
Abstract

Introduction
In the management of patients with chronic venous disease (CVD), compression therapies, in the form of stockings, wraps, and/or bandages, are an indispensable treatment option. Used as both primary therapy and adjunct before and after venous interventions, the aim of compression therapies is to provide support to the calf muscle pump and to reduce venous hypertension in the lower limbs. 1 On a macroscopic level, additional pressure provided by compression improves venous and lymphatic return, augmenting that which is already provided by the calf muscle pump system. 2
Graduated compression also has effects on microscopic changes related to CVD. Compression has been shown to reduce the levels of inflammatory markers found in the systemic circulation and plays a role in improving microcirculation within the skin, improving tissue oxygenation, and reducing the level of several cytokines which may help with preventing skin breakdown as well as with healing of venous leg ulceration.3–6 As shown in several studies, the use of compression treatment is also effective in the management of CVD symptoms including swelling. 7
This one-page guideline from the International Union of Phlebology aims to highlight the use of compression therapy in the management of varicose veins. It summarises the indications for compression therapy and key clinical considerations that all medical professionals should remember when managing patients presenting with symptomatic CVD.
Management recommendations
It is recommended that graduated compression stockings (GCS) and other compression systems such as wraps and bandaging be used to improve symptoms, to reduce leg swelling, and to help improve quality of life in CVD patients. These may be applied as a primary treatment for symptomatic varicose veins (CEAP C2 disease), oedema related to varicose veins (C3), skin changes (C4), and active and healed venous ulceration (C5 and C6) and in the patients remaining symptomatic after venous interventions. Compression treatment also plays an important role in the avoidance of the local complications and swelling in the patients undergoing invasive varicose vein treatment.
Patients should undergo individualised assessment of CVD symptoms and signs. GCS may firstly be provided for symptomatic patients or on identification of clinical signs that are indicative of venous hypertension as primary treatment or as a temporalising measure whilst awaiting venous procedures. Compression therapy is recommended for symptomatic varicose veins,7,8 or more severe stages of disease (C3 and above). It has been shown to improve CVD-related skin changes, reduce the venous leg ulcer–related pain complains, improve venous leg ulcer healing rates, and reduce the risk of ulcer recurrence.9–12 For patients with C6 disease, it should be noted that compression therapy is not the only indicated therapy and should be offered alongside good wound care and superficial venous intervention as appropriate. Additionally, compression should be offered to patients with occupational (e.g. occupations that require long durations of standing) or environmental risk factors for oedema. 13
Should patients undergo procedural treatment, GCS should be provided immediately post-procedure.14–19 This is recommended to help reduce post-procedural pain, oedema, and phlebitis. To increase the local pressure in these clinical settings, an additional eccentric compression to enhance the compression effectiveness can be applied. 20 Grade of compression and duration of therapy should be individualised, and patients with persistent clinical manifestations of CVD (e.g. oedema, pain) despite treatment would benefit from higher grades and longer durations of compression therapy. 21 There is no strong evidence that any specific form of compression therapy is better post-intervention, although studies have suggested that stockings may be more acceptable to patients. 22
Discussion
