
Abstract
Background and Objectives
Many overweight individuals develop obesity-associated functional venous insufficiency (OA-FVI), also known as obesity-associated dependency syndrome. This study investigates the impact of medical compression stockings (MCS) on the symptoms.
Patients and Methods
A total of 49 patients, 37 female and 12 male, with a body-mass-index (BMI) of 30–40 kg/m2 and a clinical presentation of OA-FVI corresponding to chronic venous insufficiency (CVI) stages C3–C5 were included. During the intervention phase, patients wore knee-length MCS compression class 2 (CCL2). In the first week, flat-knit MCS was worn on the left leg, round-knit MCS on the right leg. In the following 3 weeks, patients wore the MCS of their choice on both legs.
Results
The average patient age was 54.0 years, and the mean BMI was 35.6 kg/m2. The average daily wearing time of the MCS was 9.6 hours. Among 40 patients with analyzable data, the VVSymQ score was reduced to 57% of the baseline value (p < .00001), particularly for the key symptoms of swelling, heaviness and achiness as well as throbbing. Edema was initially present in 22 patients. During the MCS intervention, the edema healed in 73% of the affected patients. The fit and comfort of the MCS was assessed as good or very good by 98% of the patients, donning and doffing was assessed as good or very good by 89% and 78% of the patients.
Conclusions
The symptoms of OA-FVI can be effectively reduced using MCS. The obese patients showed good compliance.
Trial registry name
Deutsches Register Klinischer Studien; URL: https://drks.de/search/de/trial/DRKS00015468; registration number: DRKS00015468.
Chronic venous insufficiency (CVI) describes conditions of advanced chronic venous disease that lead to edema, skin changes, or venous ulcers. 1 These clinical symptoms can not only be triggered by varicose veins but also by other functional disorders of the venous system, such as changes in venous hemodynamics due to obesity. 2 In this context, abdominal fat tissue plays a significant role. 3 Current studies show that advanced stages of CVI, such as stasis dermatitis, atrophie blanche, and ulcus cruris (CEAP (Clinical-Etiology-Anatomy-Pathophysiology) classification C4 to C6), 4 are associated with an increased body mass index (BMI). In the large Bonn vein study, the prevalence ratio for severe CVI (C4–C6) versus C0/C1, multivariable adjusted for age, gender, a family history of varicose veins and many other risk factors, was 2.86 (95% CI: 1.74; 4.69) in obese persons (BMI ≥30 kg/m2) compared to those with normal weight (BMI <24.9 kg/m2). 5 The multivariable adjusted prevalence ratio for venous edema in the context of CVI (C3 vs C0/C1) was 3.47 (95% CI: 2.68; 4.48) for obese persons compared to those with normal weight. 5 The adjusted prevalence ratio for varicose veins, in contrast, was 1.57 (95% CI: 1.33; 1.85) for those with a BMI ≥30 kg/m2 and thus also significantly increased, but not as pronounced as for CVI. 5
Due to visceral fat tissue, obese patients may experience functional impairments in venous outflow instead of hemodynamically relevant venous insufficiencies, such as malfunction of the venous valves. This obesity-associated functional venous insufficiency (OA-FVI), also called obesity-associated dependency syndrome,6,7 can lead to severe courses of the disease with pronounced venous ulcers. 8
Compression therapy for the treatment of CVI is well established in the context of classic reflux of the superficial or deep veins or of obstructions as part of a post-thrombotic syndrome.9,10 In contrast, it has not yet been studied whether compression therapy is also effective for OA-FVI. The aim of the current study was to investigate the impact of MCS on the symptoms of OA-FVI patients and to clarify whether obese patients prefer round-knit or flat-knit MCS.
Methods
Patients
In a prospective, monocentric, controlled, comparative study, 49 patients were included, aged ≥18 years with a BMI of 30 to 40 kg/m2 (rounded) and a clinical presentation of CVI in the legs corresponding to CEAP C3 to C5, who had not worn MCS in the last 3 months. The clinical presentation included edema, hyperpigmentation, erythema, dermatoliposclerosis, and stasis dermatitis. Excluded were patients with other non-obesity-related causes of CVI, such as hemodynamically relevant insufficiencies of the superficial or deep veins, detectable by duplex ultrasound, decompensated edema diseases like renal insufficiency, liver insufficiency, or heart failure, use of medication that could significantly influence the pattern of the observed symptoms (e.g., glucocorticoids above the Cushing threshold, regular use of painkillers), significant mobility restrictions up to an arthrogenic stasis syndrome, absolute contraindications for MCS, ankle-brachial-index (ABI) < 0.6, absolute ankle pressure <60 mmHg, inability to don or doff the MCS independently (possibly with assistance of devices such as rubber gloves or metal frames), or known allergies to MCS material. Additionally, patients were excluded if the maximum thigh circumference was more than two and a half times the smallest ankle circumference, or if there were abrupt caliber changes, as this would prohibit the use of round-knit MCS. An abrupt caliber change is defined as an increase in leg circumference of more than one cm within a one-cm length change. 11
The first patient was enrolled on January 17, 2019, the last patient completed the study on March 07, 2022. The test subjects were recruited from the regular consultation hours of the Vein Center of the Dermatology and Vascular Surgery Clinics of the Ruhr University Bochum. They were primarily approached by the study nurses and then also by study physicians. All examinations and data collection took place at the above-mentioned vein center. Baseline data of the patients were collected before the start of the study by means of standardized physical examinations and questionnaires. The patients’ clinical symptoms were recorded at the start and end of the study by means of physical examinations. The frequency of side effects of MCS therapy and the assessment of fit and handling of the MCS were assessed at the end of the study by means of standardized questionnaires.
