
Abstract
Background
Complete decongestive therapy (CDT) is a conservative treatment for lymphedema that combines interventions and lifestyle changes. We evaluated the application of CDT after lymphaticovenular anastomosis (LVA) of the lower limb combined with liposuction.
Methods
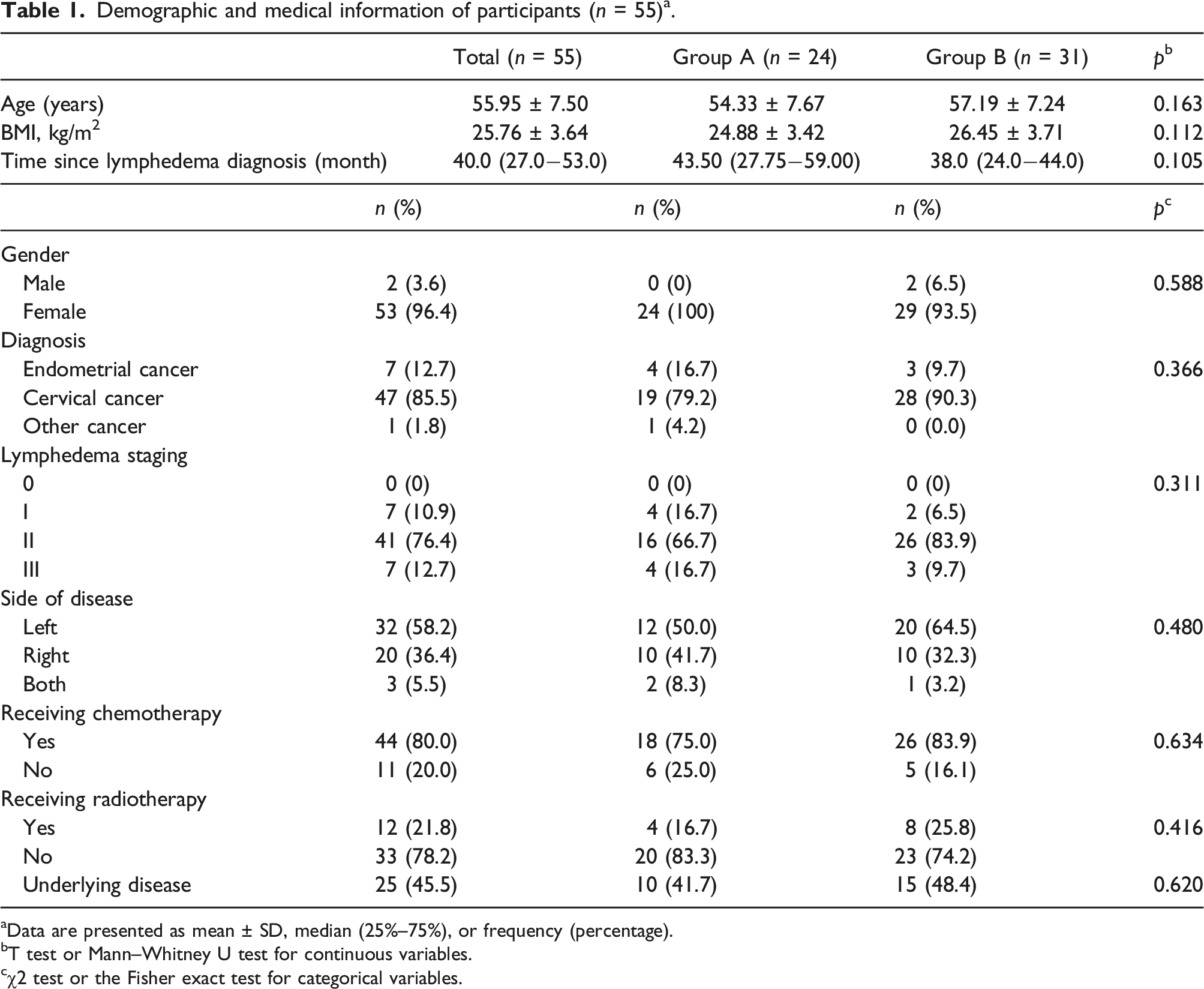
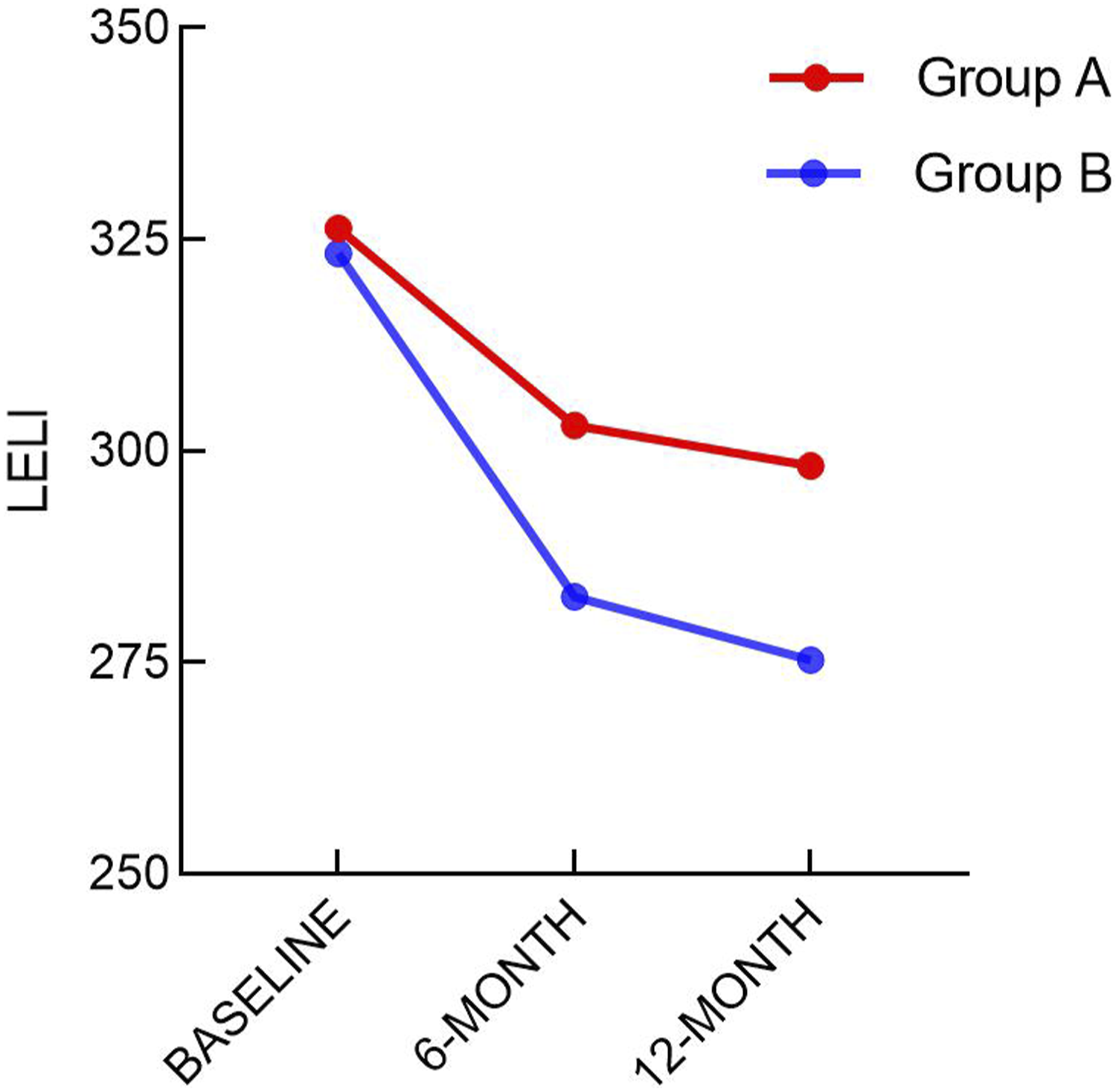
A total of 55 patients who underwent LVA of the lower limb combined with liposuction from January 2021 to July 2022 were enrolled in the study. The patients were divided into groups A (n = 24) and B (n = 31) according to whether they adhered to CDT treatment during the 12-month follow-up. Group A was the non-adherence CDT group and Group B was the adherence CDT group. Lower Extremity Lymphedema Index (LELI) and Lymphoedema Functioning, Disability, and Health Questionnaire for Lower Limb Lymphoedema (Lymph-ICF-LL) were used as prognostic indicators to observe the remission of postoperative lymphedema symptoms in the two groups.
