
Abstract
This series of articles for rehabilitation in practice aims to cover a knowledge element of the rehabilitation medicine curriculum. Nevertheless they are intended to be of interest to a multidisciplinary audience. The competency addressed in this article is ‘The trainee demonstrates a knowledge of diagnostic approaches for specific impairments including cognitive dysfunction as a result of cardiac arrest.’
Keywords
Introduction
The overall incidence of cardiac arrest in the Netherlands is 0.92/1000 inhabitants per year, resulting in approximately 16 000 cases each year.1,2 Despite continuous attempts to improve resuscitation techniques and acute medical care, the worldwide survival rates have remained stable over the last 25 years, with a survival rate to discharge from the hospital in attempted resuscitations of only 7.6%. 3 However, the expectation is that the numbers of survivors will increase due to the growing availability of automated external defibrillators in public places and use by both professionals and lay people.4,5
Survivors of cardiac arrest are at risk of hypoxic–ischaemic brain injury, which can arise after a few minutes without cardiac output and leads to cognitive impairments in about half of the survivors of out-of-hospital cardiac arrest. 6 In addition, survivors of cardiac arrest can also experience other consequences, such as problems in emotional functioning, limitations in daily life activities, reduced participation in society and a decreased quality of life.7,8 The partners of cardiac arrest survivors, or other informal caregivers, also may experience negative effects, such as a high caregiver strain and symptoms of depression or post-traumatic stress.9,10
Although sometimes the problems after a cardiac arrest are obvious, in many cases the exact nature of the consequences can be hard to define and will remain hidden. Moreover, the detection of cognitive and emotional impairments can be especially difficult and should preferably be performed by someone who is trained and experienced in screening for these health problems and who recognizes their effect on daily living. Currently, this is not common practice and as a result the negative consequences of hypoxic–ischaemic brain injury may be underdiagnosed and undertreated. We therefore decided to design a new early intervention service for survivors of cardiac arrest and their caregivers, and subject it to a formal trial.
Up to now, only two studies have addressed a psychosocial intervention for patients after cardiac arrest.11,12 However, for patients with other cardiac diseases many more studies describing the effect of psychosocial interventions have been published. 13 – 15 Although these interventions often consider emotional aspects in patients with cardiac disease, they mostly do not address possible cognitive problems. Therefore, we additionally searched for evidence on effective interventions in a patient group with cognitive impairments after acquired brain injury. We focussed on patients with traumatic brain injury, as the negative health consequences of hypoxic–ischaemic brain injury due to cardiac arrest may resemble those after traumatic brain injury: Both are a result of diffuse brain injury and, in general, result mainly in cognitive impairments without evident physical impairments. In the design of our intervention for survivors of cardiac arrest we integrated evidence on psychosocial interventions for cardiac patients with evidence on effective interventions after traumatic brain injury. 16 – 18
This paper describes the new early intervention service for survivors of cardiac arrest called ‘Stand still… , and move on’, and will present the evidence and rationale behind this programme. We chose to describe the background and design of this intervention separately from the results on its effectiveness, as we can provide more detailed information on the actual content of the intervention here. This may facilitate interpretation, reproduction and possible implementation of the intervention in clinical practice. The effectiveness of the intervention is currently being investigated in a randomized controlled trial and will be reported on in the future. 19
To give an overview, first the design process of the intervention will be described. Second, the evidence currently available on the effectiveness of existing psychosocial interventions for both cardiac patients and patients with traumatic brain injury is presented. Finally, the characteristics and content of the intervention itself will be provided.
Design of the early intervention service – overview
We reviewed articles presenting results of controlled studies of psychosocial interventions in people with cardiac arrest, other cardiac diseases and traumatic brain injury. In order to do this, a literature search was performed in the database PubMed using keywords such as ‘heart arrest’, ‘coronary artery disease’, ‘traumatic brain injury’, ‘aftercare’, ‘nursing care’, ‘follow-up programme’, ‘psychosocial intervention’ and ‘psycho-educational intervention’. We excluded several studies on patients who had received an implantable cardioverter defibrillator (ICD), but in which it was unclear whether they had also had a cardiac arrest.