The patients received no incentives for their participation in the study.
Study design and intervention
The legs of all patients were measured. During the 4-week intervention phase, they received custom-made MCS, either the flat-knit mediven® 550 or the round-knit mediven® forte, at the study center to wear at home during the day. Both MCS types were compression class II (23–32 Hg), knee-length (AD), with a closed toe, and available in caramel or black. Both products are approved as medical devices for the patient population under investigation and are commercially available.
The study was divided into three phases
During all phases, the patients documented daily their symptoms for each leg separately in a patient diary, using the German translation of the validated Varicose Veins Symptoms Questionnaire (VVSymQ) score. 12 Every day between 6 p.m. and 10 p.m., the patients documented how frequently they had noticed the symptoms of heaviness, achiness, swelling, throbbing, and itching since getting up in the morning. The six response options, which correspond to score values from 0 to 5, were: at no time, rarely, some of the time, over a long period of time, most of the time, or all the time (Supplement Table S1). The VVSymQ score is the sum of the five individual symptom ratings, therefore ranging from 0 to 25. Moreover, the patients documented the daily MCS wearing time in the diary.
Statistical analysis
The study design incorporates elements of both a controlled trial and an observational study. The primary outcome regarding the medical efficacy of MCS is based on a controlled trial. When assessing the prerequisites for the analyses (particularly residual analysis), it became evident—as expected—that the VVSymQ score of individual patients did not decrease uniformly by a constant value but rather proportionally to the baseline value (Figure S1). The commonly recommended paired t test for similar research questions would therefore be inappropriate. Instead, a proportional model (regression without an intercept) was used, as it is both statistically justified and intuitively reasonable, as well as in better alignment with medical experience. All reported p-values were calculated nominally. If necessary, consideration of multiple testing can easily be achieved by a Bonferroni correction, that is in the simplest case by multiplying the p-values by the number of tests to be considered.
On some days, some patients did not complete their VVSymQ questionnaire entries. To maximize the use of data and to ensure the best possible comparability between patients, a patient’s data was only included in a statistical analysis if complete values for the right and left leg were available from the same day for at least 5 days within a given week (referred to as “analyzable” or “sufficient” data in the results section). Unless otherwise specified, all reported VVSymQ data and results, including its five individual symptoms, are based on the mean values of the right and left leg. These, in turn, were calculated as the mean of the patient’s available data per leg over 5 to 7 days of a study week. The sample size was based on similar studies in other patient populations. 13 All statistical computations were carried out in the statistical software system R version 4.3.2 and in Excel.
Results
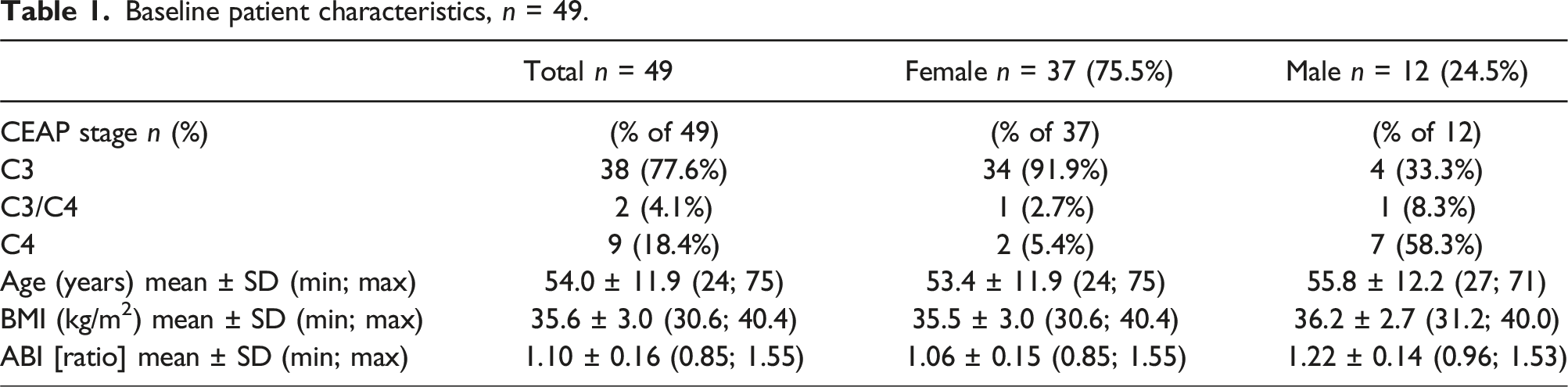
Baseline patient characteristics, n = 49.
Before the start of the MCS intervention, the mean VVSymQ score over the week varied between 0 and 19 in the 45 patients with corresponding analyzable data. The mean VVSymQ score was 6.75 (Supplement Table S2).
