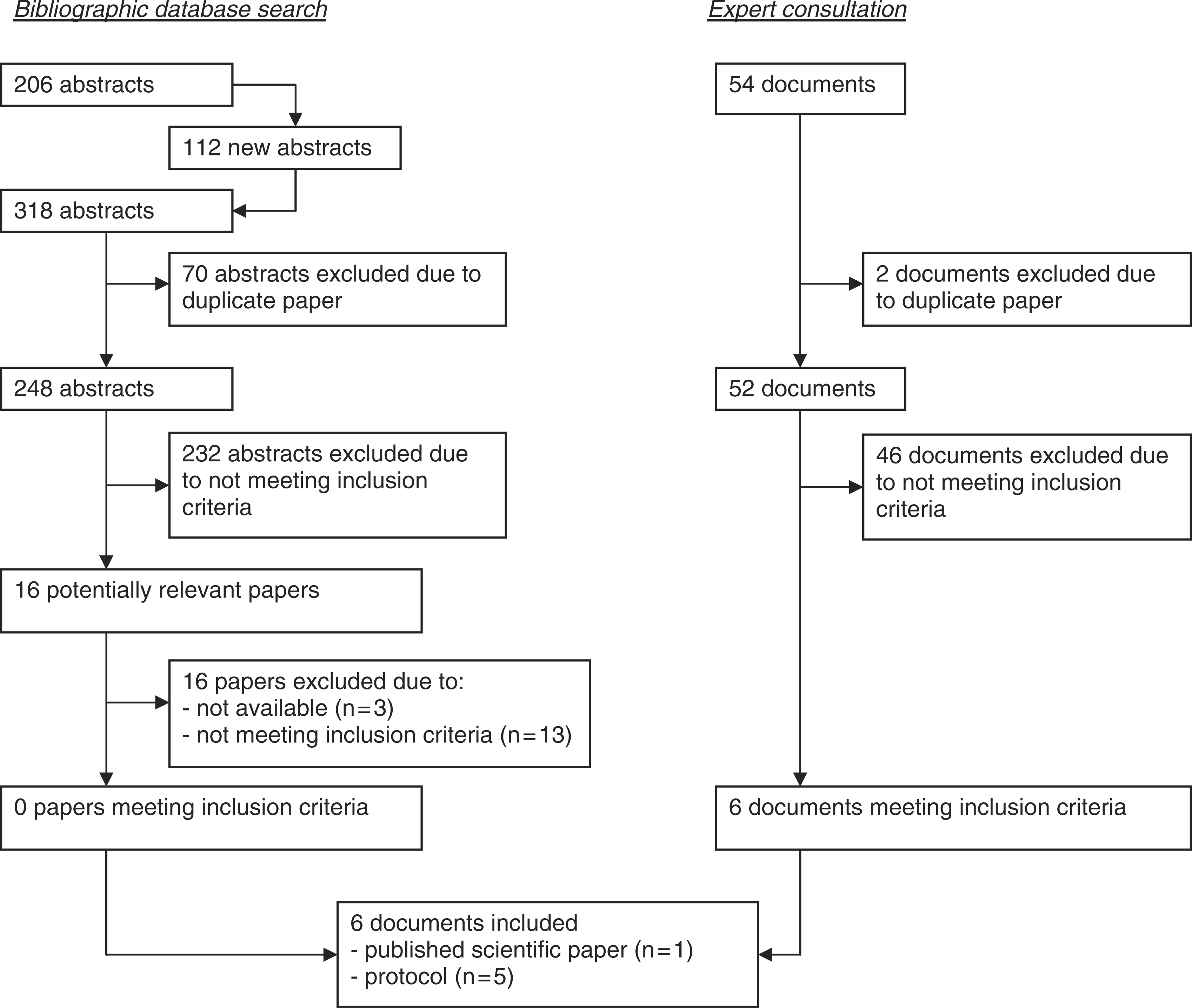
General characteristics of included documents on orientation and mobility training in the use of the identification cane
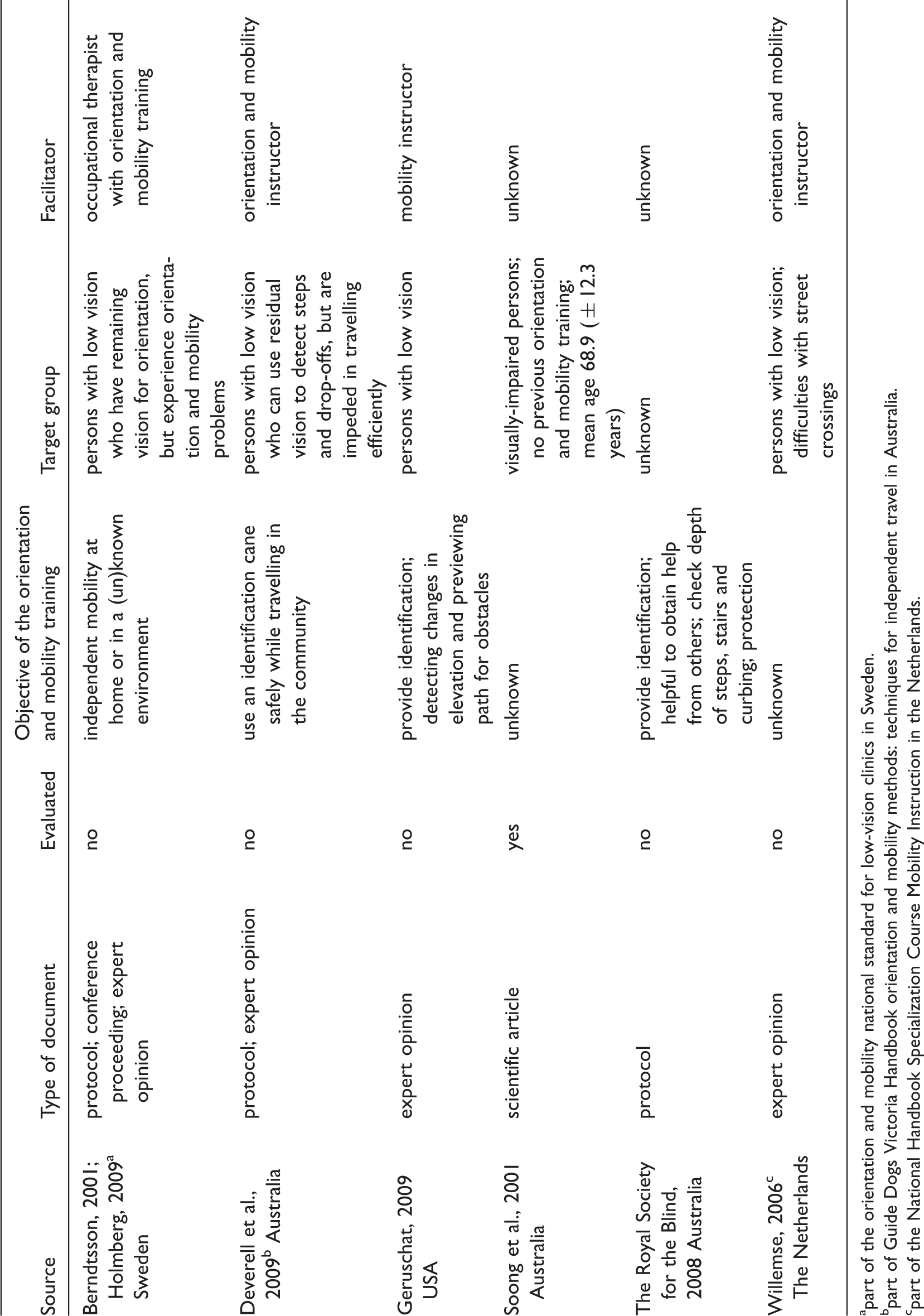
part of the orientation and mobility national standard for low-vision clinics in Sweden.
part of Guide Dogs Victoria Handbook orientation and mobility methods: techniques for independent travel in Australia.
part of the National Handbook Specialization Course Mobility Instruction in the Netherlands.