The literature study resulted in a framework for the new intervention which was then discussed during an expert meeting with three consultants in rehabilitation medicine, a trainee in rehabilitation medicine, a psychologist and a nurse from a neurology department. Next, this group designed a preliminary protocol for the intervention and, in addition, an information booklet. The protocol and the information booklet were reviewed by an advisory board consisting of another consultant in rehabilitation medicine, a cardiologist, a neurologist and several experts working in a brain injury department. In addition, patient opinion was derived from interviews with three cardiac arrest survivors and their families and they were asked to give feedback on the preliminary outline of the intervention and the information booklet. Finally, the intervention was tested on four subjects during a pilot study. All patient feedback was integrated in the final protocol.
We used a holistic biopsychomedical model of illness based on the International Classification of Function, Disability and Health as a framework to guide our study and intervention20,21 This model is commonly used in rehabilitation medicine practice and research and it distinguishes three levels of functioning, namely basic function, activities and social participation. The following are examples of the three levels in a survivor of a cardiac arrest. First, a person can have limitations in function, such as a reduced cardiac ejection fraction, memory impairments or a depressed mood. Second, at the level of activities, a person may be limited in leisure activities or in performing household activities. With regard to participation, this may affect someone’s role as a parent or partner and can result in difficulties in return to work. Moreover, the three levels of functioning can interact and are also affected by personal and environmental factors.
Review of the literature
Evidence on psychosocial interventions in patients with cardiac disease
We identified two studies on psychosocial interventions after cardiac arrest. Cowan et al. performed a controlled study that examined the effect of individual psychosocial nursing therapy after a cardiac arrest. 11 The intervention consisted of eleven 90-minute sessions given by an experienced cardiovascular nurse. During the sessions physiological relaxation was practised, self-management and coping strategies were taught and health education was given. This intervention led to a reduced risk of cardiovascular mortality and depressive symptoms two years later.
Dougherty et al. designed a telephone-based nursing intervention for survivors of cardiac arrest, who had received an ICD. 22 The intervention was directed at improving self-efficacy, outcome efficacy expectations and enhancing self-management behavioural skills. 23 The content of the intervention was based on the patients’ and partners’ concerns that were identified through multiple interviews during the first year after the cardiac arrest. In this study the following topics were considered most essential and became part of the intervention: physical changes and symptoms, activities of daily living, emotional reactions, shocks from ICD, partner relationships, safety and prevention, and dealing with health care providers. 24 The intervention was given by specialized cardiovascular nurses and started after the ICD implantation. During eight consecutive weeks, there were weekly 15–20 minute telephone contacts. Moreover, all participants could use a nurse pager system to contact a nurse at any time and an information booklet was supplied in which the experiences and successful strategies of other survivors were described. This information booklet was highly appreciated by the participants. 22 The effectiveness of this intervention was examined in a randomized clinical trial, which showed that the intervention group showed less physical symptoms, lower levels of anxiety and enhanced knowledge about cardiac arrest and living with an ICD, both in the short term and long term.12,25 The long-term results also showed an improvement in self-confidence. There was no effect on health care use.
In contrast to the limited number of studies on intervention services for survivors of cardiac arrest, there are numerous studies on psychosocial interventions for patients with other cardiovascular diseases, such as coronary artery disease or heart failure. Two meta-analyses summarizing results up to 1995 and 1998 respectively, studied the additional effect of psychosocial/psycho-educational interventions in standard rehabilitation programmes for patients with coronary artery disease.13,14 Both reviews showed that the addition of psychosocial interventions led to a decrease in cardiac mortality and lowered the recurrence of non-fatal cardiac events. Moreover, beneficial effects were found on cardiovascular risk factors, such as systolic blood pressure, heart rate, cholesterol, weight and smoking habits. In addition, the review by Linden et al. reported a positive effect on the levels of anxiety and depression, 13 but this finding was not replicated in the review by Dusseldorp et al. 14
A recent third systematic review by Allen et al. summarised 55 randomized trials of nursing interventions in patients with coronary artery disease or heart failure published between 2000 and 2008. 1 5 The majority of the interventions consisted of combinations of education, behavioural counselling and support. This review showed that a small majority of the trials demonstrated a beneficial impact on at least one of the following outcome measures: blood pressure, lipids, physical activity, dietary intake, cigarette smoking, weight loss, health care utilization, mortality, quality of life or psychosocial outcomes. Three out of ten studies showed a significant effect on psychosocial factors such as anxiety, depression, adjustment or self-efficacy. 15
All three systematic reviews described above recommend the inclusion of psychosocial treatment in cardiac rehabilitation programmes. However, none of them could identify the specific components that make the interventions effective.