During the MCS intervention in weeks 2 to 5, the VVSymQ score decreased continuously and considerably, both in all analyzable patients (Supplement Table S2) and in the group of 37 patients, who consistently contributed sufficient data over all 5 weeks of the study (Figure 1 and Supplement Table S3). The strongest symptom reduction occurred immediately after the beginning of therapy in the first week of the MCS intervention. Boxplots of the weekly mean VVSymQ scores over the five study weeks (n = 37). The black horizontal bar in the boxplots represents the median, the black filled dots represent the arithmetic means, and the horizontal line connects the mean values.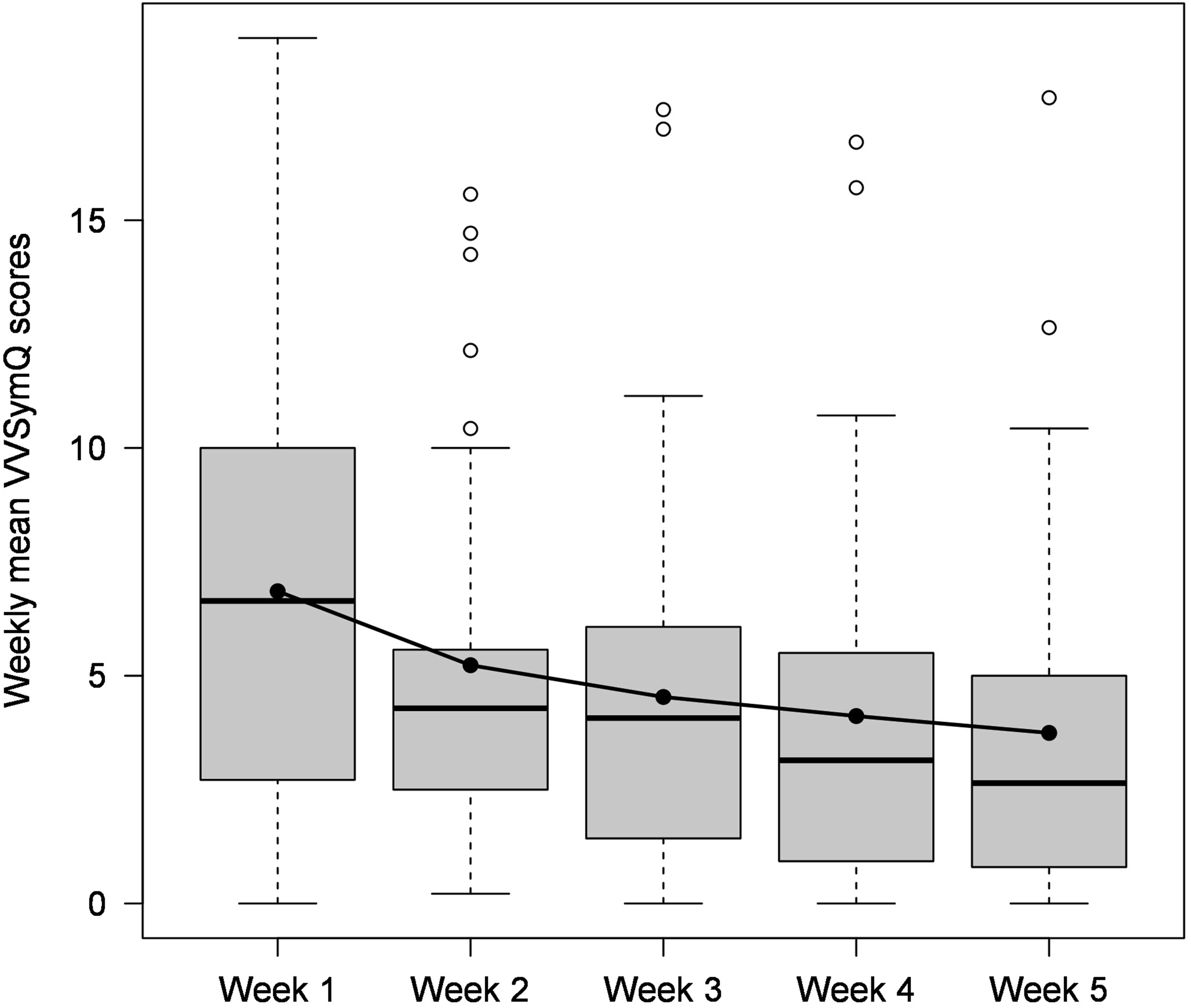
Among the 40 patients who provided sufficient data for the analysis at both baseline (week 1) and at the end of the study (week 5), one patient was symptom-free at both points in time. Among the remaining 39 patients, the VVSymQ score improved in 33 patients during the 4-week MCS wearing period. This corresponds to a success probability of 84.6% (95% CI: 71.9%, 100%; one-sided sign test: p = .000007).
