
Abstract
Objective
The objective of this study is to systemically review the literature on Anterior Saphenous Vein (ASV) reflux treatment and insurance impediments to treatment coverage.
Methods
A literature search was performed using a PRISMA framework. In addition, a cross-sectional analysis of insurance policies for ASV treatment was evaluated.
Results
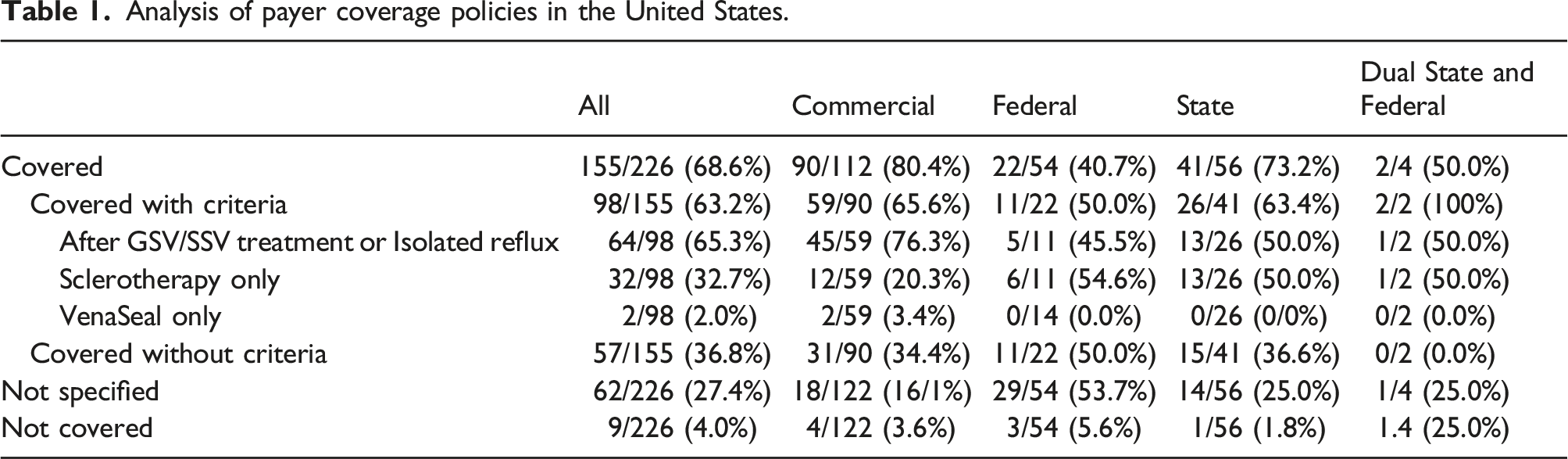
Published evidence and treatment considerations in the literature for ASV treatment are discussed. In 155 of 226 (68.6%) insurance policies reviewed coverage of ASV ablation was allowed while 62/226 (27.4%) did not specify coverage and 9/226 (4.0%) specified ASV treatment was not covered. Of the 155 that provide ASV coverage, 98 (62.2%) provide coverage with criteria such as requiring prior treatment of the great saphenous vein.
Conclusions
Vein treatment experts should continue to advocate to insurance carriers to update their varicose vein treatment policies to reflect the substantial clinical evidence so that patients with ASV reflux can be appropriately treated.
Introduction
Chronic venous disease (CVD) is a prevalent condition that tends to worsen with time. Patients initially seek treatment to relieve symptoms of leg pain, heaviness, and swelling, all of which impact their well-being. 1 As the disease progresses varicose veins become more evident, there can be proinflammatory skin changes, and in some cases, there is venous ulceration. 1 These conditions negatively impact patient quality of life and place substantial financial burdens on healthcare resources. 2 Once venous insufficiency develops a vicious cycle of inflammation and leukocyte recruitment can lead to further deterioration of vein walls and valves, increased venous hypertension, and release of additional proinflammatory mediators that further influences the progression of the problem. 3 Early treatment of CVD at the physiological level can help break the inflammatory cycle and alleviate symptoms and reduce progression to advanced disease. 3
The most common cause of superficial CVD results from reflux in the great saphenous vein (GSV) followed by the small saphenous vein (SSV). 4 What has been commonly referred to as Anterior Accessory Saphenous Vein (AASV) reflux is the third most common source of superficial venous reflux in the lower extremities in patients seeking treatment for CVD. 4 In most studies, ASV reflux is present in about 10% to 20% of patients presenting for treatment and approximately a third of patients present after prior treatment.4–8 There is an increasing appreciation that addressing ASV reflux is important not only in achieving optimal outcomes in first time treatment patients in the short term but also in addressing the risk of recurrence after treatment in the long-term.
