
Abstract
Background
Mechanochemical endovenous ablation (MOCA) was introduced to treat superficial venous insufficiency of the lower leg with less pain and haematoma. Long-term outcome is still lacking. The purpose was to report long-term outcome and to analyse possible predictors for failure.
Methods
The study was a retrospective pooled analysis of two prospective cohorts previously reported, but with prolonged long-term outcome up to 5-years follow-up.
Results
163 treated legs were analysed. Mean follow-up was 5.4±0.6 years, in which 33 total failures occurred. Four procedures were partially successful. VCSS improved significantly and remained stable after 1 and 2-years, but significantly rose again after 5-years. AVVQ dropped significantly, but increased after 1 year to 4.3 and 6.1 at 5-years follow-up.
Conclusion
MOCA was effective with minimal pain perioperative. However, anatomical success deteriorated after 1-year and showed even less results after 5-years, mainly due to partly recanalization, while clinical results were less affected. There were no clear clinical predictors for failure.
Keywords
Introduction
Endovenous techniques have replaced standard surgical treatments such as ligation and stripping of the great saphenous vein as the gold standard in the treatment of chronic superficial venous insufficiency of the lower limb. Endothermal techniques, such as endovenous laser ablation (EVLA) and radiofrequency ablation (RFA) are related to less pain, less haematoma and a faster recovery time, with the inherent risk of thermal damage to perivascular structures. Therefore, tumescent anaesthesia is always needed. To avoid these risks, mechanochemical ablation (MOCA) has been introduced combining the concept of mechanical endothelial damage with the infusion of sclerosant. In May 2008, the ClariVein® infusion catheter gained clearance from the US Food and Drug Administration (FDA) for the indication of infusion of physician-specified agents in the peripheral vasculature. ClariVein® obtained the CE mark in April 2010, with a specific indication for endovascular occlusion of incompetent veins with superficial venous reflux. 1 Thereafter, evidence accumulated on the effectiveness of MOCA with anatomic success rates at 12 months ranging from 87% to 97%. Major complications, particularly nerve injury, were rare (≤0.2%). 2 In 2019, the 2-year results of a multicenter prospective randomized controlled trial (MARADONA trial) were published comparing MOCA with RFA. 3 That study showed that MOCA of the GSV results in less postoperative pain, although the absolute difference was small. Clinical success rates were equal to those of RFA at 1- and 2-year follow-up, but with more anatomic failures, especially partial recanalizations. 4 Importantly, the inclusion within this trial was terminated before reaching the sample size on anatomic success. In the meanwhile, follow-up has extended considerably, but knowledge on possible factors influencing outcome is still lacking. The aim of the current study was to report long-term follow-up of patients treated with MOCA and to analyse whether certain factors were predictive for failure.
Methods
Study design
The design of the study was a retrospective pooled analysis of two prospective cohorts previously reported, but now with prolonged long-term follow-up. Both cohorts included patients treated with MOCA using polidocanol as the sclerosant and all patients were treated in the same tertiary referral center. The first cohort (cohort A) derived from a prospective study describing 5-year outcomes of patients treated with MOCA. 5 The second cohort was patients included in a multicenter prospective randomized controlled trial and with their follow-up extended from two to 5 years (cohort B). 4
The study was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice guidelines. The study was approved by the Medical Ethics Committee of Nijmegen (CMO 2011-091). Eligible patients who met the inclusion criteria were fully informed, and those who signed the informed consent were included.
Treatment
The procedure has been described before in detail. 1 In short, before the procedure, the area to be treated was disinfected, and sterile drapes were applied with the patient in the supine position. Subsequently, a catheter was inserted into the incompetent GSV after local anaesthesia and under Duplex ultrasound guidance. A 4 Fr introduction sheath was inserted and the tip of the ClariVein® catheter (Merit Medical®, South Jordan, UT, USA) was placed 5 mm below the orifice of the superficial epigastric vein or 2 cm below the sapheno-femoral junction (SFJ). The rotating wire was then activated for 10 s to induce vasospasm before withdrawal at a steady pullback speed of 7 s/cm while continuously injecting the liquid sclerosant in a dosage of 2 mL 3% polidocanol for the first 10 to 15 cm and 1.5% polidocanol for the last part. After treatment, the deep venous system was studied immediately with ultrasound. While the patient was still in the horizontal position, liberal calf massages and patient-induced dorsiflexion were performed. Patients were then advised to walk immediately after completion of the procedure and were discharged with class 2 compression stockings (30–40 mm·Hg) for 24 h continuously and subsequently during day time for 2 weeks.