A fourth systematic review by Jovicic et al. did investigate the specific effect of the promotion of self-management in patients with heart failure. 26 Self-management was defined as ‘enabling patients to assume a primary role in managing and improving their condition and health’, implying that an active attitude towards dealing with their problems is promoted. Self-management can, for example, be improved by acquiring several self-management skills such as problem solving, decision making, resource utilization and action planning. 27 This review showed that self-management programmes for patients with heart failure resulted in improvements in health behaviour and a decrease in hospital readmissions in patients with heart failure, but did not affect quality of life scores or mortality.
To conclude, the literature reviewed above has shown some positive effects of psychosocial interventions for survivors of cardiac arrest and other cardiac diseases. However, all reviewed studies focused mainly on the cardiac disease and emotional problems and did not address possible neurological or cognitive problems. However, cognitive impairments, especially problems with memory, attention and planning, are common after cardiac arrest and affect half of the survivors. 6 In the next paragraph, we will therefore report on an additional literature search on psychosocial interventions in patients with traumatic brain injury, as they may have symptoms comparable to those in patients with hypoxic–ischaemic brain injury after cardiac arrest.
Evidence on psychosocial interventions in patients with traumatic brain injury
Although patients with severe traumatic brain injury often require inpatient rehabilitation treatment, this is not always necessary for patients with mild or moderate traumatic brain injury. In fact, the study of Salazar et al. compared an eight-week inpatient rehabilitation programme with a limited eight-week home rehabilitation programme for military patients with moderate-to-severe closed head injury and showed that there were no differences with regard to return to work, quality of life and cognitive or psychiatric function up to one year. 28
Next, a study by Bell et al. showed that a telephone-based intervention for traumatic brain-injured patients, consisting of seven calls in nine months, appeared to be effective one year later on functional status and quality of well-being. 29 The telephone consultations consisted of brief motivational interviewing, counselling, education and, if necessary, follow-up appointments or therapy prescriptions.
Moreover, three controlled studies showed that even more concise, mostly one-session outpatient interventions, can be equally effective in patients with traumatic brain injury. 16 – 18 In the first study, Paniak et al. compared one-session educational intervention and providing a folder on head injury with a more intensive outpatient treatment including several consultations, neuropsychological assessment and additional therapy if indicated.16,30 The concise intervention was equally effective after three and twelve months on measures of participation, quality of life and vocational status, and also patient appreciation was comparable. In the second study by Wade et al. an early intervention was offered to patients who had been admitted to the hospital after any kind of traumatic brain injury. Participating patients were approached at 7–10 days after injury by an occupational therapist or psychologist. They were offered additional information, standardized information leaflets, advice, support and further assessment or interventions as needed. 31 This individually tailored intervention resulted in improvements six months after the injury in social participation and everyday activities and decreased the severity of post-concussion symptoms, such as concentration difficulties, headaches, fatigue, sleep disturbance and irritability. 17
The third study by Ponsford et al. reported on an early intervention for patients with mild traumatic brain injury who had not been admitted to the hospital. 18 In this intervention patients were contacted within 48 hours and seen 5–7 days after their injury. An information booklet was handed out concerning common symptoms and course after traumatic brain injury and possible coping strategies. This intervention led to a reduction in post-concussion symptoms and psychological distress three months later.
Summarizing the evidence on psychosocial interventions after traumatic brain injury reveals that even concise outpatient interventions consisting of at least oral and written information, support and sometimes further referral at indication, are effective up to one year after the event.