There has been confusion in the past whether the ASV is an axial vein in its own right, or a tributary of the GSV. Anatomically, the ASV is clearly an axial vein given its intrafascial course in the proximal thigh. This has led to confusion on the part of payers, creating inequities in reimbursement for patients in need of medically necessary ASV treatment. This impacts patients as ASV has a distinct natural history that can be worse in terms of progression to more advanced stages at presentation and complications such as an increased risk of superficial vein thrombophlebitis. This is an issue not only in patients presenting for first time treatment, but also for progressive patients who have had prior vein treatments.9,10 Understanding its anatomy, natural history and treatment outcomes is therefore imperative as these patients are considered for treatment planning. This manuscript is part 3 of a 4 part series where the panel recommends changing the terminology such that the “anterior accessory saphenous vein” (AASV) now be designated the anterior saphenous vein (ASV). This recommendation is supplemented by three accompanying parts to this series: Part1: The Anterior Saphenous Vein. Part 1. A position statement endorsed by the American Vein and Lymphatic Society (AVLS), the American Venous Forum (AVF), and the International Union of Phlebology (UIP). Part 2: an ultrasound study of ASV anatomy in normal controls and patients with anteromedial thigh varicosities; and Part 3: a review of the clinical and technical considerations when treating patients with ASV reflux.
Methods
Systemic literature review
PubMed and Google Scholar were searched for articles and relevant articles included were selected according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Studies were included if they specifically addressed the following search terms: “Anterior Accessory Saphenous Vein, Anterior Saphenous Vein, anterior accessory great saphenous vein, lateral saphenous vein, anterior and vein and accessory and vein.” Two independent reviewers (RD and EB) screened the abstracts considered for topics. Controversies were discussed and resolved via in-person meetings, conference calls, and discussions. Articles were excluded if they were not related to lower extremity chronic venous insufficiency in humans.
Insurance coverage analysis
We conducted a cross-sectional analysis of publicly accessible insurance policies related to treatment of varicose veins. Of those policies that extended coverage, medical necessity criteria were abstracted and evaluated using the American Venous Forum’s Venous Policy Navigator. It contains up-to-date pre-authorization terminology and documentation requirements from payers across the United States in a web-based search format. This resource is updated monthly with the most current venous coverage policies.