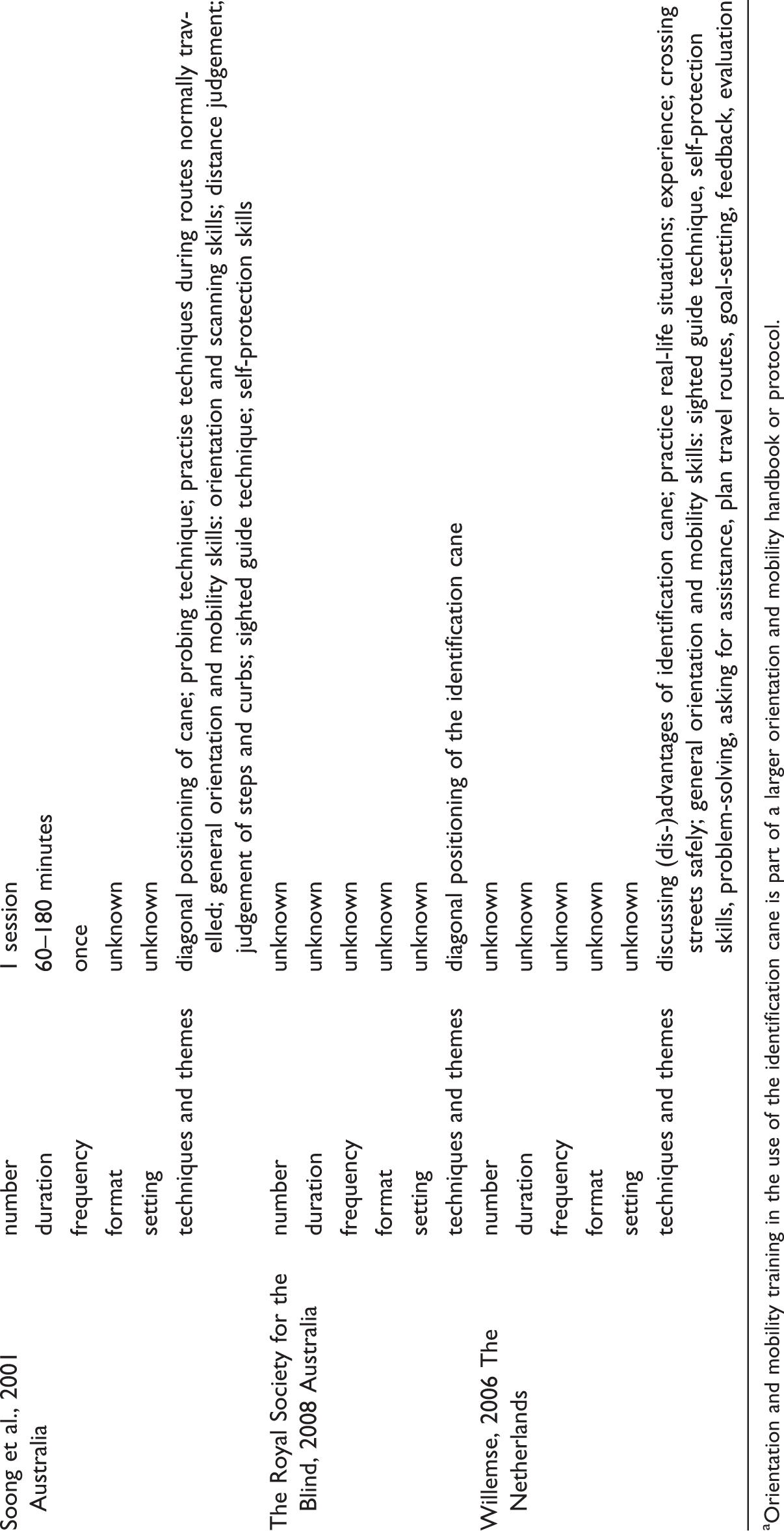
Content characteristics of included documents on orientation and mobility training in the use of the identification cane
