
Abstract
Background
The effectiveness of compression therapy (CT) and the best compression modality choice are questioned in many clinical stages of chronic venous disease (CVD). This work aims to obtain information on indications, contraindications, and the best treatment option for CT in different clinical scenarios of CVD.
Method
An online survey was made among members of the International Compression Club, experts in CT.
Results
The experts apply CT in all clinical stages of CVD, even when evidence is missing. Regarding compression materials, experts use inelastic materials in the advanced stages of CVD and compression stockings in the early or chronic stages of CVD.
Conclusion
The authors highlight the gap between experts’ practical use of CT and evidence-based medicine results. They also suggested that, given the cost of randomized clinical trials aimed at specifying specific indications for different devices, artificial intelligence could be used for large-scale practice surveys in the future.
Introduction
Compression therapy (CT) still needs to be well-defined as a therapeutic procedure. In many published papers, the applied material is not explicitly described, inclusion and exclusion criteria according to indications and contraindications are not well defined, and side effects are rarely reported.
This work aims to report the data set of an online survey to have a snapshot on what clinical scenarios (not only chronic venous disease [CVD]) are considered an indication for CT, what compression materials are used in the different situations, what are considered the contraindications to CT, and what are the main side effects of this treatment.
Methods
The survey was conducted in the period from 15.10.2021 to 25.04.2022 by using LimeSurvey among members of ICC - International Compression Club with the organization support of Lohmann&Rauscher® (Lohmann & Rauscher GmbH & Co KG, Neuwied; Germany).
Population
International Compression Club is a scientific society specifically focused on CT, gathering experts in CT from the medical field and the industry. The admission to ICC of members coming from the medical field is based on a curriculum vitae (CV) proving their practice and/or interest in CT in their daily activity. The great majority of them are phlebologists or vascular surgeons. The other members, nurses and physiotherapists, work in vascular or dermatologic departments treating patients with vascular diseases or in trauma department. The survey was carried out only among experts from the medical field to avoid conflicts of interest. The questionnaire was sent to 116 ICC members who declared in their CV to have a vast experience in applying CT. When asked how long they have been working with compression devices, they all responded to have at least 5 years of experience. The majority of them (>64%) have been working with CT for more than 20 years. None of participants disclosed any conflict of interest. A total of 61 out of 116 members (53%) provided their input in the survey. These experts represent a view coming from 28 countries all over the world. The majority (thirty-three) come from Europe, one from China, South Africa, Turkey, and Afghanistan, two from Egypt and Australia, four from Japan and South America, and nine from North America. Three did not specify their country. Therefore, the results of this survey give an exciting summary of experts’ opinions on the use of CT.
Survey questions
The experts were asked to report what kind of population received CT, in what indications they use CT, what kind of material they use in the different indications, if they had additional indications in addition to those already reported in the survey, contraindications and side effects of CT, and finally they were asked to rate their general assessment on CT concerning performance, safety, ease of use, and comfort (Appendix).
In order to make the reading of this paper easier, MCS stands for medical compression stockings, EBs for elastic bandages, IBs for inelastic bandages (including adhesive and cohesive bandages, multilayer multicomponent bandages, and zinc paste bandages), ACWs for adjustable compression wraps, and experts for the participants to this survey.
Results
The patients submitted to CT were >18 years old: adults were considered patients in the age range 18–65 years (48%), while elderly patients were >65 years old (43%). Only 9% of patients submitted to CT were <18 years old.
The results are given in the percentage of responders. Decimals up to 0.5 were rounded to the lower value and decimals >0.5 to the higher value. The responses that were not clear, raising doubts about the choice of the responders, were classified as “other” or “uncertain.” Not all the participants responded to all the questions, which was reported.
Indications
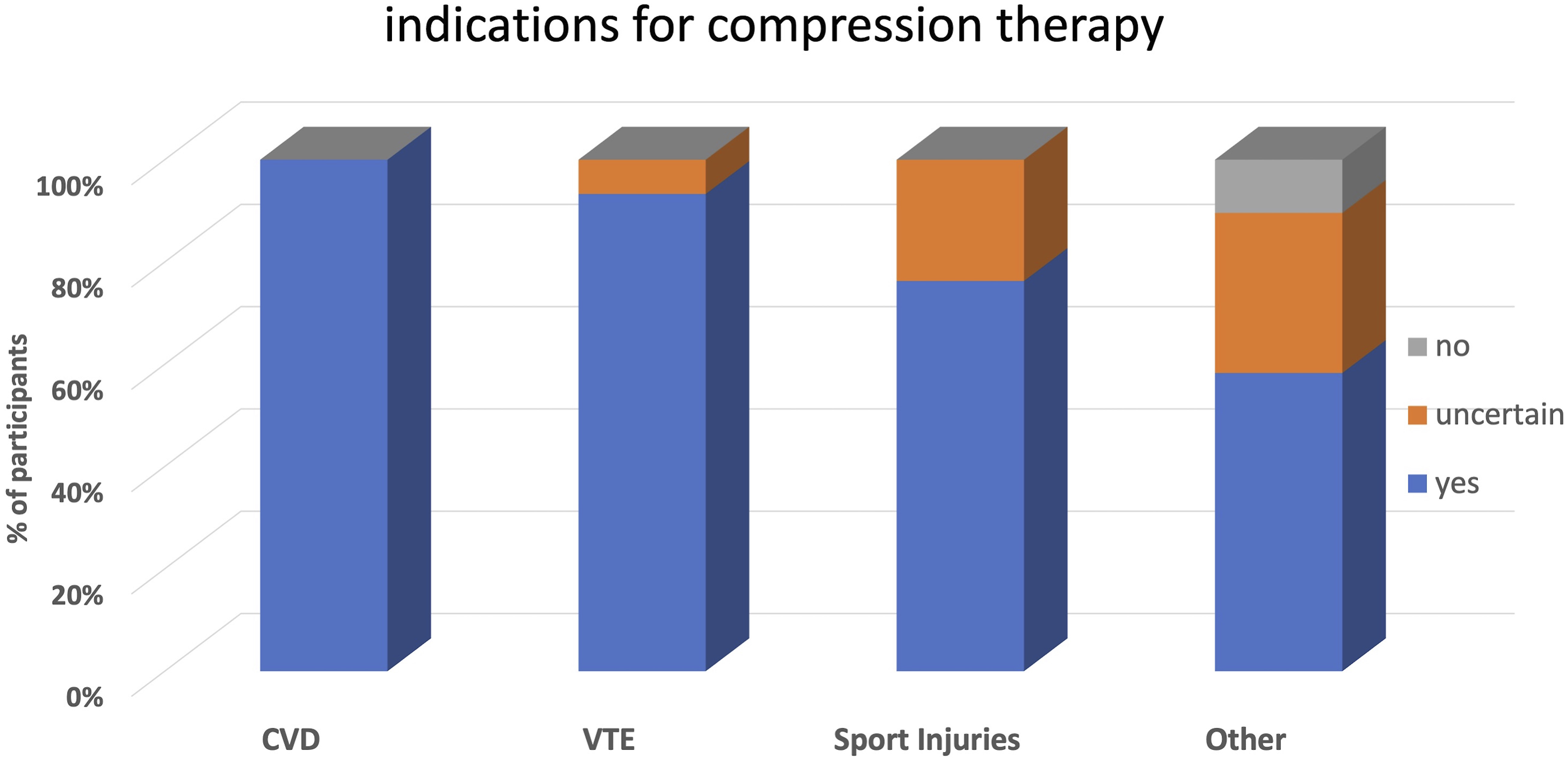
• All the experts (100%) agree that CT is indicated to treat symptoms in the different stages of CVD. • 93% apply compression in thromboembolic disease. • 76% apply CT in sports injuries. For this indication, 24% of responses were unclear and, therefore, classified as “uncertain” (Figure 1). Indications for compression therapy as stated by participants (%).