To conclude, based on the literature available, there is evidence that interventions that focus on psychosocial aspects and self-management may be effective in patients after cardiac arrest and other cardiac diseases. In addition, there is also evidence that concise and early intervention services for patients with mild to moderate traumatic brain injury can be useful and effective. Our patient group of interest, survivors of cardiac arrest, is at risk for brain injury due to a cardiac cause. Currently, we are not aware of any studies that have evaluated the effect of an early psychosocial intervention or rehabilitation programme for the consequences of hypoxic–ischaemic brain injury due to cardiac arrest. Therefore, we have developed a new intervention service for survivors of cardiac arrest, based on the combined evidence on effective interventions in the fields of cardiac disease and traumatic brain injury.
The intervention ‘Stand still… , and move on’
Assumptions and goals
The early intervention service ‘Stand still…, and move on’ is designed for all patients who have
suffered and survived a cardiac arrest and their caregivers. It is based on the following
assumptions: Any person who had a cardiac arrest may suffer hypoxic–ischaemic brain injury. Cognitive and emotional problems are common after cardiac arrest. Cognitive and emotional problems are often not recognized by health care professionals. Partners or other informal caregivers may also be affected significantly. Patients and caregivers may be helped by a relatively brief psychosocial intervention that
screens for cognitive or emotional problems and offers information, advice and support.
The intervention has the following main goals: early detection of cognitive and emotional problems; providing appropriate information and emotional and practical support; promotion of self-management techniques; referral to specialized services if necessary.