Definitions and end points
Definitions of terms used for the study have been published before. 3 In brief, anatomical success was defined as occlusion of the treated GSV segment as measured with duplex ultrasonography. Technical success was defined as initial technical success rate of the procedure, where the catheter can be safely placed at a defined distance from the SFJ and the GSV can be treated without technical problems. If the planned segment could not entirely be treated, this was scored as a partial successful procedure. During follow-up, the successful treated part of the segment was checked by duplex ultrasound; if this segment remained occluded, this was scored as no failure. Failure of treatment included either a type I failure (non-occlusion) in which the treated vein failed to occlude initially and never occluded during the follow-up, or a type 2 failure (recanalization), in which the treated vein occluded directly after treatment, but recanalized, partly (>10 cm) or completely, at a later time point during follow-up. Clinical success was defined as an objective improvement of clinical outcome after treatment, measured with the Venous Clinical Severity Score (VCSS) of at least one point. 6
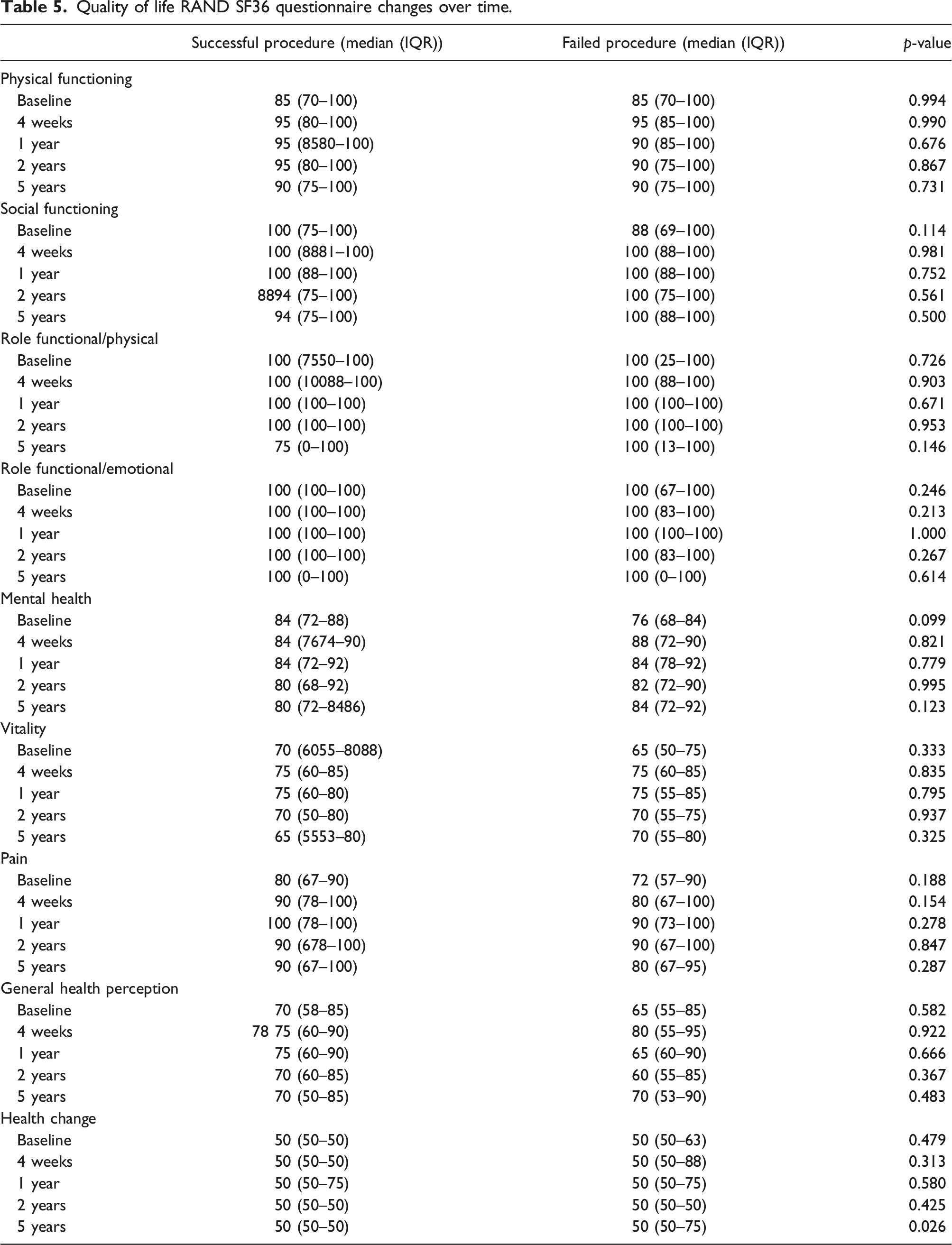
Primary endpoints were anatomic and clinical success and postprocedural pain after treatment for GSV incompetence with MOCA. Secondary endpoints were operation time, pain during the treatment, technical success, complications, disease-specific quality of life and time to return to daily activities/work. Quality of life scores were assessed with Short Form-36 (SF-36), a multidimensional measurement of general health, which yields eight domains of functional health and well-being scores. Also, the ‘Dutch translated’ Aberdeen Varicose Vein Questionnaire (AVVQ), a validated disease-specific quality of life measurement for chronic venous insufficiency, was used. 7 Both questionnaires were completed preoperatively, after 4 weeks, 1 year, 2 years and 5 years of follow-up.
Statistical analysis
Categorical variables are presented as number followed by percentage. Differences between groups were tested using Chi Square tests. Continuous variables are presented as means and standard deviation or median and interquartile range, if applicable. Distribution of continuous data was tested using the Kolmogorov–Smirnov test and by visual inspection of plots.
Univariate logistic regression was performed to identify predictors of failure of the procedure through 5 years follow-up. Variables with a p-value <.100 in univariate analysis were entered in a stepwise backward manner into a multivariate logistic regression model. Due to the number of events, no more than three variables could be entered in the final model. Significance of all other tests was set at p<.05. Statistical analysis were performed using IBM SPSS Statistics (SPSS version 25.0 for Windows, IBM Corporation, Armonk, NY, USA).
Results
Patient characteristics
Patient characteristics at baseline (N = 147 patients).
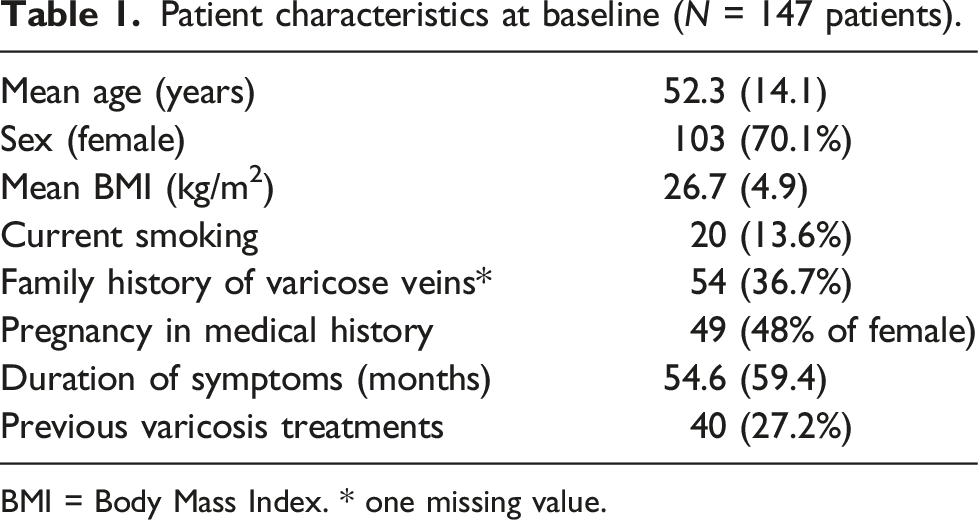
BMI = Body Mass Index. * one missing value.