Results
At 6-month and 12-month follow-up, LELI and the score of Lymph-ICF-LL in group B and group A were lower than before the operation (p < .05). The circumference of the affected limb was reduced, and the quality of life was improved in both groups after the operation. The reduction of LELI and Lymph-ICF-LL in group B was higher than in group A, and the difference was statistically significant (p < .05).
Conclusion
This study preliminarily proves the effectiveness of CDT after LVA of the lower limb combined with liposuction, which can maintain and strengthen the surgical effect. Further, CDT treatment is still needed after the operation, which is necessary to reduce the circumference of the affected limb and improve patients’ quality of life.
Keywords
Introduction
Secondary lower limb lymphedema is a common complication of cancer treatment. It often occurs after radical resection of malignant tumors such as endometrial, ovarian, colorectal, and bladder cancer, as well as after simple lymph node dissection biopsy and tumor radiotherapy and chemotherapy.1–3 The literature has reported that the prevalence of secondary lower extremity lymphedema in patients undergoing lymph node surgery, radiotherapy, or during cancer treatment is 11.5% –50.5%.4,5 Long-term lymph stasis causes limb inflammation, adipose tissue hyperplasia, and tissue fibrosis. If not intervened in time, the lesion site may permanently severe swelling, leading to disability, which will have a tremendous negative impact on the patient’s physical and psychological state.6,7
Currently, the treatment methods for lymphedema include conservative treatment, lesion tissue resection, liposuction, lymphaticovenular anastomosis (LVA), and lymph node transplantation.8–11 With the progress of microsurgery equipment and technology, super microsurgery has been used to perform LVA in clinical practice. Through the anastomosis of subcutaneous peripheral micro lymphatic vessels and their accompanying superficial veins, the stagnant lymph fluid is introduced into the venous system further to promote the lymphatic reflux of the affected limb. Because of its minimally invasive and evident effect, LVA has been recognized by more doctors and patients. 12
Liposuction can reduce the swelling symptoms of the affected limb caused by excessive fat deposition in secondary lymphedema. Using swelling technology, longitudinal aspiration, avoiding prominent lymphatic channels, preventing damage to existing lymphatic drainage, and decomposing the fibrosis of the affected limb are especially suitable for secondary lower limb lymphedema.10,13 Studies have shown that liposuction can normalize the limb volume of lymphedema.14,15
Complete decongestive therapy (CDT) is a conservative treatment of lymphedema that combines interventions and lifestyle changes. It consists of four parts: manual lymphatic drainage (MLD), compression bandaging, functional exercise, and skin care. Standardized CDT can relieve limb swelling and improve quality of life, particularly important for postoperative effect maintenance.16–18 Therefore, the study retrospectively analyzed and evaluated the application of CDT in LVA of the lower limb combined with liposuction, aiming to provide reference and guidance for clinical treatment of lower extremity lymphedema.
Material and method
Patients
This study is a retrospective analysis. 55 patients underwent LVA of the lower limb combined with liposuction from January 2021 to July 2022 at the Department of Burn and Plastic Surgery, Xi’an Central Hospital. They were selected and divided into groups A (n = 24) and B (n = 31) according to whether the patients adhered to CDT after 12-month follow-up. According to the International Society of Lymphology (ISL) stage, the patients were included in stage I–III patients with lower extremity lymphedema.
Operative technique
Every affected limb typically had three or four anastomoses. The lymphatic vessels in the subcutaneous superficial fascia layer and superficial veins were directly found under the 6–10 times surgical microscope. After determining the lymphatic vessels to be anastomosed, 11-0 nylon sutures were used under the 10–14 times surgical microscope to perform four-needle anastomosis of the distal end of the lymphatic vessels and the proximal end of the superficial vein (end-to-end anastomosis). After the anastomosis, the lymph flow into the venous lumen was observed, and there was no venous blood reflux. It was confirmed that the anastomosis was unobstructed, and the surgical incision was sutured intermittently.