Results
Systemic literature review
Of the 1971 articles published in English screened, 66 duplicates were removed and 1905 were selected for screening following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) inclusion criteria. A total of 1717 publications were found to be irrelevant and 188 full text studies were assessed for eligibility. An additional 56 were excluded as being irrelevant to the topic leading to 132 that were included in the review. (Figure 1) PRISMA Diagram.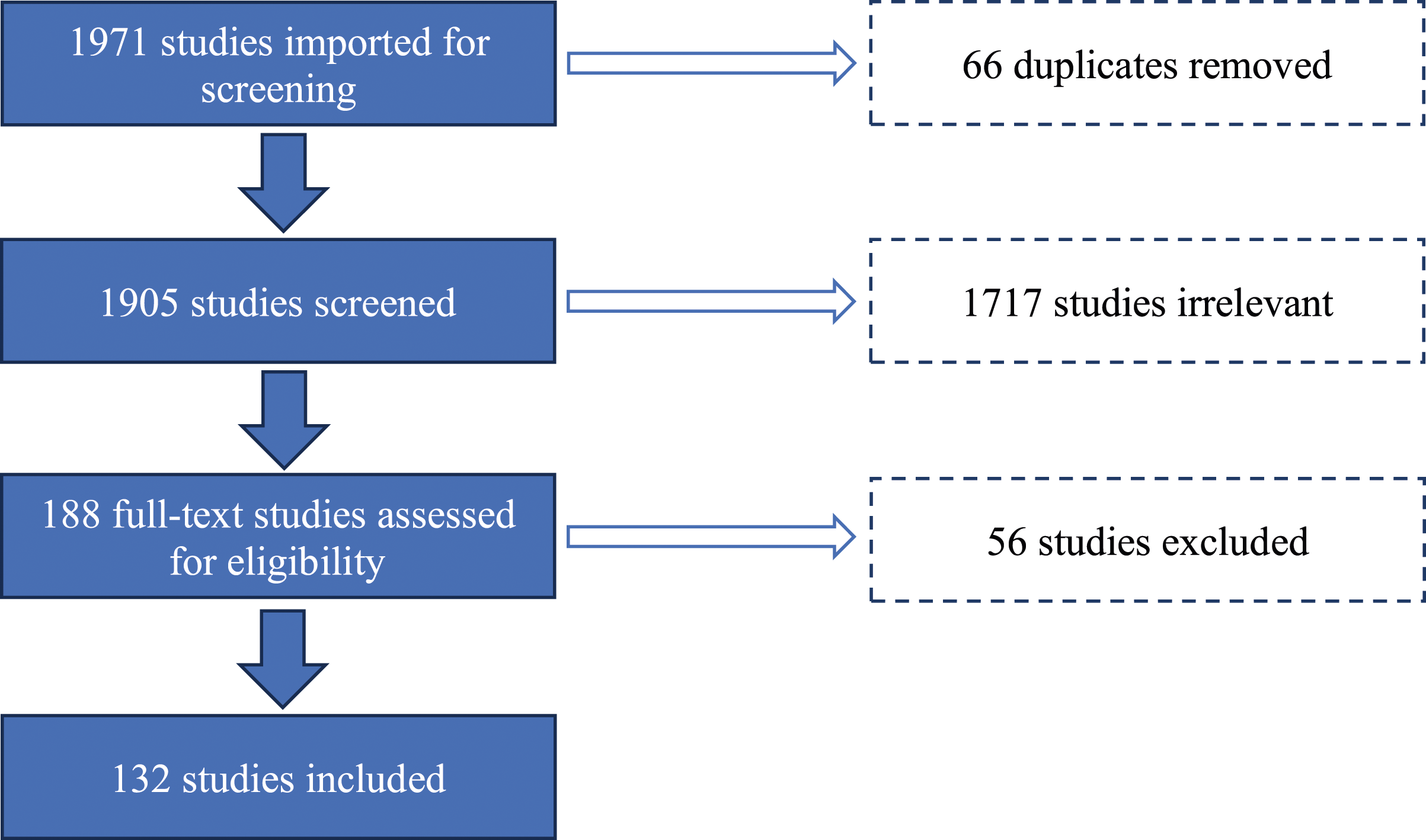
Insurance coverage analysis
Analysis of payer coverage policies in the United States.