Clinical details of venous disease at baseline (N = 163 legs) and 5 years follow-up (N=112).
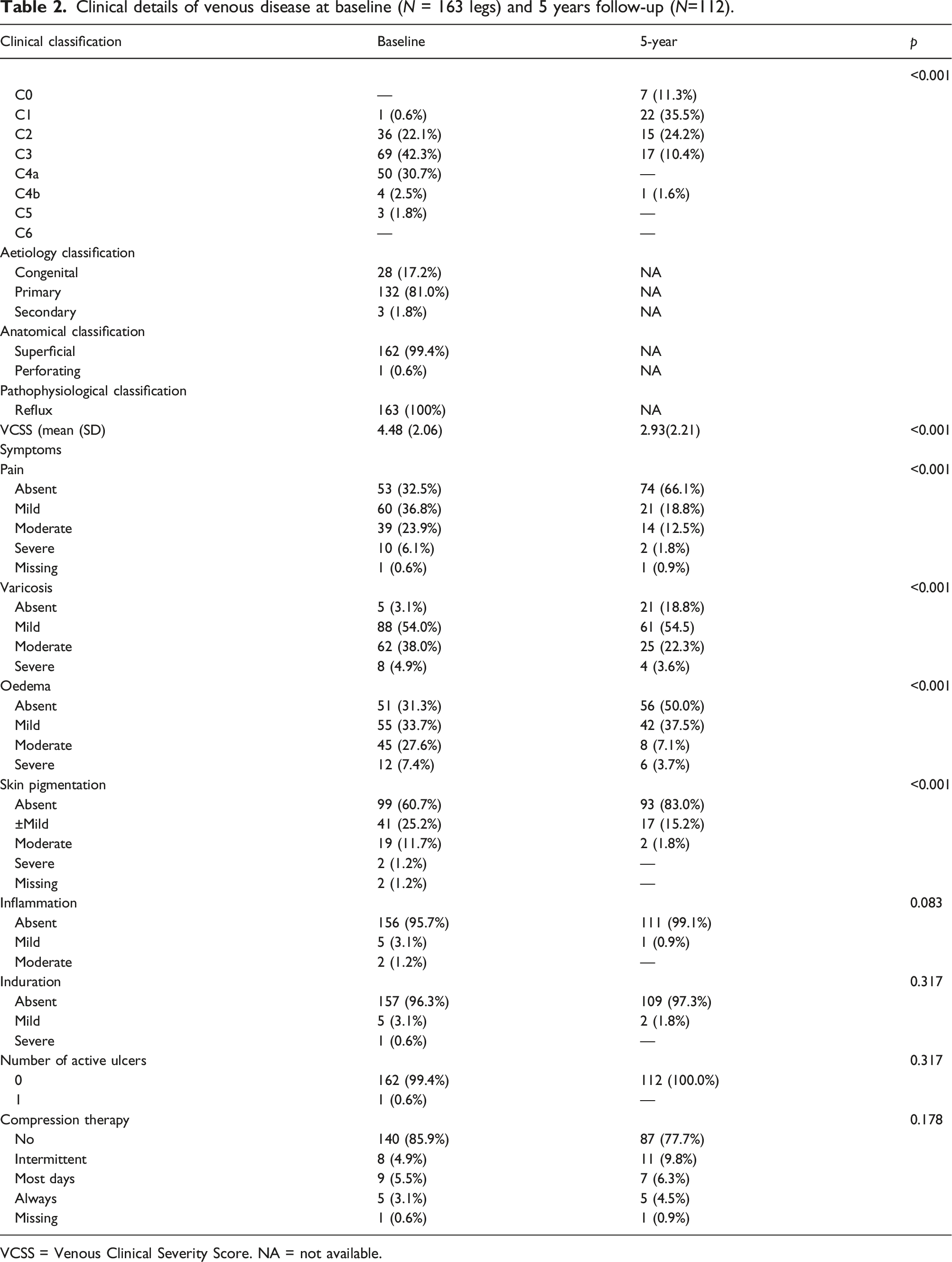
VCSS = Venous Clinical Severity Score. NA = not available.
Procedural outcomes
Procedural outcomes (N = 163 legs).
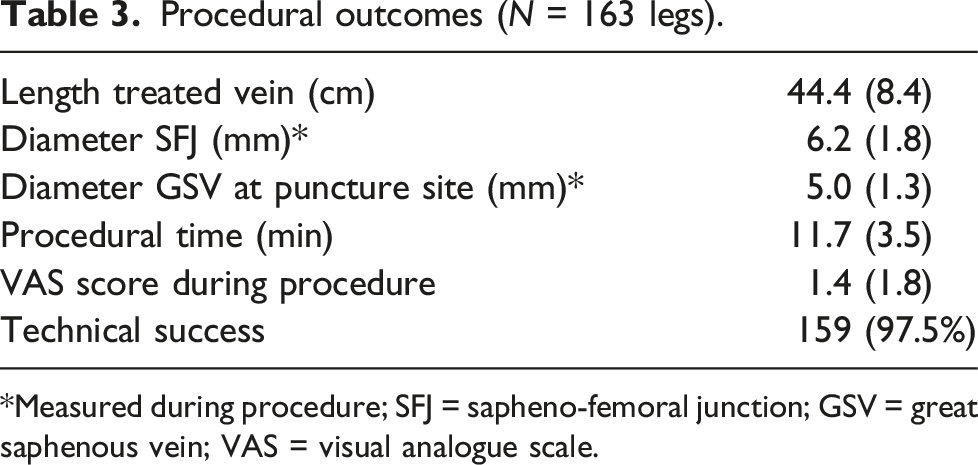
*Measured during procedure; SFJ = sapheno-femoral junction; GSV = great saphenous vein; VAS = visual analogue scale.
