
Abstract

Introduction
The treatment of truncal veins and associated tributary varicosities has evolved significantly since the development of endovenous ablation techniques towards the end of the 20th Century. 1 Today, a range of minimally invasive endovenous ablation techniques are well established and widely used worldwide for the treatment of chronic venous disease (CVD). These may be broadly divided into thermal ablation and non-thermal and non-tumescent (NT/NT) ablation techniques.
Endovenous thermal ablation (EVTA) techniques include the use of endovenous laser (EVLA), radiofrequency (RFA), and less commonly, steam ablation devices. These devices generate thermal energy within the target vessel, denaturing the vein wall and causing it to develop into a fibrous cord. Accordingly, usage of these techniques requires concurrent use of perivenous tumescent anaesthesia. This tumescence not only provides an insulation barrier to protect surrounding structures from inadvertent heat injury but also provides compression around the vein to improve opposition and contact with the thermal device and anaesthetic to minimise pain to the patient during the procedure. Ironically, this tumescence can often be the most uncomfortable part of the treatment, which may be overcome with the use of non-thermal and therefore non-tumescent ablation techniques.
NT/NT ablation techniques include cyanoacrylate adhesive closure (CAC), mechanochemical ablation (MOCA), catheter-directed sclerotherapy (CDS), and ultrasound-guided foam sclerotherapy (UGFS). These techniques utilise both chemical and mechanical methods to destroy the endothelium and parts of the vessel wall, causing inflammation which eventually leads to sclerotic changes and development into the fibrous cord.
This article seeks to highlight the management recommendations from the International Union of Phlebology (UIP), highlighting the techniques, both thermal and NT/NT, that may be used in truncal ablation. It provides advice on both first- and second-line options for ablation, stratified by target truncal vessel, and highlights the evidence grade for each ablation technique (Figure 1).
Management recommendations
For the great saphenous vein (GSV), there is Grade 1A evidence for recommendation of use of EVLA or RFA ablation. Should EVLA or RFA not be available within a centre, second-line options include UGFS (Grade 2A), CAC (Grade 2aA), MOCA (Grade 2bA), and steam (Grade 2aB). It should be noted that for each treatment modality, the grades of evidence cited are limited to a specific vessel diameter.
EVLA and RFA can be used as the first-line option for the small saphenous vein (SSV) (Grade 1A), anterior and posterior accessory GSV (Grade 1B), and the Giacomini vein and SSV cranial extension (Grade 1B). UGFS should be considered as the second-line treatment modality in all these vessels, with Grade 2A evidence for the SSV up to 10 mm and Grade 1C evidence for the other veins.
Furthermore, given the limitations of EVLA and RFA devices that preclude their usage in the treatment of more tortuous vein segments, secondary procedures should be used to address veins that are not treated using these thermal ablation methods. Clinicians should consider combining thermal ablation techniques with UGFS or phlebectomy to treat the veins that are not treatable using EVLA or RFA. One-page guideline.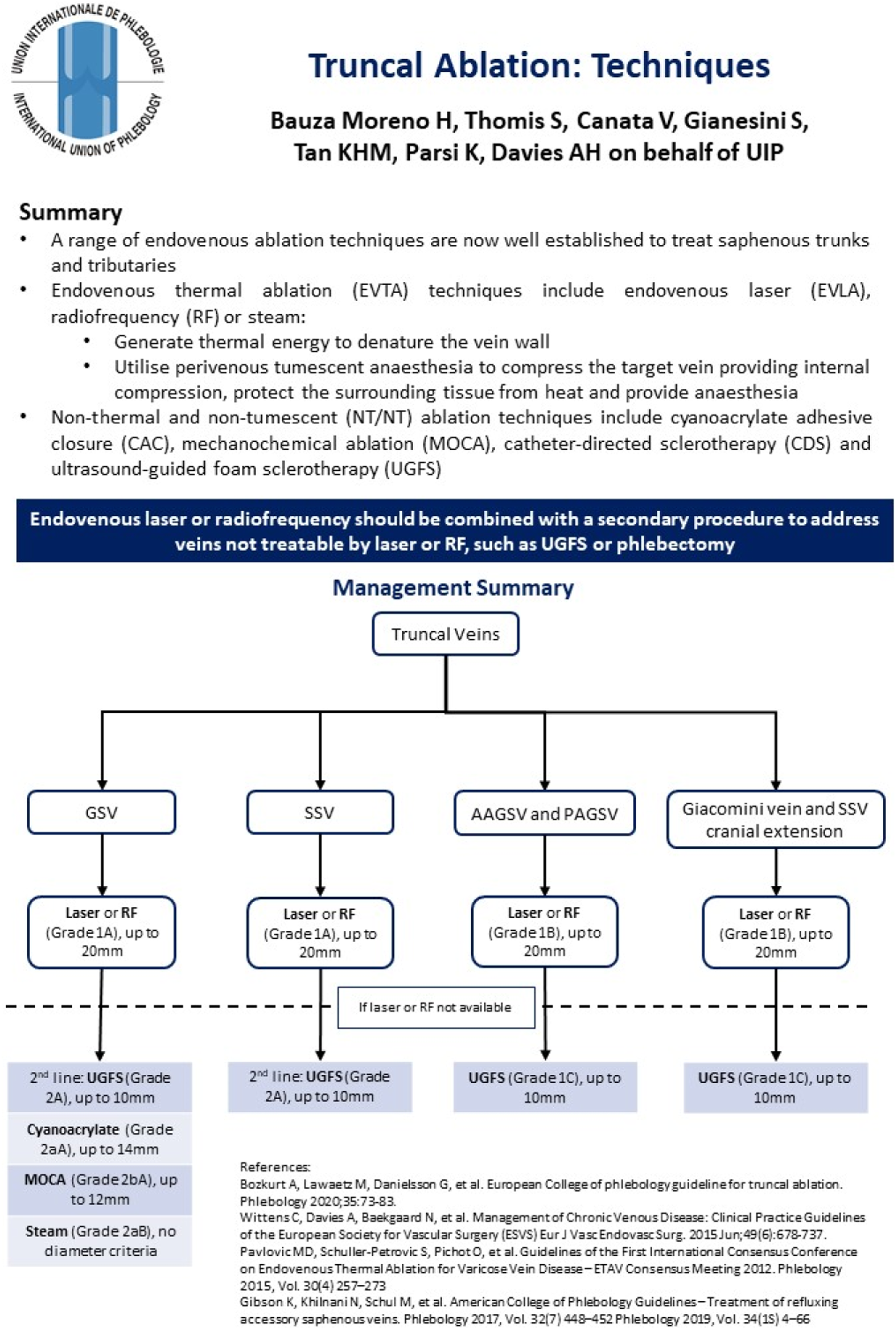