The liposuction area marked the fat accumulation in the lower limbs of the patients. After the corresponding incision was designed, the swelling fluid was evenly injected into the fat layer of the left thigh. After waiting 20 min, the lower limb fat was sucked with a negative pressure liposuction machine to avoid the anastomosis area. At the same time, the subcutaneous fat particles were evenly sucked out, and the surgical incision was closed layer by layer. A high-elastic bandage was used to prevent subcutaneous hematoma after liposuction after surgery. After 3 days, the low-pressure bandage was replaced, and the pressure dressing was continued for 2 weeks. Elastic mesh covers were worn after discharge.
Complete decongestive therapy
Standardized two-stage CDT treatment was started 3 months after operation. The treatment measures of stage 1 (treatment period) include careful skin and nail care (to prevent infection), therapeutic exercise, MLD, and elastic bandage pressure dressing. The purpose of stage 2 (maintenance phase) is to maintain and optimize the therapeutic effect of stage 1. In stage 1, the lymphedema therapist administered CDT to the patients, and the circumference and volume of the limbs were measured regularly to evaluate the efficacy. Stage 2 of the treatment included wearing elastic mesh sleeves when awake, adding polyester pads to sites of severe fibrosis at night, and continuing application of pressure with a low-elastic bandage or flexible mesh cover, along with adherence to skin care, continuous functional exercises, and self-MLD as demand. The elastic mesh sleeves should maintain a uniform pressure of 30–60 mmHg and 20–40 mmHg during the day and night.
As the central part of CDT, MLD aims to stimulate lymphatic flow through gentle and rhythmic massage, promote excessive tissue fluid removal, and soften fibrotic tissue. As a slow, rhythmic, and light touch massage technique, patients are massaged at a frequency of 5 days/week, 60∼90 min/day, for 2∼4 weeks, with minimal skin stretching to promote natural drainage in the direction of lymphatic flow. MLD has been shown to stimulate lymph lymphatic or lymphovenous anastomosises. 19 MLD includes four basic techniques (stationary circle, rotary, pump, and scoop techniques), starting from the adjacent segments of the affected limb; the direction of action is from the distal end to the proximal end, following the physiological lymphatic reflux direction. 20
In stage 1, compression bandaging is pressure bandaging through tubular bandages, finger/toe bandages, padding bandages, and low-pressure bandages. In stage 2, elastic mesh sleeves that cover from the root of the thigh to the ankle are worn to antagonize muscle contraction, which helps to reduce interstitial fluid production and lymphatic load. The elastic mesh sleeves should be replaced every 3–6 months or when they lose elasticity.
Functional exercise is essential for treating lymphedema; patients can do a series of lower limb movements such as ankle pump exercise, elevation relaxation, air boarding, and knee shaking, promoting lymphatic flow and protein absorption. The combination of flexible training and pressure bandages or elastic mesh sleeves can help to improve lymphedema and prevent tissue contracture. Resistance exercise can be used as an adjunct to pressure therapy, which will appropriately increase muscle strength and tension, stimulate the pumping of veins and lymph, and contract the lymphatic vessels of the sympathetic nerve, which is beneficial to treating lymphedema.
At the same time, meticulous skin care was carried out to maintain skin health and reduce the risk of infection. Because the average PH value of the skin surface is 5∼6 weakly acidic, use the PH value of neutral or weakly acidic emollients to clean and moisturize the skin regularly and try to avoid long-term hot baths, hot springs, and exposure to cold. 21
Lower Extremity Lymphedema Index
LELI
22
was developed by Yamamoto et al. The LELI was calculated from the circumference and body mass index (BMI) after lower extremity circumference measurements at the superior edge of the patella, 10-cm above and below the patella, the lateral malleolus, and the dorsum of the foot. The calculation formula is
Lymphoedema Functioning, Disability, and Health Questionnaire for Lower Limb Lymphoedema
Lymphoedema Functioning, Disability, and Health Questionnaire for Lower Limb Lymphoedema (Lymph-ICF-LL) 25 has 28 items divided into five subscales: physical function, mental function, general tasks/household, mobility, and life domains/social life. The scores of scale range from 0 to 100. According to score of Lymph-ICF-LL, the lower extremity lymphedema was classified as no edema (score 0–4), mild edema (score 5–24), moderate edema (score 25–49), severe edema (score 50–95), and highly severe edema (score 96–100). The results show that Lymph-ICF-LL has good reliability and validity in Chinese version 26 and other language versions.27,28 The Chinese version of Lymph-ICF-LL was filled out three times pre-operation, 6-month follow-up and 12-month follow-up to evaluate the improvement of postoperative quality of life.