Structure of the intervention
Characteristics of the early intervention service
The intervention is focused on the neurological sequelae of hypoxic–ischaemic brain and on emotional or other problems that may arise after the cardiac arrest. This intervention does not address any specific cardiac or physical rehabilitation goals, although we do not exclude the possibility of combining the content of this intervention with more physically oriented cardiac rehabilitation programmes.
This early intervention service is given on an individual basis. Sometimes, psychosocial or self-management programmes are offered as a group programme, but the low numbers of possible participants per hospital per month implied that it would take several months to form a new group. Thus, because the intervention is meant to start soon after discharge from the hospital, we designed an individualized programme. This also makes it possible to offer a more individually tailored intervention that can be adapted to the needs and wishes of the participants.
Specialized nurses
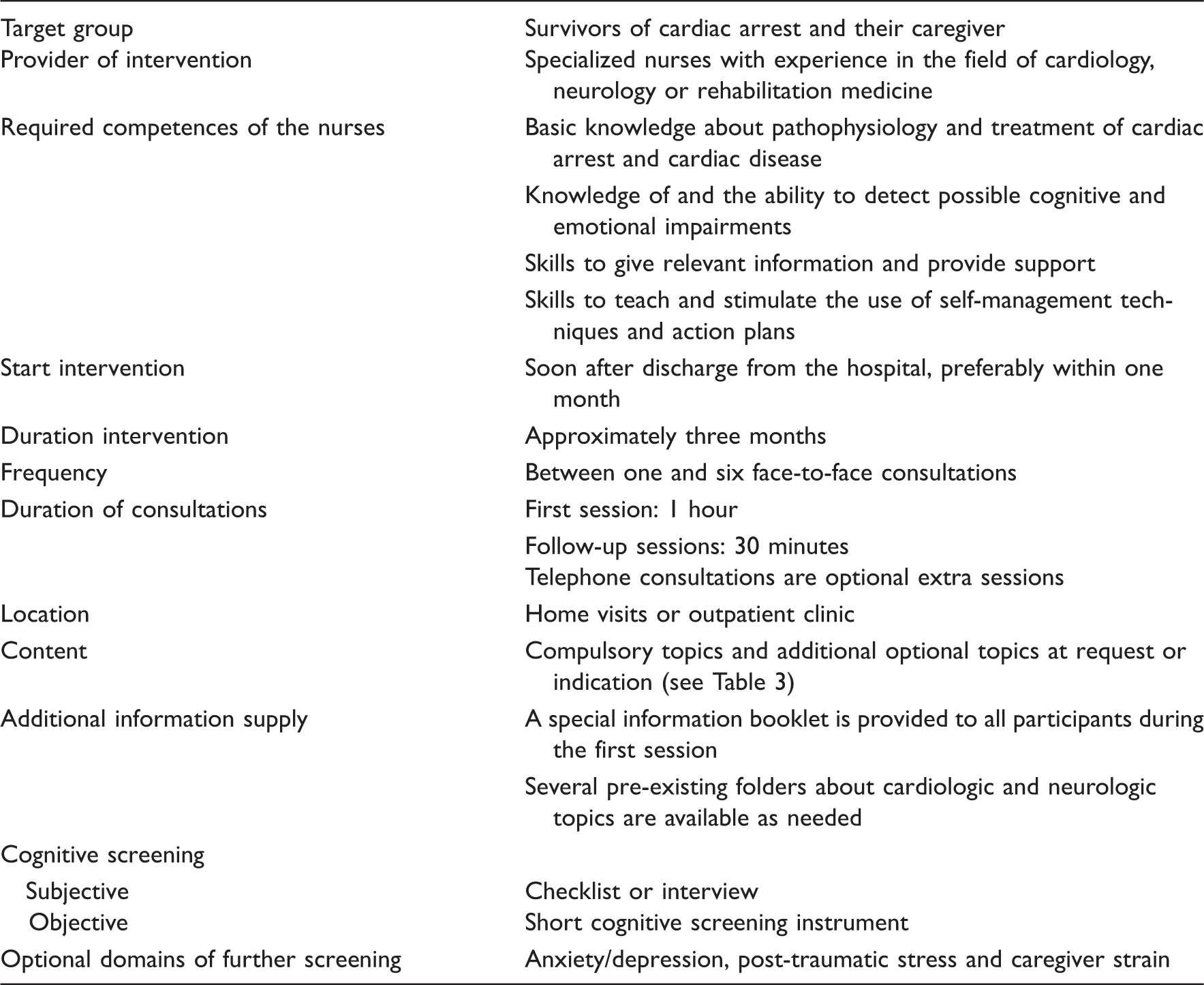
The early intervention service can be provided by nurses with a background in cardiology, neurology or rehabilitation medicine. The nurses participating in the trial received a 12-hour training programme focused on acquiring the necessary competences (Table 1). In the training special attention was directed at acquiring skills to detect cognitive and emotional impairments and skills to teach and promote self-management techniques. We prefer nurses as providers of the intervention since having a medical background is, to our opinion, important as patients may still have medical questions after discharge from the hospital. Next to that, nurses are trained in dealing with a diverse spectrum of