Discussion
ASV reflux is quite common in patients presenting for treatment for CVD. In a study by Zollmann and colleagues of 2019 patients, 10.9% had isolated ASV reflux, and 11.3% had both GSV and ASV reflux representing nearly 22% of patients in this series. 11 Likewise, Schul noted that 13.9% has ASV reflux in their series, and a total of 4.3% has ASV reflux combined with GSV reflux. 9
The severity of symptoms in patients with ASV tends to be similar to what is commonly seen with GSV reflux. In an analysis of the American Vein & Lymphatic Society PRO Venous Registry, the severity of the presenting symptoms in 2604 patients with venous reflux, as measured by the rVCSS, was higher for patients with ASV reflux when compared to patients with GSV alone suggesting that ASV reflux may present in more advanced stages than GSV alone. Further the proportion of ASV limbs with superficial thrombosis events (12.9%) was significantly higher than that for GSV alone (2.7). 9
The severity of symptoms is also worse in ASV reflux patients presenting primarily, compared to those with ASV reflux in the progressive group who have prior been treated. Specifically, patients in the primary group presented with CEAP class C4 and above in 43.1% vs 24.8% in the progressive group. Again, the incidence of superficial vein thrombosis for the ASV patients (6.4%) was significantly higher than that of the in the progressive group (2%). This data demonstrates that primary patients are more likely to have more edema, skin changes, refluxing veins above and below the knee and a greater need for compression than the progressive group with ASV reflux. That is not surprising as those in the progressive group have the benefit of prior treatment to reduce the burden of their reflux. 9
Taken together this data suggests that in the absence of treatment patients with ASV reflux may be more prone to continue to have significant venous symptoms progress and go on to develop advanced disease and are more prone to suffer from bouts of superficial vein thrombophlebitis. These findings support the consensus that ASV reflux is far from being a less important afterthought following GSV treatment and may in fact have as bad natural history if left untreated.
ASV as the source of recurrence after prior GSV treatment
In the era prior to endovenous ablation with thermal and other modalities, open surgical saphenofemoral ligation and stripping of the GSV was the primary approach to treat patients with CVD. When those patients had recurrence, about half that returned with progressive disease had a recurrence from the groin. 12 In those series, ASV reflux was a common cause of recurrent reflux from the groin. 7 In a study of 186 patients evaluated over a 36-month period, 32% had a recurrence due to a persistent ASV. In these cases, the ASV was presumably flush ligated when it connected with the SFJ. However, it was unclear how often the ASV was then stripped. Even if the SFJ confluence was surgically divided, the remaining unstripped ASV could be a location for disease progression leading to worsening of symptoms.
In the current endovenous ablation era, the ASV remains an important source of recurrence in approximately 10 to 16% of patients.13–15 In the RELACS study, four hundred patients with GSV incompetence were randomized to endovenous laser ablation (EVLA) or high ligation and stripping (HLS) of the GSV with the main outcome measures of clinical recurrent varicose veins after surgery. In this series, recurrent varicose veins were similarly observed in both groups: 45% (EVLA) and 54% (HLS). Recurrence from the groin was considered a same site recurrence. This included recanalization of the GSV, ASV reflux, or a large perforator in the proximal thigh. Patients of the EVLA group showed significantly more clinical recurrences in the operated region 18% versus 5%. While most were from recanalization of the GSV nearly half (48%) were from ASV reflux. 14 In a meta-analysis of randomized trials comparing endovenous treatment to high ligation and stripping, O’Donnell and colleagues reported the most common source of recurrence was recanalization of the GSV with ASV reflux in 16% of patients with recurrence after prior endovenous treatment. 16 In the modern era of endovenous ablation, recanalization of the GSV is far less common as most ablation modalities such as RFA or cyanoacrylate have long-term occlusion rates that exceed 90%. 17
The importance of ASV reflux after prior GSV ablation is reflected in more modern series. In a long-term study by Whiteley and colleagues over 15 years, 51.6% patients developed de novo reflux after prior RFA showing disease progression in veins that were originally competent. In this study, ASV reflux was noted in 43% of the patients and 34% of the legs. In contrast to prior eras when saphenofemoral ligation and stripping were the norm, neovascularization was not found in any patients who had prior endovenous ablation procedures. 18 These studies suggest as the role for HLS fades and endovenous ablation increases, there will likely be an even bigger role of ASV reflux in progression of disease after prior treatment in the coming years. This is because the ASV was likely treated in the HLS series by at least ligation whereas in endovenous ablation the ASV is not in the absence of reflux.