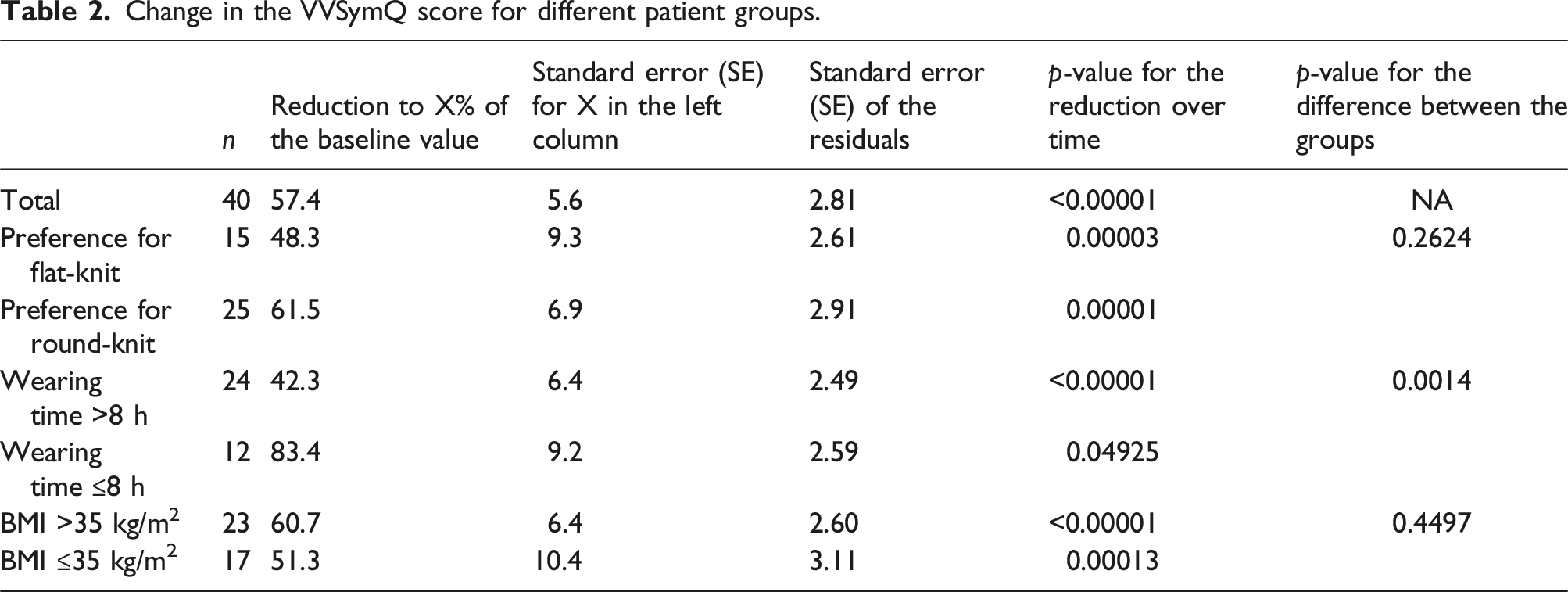
Quantitatively, the VVSymQ score for all 40 patients was reduced to an average of 57.4% of the baseline value (95% CI: 46.2%, 68.7%; one-sided test ‘proportionality factor = 100% vs proportionality factor <100%’: p < .00001).
At the beginning of the study, patients were primarily affected by the key VVSymQ symptoms swelling, heaviness, and achiness with mean values ranging from 2.03 to 1.67 on a scale from 0 to 5. Throbbing and itching were significantly less pronounced, with mean values of 0.62 and 0.47, respectively (Supplement Table S4).
During the MCS intervention in weeks 2 to 5, the symptoms swelling, heaviness, achiness, and throbbing decreased continuously and considerably, both in all participants with analyzable data in different study weeks (Supplement Table S4) and in the group of 37 patients who consistently provided sufficient data over all five study weeks (Figure 2 and Supplement Table S5). Itching was reported as slightly stronger in the first intervention week but returned to pre-intervention levels during the course of the MCS intervention. Arithmetic means of the five VVSymQ symptoms from the weekly mean ratings over the five study weeks (n = 37).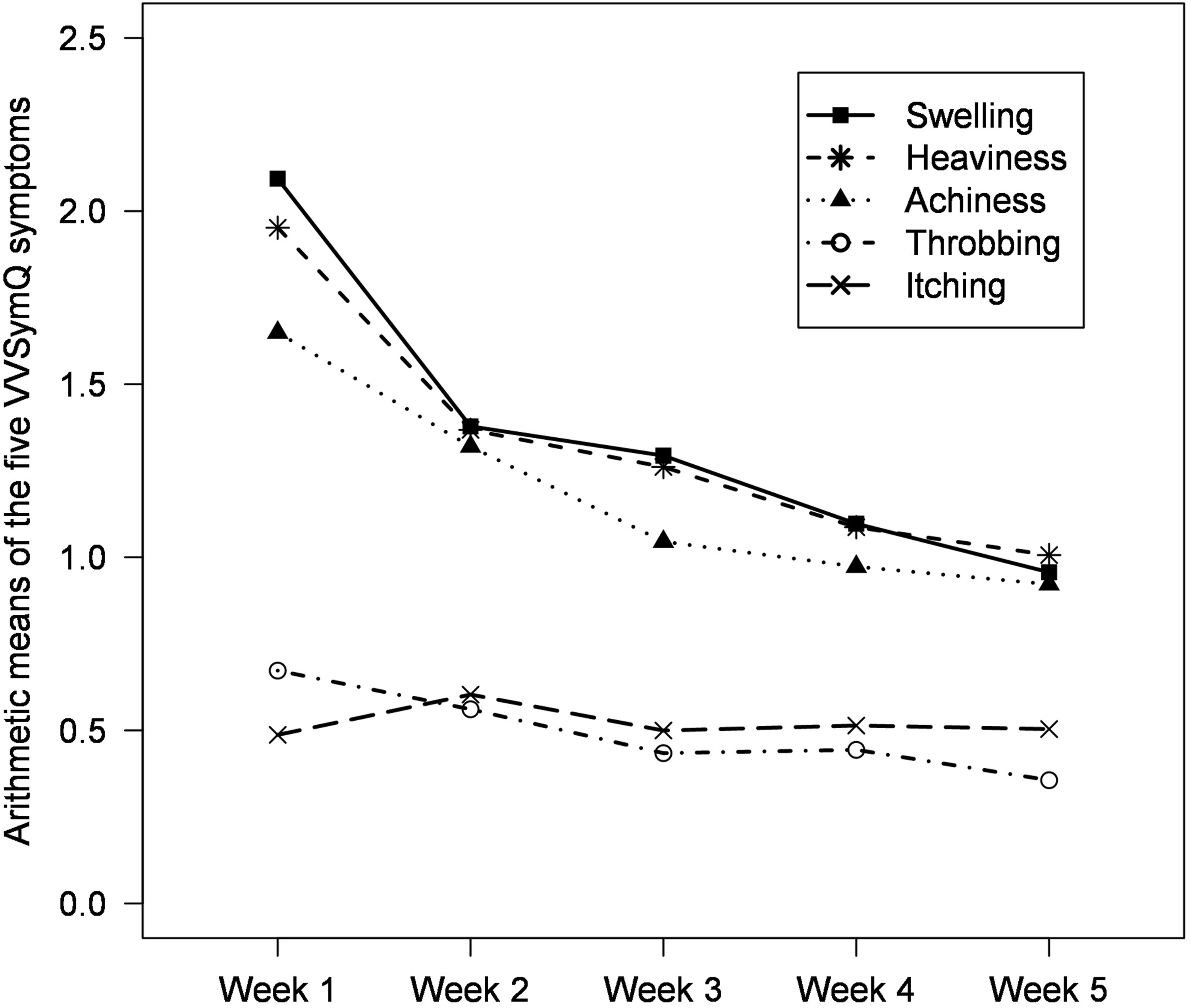
In the second week of the study, in which the patients wore flat-knit MCS on the left leg and round-knit MCS on the right leg, no systematic difference was observed between the VVSymQ scores of the two legs (Supplement Figure S2).