Compression devices mostly used in different indications
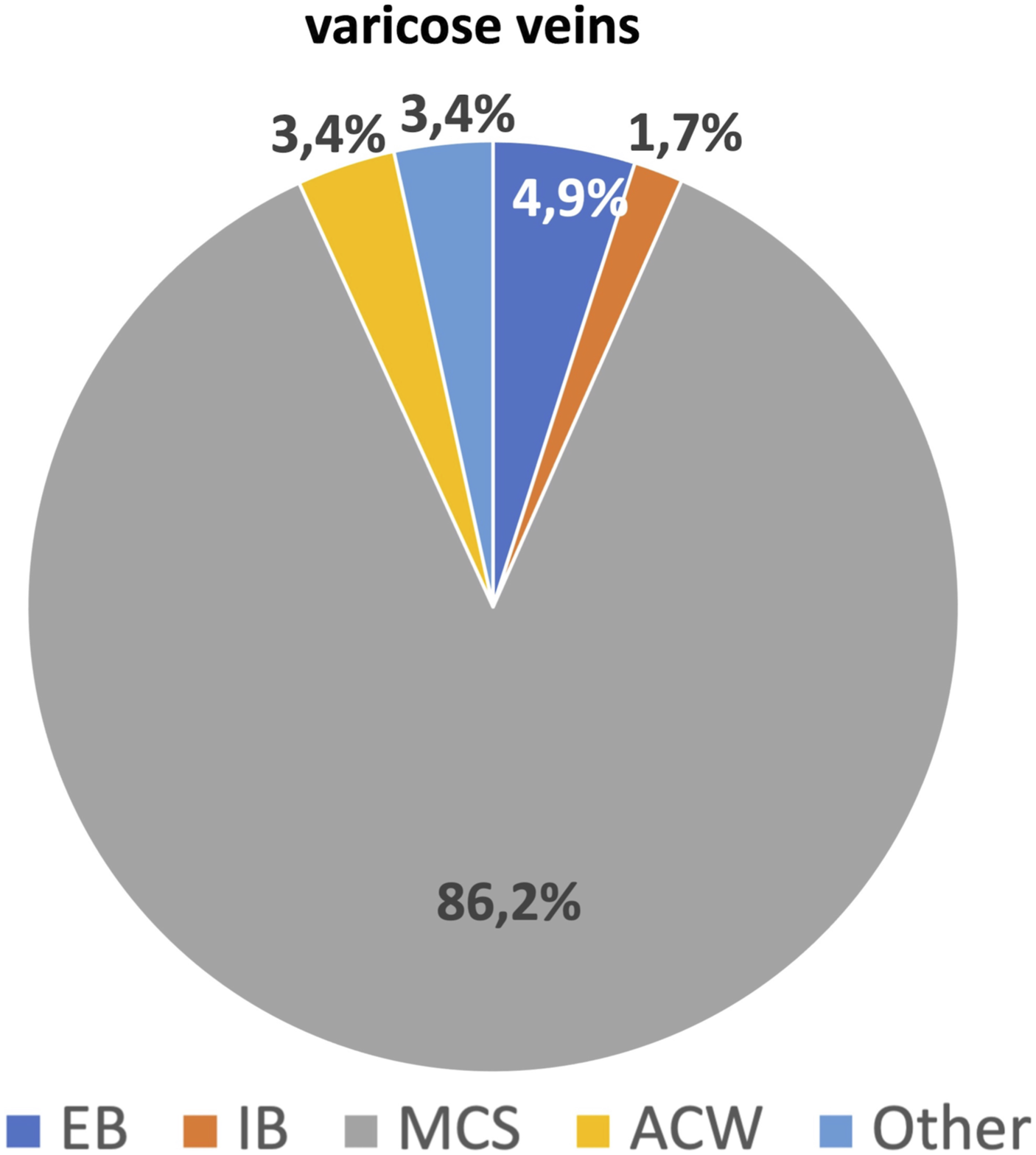
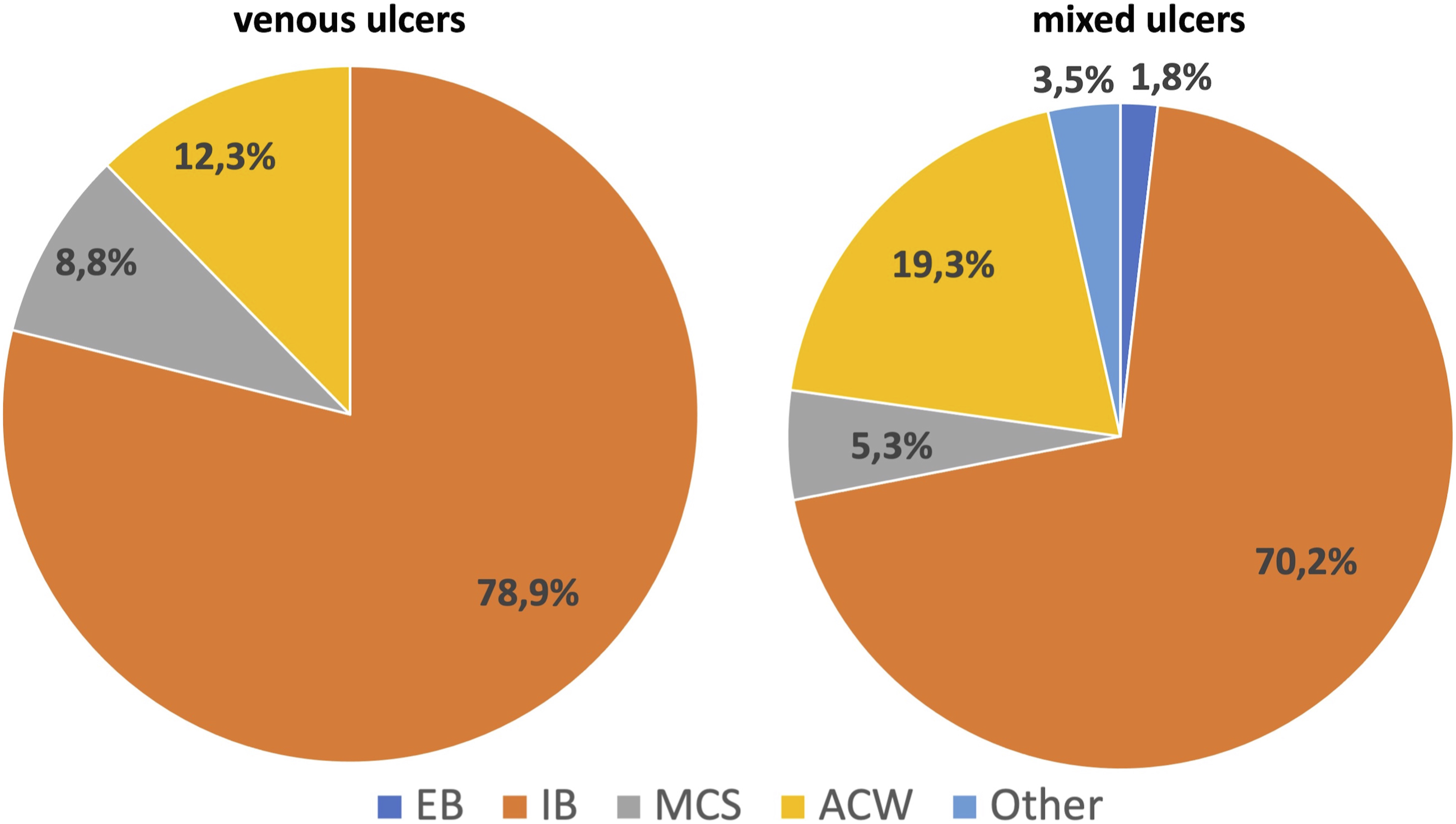
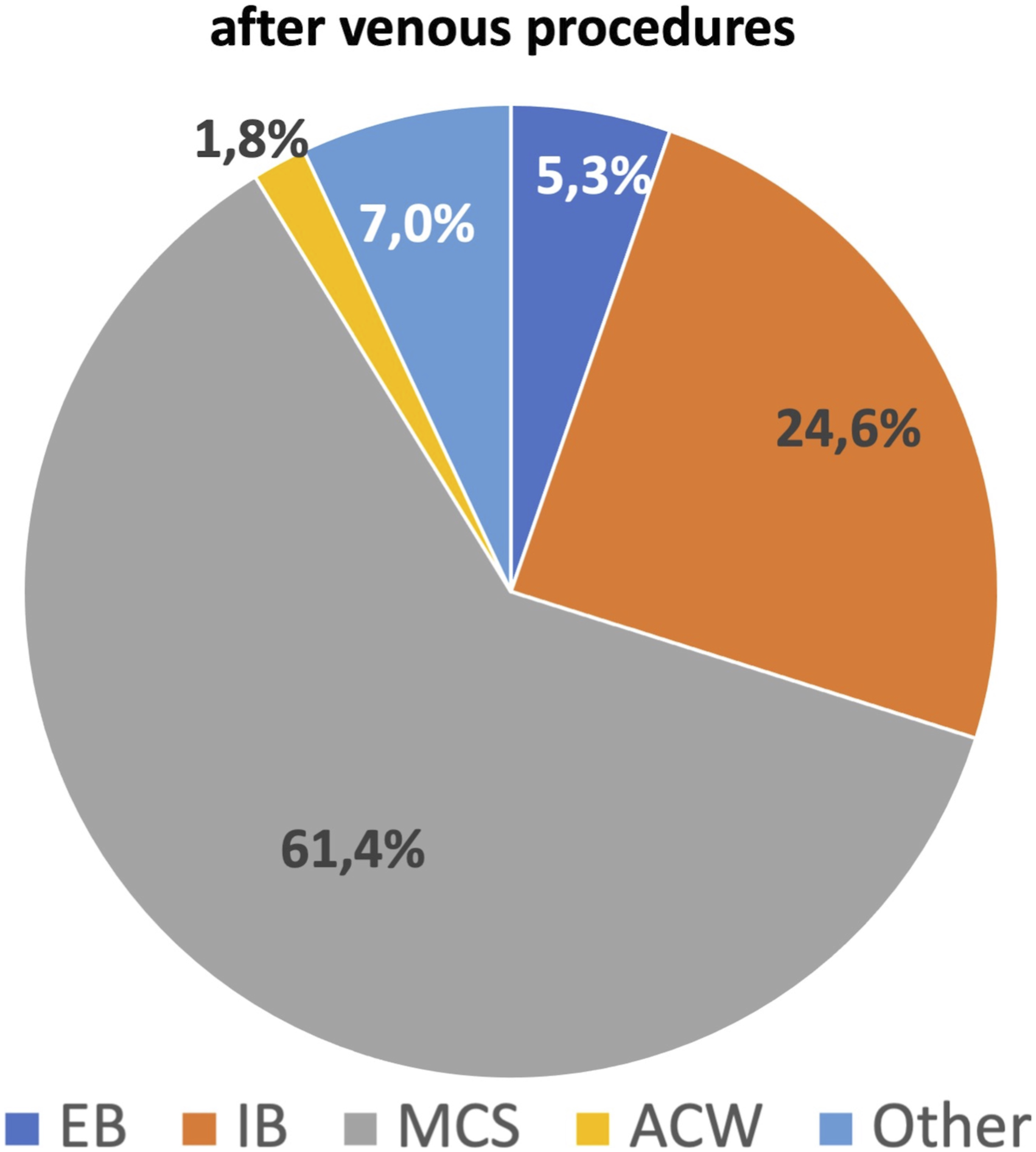
⁃ Symptomatic varicose veins: 86% of experts apply MCS. The remaining 14% apply EB (5%), IB (2%), ACW (2%), and other (5%) (Figure 2). ⁃ CEAP C3-C5: 63% apply MCS and 27% apply IB (15%), ACW (10%), or other (2%). ⁃ Venous leg ulcers (VLU): 79% apply IB, 12% ACW, and 9% MCS. ⁃ Mixed ulcers: 75% apply IB, 19% ACW, 3% MCS or EB, and 3% other (Figure 3). ⁃ Post-procedures (surgery and chemical or physical endovascular procedures): 61% apply MCS. The remaining 39% apply EB (5%), IB (25%), ACW (2%), or other (7%) (Figure 4). Types of compression devices used in varicose veins. EBs: elastic bandages; IBs: inelastic bandages; MCSs: medical compression stockings; ACWs: adjustable compression wraps. Types of compression devices used in venous and mixed ulcers. EBs: elastic bandages; IBs: inelastic bandages; MCSs: medical compression stockings; ACWs: adjustable compression wraps. Types of compression devices used after venous procedures. EBs: elastic bandages; IBs: inelastic bandages; MCSs: medical compression stockings; ACWs: adjustable compression wraps.
More detailed information was asked for edema treatment, thromboembolic disease, and sports injuries.
Leg edema
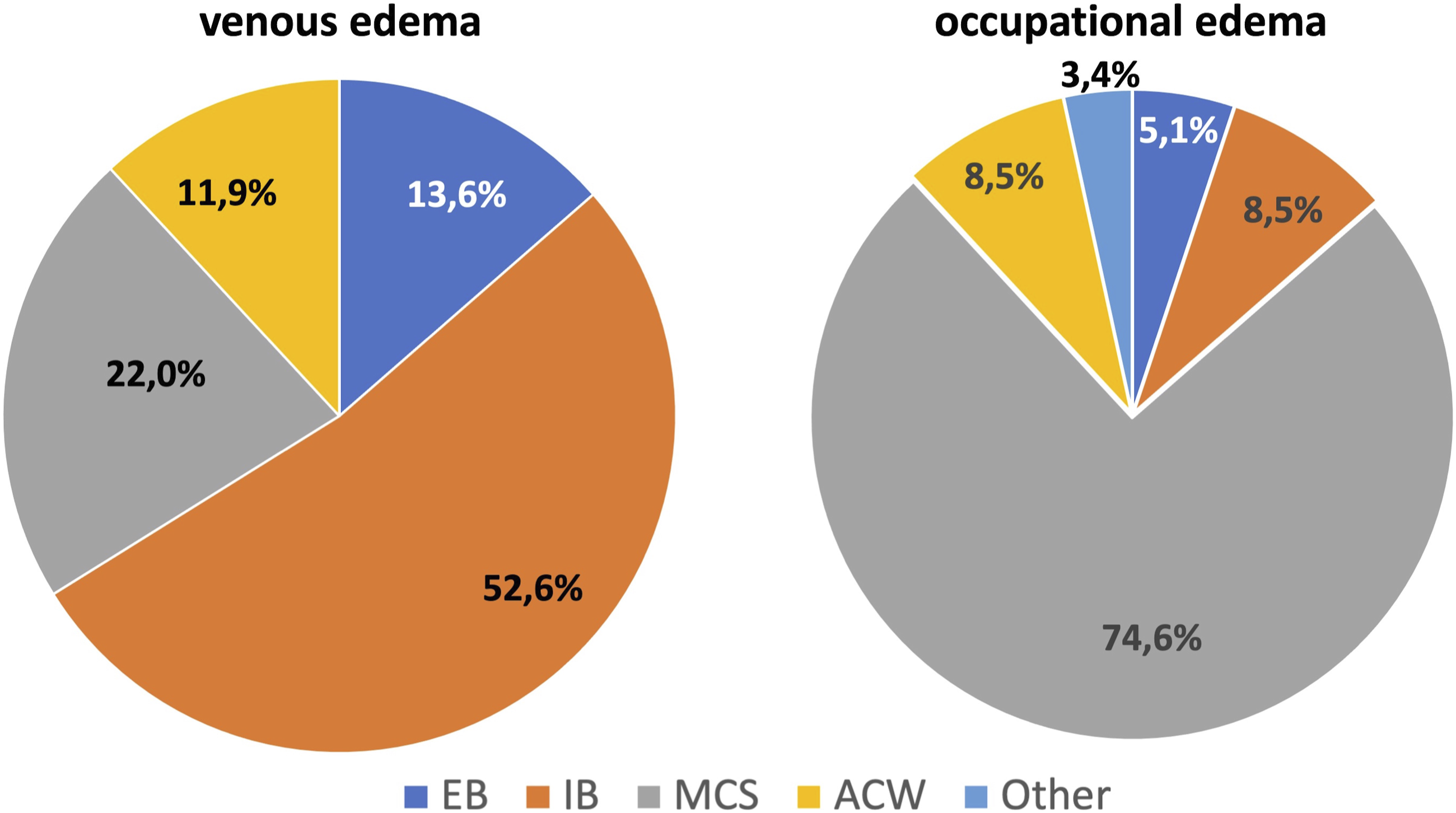
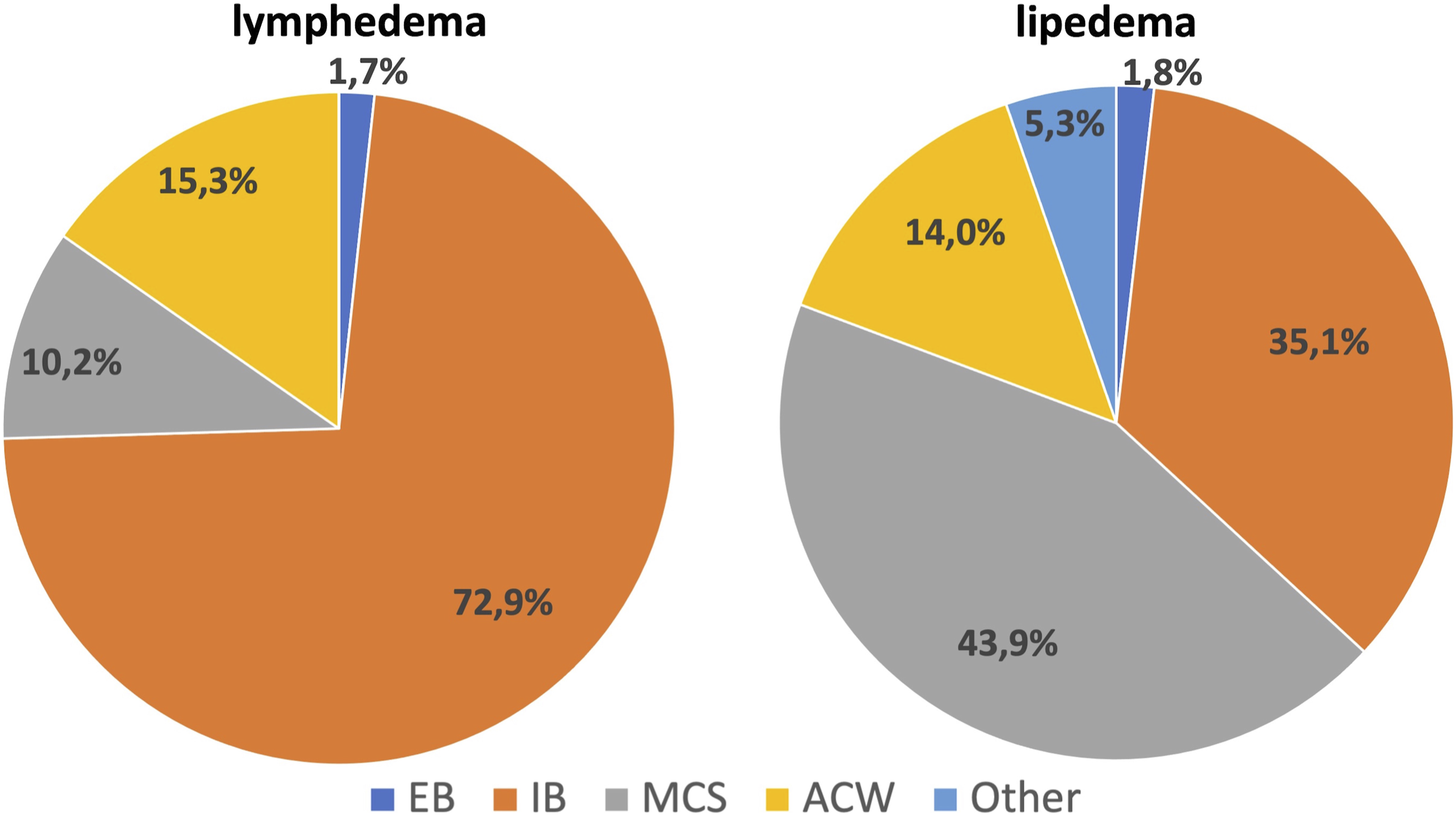
⁃ Venous edema: 52% of medical experts apply IB, 14% EB, 22% MCS, and 12% ACW. ⁃ Occupational edema: 75% apply MCS, 5% EB, 5% IB, 10% ACW, and 5% other (Figure 5). ⁃ Lymphedema: 73% apply IB, 15% ACW, 10% MCS, and 2% EB. ⁃ Lipedema: 44% apply MCS, 35% IB, 14% ACW, 2% EB, and 5% other (Figure 6). ⁃ Post-traumatic edema: 59% apply IB, 15% MCS, 12% EB, 10% ACW, and 4% other. ⁃ Post-operative edema: 47% apply IB, 24% MCS, 17% EB, 7% ACW, and 5% other. ⁃ Edema in pregnancy: 82% apply MCS, 8% IB, 3% elastic bandages, 2% ACW, and 5% other. Types of compression devices used in venous edema and occupational edema. EBs: elastic bandages; IBs: inelastic bandages; MCSs: medical compression stockings; ACWs: adjustable compression wraps. Types of compression devices used in lymphedema and lipedema. EBs: elastic bandages; IBs: inelastic bandages; MCSs: medical compression stockings; ACWs: adjustable compression wraps.
Thromboembolic disease
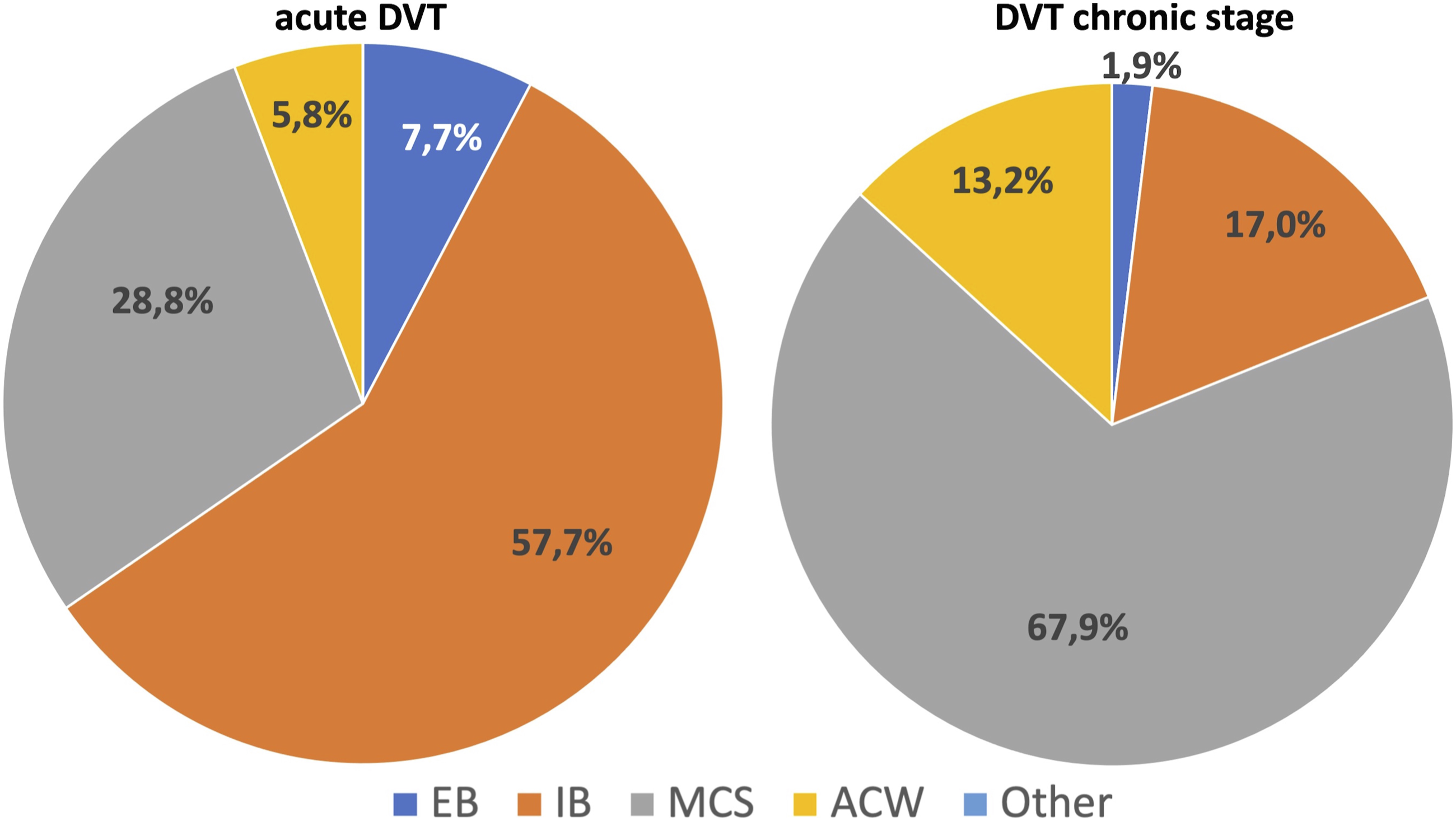
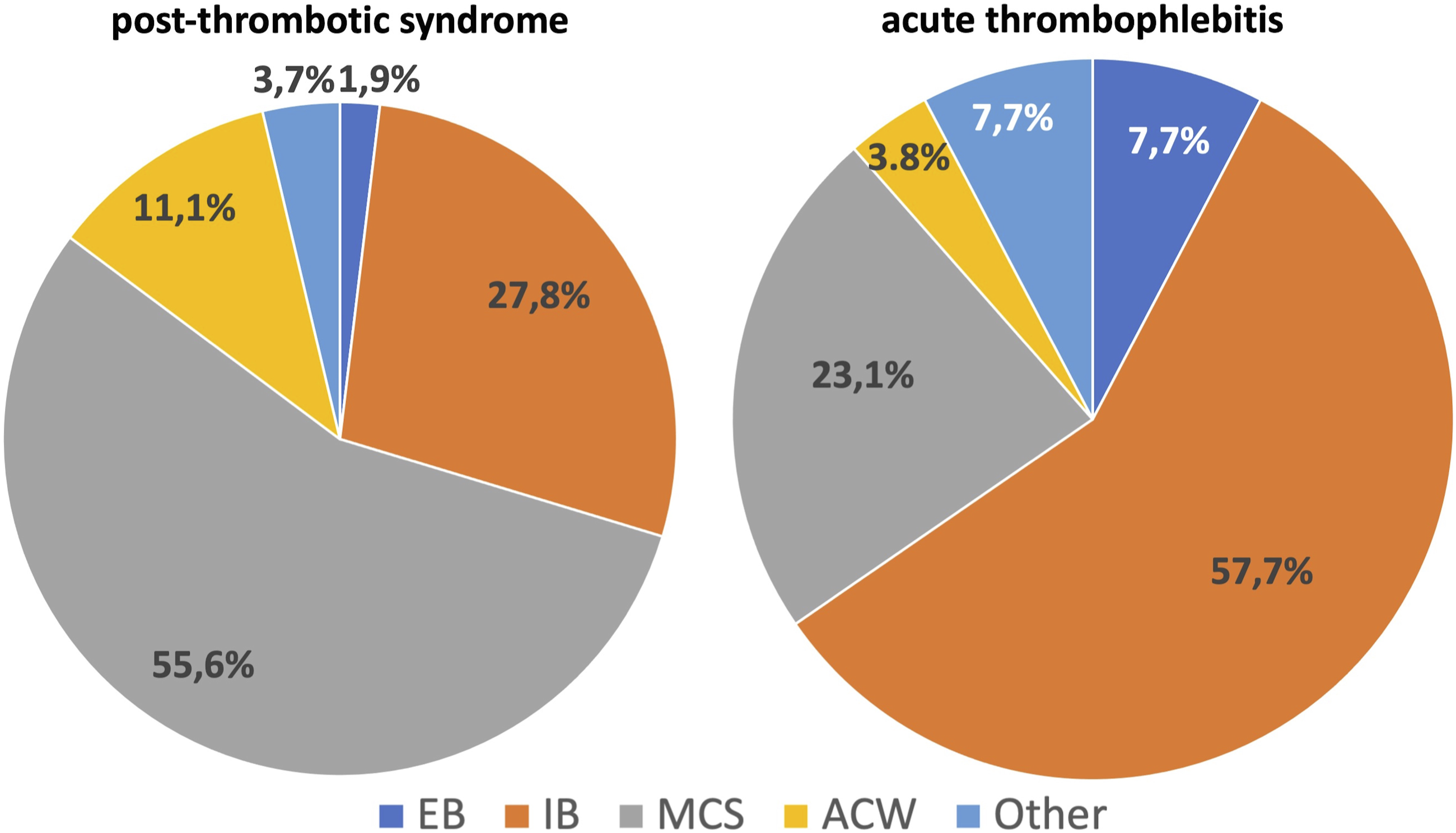
• Acute deep vein thrombosis: 57% apply IB, 29% MCS, 8% EB, and 6% ACW. ⁃ Deep venous thrombosis in chronic stage: 68% apply MCS, 13% IB, 13% ACW, 2% EB, and 4% other (Figure 7). ⁃ Post-thrombotic syndrome: 56% apply MCS, 27% IB, 11% ACW, 2% EB, and 4% other (Figure 8). ⁃ Thromboprophylaxis in ambulatory patients: 85% apply MCS, 4% IB, 4% EB, 6% ACW, and 1% other. ⁃ Superficial venous thrombosis: 57% apply inelastic bandages, 23% MCS, 8% elastic bandages, 4% AVW, and 8% other (Figure 8). Types of compression devices used in acute deep venous thrombosis and in its chronic stage. EBs: elastic bandages; IBs: inelastic bandages; MCSs: medical compression stockings; ACWs: adjustable compression wraps. Types of compression devices used in post-thrombotic syndrome and in acute thrombophlebitis. EBs: elastic bandages; IBs: inelastic bandages; MCSs: medical compression stockings; ACWs: adjustable compression wraps.
Sport and traumatic injuries
⁃ Contusions: 60% apply IB, 30% EB, 8% MCS, and 2% other. ⁃ Sprains: 31% apply EB, 54% IB, 5% MCS, 5% ACW, and 5% other compression devices. ⁃ Tendon injuries: 70% apply IB, 10% EB, 5% MCS, 8% ACW, and 8% other compression systems. ⁃ Joint dislocations: 53% apply IB, 21% EB, 5% MCS, 5% ACW, and 16% “Other.” ⁃ Healed fractures: 46% apply MCS, 18% IB, 14% EB, 13% ACW, and 9% “Other.”
Additional indications
• Revascularization edema that is to be treated by inelastic bandages. • Blunt injuries that are to be treated by inelastic bandages. • Vasculitis that is to be treated by MCS. • Cellulitis. • Edema caused by systemic disease (cardiopathies and renal disease) without a clear indication of what compression device has to be applied.