Early results
The mean VAS at 14 days after treatment was 0.6± 0.9. Mean patient satisfaction at 30-days, related to treatment on a scale from 0 to 10, was 8.8± 1.0. Further details of early results have been described before in separate reports of cohorts A and B.4,5
Late results
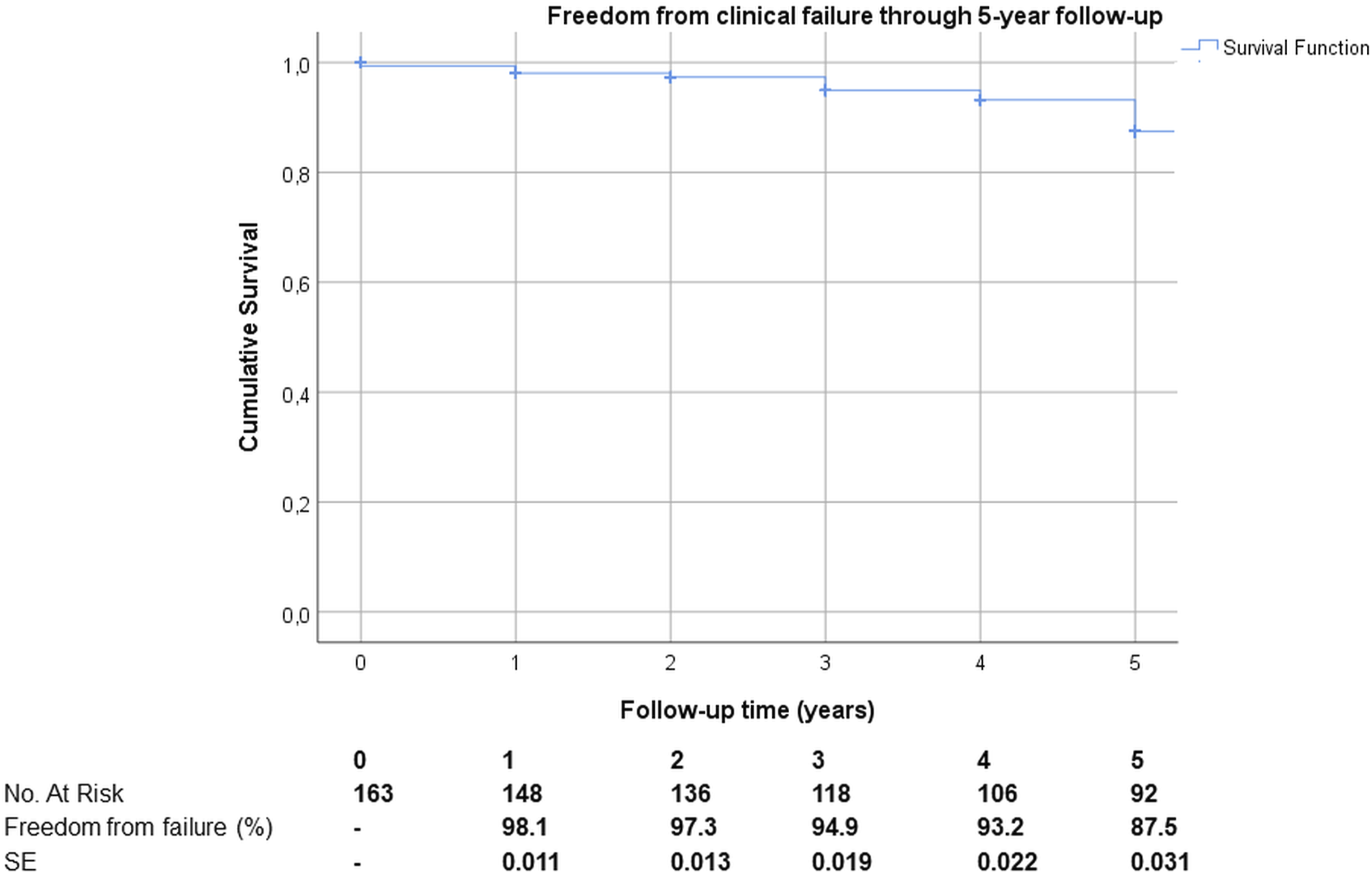
Mean follow-up was 5.4±0.6 years. During this period of time, 33 anatomic failures occurred, 22 from cohort A (23.7%) and 11 from cohort B (16.7%), p = .284. As a consequence, 126 legs were treated successfully, 4 were partly successful procedures (meaning not the entire planned segment could be treated, but an important part was treated successfully) and 33 legs