Following the second study week, 30 of the 49 patients chose the round-knit MCS, while 18 of the 49 patients opted for the flat-knit MCS. One patient discontinued the study in the second week due to discomfort in the area of the thigh. Patients who selected either the round- or flat-knit MCS did not differ substantially in terms of CEAP stage, gender, age, BMI, or ABI (Supplement Table S6).
Overall, the MCS were worn for an average of 9.6 hours per day over the course of the study. Patients who chose flat-knit MCS wore them on average slightly longer per day across all study weeks compared to those who chose round-knit MCS (Figure 3). Boxplots of the weekly average MCS wearing time for the 4 weeks of the MCS intervention, separated by use of flat-knit (FK) and round-knit (RK) MCS. Weekly averages based on fewer than 4 days were not considered. The black bar in the box plots represents the median, the black filled dot represents the arithmetic mean of the FK wearers, the black filled triangle the arithmetic mean of the RK wearers, the solid line connects the mean values for FK wearers, and the dashed line connects the mean values for RK wearers.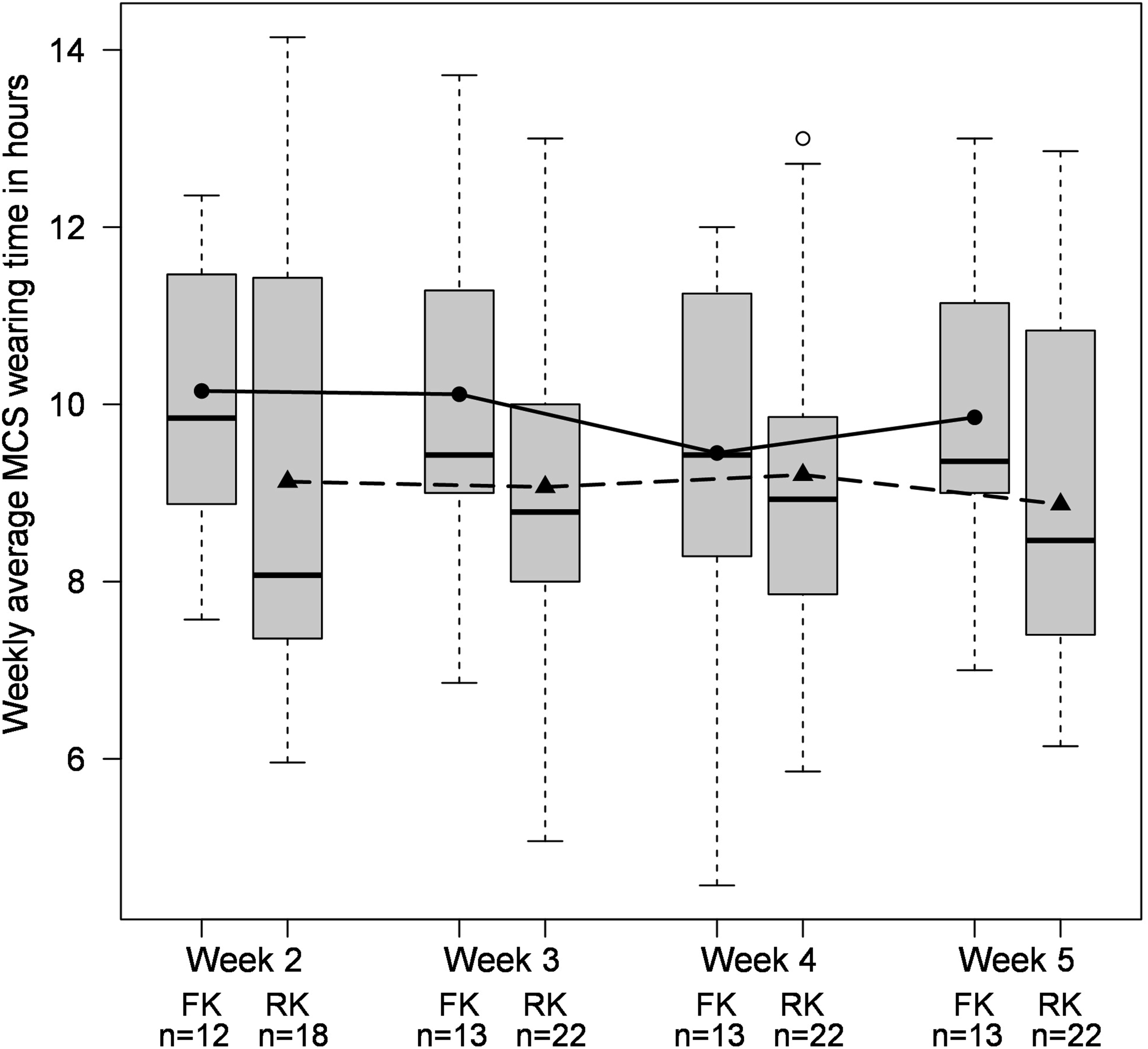
Change in the VVSymQ score for different patient groups.