In the early era of endovenous ablation, the stump remaining after a GSV ablation was initially speculated as a potential source of neovascularization; however, this has not turned out to be a common finding. 19 What is apparently more common is de novo reflux developing in veins that were competent at the first treatment. Proebstle and colleagues completed a prospective study where GSV reflux was treated and the ASV was monitored for the presence of significant ASV reflux over 4 years. They identified 93 limbs with 82 available for follow-up over this time period. In the initial follow-up evaluation, 43 (46%) limbs had clinical evidence of ASV disease with only 2% demonstrating reflux at baseline. Over the course of the analysis, 65 limbs (71%) demonstrated clinical evidence of ASV reflux, and 24 limbs demonstrated new onset reflux. Of these 24 limbs, 55% were in the initial patients with clinically visible ASVs and the remainder were newly diagnosed with ASV reflux. Notably, not only did the proportion of refluxing ASVs increase, but the proportion of legs with a detectable ASV increased from 43 legs (46%) at baseline to 71% at 4-year follow-up. Thus, after 4-year follow-up of endothermal GSV ablation, ASVs were observed in more than 70% of legs. 20 Similar outcomes were also shown by Bush et al., with 24% of recurrent varicose vein patients after GSV ablation having new ASV reflux, and O’Donnell et al., who showed in a meta-analysis of published randomized clinical trials that following recanalization, new ASV reflux was the second most common cause of recurrent varicose veins after prior endovenous ablation occurring in 19% of patients.6,16
These data suggest that even if there is a visible ASV without reflux, or no visible ASV at the initial GSV procedure, the ASV should be recognized as a common source for recurrence in a sizeable number of patients who return for treatment years later. The apparent potential for the ASV to play a major role in recurrent reflux after GSV ablation has led some investigators to question if it should be treated at the same time as the GSV reflux is treated. How to best monitor these patients and when to intervene remains an open question that is being addressed in at least one ongoing randomized prospective trial. 21
ASV treatment outcomes
Endovenous therapies for the treatment of symptomatic ASV reflux have consistently demonstrated similar outcomes compared to patients with symptomatic GSV reflux in multiple clinical trials and meta-analysis.22–26 These studies have shown treatment of the ASV is as safe and effective as treating the GSV and SSV with the same ablation modalities. 27 In a meta-analysis with 609 patients included, the pooled anatomic success rates were 91.8% after endovenous laser ablation and radiofrequency ablation (EVLA, RFA, 11 studies), 93.6% after cyanoacrylate closure (3 studies), and 79.8% after sclerotherapy (2 studies). 24 The rate of endothermal heat induced thrombosis does not appear higher than with ablation of the GSV. 28 Even high body mass index patients do not appear to have more recanalization after thermal treatment of the ASV. 29 Deol and colleagues evaluated an extensive database that reported both physician and patient reported outcomes that included a stand-alone ASV ablation cohort. Compared to GSV treatment, ASV stand-alone treatment demonstrated equivalent 1- and 6-month outcomes, by rVCSS scores. 23 These studies support that in comparison to concomitant treatment with the GSV, stand-alone ASV reflux treatment is safe and effective even in the absence of GSV or other axial reflux.
International consensus on ASV treatment
There are numerous clear and consistent evidenced based consensus statements emphasizing the importance for ASV treatment when medically necessary. In the American College of Phlebology Guidelines regarding the treatment of ASV reflux, Grade 1, level of evidence C, recommendation was made for treatment of symptomatic incompetence using endovenous thermal ablation or foam sclerotherapy to reduce symptomatology.22,30 In the 2011 practice guidelines of the Society for Vascular Surgery and the American Venous Forum, it was recognized that ASV reflux is common in patients with venous reflux disease both in primary and progressive cases. The expert panel further concluded that treatment of ASV reflux is as safe and effective as treatment of the GSV and SSV with the same modalities and that vein closure rates and improvement in patient symptoms and quality of life. 31
Likewise, in a consensus statement defining Appropriate Use Criteria (AUC) led by Masuda and colleagues’, treatment considerations for patients with ASV reflux were evaluated by experts from the American Venous Forum, the Society for Vascular Surgery, the American Vein and Lymphatic Society, and the Society of Interventional Radiology. 32 They concurred that ablation of the ASV in a symptomatic patient with varicose veins when the ASV demonstrates axial reflux directed to affected area is efficacious and indicated. Of note, they found it was rarely appropriate to ablate the ASV with no reflux in the setting of GSV reflux. 33 In the most recent clinical practice guidelines from the European Society of Vascular Surgery (ESVS), experts concluded endovenous thermal ablation of the ASV is a Class IIa recommendation and ultrasound-guided foam sclerotherapy is a Class IIb recommendation due to effective closure rates and improvements in quality-of-life scores. 34 In the recent 2023 publication of the clinical practice guidelines of the Society for Vascular Surgery and the American Venous Forum a grade 2C recommendation was provided for the treatment of symptomatic ASV reflux with thermal or non-thermal approaches. 30
Thus, not only are there ample published clinical studies to support treatment of symptomatic ASV reflux, but there are also consistent international expert consensus statements that support medically necessary ASV reflux treatment when indicated as well.