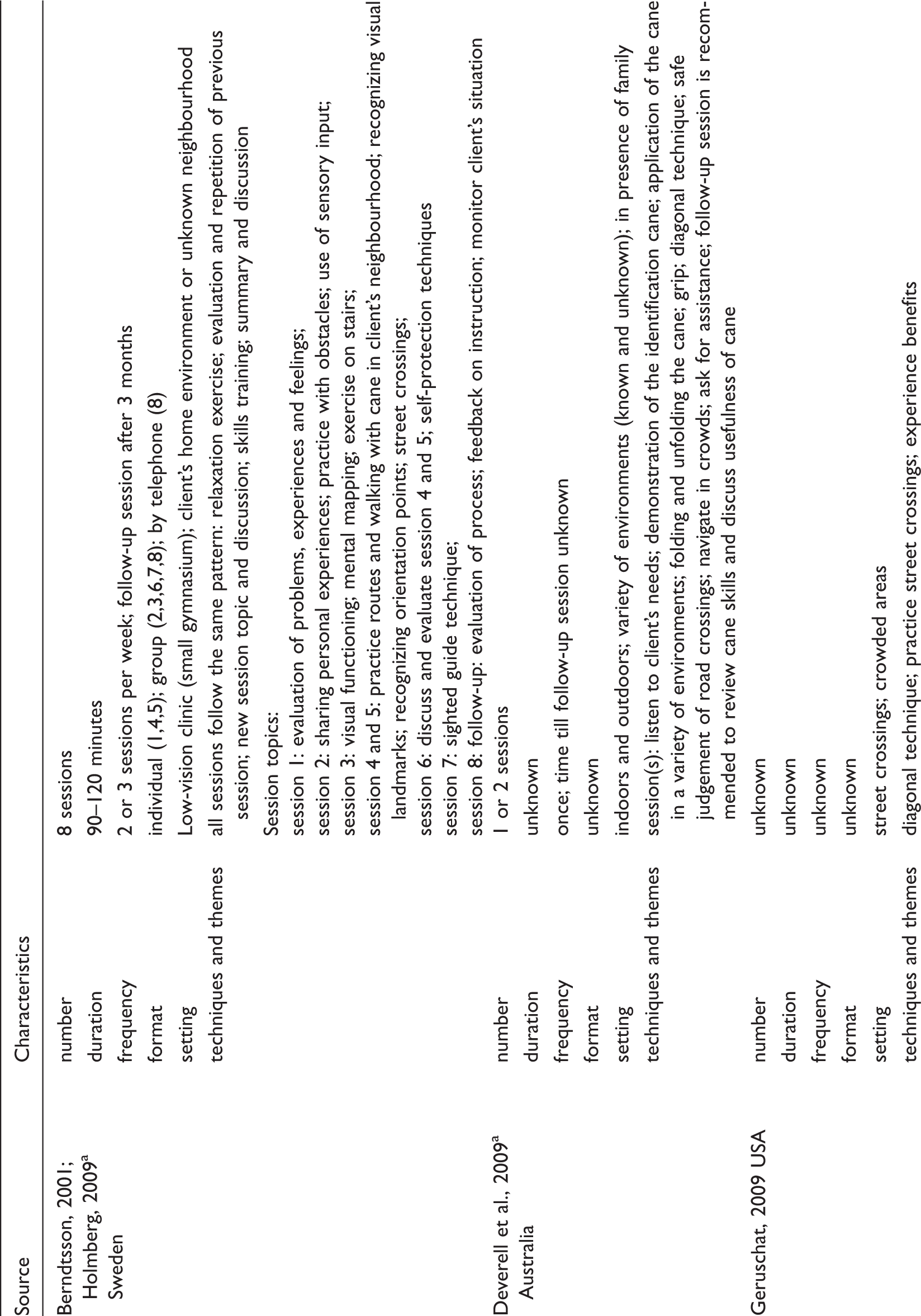
Orientation and mobility training in the use of the identification cane is part of a larger orientation and mobility handbook or protocol.