Absolute and relative contraindications (CIs)
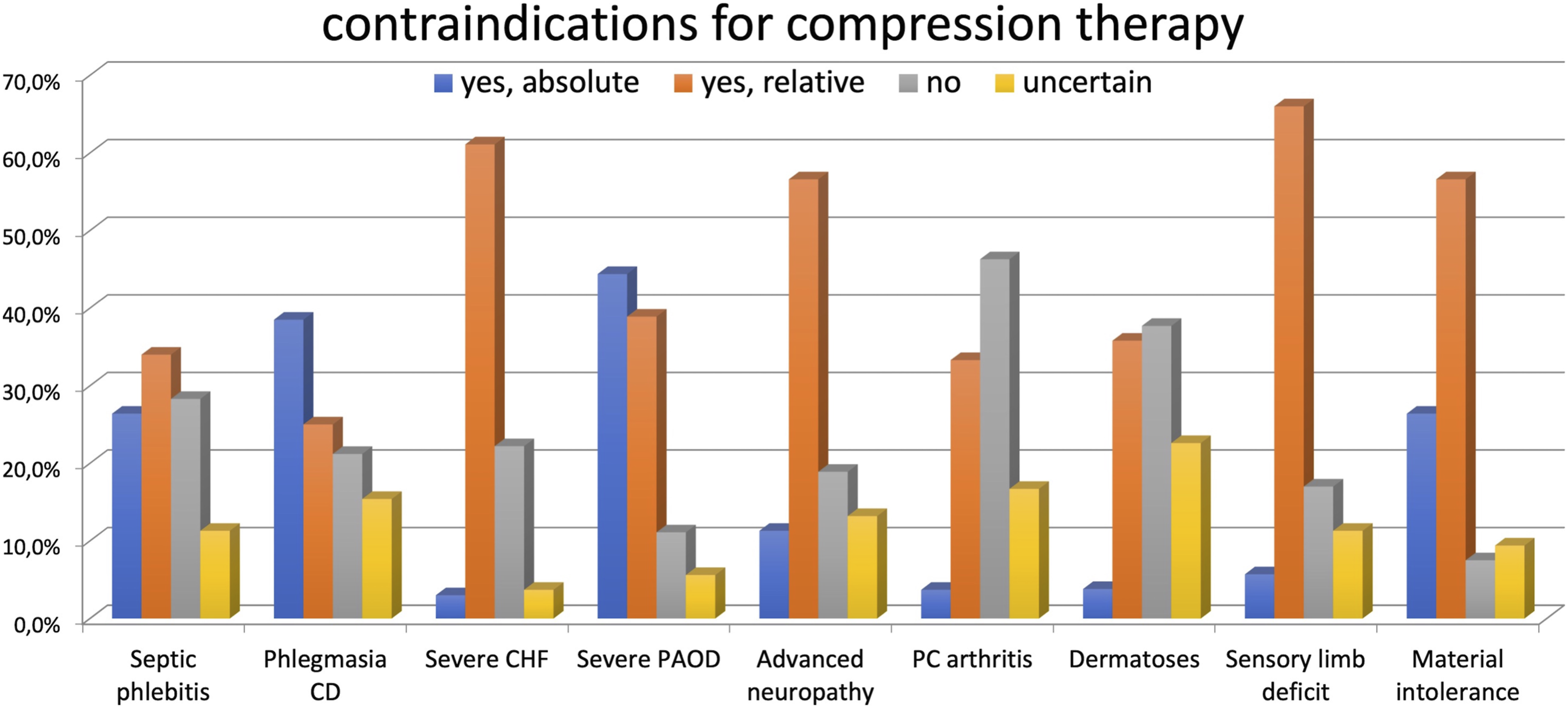
⁃ Septic phlebitis: absolute for 26% of the medical experts, relative for 34%, and not a CI for 29%. 11% were unsure about this CI (Figure 9). ⁃ Phlegmasia cerulea dolens: absolute for 38%, relative for 25%, and not a CI for 22%. 15% were unsure about this CI. ⁃ Congestive heart failure: absolute for 13%, relative for 61%, not a CI for 22%, while 4% were unsure this is a CI. ⁃ Advanced peripheral arterial occlusive disease: absolute for 44%, relative CI for 39%, and not a CI for 11%. 6% were unsure concerning this CI. ⁃ Advanced peripheral neuropathy: absolute for 11%, relative for 57%, not a CI for 19%, while 13% were unsure about this CI. ⁃ Sensory disturbance of the limb: absolute for 6%, relative for 66%, not a CI for 17%, while 11% were unsure about this CI. ⁃ Primary chronic arthritis: absolute for 4%, relative for 33%, and not a CI for 47%. 16% were unsure regarding this CI. ⁃ Concomitant dermatoses: absolute for 4%, relative for 36%, and not a CI for 38%. 22% were unsure regarding this CI. ⁃ Intolerance to the material: absolute for 27%, relative for 57%, it is not a CI for 8%, while 9% are unsure regarding this CI. Contraindications for compression therapy. Phlegmasia CD: phlegmasia cerulea dolens; CHF: chronic heart failure; PAOD: peripheral arterial occlusive disease; PC arthritis: primary chronic arthritis.
Additional CI
⁃ Superficial bypass; ⁃ pain ⁃ cellulitis in venous and lymphatic disease; and ⁃ elastic material was considered contraindicated in all the acute phases of venous disease, where inelastic material should be preferred, moving to MCS in the maintenance phase.
Side effects
The following side effects were reported by applying compression devices: ⁃ Allergies or skin irritations. Can occur: 68% of the experts; cannot occur: 9%. 23% did not respond. ⁃ Strangulation and pressure marks. Can occur: 63%; cannot occur: 15%. 22% did not respond. ⁃ Necrosis. Can occur: 51%; cannot occur: 18%. 31% did not respond. ⁃ Pressure damage on the peripheral nervous system. Can occur: 48%; cannot occur 21%. 31% did not respond.
Additional side effects
⁃ Itching.
General assessment rating
Performance
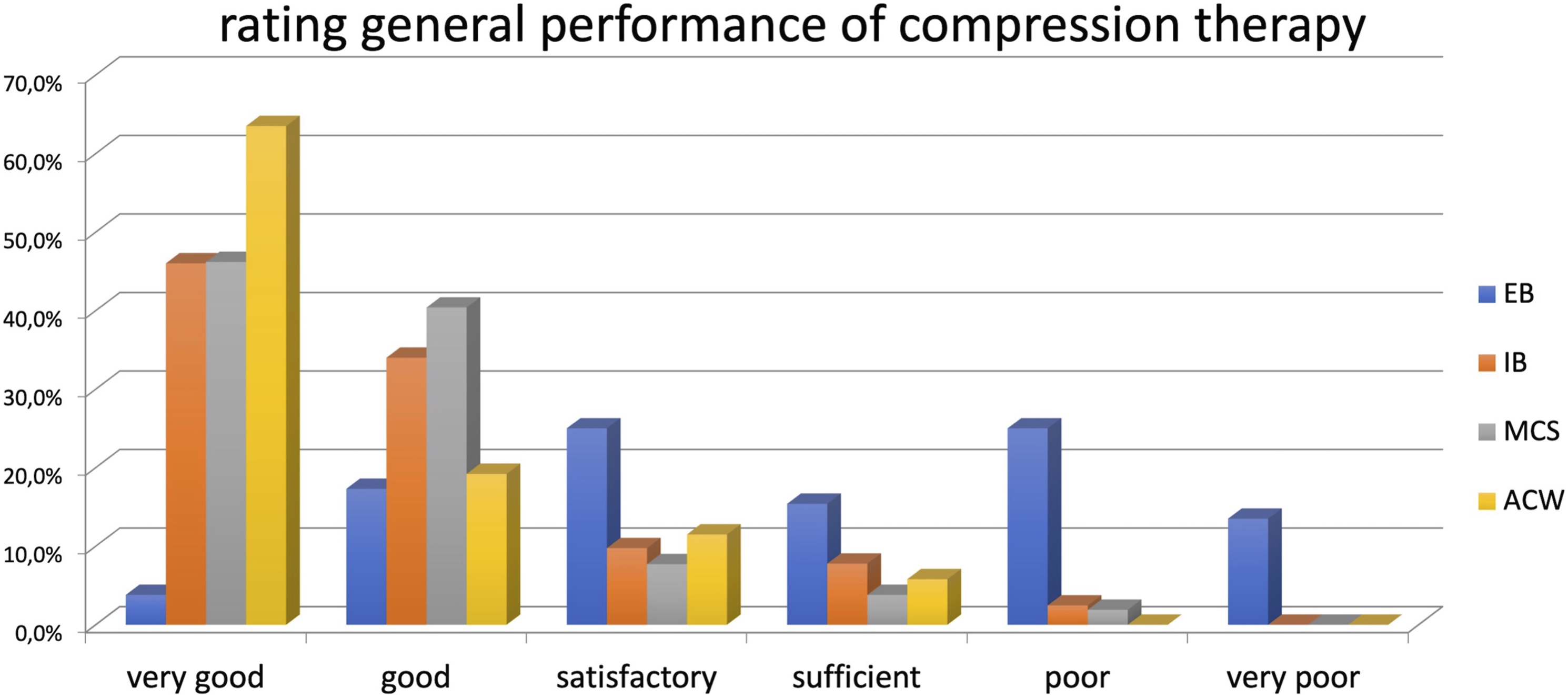
⁃ Elastic bandages: 4% answered very good, 17% good, 25% satisfactory, 15% sufficient, 25% poor, and 14% very poor (Figure 10). ⁃ Inelastic bandages: 58% answered very good, 35% good, 4% satisfactory, 2% sufficient, and 2% poor. ⁃ Medical compression stockings: 46% very good, 40% good, 8% satisfactory, 4% sufficient, and 2% poor. ⁃ Adjustable compression wraps: 64% responded very good, 19% good, 11% satisfactory, and 6% sufficient. Rating general performance of compression therapy according to applied compression devices. EBs: elastic bandages; IBs: inelastic bandages; MCSs: medical compression stockings; ACWs: adjustable compression wraps.