failed (Figure 1). From clinical perspective results were better at all yearly time points measured and are depicted in Figure 2. Freedom from anatomic failure after MOCA treatment during 5 years follow-up. Freedom from clinical failure after MOCA treatment during 5 years follow-up.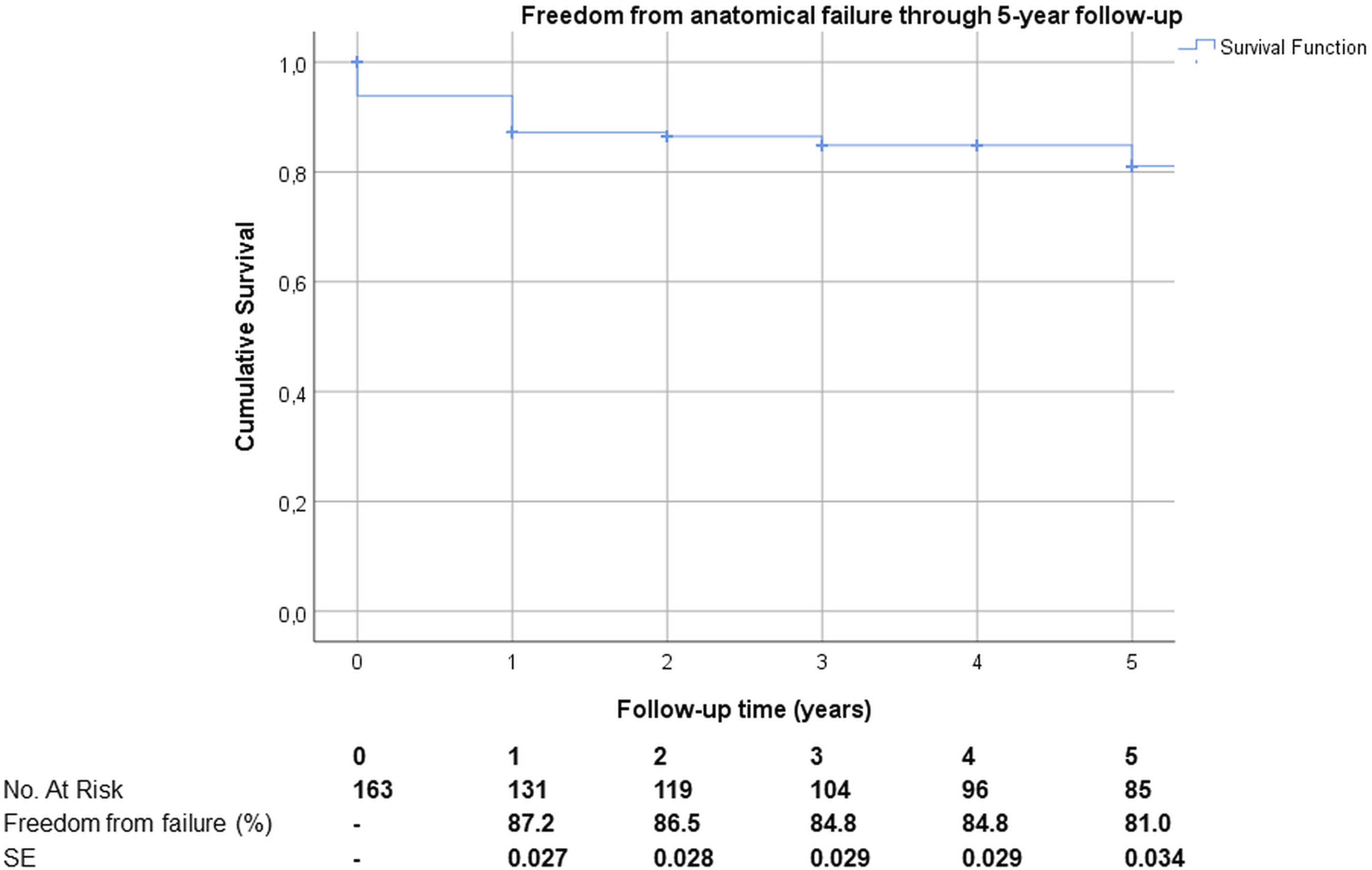
Univariate comparison of successful and failed MOCA procedures during follow-up (N = 163 legs).
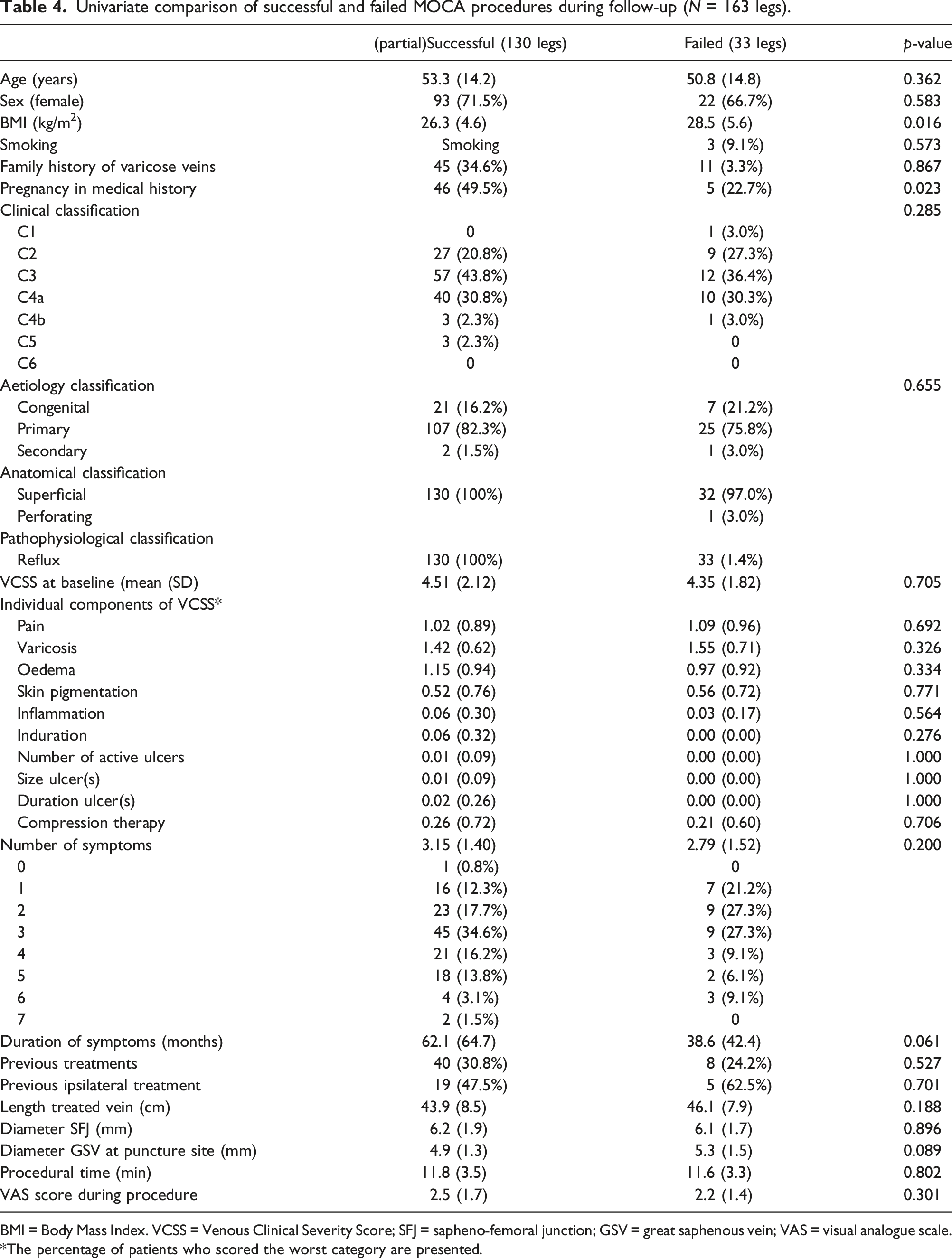
BMI = Body Mass Index. VCSS = Venous Clinical Severity Score; SFJ = sapheno-femoral junction; GSV = great saphenous vein; VAS = visual analogue scale. *The percentage of patients who scored the worst category are presented.