As can be seen in Table 1, which presents the general characteristics, the objectives of orientation and mobility training were generally safe and independent travel in the environment while using an identification cane, being recognizable, and possibly detecting changes in elevation. In two documents the objective of orientation and mobility training in the use of the identification cane was not described.17,33 The target group was frequently defined as persons with low vision experiencing orientation and mobility problems and the facilitator as a person specialized in orientation and mobility instruction.
The content characteristics of orientation and mobility training are presented in Table 2. The number of training sessions varied from one to eight.17,28–30,32 The orientation and mobility training described by Berndtsson (2001) and Holmberg (2009) consisted of two or three sessions per week of approximately 90 to 120 minutes and a follow-up session after three months. Soong and colleagues (2001) reported on a single orientation and mobility training session with a duration of approximately 60 to 180 minutes. Deverell and colleagues (2009) described orientation and mobility training of one or two sessions including a follow-up session whose duration was not reported. The setting of the orientation and mobility training was a mix of indoor and outdoor settings in clients’ neighbourhood or in an unknown environment. In the training presented by Deverell and colleagues (2009), family members are invited to join the orientation and mobility training where possible in order to promote safe and correct use of the identification cane by the client after the training. In addition, Berndtsson (2001) and Holmberg (2009) described the application of a sighted guide technique, where a close acquaintance learns how to guide efficiently.
Generally, in the six documents included, three main themes of orientation and mobility training were described: (1) crystallizing clients’ needs; (2) providing information (e.g. on the benefits of the use of the identification cane); and (3) training these techniques outdoors while the client applies the identification cane, such as holding the cane or practising in complex situations. In addition, one document explicitly reported on the application of techniques, such as evaluation, repetition, summarizing, and providing feedback during orientation and mobility training.29,32 Furthermore, in two documents a follow-up session was described: Deverell and colleagues (2009) recommended a follow-up session to review cane skills and discuss usefulness of the cane, whereas Berndtsson (2001) and Holmberg (2009) reported on a standard follow-up session by telephone or in group format, three months after the final group session, which incorporated an evaluation of the process, feedback on the instruction, and a check on the client’s situation.
Soong and colleagues (2001) evaluated the effectiveness of different types of orientation and mobility training (i.e. in the use of the long cane (n = 10), support cane or identification cane (n = 6) or no travel aid (n = 3)) compared with a matched control group who received no orientation and mobility training (n = 18), and found no improvement in mobility performance (i.e. preferred walking speed and error score during an indoor obstacle course) of visually-impaired adults. Findings regarding the methodological quality assessment of this study were as follows: no randomization procedure was adopted; neither participants nor outcome assessors were blinded to intervention status; it was unknown whether the groups were similar at baseline with regard to the most important prognostic indicators and if co-interventions were avoided or similar; information regarding the compliance, drop-out rate, and intention-to-treat analysis was not provided; the timing of the outcome assessment in all groups was similar.
Discussion
The results of our systematic review of the literature indicate that worldwide there is a noteworthy lack of documents and studies reporting on the development, content, feasibility and effectiveness of orientation and mobility training programmes in the use of the identification cane for partially-sighted adults. Our extensive search strategy provided only six documents and generally the information presented in these documents was incomplete and of low methodological quality.
At least two observations can be made concerning the outcomes of the literature review. First, literature regarding orientation and mobility training in the use of the identification cane is rarely available. Since orientation and mobility training programmes are practice-based it is likely that greater knowledge is available among orientation and mobility trainers. Our comprehensive search revealed only six documents, which were all obtained via expert consultation. The limited documents available may be explained by the focus of low-vision rehabilitation and research on orientation and mobility training in the use of the long cane, which is more common, involves higher-intensity training and teaching of different techniques. 23 Given this variation, papers and documents reporting on orientation and mobility training in the use of the long cane were not included in this review.