problems and in giving practical support and advice. We also expected that a nurse-based intervention will have a higher cost-effectiveness compared with screening by a physician. However, we do not rule out that persons with another background or profession could deliver this intervention as well, provided that they have had suitable experience and training. In our trial the nurses worked under the supervision of a consultant in rehabilitation medicine, with whom they also discussed potential referrals.
Content of the intervention
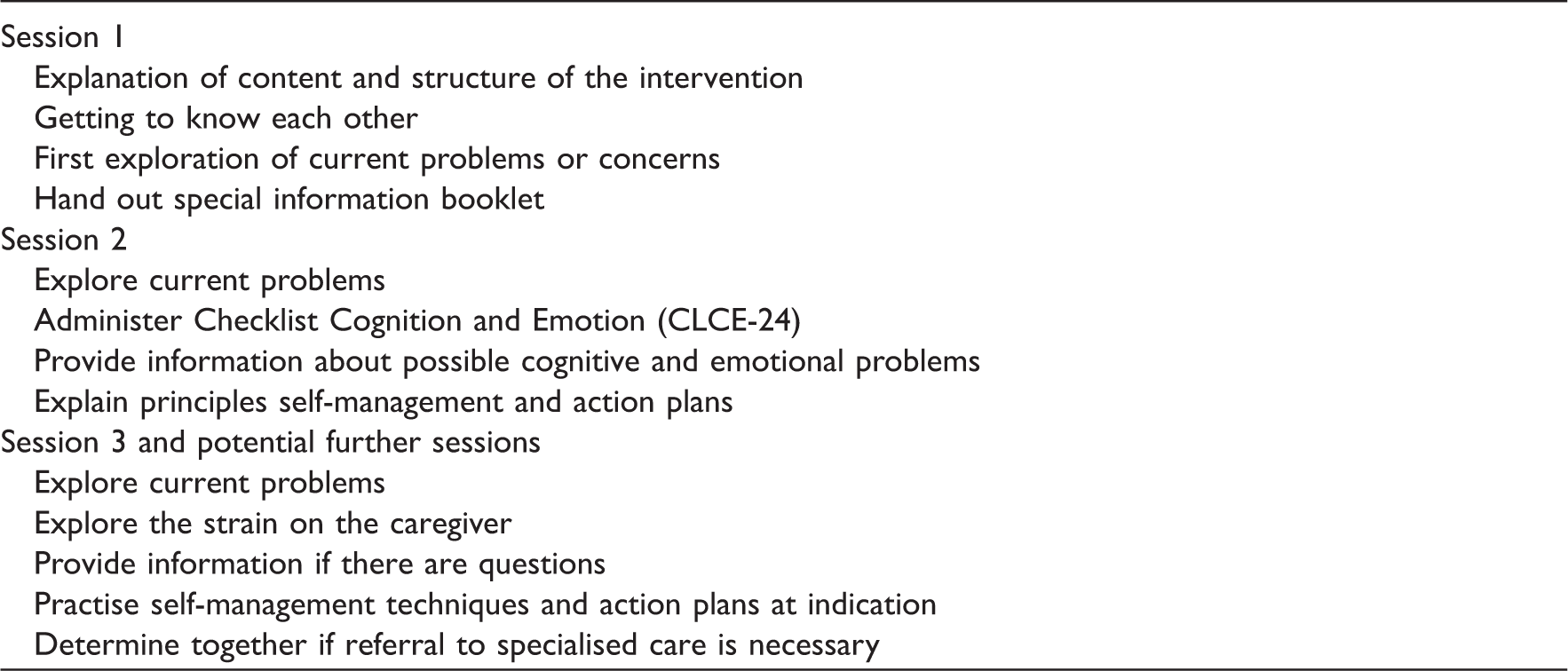
Suggested content of the sessions
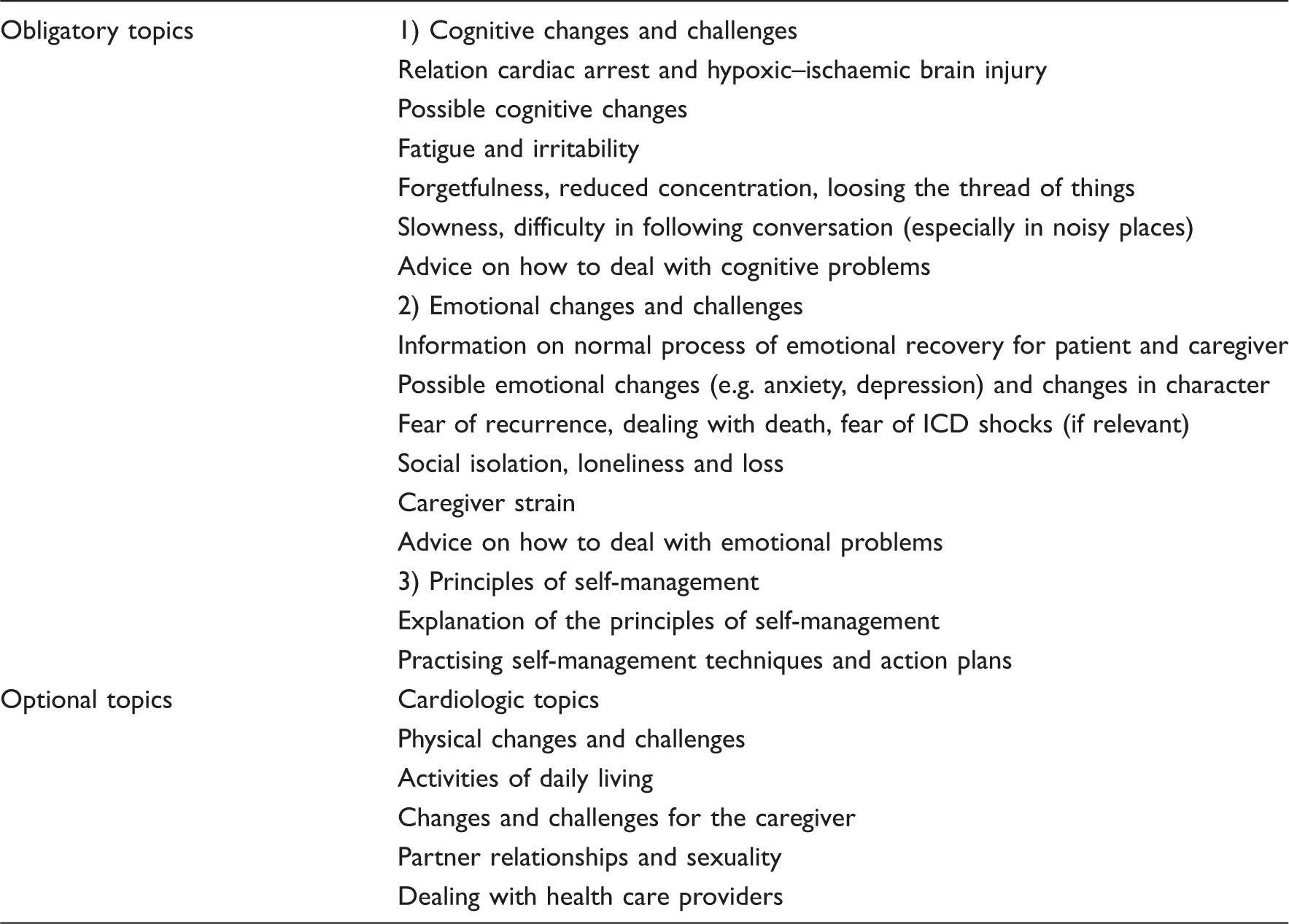
Obligatory and optional topics of the intervention
Caregivers, usually a partner or spouse and occasionally another informal carer, are also invited to participate because they often have difficulties such as feelings of depression or post-traumatic stress and can experience a high burden.9,10,32 Information, reassurance and support might be also useful for them. In addition, caregivers can help the patient to remember the information provided during the consultations and they can provide insight about the actual functioning of the cardiac arrest survivor. The nurse will proactively investigate caregiver strain and may suggest coping strategies. This is usually deferred to session 3 but can be started earlier if there is need to do so.
The nurse also discusses with the participants whether further referral is necessary, usually during the last session, but earlier if needed. Depending on the current problems, referrals can be made, for example to a consultant in rehabilitation medicine in order to evaluate the necessity of a multidisciplinary rehabilitation treatment, to a neuropsychologist for further cognitive testing or to a cardiologist in case of cardiac symptoms or concerns.
Self-management