Statistical analyses
SPSS 22.0 statistical software was used to analyze the data. The measurement data conforming to the normal distribution were expressed as mean ± standard deviation (
Results
Demographic and medical information of participants (n = 55) a .
aData are presented as mean ± SD, median (25%–75%), or frequency (percentage).
bT test or Mann–Whitney U test for continuous variables.
cχ2 test or the Fisher exact test for categorical variables.
Comparison of LELI between the two groups at different times [

Comparison of LELI between the two groups at different time points.
Comparison of Lymph-ICF-LL scores between the two groups at different times [

Comparison of score of Lymph-ICF-LL between the two groups at different time points.
Case reports
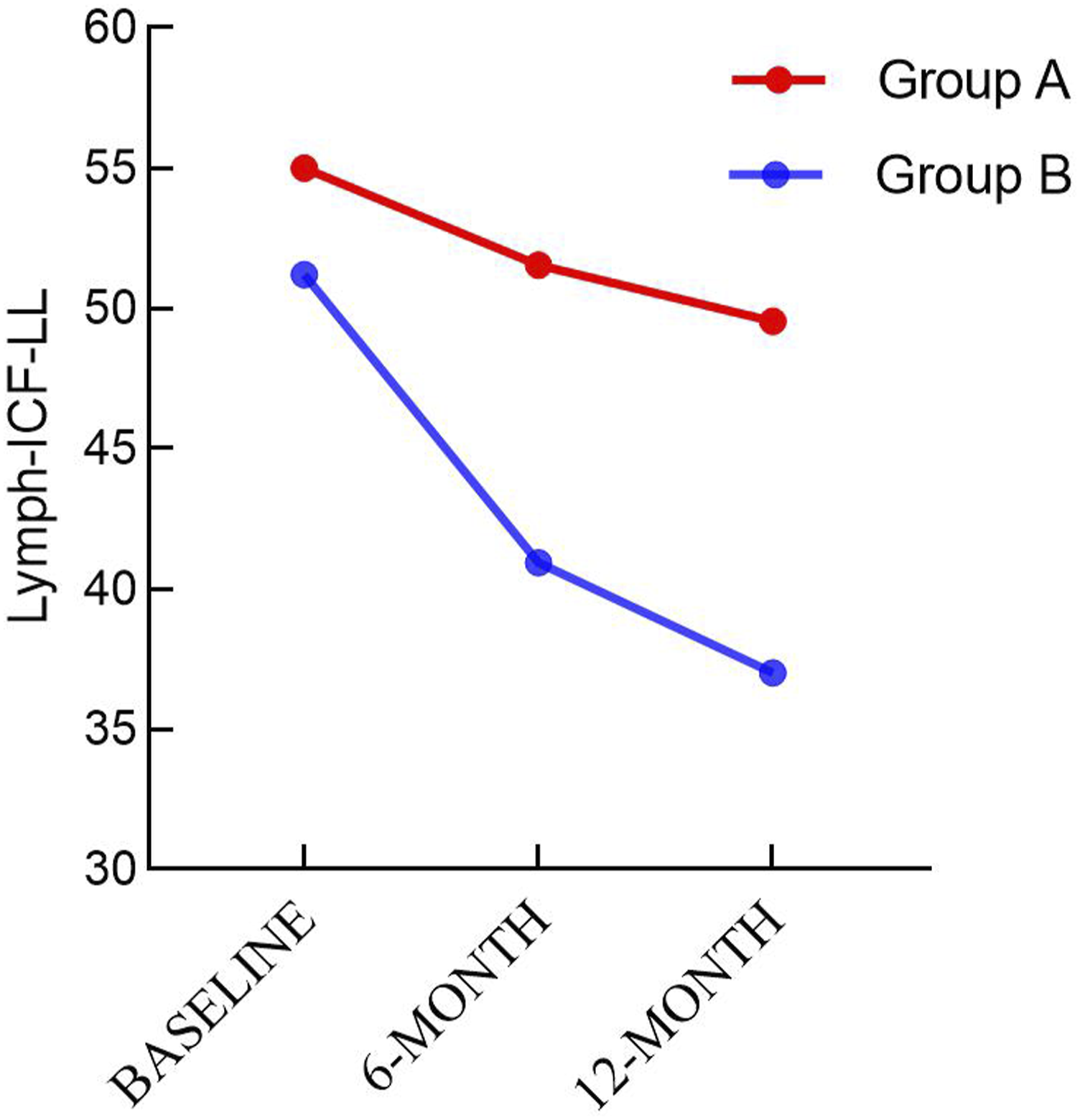
A 49-year-old female patient underwent operation for liposarcoma of the left thigh 13 years ago and received 20 times of postoperative radiotherapy. She developed secondary lymphedema of the left lower extremity 10 years ago and was treated with lymphatic vein anastomosis combined with liposuction in our department. Anastomosis was performed on the inside of the thigh, the inside of the knee joint, the outside of the knee joint, and the inside of the calf. The capacity of liposuction in the left lower limb is 1400 mL. Postoperative standardized CDT comprehensive detumescence treatment 3 months after operation. The LELI of patients before the operation, 6 months after