Discussion
This article provides a one-page clinical practice guideline summarising the various thermal and NT/NT techniques that may be utilised for truncal ablation. It is part of a series of publications for the International Union of Phlebology (UIP) One-Page Guidelines which are aimed at ensuring that patients with venous disease receive timely and appropriate care based on current best evidence and expert consensus.
Most national and international guidelines consider thermal ablation methods to be first line in the treatment of truncal veins, assuming anatomical suitability and availability within the centre. Despite this, it must be noted that endothermal ablation techniques are associated with more complications including pain, bruising, skin burns, nerve damage, deep venous thrombosis, and endothermal heat-induced thrombosis, which the use of NT/NT techniques can help avoid. Clinical trials have suggested that NT/NT can give similar technical outcomes (e.g. occlusion rates) and quality of life improvements to thermal ablation methods, but the reduction in pain and post-operative complications has yet to be definitively proven. 1
It is common that a combination of both thermal and NT/NT ablation techniques is utilised in the treatment of patients presenting with CVD. The UIP recommends that further procedures are performed if there are target veins that are not treatable with EVLA or RFA, but there still exists debate if concomitant or sequential treatment, following truncal ablation, is definitively better for patients. While concomitant treatment has been shown to improve disease severity and patient quality of life 2 and can reduce the need for secondary procedures, 3 other studies have suggested that this might represent an overtreatment of patients, with regression of varicose veins seen after index treatment of truncal veins.4,5 Further trials are still required to determine if timing and if the technique choice (UGFS or phlebectomies) result in difference in clinical and quality of life outcomes.
For all healthcare professionals involved in the treatment of venous disease, this article and summary document should act as a convenient summary of the first- and second-line ablation options for truncal vein treatment. In line with multiple national and international guidelines6–9 and reinforced by this one-page guideline, vascular specialists who routinely treat patients with truncal reflux should be reminded of the alternative ablation techniques should EVLA or RFA not be appropriate. This is with the caveat that all recommendations are based on the current levels of evidence available. With ongoing technical development of devices and ablation methods, especially with the NT/NT techniques, the relative effectiveness of techniques may alter the recommendations contained within this document in the future.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Professor Alun Davies on behalf of the UIP.
Contributorship
K.P. and A.H.D. conceptualised the design of the short report and one-page guideline.
H.B.M., S.T., V.C., and S.G. contributed to the literature review and formulation of the recommendations.
M.T. contributed to the formatting and layout of the one-page guideline (![]() ) and wrote the initial draft of the short report.
) and wrote the initial draft of the short report.
All authors reviewed the short report prior to submission.