Safety
⁃ Elastic bandages: 19% answered very good, 15% good, 25% satisfactory, 15% sufficient, 19% poor, and 3% very poor. ⁃ Inelastic bandages: 36% answered very good, 39% good, 15% satisfactory, 5% sufficient, and 4% poor. ⁃ Medical compression stockings: 46% answered very good, 40% good, 12% satisfactory, and 2% sufficient. ⁃ Adjustable compression wraps: 58% answered very good, 29% good, 4% “satisfactory,” 8% sufficient, and 2% poor.
Ease of use
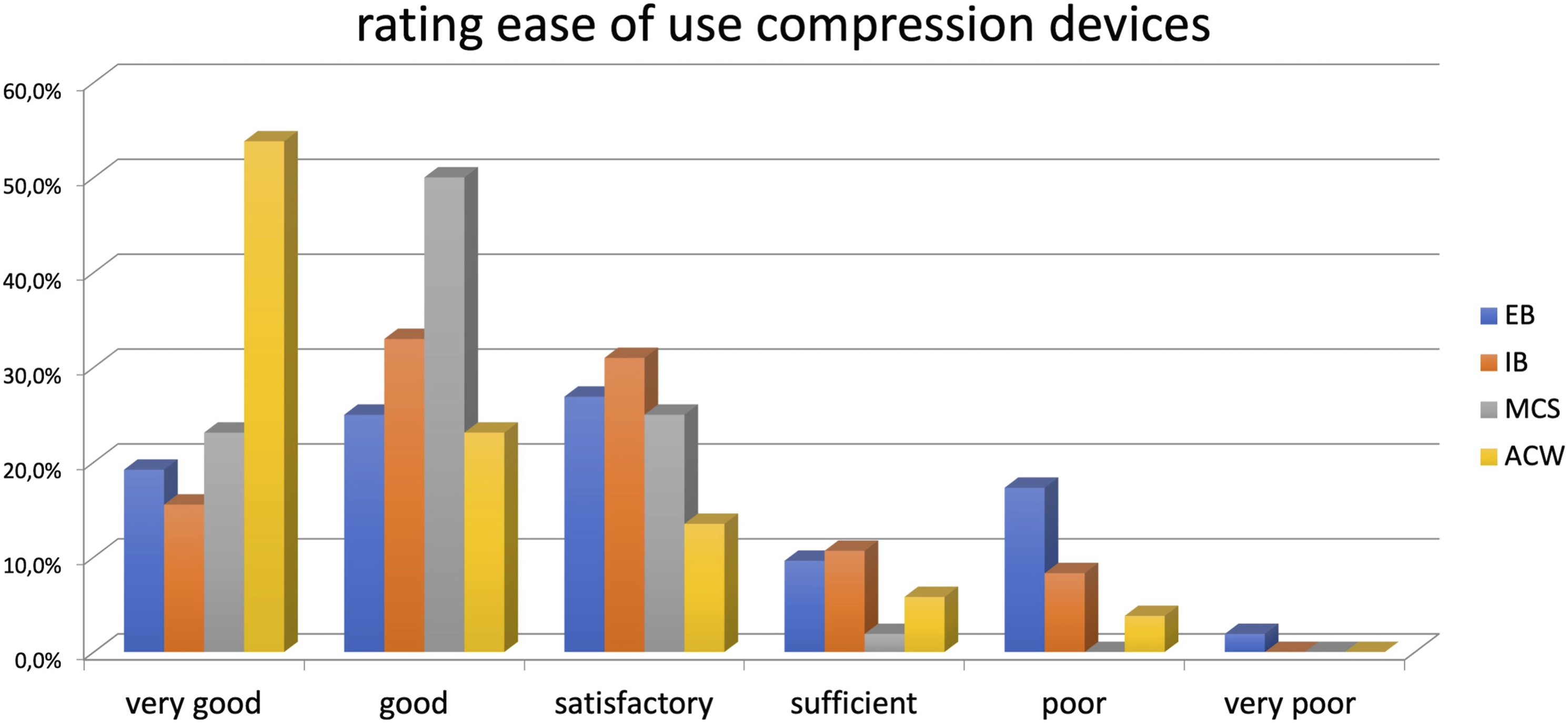
⁃ Elastic bandages: 19% answered very good, 25% good, 27% satisfactory, 10% sufficient, 17% poor, and 2% very poor (Figure 11). ⁃ Inelastic bandages: 15% answered very good, 33% good, 31% satisfactory, 11% sufficient, and 2% poor. 9% of experts did not respond. ⁃ Medical compression stockings: 23% answered very good, 50% good, 25% satisfactory, and 2% sufficient. ⁃ Adjustable compression wraps: 54% answered very good, 23% good, 14% satisfactory, 6% sufficient, and 4% poor. Rating ease of use of compression therapy according to applied compression devices. EBs: elastic bandages; IBs: inelastic bandages; MCSs: medical compression stockings; ACWs: adjustable compression wraps.
Comfort
⁃ Elastic bandages: 10% answered very good, 23% good, 35% satisfactory, 10% sufficient, 13% poor, and 9% very poor. ⁃ Inelastic bandages: 20% answered very good, 44% good, 20% satisfactory, 13% sufficient, and 3% poor or very poor. ⁃ Medical compression stockings. 28% answered very good, 55% good, 16% satisfactory, and 2% sufficient. ⁃ Adjustable compression wraps: 56% answered very good, 27% good, 12% satisfactory, 4% sufficient, and 2% very poor.
Discussion
Compression therapy is one of the best treatment modalities in the conservative management of venous disease and the treatment of minor sports injuries or traumatic soft tissue damage.
Unfortunately, even though CT is reported as effective in many clinical scenarios, the data in favor of CT are often weak, mainly due to the poor quality of studies.1,2 Therefore, only a few medical indications for CT are endorsed by evidence-based medicine. Nevertheless, the expert healthcare personnel participating in this survey routinely apply compression in all the stages of CVD even when shreds of evidence are poor or conflicting, as in symptomatic varicose veins,1,2 post-venous procedures,3,4 post-thrombotic syndrome,5,6 thromboprophylaxis in medical patients,7,8 or when CT is not even mentioned in official guidelines as in superficial venous thrombosis. 9 Although the percent of responders is reduced, also the application of compression after traumatic injuries, for example, in sports, is widely used despite supporting evidence being of relatively low quality.10–12 Pain and swelling reduction and speed increase of functional recovery are well known from experts in CT and justify its extensive use.