Teaching self-management is an important part of the programme. The goal of self-management is to stimulate patients to take responsibility in striving for the best quality of life with their condition. Acquisition of self-management techniques includes acquiring problem solving skills and making action plans. 27 Controlled studies in several chronic patient groups in primary care have shown that patient education programmes that include the teaching of self-management skills are more effective compared with information-only education programmes. 33 It has also been shown that the inclusion of action plans, in which patients make a plan how to gradually work towards a short-term achievable goal, makes self-management interventions even more effective. 33 During the intervention, the nurse explains the background of self-management, teaches self-management skills and stimulates the patient to make action plans, which are evaluated in the next session.
Information booklets
As part of the intervention, a special information booklet was written; this is handed out during the first session. In this booklet information concerning the mechanism and possible consequences of hypoxic–ischaemic brain injury due to cardiac arrest is presented. It highlights the most frequently reported cognitive and emotional problems encountered by patients after cardiac arrest and provides information about possible coping strategies. In addition, the potential negative impact upon the caregivers is addressed.
Furthermore, the nurses also have access to several pre-existing folders that can be handed out at indication. These focus on related topics in the field of cardiology (e.g. cardiac medication, cardiac treatments and implantation of an ICD), neurology (e.g. stroke, coma, memory problems and fatigue) or driving restrictions. Such folders are largely freely available.