Change in clinical symptoms over the course of the study.
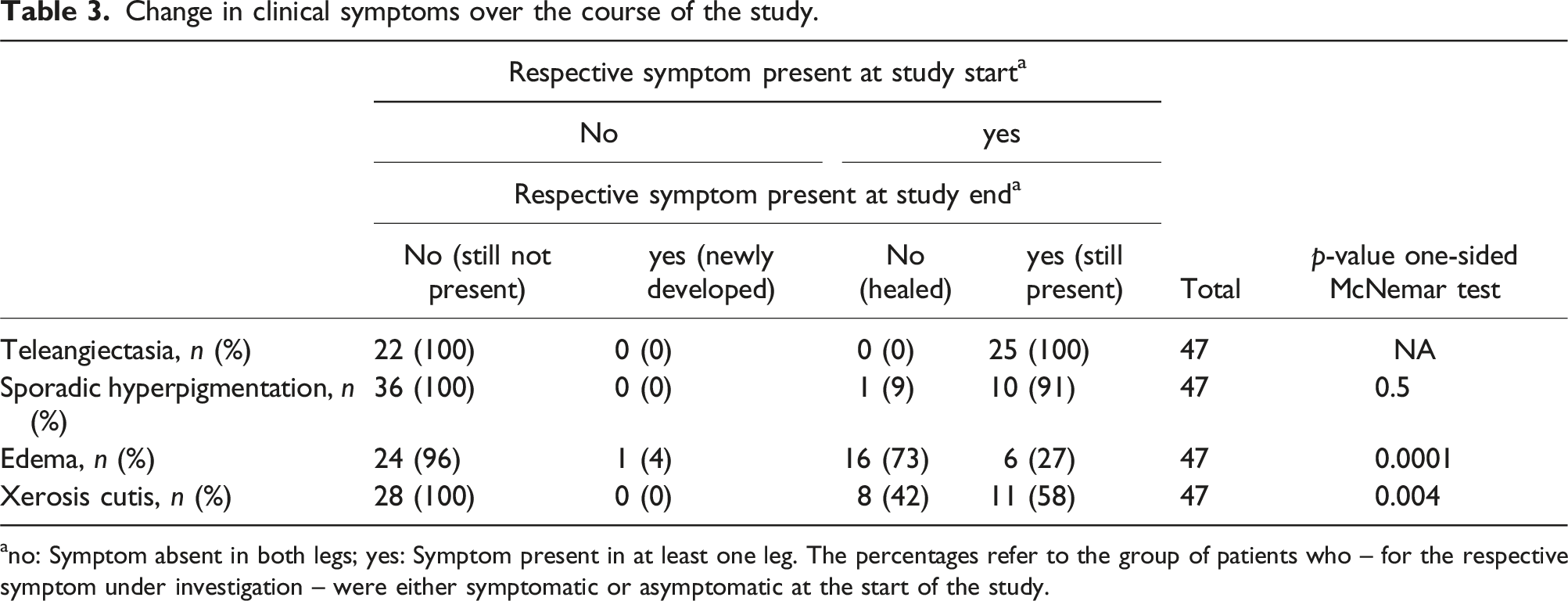
ano: Symptom absent in both legs; yes: Symptom present in at least one leg. The percentages refer to the group of patients who – for the respective symptom under investigation – were either symptomatic or asymptomatic at the start of the study.
Frequency of side effects of MCS therapy at the end of the study.
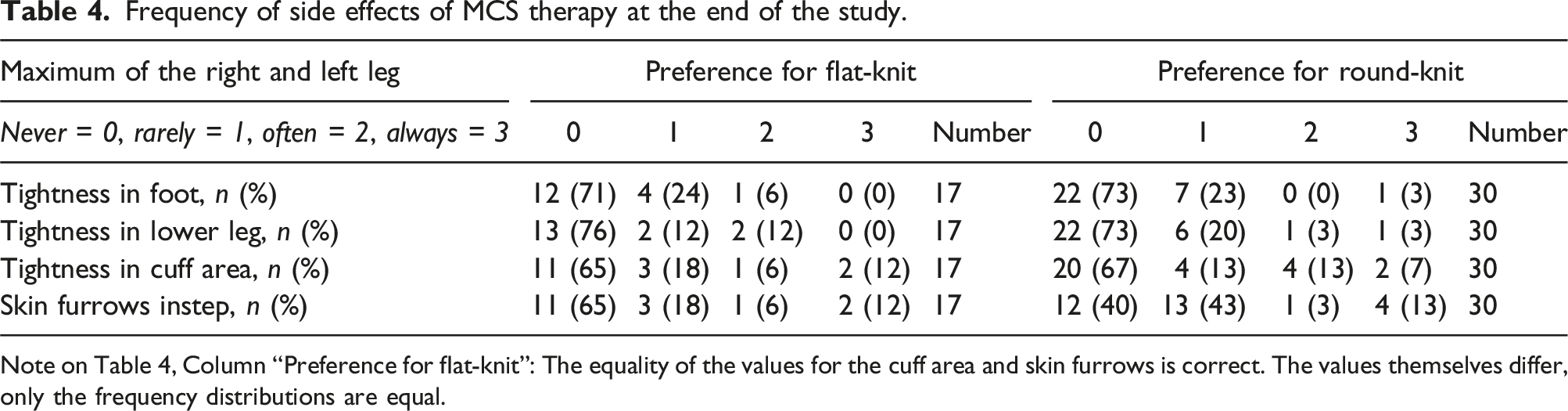
Note on Table 4, Column “Preference for flat-knit”: The equality of the values for the cuff area and skin furrows is correct. The values themselves differ, only the frequency distributions are equal.