The importance of tributary varicosity treatment
Opinions differ if targeting the primary axial vein reflux for endovenous ablation alone is adequate as the initial treatment of choice, or if concomitant treatment of associated tributary varicosities is needed to optimize long term relief of venous symptoms. One camp promotes the concept that many tributary veins will regress with inflow ablation alone, while others consider concomitant tributary vein treatment with ambulatory phlebectomy or sclerotherapy necessary to achieve optimal short and long-term outcomes. In metanalysis of ASV treatment, the data suggest that concomitant treatment may result in earlier improvement in quality of life and reduce recurrence rates; however, the data in randomized data sets is less clear. 35 In the studies by both Deol and Theivacumar, improvement was less sustained if the associated tributary veins were not treated concomitantly.13,23 At 6 months, standalone ASV ablation without concomitant varicosity treatment symptoms returned and paralleled those for preintervention GSV reflux. However, if phlebectomy was performed with an ASV ablation, 6-month outcomes remained improved and mirrored those of 6-month GSV ablation.13,23 These data suggest that treating the tributary veins may hold an advantage when included in the initial treatment plan rather than waiting to see if these tributaries regress after ASV ablation alone.
For these reasons, clinical practice guidelines suggest a shared medical decision making with the patient to determine if the tributary varicosities should be treated at the same time as the axial ablation or delayed. 34 Specifically, for ASV treatment evidence suggests there may be an advantage to early concomitant treatment of the varicosities rather than waiting to see if they regress with time.
The importance of payor advocacy on behalf of CVD patients
Despite ample published evidence and expert consensus-based recommendations, clinicians in the United States have voiced frustrations with a variety of insurance payers with what appear to be confusing and not evidenced based treatment policies that prevent some patients with medically necessary needs for ASV reflux to receive care. Generally, payer treatment policies are changed following evidence consensus and should be consistent with peer reviewed and published national treatment guidelines and appropriate use criteria. Despite these national and international clinical practice guidelines which promote a very clear and appropriate approach to patients with ASV reflux to obtain medically necessary treatments, many insurance companies continue to have policies that preclude treatment of the ASV.
Using the American Venous Forum Venous Policy Navigator, an analysis of national varicose vein treatment policies demonstrate that most payers offer coverage for ASV treatment when medical necessary. Currently in the United States nearly 70% of insurance carriers cover medically necessary treatment of ASV reflux. However, there are a sizeable number of restrictions on when such coverage is applied. Of those that restrict coverage, about two-thirds will only approve ASV treatment after prior GSV or SSV treatment or if it demonstrated that there is isolated ASV reflux. About a third of policies only cover sclerotherapy, suggesting a misunderstanding that the ASV is a tributary, not an axial vein that needs a more ablative approach such as thermal or non-thermal ablation to sustain optimal results long term.