Screening instruments
The detection of possible cognitive or emotional problems is one of the most important goals of this intervention and can be supported by both subjective and objective screening instruments. An example of a subjective instrument is the Checklist Cognition and Emotion (CLCE-24). Originally, the CLCE-24 was designed to detect cognitive and emotional problems in stroke patients. 34 This checklist describes over 20 common cognitive and emotional problems and during a semi-structured interview the patient and caregiver are asked whether they recognize any of these problems. Alternatively or in addition, an objective cognitive screening instrument may be used. We recommend the use of an instrument that includes at least a minimum set of assessments on memory, attention and executive functioning, as these cognitive domains are most often impaired after cardiac arrest. 6 In our study the Cognitive Log (Cog-log) was used for this purpose, 35 but our experience so far suggests that it may not be sensitive enough to detect cognitive impairments in this patient group. Another potential cognitive screening instrument is the Montreal Cognitive Assessment (MoCA). 36 The MoCA is a brief cognitive screening instrument with a good sensitivity and specificity for the detection of mild cognitive impairments and includes items measuring executive functioning and attention, but it has not yet been studied in patients with hypoxic–ischaemic brain injury. The Mini-Mental State Examination (MMSE) has been shown to be an invalid and insensitive instrument without an appropriate cut-off point for the detection of cognitive problems in both acute and chronic stroke, and is probably not particularly useful in our patient group. 3 7, 38
The specialised nurse can also use additional instruments for the screening of symptoms of anxiety/depression, post-traumatic stress and caregiver strain, if this seems clinically relevant. In our protocol we used the Hospital Anxiety and Depression Scale, 39 Impact of Event Scale 40 and the Caregiver Strain Index 41 for this purpose respectively, but several other good instruments are available.
Discussion
Survivors of cardiac arrest are at risk for cognitive or emotional problems, which can lead to limitations in daily activities, social participation and quality of life and may also affect the caregivers. In this article we have described a new early intervention service consisting of four components: (1) early screening on cognitive and emotional problems, (2) supply of information and support, (3) promotion of self-management techniques and (4) referral to specialized care if necessary. These four components are all expected to contribute to the effectiveness of the intervention and will now be discussed respectively.
Our first assumption is that, especially in case of the ‘hidden’ cognitive and emotional problems, an active screening method is indicated. Patients may not anticipate on a link between their cardiac arrest and, for example, the memory problems or depressive mood they experience, and therefore will not actively seek for support themselves. A study on stroke patients already showed that formal screening resulted in the detection of a much higher number of cognitive and emotional impairments compared with information obtained from the patient’s chart at discharge. 42
Second, we assume that the provision of information and support may have a positive effect on both the patient and the caregiver. Information about the cardiac arrest and common symptoms in patients and caregivers can reduce stress, as it may stop the vicious circle of symptoms and worries. Next to that, the nurse can promote an active coping style and suggest compensation strategies. 17
Third, the intervention promotes the use self-management techniques. The use of self-management has previously been shown to be effective in heart failure 26 and several other chronic illnesses. 27
Fourth, if during the intervention severe or disabling problems are detected, this should lead to a referral for further assessment and treatment. We expect that early detection and early treatment may prevent or reduce future problems.
To conclude, the design of this early intervention service for survivors of cardiac arrest was based on current evidence, expert opinion and patient experiences and has a clear rationale behind it. The next step is to determine its effectiveness objectively, taking also the cost-effectiveness into account. This is currently being investigated in a randomized controlled multicentre trial with a one-year follow-up in which the new intervention is compared with care as usual. 19 In addition, a process evaluation will be performed in which we will monitor the actual implementation of the intervention, determine whether the intervention was delivered according to protocol and evaluate the experiences of the participants and the nurses.
Clinical messages
Survivors of cardiac arrest may have cognitive and emotional impairments due to hypoxic–ischaemic
brain injury, leading to limitations in daily activities, a decreased level of participation in
society and a lower quality of life. In current care these problems are probably underdiagnosed and undertreated. A new early intervention service designed to detect and manage these problems is described.
Footnotes
Acknowledgements
We would like to thank Brigitte Cobben for her help in the design and testing of the intervention. We also thank the patients and caregivers for their valuable contributions and feedback on the intervention and the information booklet.
Funding
This study is funded by the Netherlands Organization for Health Research and Development (ZON/MW); and Fonds Nuts Ohra.
Conflict of interest
The authors declare that there is no conflict of interest.