Predictors for anatomic failure at multivariate logistic regression analysis
At multivariate logistic regression analysis, BMI was not a predictor for failure (OR 1.090, 95% CI 0.996–1.193, p = .060), but again, pregnancy in medical history appeared to be a predictive for successful procedure (OR 0.260, 95% CI 0.082–0.820, p = .022). In addition, duration of symptoms was also predictive for success, although this was not a strong predictor (OR 0.988, 95% 0.977–1.000, p = .047). Age and sex adjusted analyses showed similar results without significant differences.
Venous clinical severity score
Compared with baseline, VCSS score dropped significantly from a median of 4.0 to 1.0 at 4 weeks, and remained stable after 1 year and 2 years follow-up. At 5 years follow-up, again a significant rise to 2.0 was noted (Figure 3). Venous Clinical Severity Score (VCSS) assessment and results over time through 5 years follow-up.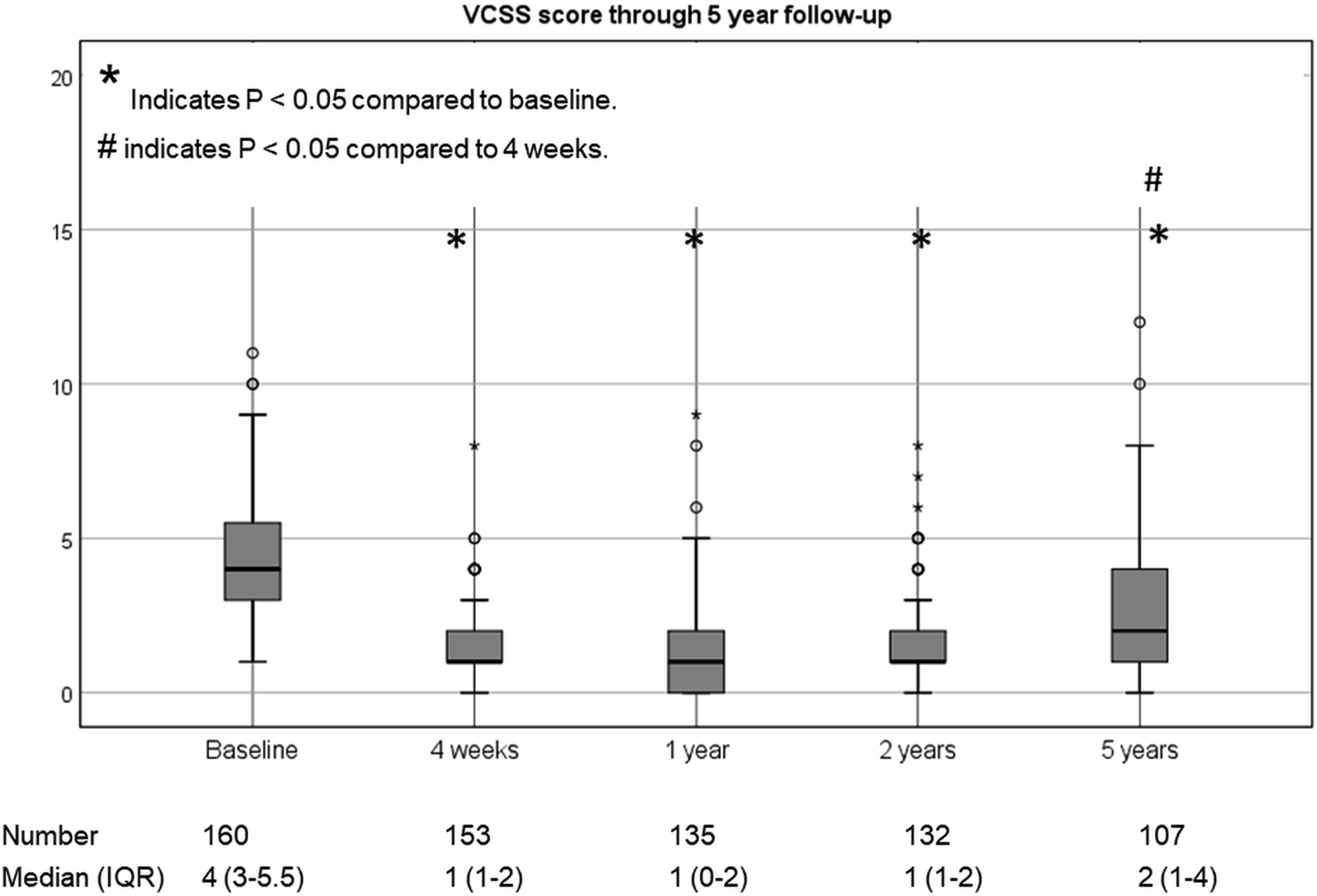
Quality of life
Completely filled-in AVVQ forms were returned at baseline by 105 patients (64%), at 4 weeks by 136 patients (83%), at 1-year by 110 patients (67%), 2-years by 104 patients (63%) and at 5-years by 82 patients (50%). Compared with baseline, total AVVQ score dropped significantly from a median of 10.4 to 1.5 at 4 weeks, but increased again after 1 year to 4.4 and 6.2 at 5 years follow-up. The rise between 4 weeks and the following years was significant (Figure 4). Aberdeen Varicose Vein Questionnaire (AVVQ) assessment and results over time through 5 years follow-up.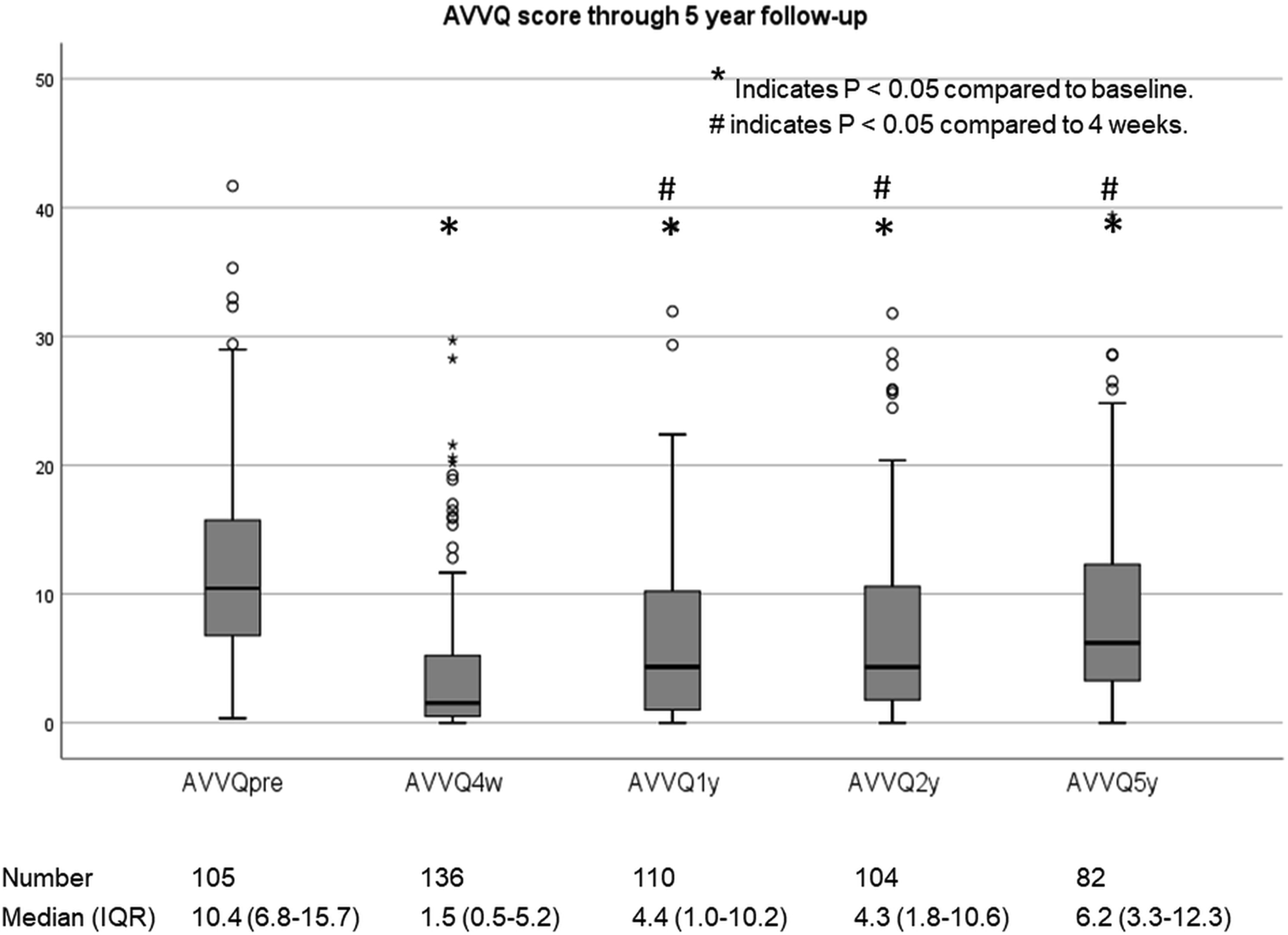
Quality of life RAND SF36 questionnaire changes over time.