This article provides a one-page clinical practice guideline summarising compression therapy for the management of VVs. It is part of a series of publications for the UIP One-Page Guidelines which are aimed at ensuring that patients with venous disease receive timely and appropriate care based on current best evidence and expert consensus and in line with other guidelines and consensus documents from other institutions (Figure 1).
21
The one-page guideline.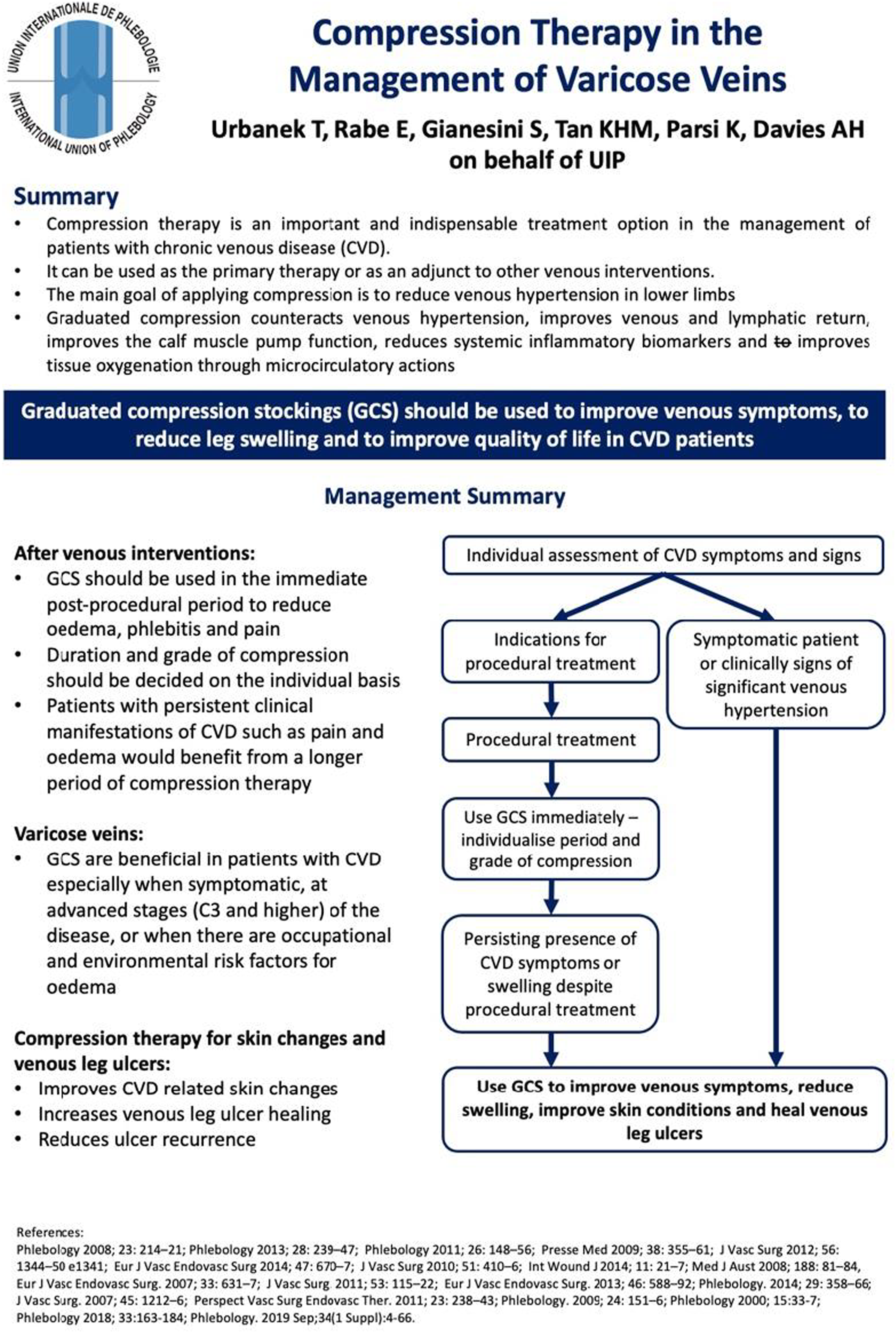
While it is undeniable that compression plays a large role in the management of all manifestations of CVD, the evidence in the current literature largely focuses on the efficacy of the compression in the venous leg ulcer treatment and recurrence prevention, the comparisons between compression and interventional treatment as well as the use of the periprocedural compression treatment in the patients undergoing invasive treatment of the chronic venous disease.18,23,24 Post-procedural compression is widely practiced and is recommended in this document, with compression type and duration to be individualised based on patient characteristics and symptom profile. While patients with symptoms such as pain and oedema that persist after venous intervention should be provided with compression for longer durations, the length of compression treatment is very much dependent on clinician zeitgeist before further treatment is considered or offered to this patient population.
Additionally, fewer studies, which are in the majority largely observational in design, have focused on the isolated effect of compression on symptomatic varicose veins when compared to no treatment.25,26 These studies, while undoubtedly showing a potential benefit of compression stockings, also fail to determine if these improvements are cost-effective due to the lack of health-related quality of life measures used. Due to often symptomatic CVD disease course, in many patients prolonged use of the medical compression stocking is advised. The question if asymptomatic CVD patients (e.g. C1 or C2) should be treated by compression to avoid disease progression is still open for the discussion. Despite an influence on the venous hypertension decrease, there are no well-designed studies available focusing on an influence of the compression on the CVD progression and no EBM recommendation can be made and proposed in this particular indication. A well-designed large randomised clinical trial with head-to-head comparison would be useful in clarifying these deficits in the literature.
It is also important to note that while compression has been shown to be useful in the management of CVD, it is only useful if patients are able to tolerate and comply to the compression regimen. Poor compliance to compression has been reported widely in the literature, with reasons for non-compliance including discomfort, difficulty putting compression on, and itchiness. 27 Improving adherence improves outcomes related to CVD, but no intervention has been shown to consistently improve compliance to compression. 28 Further work to understand the pitfalls of compression and develop multi-dimensional strategies to improve adherence is clearly required to maximise the benefit of compression therapies. The growing research and experience concerning the use of compression also increased the current knowledge on the potential contraindications to the compression treatment. In candidate for compression therapy, the subject of potential lack of the compliance, together with presence of the potential contraindications should be assessed. This in turn can potentially decrease the risk of the compression complications as well as allow to choose the optimal way to provide compression therapy for the individual patient. 29
Footnotes
Author contributions
K.P. and A.H.D. conceptualised the design of the short report and one-page guideline. T.U., E.R., and S.G. contributed to the literature review and formulation of the recommendations. M.T. contributed to the formatting and layout of the one-page guideline (![]() ) and wrote the initial draft of the short report. All authors reviewed the short report prior to submission.
) and wrote the initial draft of the short report. All authors reviewed the short report prior to submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Professor Alun Davies on behalf of the UIP.