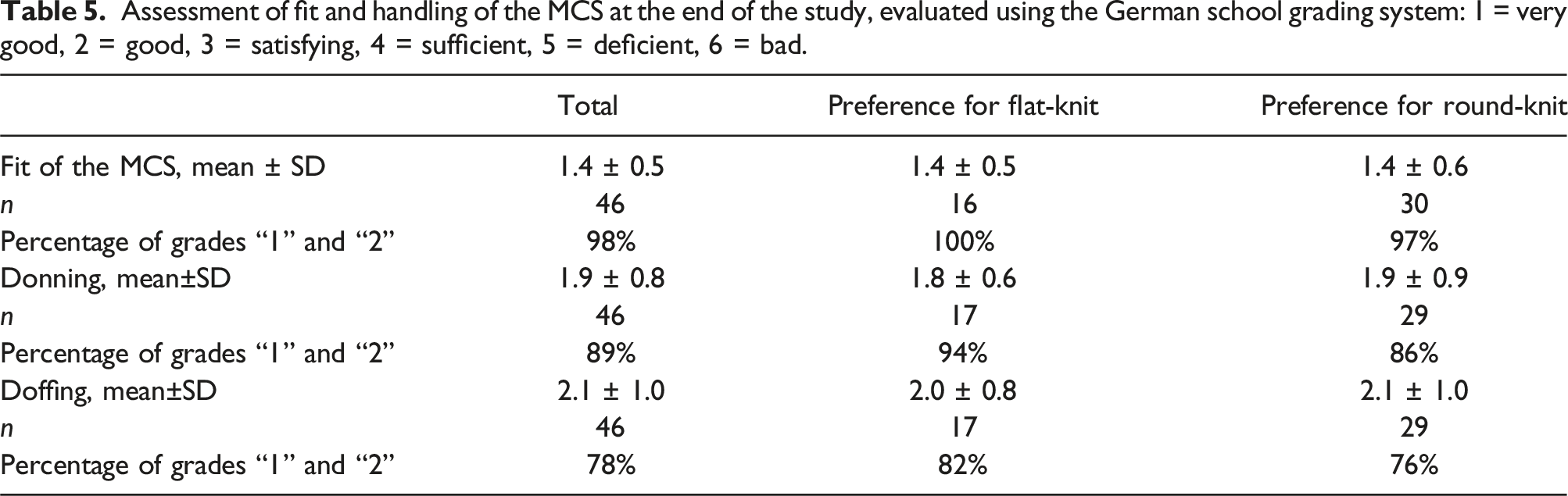
Assessment of fit and handling of the MCS at the end of the study, evaluated using the German school grading system: 1 = very good, 2 = good, 3 = satisfying, 4 = sufficient, 5 = deficient, 6 = bad.
Discussion
This study was the first to investigate the effects of compression therapy on symptoms of functional venous insufficiency in individuals with obesity. Although the leg veins of the examined obese patients showed neither reflux nor lumen narrowing, they still experienced significant symptoms under the clinical picture of CVI. These symptoms rapidly improved under compression therapy.
The prevalence of obesity in the OECD (Organization for Economic Cooperation and Development) countries is on average 19.5% and in the United States as high as 38.2%, 14 but there is hardly any evidence on the treatment of venous diseases in obese patients. 15 This is particularly true for compression therapy.
It is often argued that obese patients, due to their reduced mobility, find compression stockings difficult to handle, leading to poor compliance to compression therapy.15,16 Furthermore, a previous study found that overweight patients with a BMI ≥25 kg/m2 tended to experience compression-induced skin furrows more frequently than non-overweight patients (35.0% vs 19.2%, p = .06). 17 While obese patients have been excluded in many, if not most, studies on the treatment of venous diseases of the legs, 15 the present study now provides specific data on compression therapy in obese individuals for the first time.
The results show that 98% of obese patients rate the wearing comfort of MCS and 84% their handling as good or very good. Additionally, the obese patients experienced only very few side effects. The average wearing time ranged from 9 to just over 10 hours per day, which is comparable to a representative sample of patients with venous and lymphatic diseases in Germany, who also predominantly wear MCS daily for an average of 11 hours per day. 18 It can be assumed that the high therapy compliance was associated with the good wearing comfort and, in particular, with the very rapid and significant reduction of venous symptoms reported by the obese patients. The effects were already visible in the first week of the intervention. While the average VVSymQ score at the beginning of the study was approximately 6.8 points, the complaints had decreased to about 3.7 points by the end of the study. The key symptoms swelling, heaviness, and achiness but also throbbing, which caused the obese patients noticeably less discomfort than the other symptoms, all decreased by a similarly strong proportion. Moreover, in the majority (73%) of patients who had leg edema at the beginning of the study, the edema resolved over the course of the 4-week MCS therapy.