the operation, and 12 months after the operation were 311,260 and 239, respectively; Lymph-ICF-LL scores before the operation, 6 months after the operation, and 12 months after the operation were 45, 24, and 20, respectively; the patient’s limb circumference was reduced, and the quality of life was improved (Figure 3). Before the operation (a). 6-month follow-up (b). 12-month follow-up (c).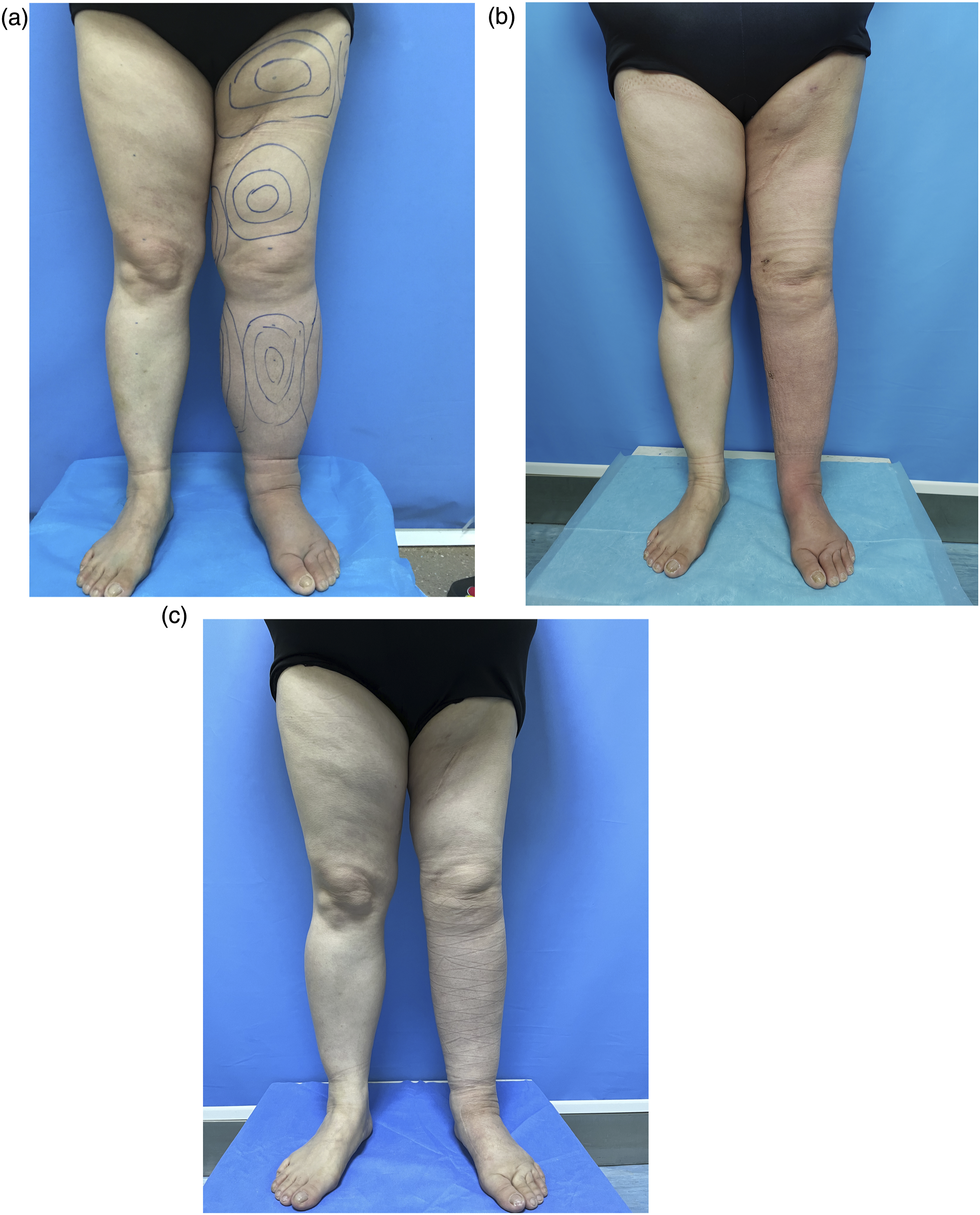
Discussion
Lymphedema is a chronic disease, usually incurable, like other chronic diseases, and requires lifelong care, attention, and psychological support. 10 For example, diabetic patients need drugs (insulin) or special diets (low calorie and low sugar) to maintain metabolic homeostasis; hypertensive patients need continuous drug therapy to control blood pressure. Patients with lymphedema need lifelong treatment to minimize edema, fat sclerosis, and skin ulcers. Poor control of lymphedema symptoms can cause the affected limb to repeatedly suffer from cellulitis or erysipelas infection, resulting in long-term unhealed ulcers, rubber swelling, and even disability. In rare cases, it develops into a highly lethal lymphangiosarcoma (Stewart-Treves syndrome).29,30
As a particular technique, MLD can mobilize the skin and stimulate the lymphatic system to promote lymphatic flow into the venous circulation through lymphatic vessels and existing lymphatic-venous anastomosis. 31 PDT supports deep subcutaneous tissue and counteracts random muscle activity, preventing subcutaneous effusion. The patients also performed regular functional exercises to improve the efficiency of the muscle pump and increase lymphatic circulation. Health education strategies, including exemplary skin care, are essential to improve comprehensive detumescence therapy, which can maintain skin integrity and reduce the risk of infection.
In a related study conducted by Yamamoto et al., 32 82 women received CDT treatment for upper or lower limb lymphedema for 6 and 10 days, respectively. The results showed that upper limb edema was reduced by 58.9%, and lower limb edema was reduced by 73.4%. In a prospective study of Michopoulos E et al., 11 72 patients with stage I lower extremity lymphedema received 20 CDT treatments for 4 weeks. The results showed that the percent reduction of excess volume (PREV) was up to 71.5%. The results of this study showed that according to the LELI and the score of Lymph-ICF-LL, the limb circumference, and quality of life of the two groups of patients were improved. However, patients who insisted on comprehensive CDT treatment after operation had more improvement. Comparing the effectiveness of the above CDT after LVA combined with liposuction, group A showed a more effective improvement in quality of life and a significant reduction in pain. In the first 6 months, CDT played a higher role in reducing limb swelling and improving quality of life and continued to play a slower role in the next 6 months.