These policies, that have real world effects on patients access to appropriate care, go against ample evidence to support ASV treatment when medially indicated. Further, there is an absence of evidence to either support their policy to restrict its use or not cover it at all. Therefore, payers should update their policies to be consistent with current evidence and consensus. Specifically, based on the available evidenced and published clinical guidelines for lower extremity chronic venous insufficiency secondary to symptomatic ASV reflux, payers should consider incorporating the following in their coverage policies for venous insufficiency: Treatment of patients with symptomatic ASV reflux should be covered without any criteria other than that the patient have reflux and the medical necessity criteria be present. Specifically, prior GSV or SSV treatment should not be a requirement, especially in the case if the GSV is in fact without reflux. This is especially relevant when both GSV and ASV are present, and both can be efficiently treated concomitantly in the same operative setting or during the initial treatment plan. Detailed anatomic series demonstrate that not all ASVs originate from the SFJ since some can drain directly to the deeper pelvic veins. 14 Thus, treatment of ASV reflux should not require associated SFJ incompetence since not all ASV reflux derives from an incompetent SFJ. Further, policies should be inclusive of the need at times to concomitantly treat the pelvic venous sources that can contribute to ASV reflux in some cases. There is no evidence to support arbitrary size cut off for the diameter of the ASV to be treated. Requiring physician compounded sclerotherapy as the sole treatment for ASV reflux is generally inferior to other forms of thermal (RFA and Laser) or non-thermal (Cyanoacrylate closure or proprietary non compounded microfoam). Treating providers should be given the choice of which ablation modality they offer patients in a shared medical decision-making process since there is no evidence that one form of axial ablation is superior to another.
Conclusions
There is substantial published evidence, including meta-analysis and expert consensus, supporting treatment of ASV reflux when it is the source of venous symptoms, and thus there is no reasonable clinical rationale to consider its treatment experimental or unproven. It is entirely without a sound evidenced based clinical foundation to require treatment of a normal GSV prior to the treatment of ASV reflux. Likewise, it is currently without clincal rationale or support from published evidence to treat a normal ASV concomitantly with a refluxing GSV. Given the variability of its confluence with the deep system, reflux in the SFJ as a requirement for treatment, regardless of GSV or ASV, is unfounded. Just as has been shown for treatment of the GSV reflux, when ASV reflux is present along with medically necessary symptoms, the treatment of the ASV with ablation has excellent outcomes that can improve patient quality of life. Given the challenges to obtain authorization from some payers to treat ASV reflux, vein experts should continue to advocate to insurance carriers to update their varicose vein treatment policies to reflect the substantial clinical evidence on this subject. Without such advocacy and revision of inappropriately restrictive treatment policies, some patients will be excluded from effective therapy and thus be subject to ongoing risks of SVT, DVT, and venous ulceration that could simply be treated if such policies were not prohibitive.
Supplemental Material
Supplemental Material - The anterior saphenous vein. Part 3. Systematic review of the literature and payor coverage policies. Endorsed by the American Vein and Lymphatic Society, the American Venous Forum and the International Union of Phlebology
Supplemental Material for The anterior saphenous vein. Part 3. Systematic review of the literature and payor coverage policies. Endorsed by the American vein and lymphatic society, the American Venous Forum and the International Union of Phlebology by Rachel Drgastin, Edward M Boyle, Nicos Labropoulos, Alberto Caggiati, Antonios Gasparis, Suat Doganci, and Mark Meissner in Phlebology
Footnotes
Acknowledgments
The authors acknowledge Michael Thompson for helping organize the group to develop and complete the project.
Author notes
Authors represented: Meissner M (MM); Boyle EM; (EB) Labropoulos N (NL); Caggiati A (AC); Drgastin R (RD); Dognaci S (SD); Gasparis A (AG).
Additional consideration
As detailed in the letter to the editor upon the submission, these works have been endorsed by the AVLS, UIP and AVF and are being simultaneously submitted to both Phlebology and JVS_VL.
Contributorship
MM, AG, NL and SD conceived of the project. MM, AG, NL, EB, RD, AC and SD all contributed to developing the articles and contributing to the analysis and conclusions. EB, RD and AC wrote the drafts of the articles and all parties approved of the final manuscripts.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RD, EB, AC, SD, and MM reports no conflicts. NL is a Consultant/Speaker with Philips, Medtronic, BD Bard, Boston Scientific; AG is a Consultant/Speaker: Medtronic, BD Bard, Boston Scientific.
Funding
The open access publication fees for this article was financially supported by Boston Scientific Corporation. No other funding was provided.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.