Discussion
This study supports findings of previous studies in which MOCA was found to be as effective in the early postoperative phase as other treatments in patients with chronic venous insufficiency of the lower leg due to GSV incompetence and with less severe pain during and after the procedure. However, anatomical success with MOCA at the long-term seems to be lower compared to data reported for with thermal ablation. Nugroho et al. reported a meta-analysis of four randomized clinical trials (RCTs) comparing the anatomical success of MOCA for GSV insufficiency to thermal ablation. Anatomical success rate at 1 month (short-term) and a period of more than 6 months but less than 1-year follow-up was 93.4% and 84.5%, respectively, with MOCA, and 95.8% and 94.8%, respectively, with thermal ablation. 8 Thereafter, another RCT appeared with 3-year follow-up and showing a statistically significantly lower GSV occlusion rate of 82% after MOCA versus 100% after thermal ablation (p = .005). In the MOCA group, GSVs that were larger than 7 mm in diameter preoperatively were more likely to recanalize during the follow-up period, something that was not confirmed in the current analysis. Moreover, the partial recanalizations observed in the proximal GSV at 1-year progressed during the 3-year follow-up. 9 Our current study had a longer follow-up of 5-years and included a three-fold number of patients treated with MOCA. A clear relation of recanalizations with the diameter of the treated vein segment could not be found, but the deterioration in terms of anatomical success at the longer term was likewise. Clinical effects, and more so quality of life, was less affected in both studies. 9
Factors that may have contributed to the less favourable results at longer term include the fact that most patient have been treated within the relatively early learning curve and meanwhile an evolution has taken place on various aspects of the procedure. First, in general, the concentrations of polidocanol used in the Netherlands have been too low. In the early Dutch studies, two levels of sclerosant concentration were used, that is, 2 mL of 2% polidocanol to treat the first 10 cm and 1.5% to treat the remaining vein length. In a dose finding study, different concentrations of liquid polidocanol were used (2% and 3%) and were compared with 1% polidocanol microfoam in a RCT. The 1% foam was clearly less effective than 2% or 3% liquid polidocanol (p < .001) for the treatment of GSV incompetence, 10 but it needs to be emphasized that ClariVein® is not intended to be used with foam. In a second dose finding study, patients with symptomatic primary GSV incompetence were randomized to MOCA with 2% polidocanol liquid or MOCA with 3% polidocanol liquid. The results showed a higher success rate for MOCA with 3% polidocanol liquid than for MOCA with 2% polidocanol liquid at 6 months of follow-up. However, the difference in quality of life was not significant. 11 Second, the device was initially purged with saline. The device retained about 1 mL of liquid so the first mL entering the vein was saline; many people are now purging with sclerosant. Also, leakage of sclerosant by improper use of the stopcock may have taken place, the reason why now the stopcock has been removed. Third, in the beginning, it was not the practice to check the first 10 cm and to retreat if the vein was not closed. Finally, in contrast with other studies, in our current study, and especially in cohort B, the percentage of patients treated was mainly C3 or higher, as only these patients were amendable for reimbursement during the enrolment period. Despite these liabilities, the recent European Society for Vascular Surgery (ESVS) 2022 Clinical Practice Guidelines on the Management of Chronic Venous Disease of the Lower Limbs state that MOCA is a reasonable alternative for patients preferring non-thermal non-tumescent treatment, even if the occlusion rate at 3-years was inferior to that of thermal ablation. In terms of recommendation, for patients with GSV incompetence requiring treatment, mechanochemical ablation may be considered when a non-thermal non-tumescent technique is preferred (Class IIb, Level A). 12
The current study did not reveal clear clinically important predictors for failure. BMI seemed to have some negative influence at univariate analysis, but this effect disappeared at multivariate analysis. Some studies appeared focusing on BMI in patients who underwent thermal ablation. In a large single-center, retrospective cohort study with 9739 endovenous ablations performed on 3070 patients (3862 endovenous laser procedures and 5831 radiofrequency ablation procedures), an increased recanalization risk was found with ablations performed on perforator veins. A secondary multivariate analysis was performed with the exclusion of perforator veins due to their five times increased risk of recanalization, and showed no significant difference of recanalization across all BMI subgroups. 13 A recent narrative review after risk factors for saphenous vein recanalization after endovenous radiofrequency ablation showed BMI and saphenous trunk diameter to be the only two recognized characteristics that may affect short and long-term recanalization rate. 14 Every 1-point increase in BMI would result in an 8.9% increase in the hazard of developing recurrent GSV flow. 15 In another multicenter, retrospective cohort study including 65,329 patients who had undergone a venous procedure (endovenous thermal ablation, phlebectomy or ultrasound-guided foam sclerotherapy), outcomes progressively worsened with a BMI >35 kg/m2. The treatment outcomes for patients with a BMI ≥46 kg/m2 were so poor that weight loss management was advised before offering CVD treatment. 16
The protective finding of previous pregnancy related to a successful outcome after MOCA cannot be explained or supported by literature. During pregnancy, maximum changes are seen in the superficial venous system in the thigh. The effect seems to be more pronounced on the left and the changes in reflux return to pre-pregnancy levels in the puerperium.17,18 Furthermore, number of pregnancies is correlated with the incidence of pelvic vein insufficiency,19,20 but not with GSV reflux. 21 Unfortunately, to our knowledge, no literature exist on the relation between MOCA outcome and pregnancy.
This study has some limitations. First, data are derived from the early phase of MOCA treatment and may therefore not reflect current practice. Other non-thermal non-tumescent techniques such as Flebogrif® have entered the market as well, but we have to await their long-term results. Also the possible favourable effect of sodium tetradecyl sulfate instead of polidocanol should be further explored. In the current studies, polidocanol was used as tetradecyl sulfate is not registered in the Netherlands. Second, not all questionnaires were complete, although compared to other venous studies, they compared favourably. Another limitation of this study is that during follow-up, no information on the entire CEAP classification was gathered, but only the C was scored.
In conclusion, MOCA was effective in the early postoperative phase in patients with chronic venous insufficiency of the lower leg due to GSV incompetence with minimal pain during and after the procedure. However, anatomical success with MOCA deteriorates after 1-year and showed even less results after-five years, mainly due to partly recanalizations, while clinical outcome was less affected. No recommendations can be given with regard to predictors for failure.
Footnotes
Acknowledgements
With regard to Cohort A: This was an investigator-initiated study supported by Vascular Insights Ltd. Vascular Insights was not involved in study design, data collection, data analysis, manuscript preparation, or publication decision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Vascular Insights Ltd.
Author’s note
This paper has been presented at the 19th World Congress of the International Union of Phlebology, Istanbul (Turkey), 12-16 September 2022.
Guarantor
CJZ.
Contributorship
ME Conception and design, analysis and interpretation, writing the manuscript, critical revision, approval of the manuscript, agreement to be accountable. S Conception and design, analysis and interpretation, data collection, critical revision, approval of the manuscript, agreement to be accountable, statistical analysis. D Analysis and interpretation, data collection, critical revision, approval of the manuscript, agreement to be accountable, statistical analysis. MMPJ Conception and design, analysis and interpretation, critical revision, approval of the manuscript, agreement to be accountable. CJ analysis and interpretation, writing the manuscript, critical revision, approval of the manuscript, agreement to be accountable.