In a randomized controlled clinical trial, Wang X et al. 33 showed that CDT treatment 1 week after operation can effectively prevent lower extremity lymphedema in patients with cervical cancer after laparoscopic radical hysterectomy + pelvic lymphadenectomy, which can reduce the incidence of lower extremity lymphedema by 13.6%. Deura et al. 34 conducted a retrospective study to describe the incidence of lower extremity lymphedema in 126 patients with gynecological cancer after 4 months of periodic complex detumescence physiotherapy. The overall incidence was 45.2%, higher than that of Wang X et al.’s study. This may be attributed to a delay in providing CDT. At the same time, it has also been reported that some patients can be treated with prophylactic anastomosis in radical resection of malignant tumors. Clinically, there is no clear statistical standard for when to perform CDT after LVA or liposuction. However, according to our clinical experience, early CDT treatment is more conducive to maintaining surgical results, which is most suitable for 2–3 months after operation.
CDT treatment is usually used to relieve lymphedema in patients with stage I to stage II lymphedema. For patients with stage III lymphedema, due to the apparent limitation of lymph reflux, operation is generally used to relieve edema. However, this study included some patients in the stage III, and standardized CDT treatment was still performed after the operation, which still had a good effect. Therefore, expanding the indications of CDT is recommended, and advanced lymphedema can be surgically linked to CDT to relieve symptoms.
In 2014, the Netherlands published a guideline for multidisciplinary cooperative treatment of lymphedema to delay the disease and improve the quality of life of patients with lymphedema, focusing on the use of a new model of “chronic care model” for the treatment of chronic diseases. 35 In this model, patients play a central role through self-management and active participation. At the same time, the International Classification of Functioning, Disability, and Health (ICF) is used to evaluate the condition, ICF is a conceptual framework used to reflect the function of the human body. The purpose is to provide appropriate diagnosis and treatment, education, and help for patients with specific diseases.36–38 European scholars have applied ICF to the group of patients with lymphedema. Lymph-ICF-LL is a questionnaire based on ICF, which mainly emphasizes the impact of disease on limb function and daily activities of patients.25,39,40 This study shows that the standardized treatment of CDT after operation can reduce the score of Lymph-ICF-LL and improve the quality of life more effectively. However, 6 months after the operation, the improvement in patients’ quality of life is insignificant. Lymph-ICF-LL is a subjective evaluation questionnaire, which will be affected by patients’ subjective thinking and education level and has certain limitations. It must be combined with physical measurement data and imaging examination to evaluate the condition better.
This study has the following limitations: First, the sample size is small, and more patients with lower extremity lymphedema should be included for analysis in the future. Second, the representativeness of the sample is limited. Most of the patients included in the study are women with a history of gynecological malignant tumors, which cannot fully reflect the diversity of the causes of lower extremity lymphedema. In the future, male patients with more history of prostate cancer or patients with primary lymphedema can be included in the study. Third, most patients have moderate and severe lower extremity lymphedema treated in the Department of Burn and Plastic Surgery, which is prone to Berkson bias. For evaluation, mild lymphedema cases should be recruited from other departments such as general surgery, gynecology, and oncology, etc.
Conclusion
This study demonstrated the effectiveness and necessity of CDT after LVA of the lower limb combined with liposuction, which can maintain and strengthen the surgical effect. CDT treatment is still needed after operation, which is necessary to reduce the circumference of the affected limb and improve patients’ quality of life.
Footnotes
Author’s note
The information in the paper is new with neither the entire paper nor any part of its content has been published or has been accepted elsewhere; it is not being submitted to any other journal. Each of the authors has contributed to, read, and approved the manuscript. The journal Phlebology will retain copyright to the published manuscript and its contents.
Acknowledgments
We would like to thank Sameer Grover for editorial support during preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Xi’an Innovation Basic Strengthening Plan - Medical Research Project (22YXYJ0077).
Ethical Statement
Guarantor
Bin Liu (Department of Burn, Plastic and Cosmetic Surgery, Xi’an Central Hospital, Xi’an Jiaotong University).
Contributorship
Dr Xuchuan Zhou, Dr Gejia Ma, N Xi Qi, Dr Aoshuang Qin, and Dr Bin Liu designed and conducted this study, including patient recruitment, data collection, and data analysis. Dr Xuchuan Zhou analyzed and interpreted the data and drafted the manuscript. Dr Gejia Ma led the LVA and liposuction. N Xi Qi and Dr Aoshuang Qin followed up the patients and collected data. Dr Bin Liu was the lead of this study, provided technical material support, and reviewed the write-up and submission. All authors approved the final manuscript.