Worth to be highlighted are some additional indications listed by the participants in this survey. In particular, compression for edema after revascularization. Compression for this indication has already been reported in the past, both by intermittent pneumatic compression and sustained compression,13,14 but is strongly opposed by most surgeons. A new revision of this topic was recently performed, confirming the safety and effectiveness of CT in this indication. 15 Also, vasculitis was listed as an indication for CT confirming what was recently reported.16–18 Cellulitis is also worth highlighting as some participants mentioned it as an indication of CT and some other participants as a contraindication for CT. This contrast reflects the change in indication that has occurred in recent years. In the past, cellulitis has been considered a contraindication for CT due to the fear of systemizing skin infection. This contraindication was reported in guidelines or consensus documents. 19 More recently, it has been shown that this never happens, and CT is now considered a good indication both to treat20,21 and to prevent cellulitis 22 due to its anti-inflammatory effects. Regarding compression modality, inelastic materials are primarily applied in venous ulcers, mixed ulcers, venous edema, lymphedema, post-traumatic and post-operative edema, acute deep and superficial thrombosis, and some post-traumatic injuries (contusions, tendon injuries, and joint dislocations). Inelastic bandages are mainly used as inelastic material, but ACWs have become popular and are used in >10% of cases in venous leg ulcer and edema treatment. We want to highlight the inelastic material preference for leg ulcer treatment by most of our experts (91%), even though elastic stockings are still claimed to have a higher effect in some important publications.23,24 We cannot agree more with this preference. The inelastic material should be preferred in venous ulcer treatment due to its higher hemodynamic effectiveness than the elastic material.25–29 If venous ulcers are due to a venous hemodynamic impairment, the most effective compression modality in counteracting the hemodynamic impairment should be the most effective one in favoring venous ulcer healing. In addition, the studies comparing elastic and inelastic materials have many methodological flaws that make their conclusions hard to trust. 30 However, unfortunately, we must recognize that a high-quality study comparing elastic and inelastic material in venous ulcer treatment does not yet exist. Regarding the choice between IB and ACW, we want to underline the advantages of ACWs over IBs regarding comfort and ease of use. Some papers also reported a higher effectiveness of ACWs in increasing the venous leg ulcer healing rate.31,32 This superiority suggests that adopting an ACW approach in the vast group of healthcare providers dealing with leg ulcer treatment could significantly improve the treatment success. The expert participants’ skills in applying IB to our survey can explain their preference for this material. However, no ultimate conclusions can be drawn as to the most appropriate compression treatment as the cost and difficulty of performing RCTs are holding back the development and technical evolution of ACWs.
We also agree with IB application in acute DVT and SVT. Although both inelastic bandages and elastic stockings are recommended in the treatment of the acute phase of DVT and in the more recent guidelines, 9 there is a practical reason to prefer IB in the very initial phase after diagnosis. According to guidelines 9 and best medical practice, compression must be started immediately after the DVT diagnosis. Bandages are always available in phlebological departments or outpatient offices and can immediately be applied to the patient’s leg. Medical compression stockings must be prescribed; some days can pass if they are not immediately available at the shop, causing a treatment delay that should be avoided. The same practical reason is valid for edema treatment where, again, inelastic bandages are preferred by the experts participating in this survey. Cost issues represent an additional reason. Starting edema treatment by MCS can lead to the prescription of a new stocking fitting the new leg size when edema is reduced. Two stockings prescription will increase the cost to patients or the national health service. Starting with an inelastic bandage, the final MCS can be prescribed when the edema has been treated to maintain the result and prevent recurrence.
Our experts mainly prescribe elastic stockings to control venous symptoms in stages C2–C4 and prevent ulcer recurrences. Occupational edema, edema during pregnancy, subacute stage of DVT, post-thrombotic syndrome, and thromboprophylaxis are excellent indications for MCS according to our experts. There are no particular remarks regarding contraindications or side effects. Our experts agree with what are generally considered contraindications.19,33 Actually, very few apply compression, even in clinical situations where it is considered an absolute contraindication, like advanced arterial disease. Maybe the survey needed to be more transparent regarding the level of advanced arterial disease. Recent guidelines and consensus documents recommend/suggest CT when the ankle-brachial pressure index is >0.5 and the perfusion pressure (the pressure at ankle level) >60 mm Hg.21,34–36 It could be that an arterial impairment with these values was considered as “advanced.” Also, concomitant dermatoses are considered a contraindication (absolute or relative) by 40% of our experts, while 22% are doubtful if considering these clinical conditions as contraindications. Currently, some dermatologists are applying CT in these clinical situations 18 and maybe dermatoses will be turned from contraindications to good indications as already happened for other contraindications when more studies will be published. 37
Regarding the general performance of compression devices, it is remarkable that the majority of our experts rated as “very good” and “good” IB (94%), ACW (83%), and MCS (86%) while elastic bandages were considered as “very good” and “good” only by 21% of the experts.
Experts consider CT safe, with different ratings between the different compression devices. Only a minority of experts (about 2%–3%) rated the safety of different compression devices as poor. It is possible that every one of them is familiar with one or two compression systems and considers the devices they are not familiar with as less safe. Concerning ease of use, ACW achieved the highest rate. This is not surprising, too. Bandages are not easy to handle, and MCS are easy to handle only for people with sufficient strength, ability to bend, and without any joint impairment especially concerning hands. Adjustable compression wraps are considered also the most comfortable compression device even if putting together the rate “very good” and “good” about 80% of expert consider comfortable also IB and MCS.
Weak points: it could be possible to raise the doubt that being experts in CT does not necessarily mean experts in the conditions/indications/contraindications surveyed. Nevertheless, it must be taken into account that the participants in this survey are phlebologists or vascular surgeons or nurses working in departments treating patients with vascular diseases or trauma. We think we must credit them of the necessary experience to correctly evaluate the conditions/indications/contraindications surveyed. An additional weak point could regard the interpretation of the results coming from this survey. It must be taken into consideration the possible intellectual bias of this very specific group of interest or enthusiasts about CT leading us to interpret very cautiously their results. However, even if an intellectual bias cannot be completely excluded, we believe that doctors or nurses used to apply CT in their daily practice know very well the beneficial effect, the multiple indications,19–22 and the very few contraindications 33 of this treatment and are more prone to extensively apply CT even where precise data are missing.
Outlook for the future: The contradiction concerning the gap between the benefits of experience and the findings of evidence-based medicine highlights the need of new studies of high-scientific level. Indeed, many of published trials had many methodological flaws, such as recruitment biases and questionable statistical analyses, ultimately providing limited answers to the unresolved questions. Unfortunately, the budgets needed to carry out new trials can become disproportionate to the potential benefits coming from the new data, particularly in the case of medical compression. In the next future, new powerful tools like artificial intelligence may have the potential to surpass our current visions and ultimately to correct some of the contradictions that have arisen with the evolution of our knowledge. Analyzing hundreds of data sets from thousands of patients will no longer be an obstacle to making the best use of treatment. Collecting data as part of a large-scale medico-economic survey on the use of different compression devices, with an AI analysis, would enable a study to be carried out under real conditions and at a lower cost.
Conclusions
Doctors and nurses who know the beneficial effects of good compression apply CT extensively even when the indications are inconclusive. Inelastic devices are used in “complicated” clinical scenarios like venous ulcers, DVT, and lymphedema, while MCSs are used in initial or less advanced phases of venous disease. From this survey, we got the impression that elastic bandages are being used less and less and considered not as effective and safe as other kinds of compression modalities. In turn, ACWs are increasingly used; they are considered easy to use, effective, and safe. These last data have to be confirmed in future surveys.
Footnotes
Acknowledgments
We want to acknowledge Lohmann&Rauscher for its unconditioned support in spreading the survey and collecting the responses.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
International Compression Club.
Contributorship
Giovanni Mosti, Jean Patrick Benigni, Eduardo da Matta, Hugo Partsch, Angrit Namislo, and Martin Abel prepared the questionnaire for the survey. Angrit Namislo, Martin Abel, and Michael Schmitz collected the responses and ordered the data. Giovanni Mosti wrote the first draft of the manuscript and finalized the manuscript after other authors (below specified) gave him comments and suggestions. Angrit Namislo, Martin Abel, Jean Patrick Benigni, and Eduardo da Matta revised the manuscript and offered their comments and suggestions.