Skin irritations, such as xerosis cutis and itching, are commonly considered side effects of MCS. In the present study, 40% of obese patients who had not received medical compression therapy before the study showed signs of xerosis cutis. During the 4-week MCS therapy, this condition healed in nearly half (42%) of those affected, while no new cases of xerosis cutis developed among those who were unaffected at the start of the study.
Itching, one of the five clinical symptoms assessed in the VVSymQ score, was reported as mild by patients both at the beginning and the end of the study.
This finding is remarkable given that obesity is often associated with impaired epidermal barrier function. This impairment manifests in a significantly increased transepidermal water loss and an increased tendency to erythema compared to individuals with normal weight, 19 clinically leading to an increased prevalence of dry skin 20. Additionally, the plantar hyperkeratoses frequently observed in obese individuals 21 did not result in any limitations of compression therapy in this study.
Among the obese patients included in the study, 62.5% chose round-knit MCS, while 37.5% opted for flat-knit MCS. Obese patients with abrupt caliber changes, who can only be treated with flat-knit MCS, were not included in the study to allow for a direct comparison between the two types of MCS. Both round-knit and flat-knit MCS proved to be effective. A correlation was observed between the extent of VVSymQ reduction and the duration of MCS wear. Patients who wore their MCS for an average of more than 8 hours per day achieved a considerably greater reduction in symptoms.
Due to visceral fat tissue, obese patients may experience functional impairments in venous drainage instead of hemodynamically relevant venous insufficiencies, such as valve dysfunction. In OA-FVI, the visceral fat tissue masses cause obstruction of the groin veins, which subsequently leads to increased intravascular pressure in the lower extremity. A BMI of 25 kg/m2 already may result in a pressure of 20 mmHg in the groin fold, which in turn affects the pressure conditions in the peripheral veins of the extremity. With a further increase in BMI, the pressure in the groin fold and in the venous system of the lower extremity also rises. Due to the increased intravascular pressure in the venous system of the lower extremity, the blood flow velocity decreases, resulting in a reduced venous drainage. 22 Compression therapy reduces the diameter of the vessels and thus improves venous drainage, as the venous valves can close better again and act as backflow valves. The improved venous outflow reduces the transmural pressure in the veins of the extremities and reduces existing edema in the legs, as the veins have more capacity to absorb tissue fluid and transport it to the heart. This improved venous function may also explain the improvement in VVSymQ symptoms.23,24
These findings are highly relevant to clinical care, as obesity is a widespread condition, and prolonged, untreated venous insufficiency can lead not only to subjective discomfort but also to the development of CVI-typical complications such as edema, hyperpigmentation, dermatoliposclerosis, erysipelas, atrophie blanche, impaired wound healing, or ulcers.6,22,25 Furthermore, obesity is an independent risk factor for thrombosis,26,27 which can also be effectively prevented with compression therapy. 9
A limitation of the study is that it is not a randomized controlled trial, as the main analysis is based on an intraindividual comparison in which each participant’s own pre-intervention data represents the control data. Another limitation is that our study was restricted to obese patients with a BMI between 30 and 40 kg/m2, so that we cannot say whether patients with a higher BMI benefit as much as the group studied. This restriction was made deliberately, as the risk of special individual body shapes increases with the severity of obesity, which can no longer be treated with the round-knit technique. A fair comparison between the two MCS types would therefore no longer have been possible. Furthermore, the prevalence of additional obesity-associated lymphedema increases with the severity of obesity, which should be specifically treated with flat-knit according to guideline recommendations 28 and expert opinions. 29 Apart from this, however, the study results can be largely generalized, as the patients wore the MCS in their home environment, there were very few dropouts and compliance was high, although we did not offer any incentives to the study participants.
Conclusion
The complaints and symptoms of obesity-associated functional venous insufficiency can be treated effectively and with few side effects using MCS. The effects are immediate, occurring within the first week of wear. Swelling, heaviness, achiness and throbbing are reduced. With an average daily wearing time of between 9 and just over 10 hours, compliance to compression therapy in obese patients is not lower than in the normal population. Some patients prefer round-knit, others flat-knit, both MCS are medically effective. The assessment of the MCS in the obese patients with a BMI of 30–40 kg/m2, is predominantly good or very good in terms of both wearing comfort and handling. The results are highly relevant for the treatment of obesity and venous disease, as prolonged, untreated venous insufficiency can lead to serious complications such as erysipelas, wound healing disorders or ulcerations in addition to the subjective symptoms.
Supplemental Material
Supplemental Material - Medical compression stockings reduce the symptoms of obesity-associated functional venous insufficiency
Supplemental Material for Medical compression stockings reduce the symptoms of obesity-associated functional venous insufficiency by Markus Stücker, and Walter Olbricht in Phlebology.
Footnotes
Acknowledgements
The authors thank Stefanie Reich-Schupke, PhD, Vein Centre of the Departments of Dermatology and Vascular Surgery, Katholisches Klinikum Bochum, Bochum, Germany, for the initial study concept.
Author contributions
MS researched literature, conceived the study, developed the protocol, gained ethical approval, recruited the patients and wrote the manuscript. WO conducted the statistical analysis of the data. Both authors approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MS has received consulting fees from Bauerfeind AG and URGO GmbH and speaker fees from Juzo GmbH and URGO GmbH. WO has received a consulting fee from Katholisches Klinikum Bochum gGmbH.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by medi GmbH & Co. KG.
Guarantor
MS.
Ethical statement
Data Availability Statement
Raw data were generated at vein centre of Ruhr-University Bochum. Derived data supporting the findings of the study are available from the corresponding author on request.
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.