Second, literature on the development and feasibility of orientation and mobility training in the use of the identification cane is lacking, the content of the training is rather briefly described and only one study, which appeared to be of relatively low methodological quality, reported on the effectiveness of this training. 17 In this study, no improvement in mobility performance of visually-impaired adults after receiving orientation and mobility training was shown. Additionally the study has several limitations. To begin with the desired outcome of the intervention was probably not predefined, since the objective of their orientation and mobility training is unknown (see Table 1). For instance, successful outcomes following orientation and mobility training in the use of the identification cane might be improved mobility or quality of life, reduction of falls or accidents, or increased walking speed. Next, an accurate description of the content of the training is lacking. Hence, it is unclear what was exactly evaluated. Then, the effects of orientation and mobility training in general were evaluated, i.e. no distinction was made in orientation and mobility training with respect to the low-vision travel aid applied and, notably, only a small proportion of the subjects received orientation and mobility training in the use of the identification cane. Moreover, our methodological quality assessment revealed several potential sources of bias. Finally, the effectiveness of orientation and mobility training could not be established.
Nevertheless, a strength of this review is that it provides insight into several aspects of low vision care interventions, such as development, content, feasibility and effectiveness to establish feasible and effective low-vision rehabilitation care for partially-sighted older adults. The obvious increase of older adults experiencing vision loss and associated mobility problems in Western countries requires special attention for early interventions, such as orientation and mobility training in the use of the identification cane. These interventions need to slow functional decline, encourage independent functioning, and improve social participation and quality of life.
Several attempts were made to minimize bias. First, a sensitive and systematic search strategy was conducted in several bibliographic databases. Second, international expert consultation was added to the search to reduce publication bias. Third, data extraction was performed by two independent reviewers using a standardized form to extract the data. Fourth, in addition to the English language, documents in Dutch, German and Spanish were included. Finally, there were no restrictions on type of outcome measures in effect evaluations.
Recommendations regarding future research include increasing knowledge on the development and content of orientation and mobility training programmes in the use of the identification cane for partially-sighted older adults. Further, studies of high methodological quality that investigate the effectiveness and feasibility of this particular orientation and mobility training are required. Currently, a randomized controlled trial is being conducted to evaluate the standardized orientation and mobility training regarding the effects of the training on clients’ self-care activities in everyday life, functioning with respect to distance activities and mobility, and a variety of other outcomes, and its feasibility for trainers and clients. 34
Overall, our literature review showed that studies concerning the development, content, feasibility or effectiveness of orientation and mobility training in the use of the identification cane for partially-sighted older adults are lacking. The scientific knowledge base regarding the effectiveness of low vision rehabilitation care on client outcomes is scarce because of the lack of randomized controlled trials. Methodologically sound research is needed to provide explicit recommendations regarding the application of low vision rehabilitation care in general and the orientation and mobility training in particular in view of providing evidence-based care for people with vision loss. Further, from a clinical perspective, this review emphasizes the need for standardized, protocol-based interventions in the area of low vision rehabilitation.
Clinical messages
Knowledge about the development, content, feasibility and effectiveness of orientation and
mobility training in the use of the identification cane for partially-sighted older adults is
extremely sparse and there is no clinical evidence-base for orientation and mobility training
related to successful identification cane use. From a clinical perspective, orientation and mobility training represents an essential tool for
independent functioning and participation of partially-sighted adults.
Footnotes
Acknowledgements
We kindly thank the following orientation and mobility experts and organization who provided their assistance in the expert consultation: I Berndtsson, L Deverell, M van Doorn, B Ebrahim, M Flax, D Gallimore, D Geruschat, P Greber, K Grizelle, G Holm, M IJsseldijk, S La Grow, N van der Meent, J Nagel, P Rechsteiner, S Rosen, B Scott, E Smit, D Seybold, H van der Velde, P Verstraten, S Yu, K Zelaya, and the Swedish Institute of Assistive Technology.
Funding
This study was funded by Zon Mw–The Netherlands Organization for Health Research and Development, Program In Sight (grant 94305004).